
Correlation of Intravascular Ultrasound with Histology in Pediatric Pulmonary Vein Stenosis

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Postmortem Samples
2.2. In Vivo Samples
2.3. Intravascular Ultrasound in Live Patients
2.4. Measurements
2.5. Ethics Statement
3. Results
3.1. Patients
3.1.1. Postmortem Samples
3.1.2. In Vivo Samples
3.2. Intravascular Ultrasound
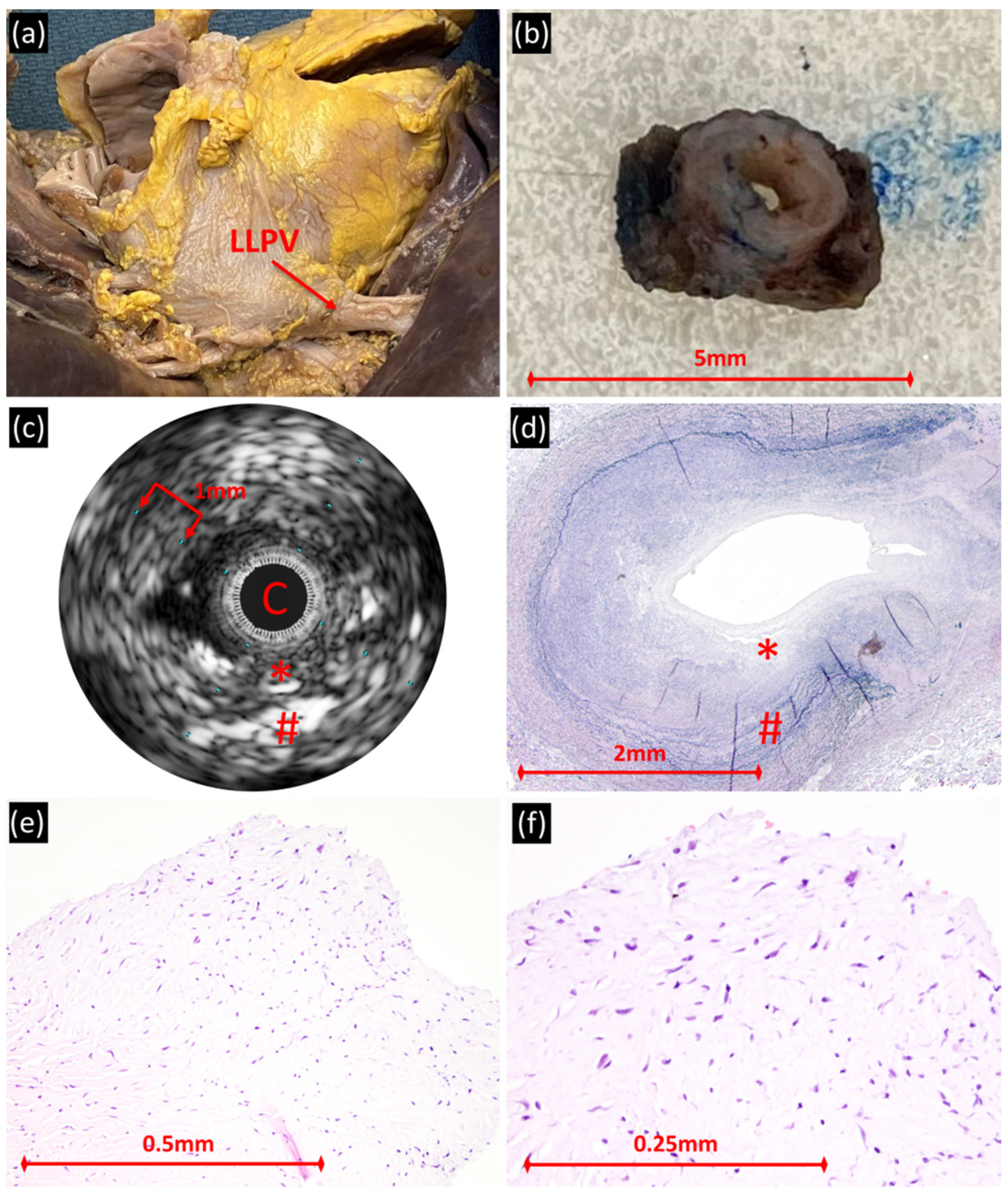
3.2.1. Postmortem PVS Veins
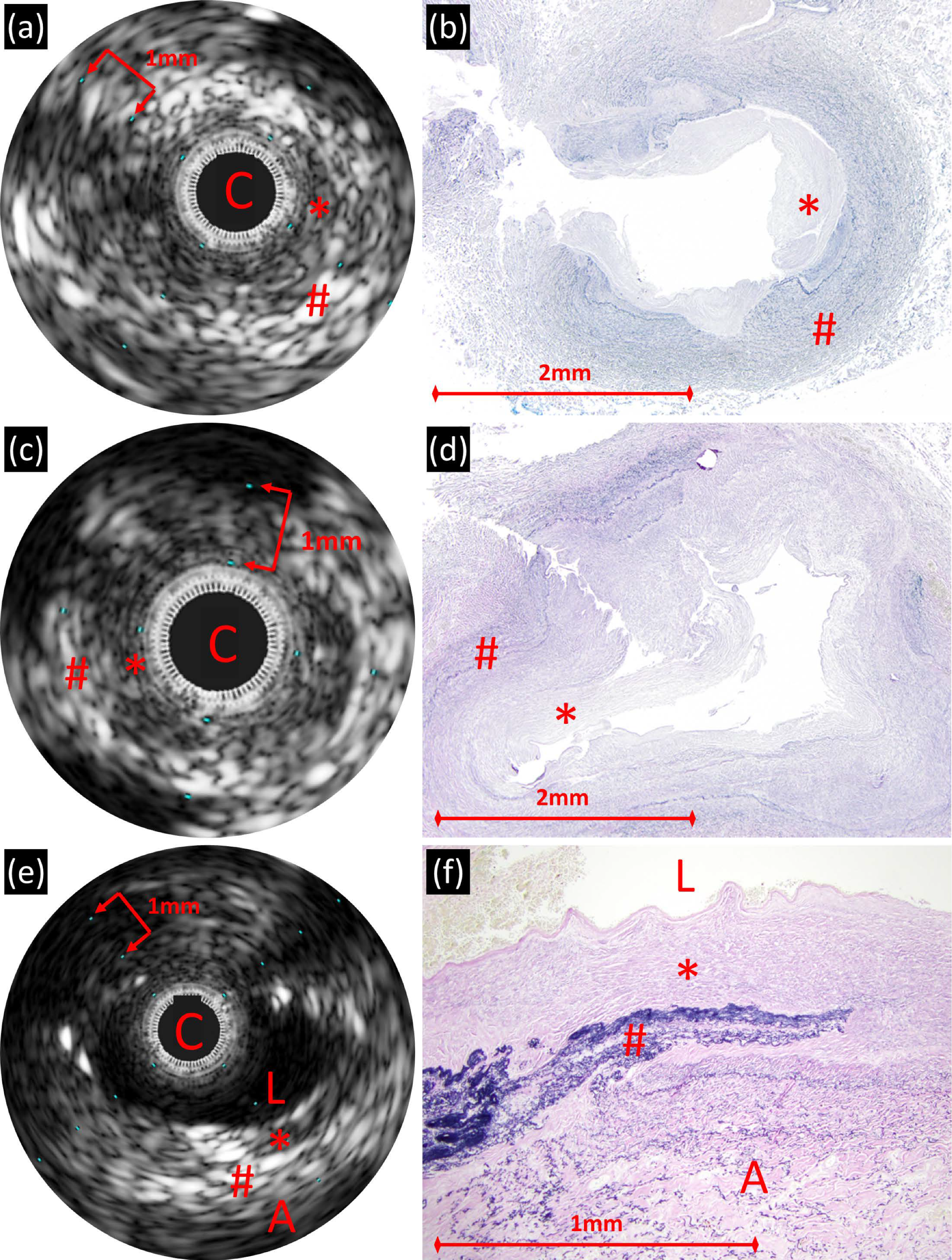
3.2.2. In Vivo PVS Veins
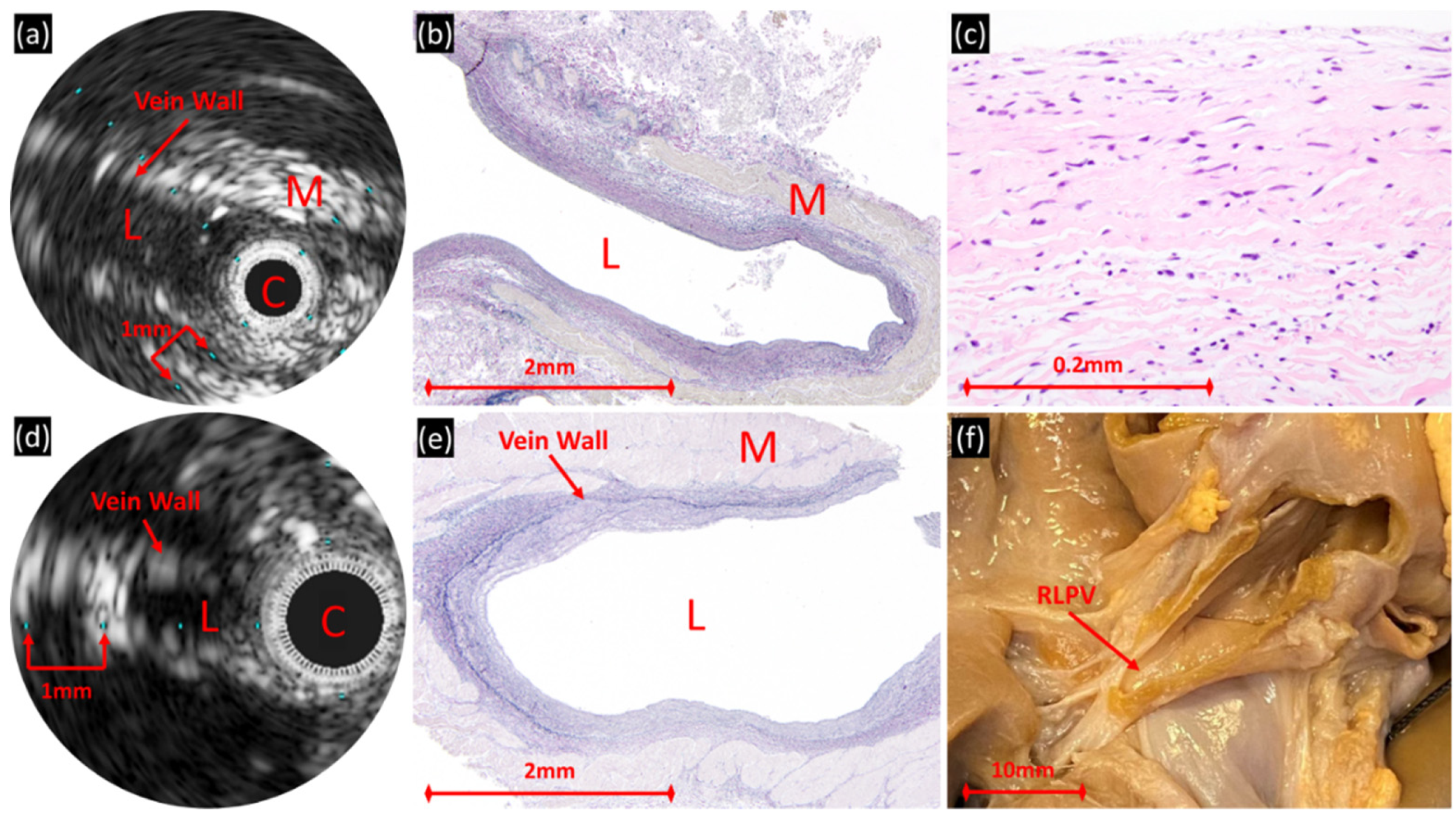
3.2.3. Control Veins
3.3. Histology
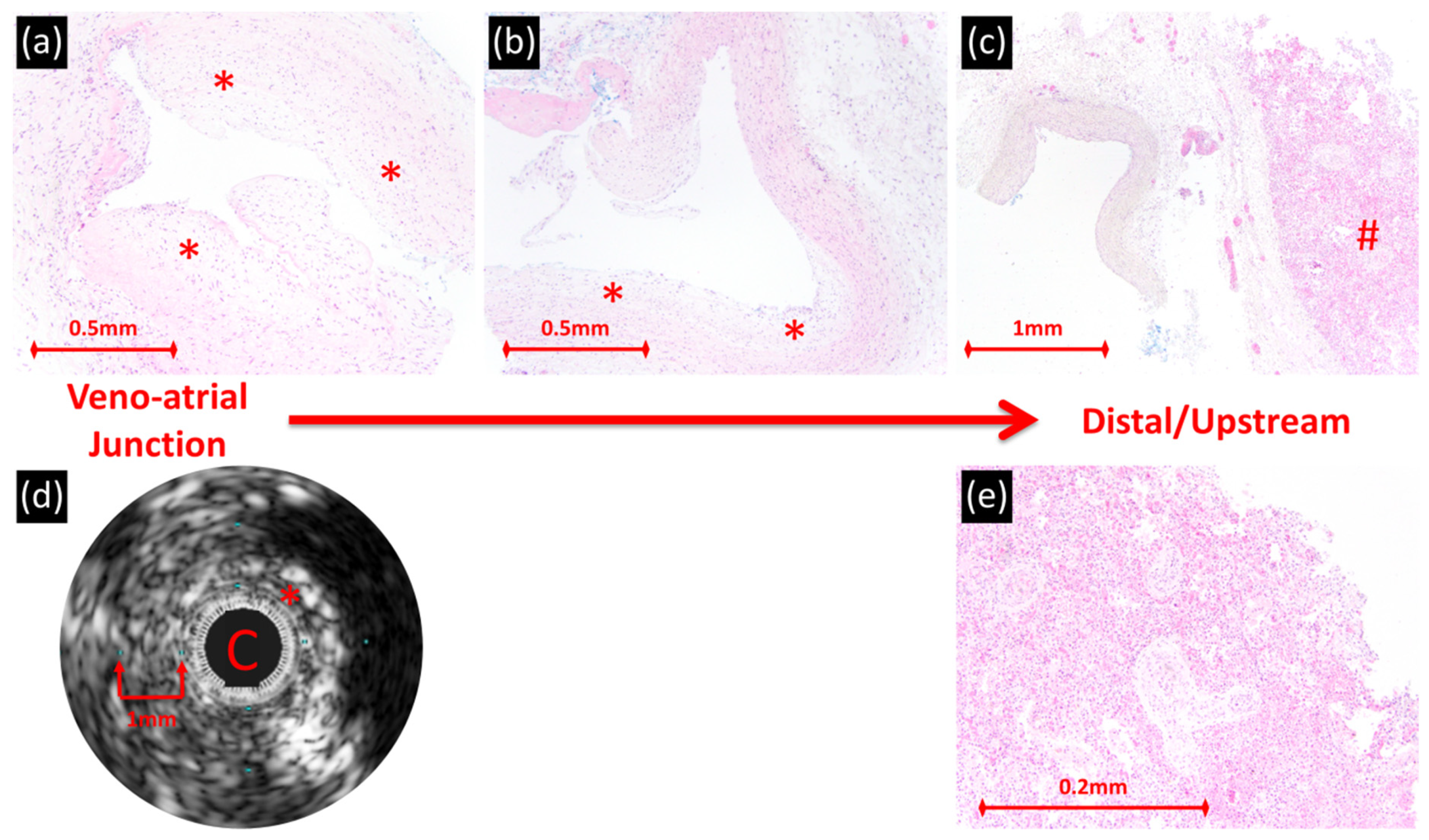
3.3.1. PVS Veins
3.3.2. Control Veins
3.4. IVUS/Histology Correlation
3.4.1. Postmortem PVS Veins
3.4.2. In Vivo PVS Veins
3.4.3. Control Veins
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sadr, I.M.; Tan, P.E.; Kieran, M.W.; Jenkins, K.J. Mechanism of pulmonary vein stenosis in infants with normally connected veins. Am. J. Cardiol. 2000, 86, 577–579. [Google Scholar] [CrossRef]
- Riedlinger, W.F.J.; Juraszek, A.L.; Jenkins, K.J.; Nugent, A.W.; Balasubramanian, S.; Calicchio, M.L.; Kieran, M.W.; Collins, T. Pulmonary vein stenosis: Expression of receptor tyrosine kinases by lesional cells. Cardiovasc. Pathol. 2006, 15, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Kovach, A.E.; Magcalas, P.M.; Ireland, C.; Mcenany, K.; Oliveira, A.M.; Kieran, M.W.; Baird, C.W.; Jenkins, K.; Vargas, S.O. Paucicellular Fibrointimal Proliferation Characterizes Pediatric Pulmonary Vein Stenosis. Am. J. Surg. Pathol. 2017, 41, 1198–1204. [Google Scholar] [CrossRef] [PubMed]
- Callahan, R.; Kieran, M.W.; Baird, C.W.; Colan, S.D.; Gauvreau, K.; Ireland, C.M.; Marshall, A.C.; Sena, L.M.; Vargas, S.O.; Jenkins, K.J. Adjunct Targeted Biologic Inhibition Agents to Treat Aggressive Multivessel Intraluminal Pediatric Pulmonary Vein Stenosis. J. Pediatr. 2018, 198, 29–35.e5. [Google Scholar] [CrossRef] [PubMed]
- Seale, A.N.; Uemura, H.; Webber, S.A.; Partridge, J.; Roughton, M.; Ho, S.Y.; McCarthy, K.P.; Jones, S.; Shaughnessy, L.; Sunnegardh, J.; et al. Total anomalous pulmonary venous connection: Outcome of postoperative pulmonary venous obstruction. J. Thorac. Cardiovasc. Surg. 2013, 145, 1255–1262. [Google Scholar] [CrossRef] [Green Version]
- Kotani, Y.; Zhu, J.; Grosse-Wortmann, L.; Honjo, O.; Coles, J.G.; Van Arsdell, G.S.; Caldarone, C.A. Anatomical risk factors, surgical treatment, and clinical outcomes of left-sided pulmonary vein obstruction in single-ventricle patients. J. Thorac. Cardiovasc. Surg. 2015, 149, 1332–1338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donnell, C.P.; Lock, J.E.; Powell, A.J.; Perry, S.B. Compression of pulmonary veins between the left atrium and the descending aorta. Am. J. Cardiol. 2003, 91, 248–251. [Google Scholar] [CrossRef]
- Peng, L.F.; Lock, J.E.; Nugent, A.W.; Jenkins, K.J.; McElhinney, D.B. Comparison of conventional and cutting balloon angioplasty for congenital and postoperative pulmonary vein stenosis in infants and young children. Catheter. Cardiovasc. Interv. 2010, 75, 1084–1090. [Google Scholar] [CrossRef] [PubMed]
- Quinonez, L.G.; Gauvreau, K.; Borisuk, M.; Ireland, C.; Marshall, A.M.; Mayer, J.E.; Jenkins, K.J.; Fynn-Thompson, F.E.; Baird, C.W. Outcomes of surgery for young children with multivessel pulmonary vein stenosis. J. Thorac. Cardiovasc. Surg. 2015, 150, 911–917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rito, M.L.; Gazzaz, T.; Wilder, T.J.; Vanderlaan, R.D.; Van Arsdell, G.S.; Honjo, O.; Yoo, S.-J.; Caldarone, C.A. Pulmonary vein stenosis: Severity and location predict survival after surgical repair. J. Thorac. Cardiovasc. Surg. 2016, 151, 657–666. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cabrera, J.A.; Sánchez-Quintana, D.; Farré, J.; Navarro, F.; Rubio, J.M.; Cabestrero, F.; Anderson, R.H.; Ho, S.Y. Ultrasonic Characterization of the Pulmonary Venous Wall. Circulation 2002, 106, 968–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guerra, P.G.; Thibault, B.; Dubuc, M.; Talajic, M.; Roy, D.; Crepeau, J.; Nattel, S.; Tardif, J.-C. Identification of atrial tissue in pulmonary veins using intravascular ultrasound. J. Am. Soc. Echocardiogr. 2003, 16, 982–987. [Google Scholar] [CrossRef]
- Gagne, P.J.; Tahara, R.W.; Fastabend, C.P.; Dzieciuchowicz, L.; Marston, W.; Vedantham, S.; Ting, W.; Iafrati, M.D. Venography versus intravascular ultrasound for diagnosing and treating iliofemoral vein obstruction. J. Vasc. Surg. Venous Lymphat. Disord. 2017, 5, 678–687. [Google Scholar] [CrossRef] [PubMed]
- Montminy, M.L.; Thomasson, J.D.; Tanaka, G.J.; Lamanilao, L.M.; Crim, W.; Raju, S. A comparison between intravascular ultrasound and venography in identifying key parameters essential for iliac vein stenting. J. Vasc. Surg. Venous Lymphat. Disord. 2019, 7, 801–807. [Google Scholar] [CrossRef] [PubMed]
- Callahan, R.; Jenkins, K.J.; Bs, Z.G.; ScD, K.G.; Porras, D. Preliminary findings on the use of intravascular ultrasound in the assessment of pediatric pulmonary vein stenosis. Catheter. Cardiovasc. Interv. 2021, 97. [Google Scholar] [CrossRef] [PubMed]
- Nasr, V.G.; Callahan, R.; Wichner, Z.; Odegard, K.C.; Dinardo, J.A. Intraluminal Pulmonary Vein Stenosis in Children. Anesthesia Analg. 2019, 129, 27–40. [Google Scholar] [CrossRef] [PubMed]
- Pogoriler, J.E.; Kulik, T.J.; Mullen, M.P.; Jenkins, K.J.; Casey, A.M.; Baird, C.W.; Vargas, S.O. Lung Pathology in Pediatric Pulmonary Vein Stenosis. Pediatr. Dev. Pathol. 2016, 19, 219–229. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Median (Range) or n (%) | |||
|---|---|---|---|
| Patient Demographics | Postmortem PVS Patients (n = 4) | In Vivo Patients (n = 4) | Control Patients (n = 3) |
| Age at Death or IVUS Catheterization (months) | 16.5 (5–21) | 16 (3–26) | 7.5 (7–8.4) |
| Postmortem or IVUS Catheterization Weight (kg) | 7 (4.2–9.6) | 8.1 (4.7–9.3) | 4.9 (3.9–7) |
| Pulmonary Vein Imaged | 5 | 7 | 3 |
| Right Upper PV | 2 (40) | 2 (29) | 2 (67) |
| Right Lower PV | 1 (20) | 1 (14) | 1 (33) |
| Left Upper PV | 0 (0) | 3 (43) | 0 (0) |
| Left Lower PV | 2 (40) | 1 (14) | 0 (0) |
| Pulmonary Vein Diagnosis | |||
| Primary | 3 (75) | 0 (0) | 0 (0) |
| Prematurity | 0 (0) | 2 (50) | 1 (33) 1 |
| Congenital Heart Disease | 1 (25) | 2 (50) | 1 (33) 2 |
| Other Diagnosis | 1 (33) 3 | ||
| Mean ± Standard Deviation or % (Range) | |||
|---|---|---|---|
| Vein Characteristics | Postmortem PVS Veins (n = 5) | In Vivo PVS Veins (n = 5) | Control Veins (n = 3) |
| Vein Diameter (mm) | 5.0 ± 1.2 | 5.1 ± 0.7 | 4.1 ± 1.1 |
| Lumen Diameter (mm) | 2.4 ± 0.8 | 3.1 ± 0.7 | 3.0 ± 0.8 |
| Wall Thickness (mm) | 1.4 ± 0.5 | 1.0 ± 0.2 | 0.5 ± 0.05 |
| Inner Layer Thickness (mm) | 0.8 ± 0.2 | 0.9 ± 0.3 | n/a |
| Outer Layer Thickness (mm) | 0.6 ± 0.6 | 0.5 ± 0.2 | n/a |
| Percent Wall Thickness (%) 1 | 52 (37–69) | 40 (32–50) | 25 (20–27) |
| Percent of Wall Thickness that is the Inner Layer (%) 2 | 60 (52–79) | 86 (69–100) | n/a |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Callahan, R.; Gauthier, Z.; Toba, S.; Sanders, S.P.; Porras, D.; Vargas, S.O. Correlation of Intravascular Ultrasound with Histology in Pediatric Pulmonary Vein Stenosis. Children 2021, 8, 193. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030193
Callahan R, Gauthier Z, Toba S, Sanders SP, Porras D, Vargas SO. Correlation of Intravascular Ultrasound with Histology in Pediatric Pulmonary Vein Stenosis. Children. 2021; 8(3):193. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030193
Chicago/Turabian StyleCallahan, Ryan, Zachary Gauthier, Shuhei Toba, Stephen P. Sanders, Diego Porras, and Sara O. Vargas. 2021. "Correlation of Intravascular Ultrasound with Histology in Pediatric Pulmonary Vein Stenosis" Children 8, no. 3: 193. https://0-doi-org.brum.beds.ac.uk/10.3390/children8030193