
Long-Term Outcomes and the Post-Intensive Care Syndrome in Critically Ill Children: A North American Perspective


1
Department of Anesthesiology, Section of Pediatric Critical Care Medicine, Wake Forest University School of Medicine, Winston-Salem, NC 27157, USA
2
Department of Pediatrics, Division of Critical Care, McMaster University, Hamilton, ON L8S 4K1, Canada
3
Department of Health Research Methods, Evidence and Impact, McMaster University, Hamilton, ON L8S 4K1, Canada
*
Author to whom correspondence should be addressed.
Children 2021, 8(4), 254; https://0-doi-org.brum.beds.ac.uk/10.3390/children8040254
Submission received: 12 February 2021
/
Revised: 17 March 2021
/
Accepted: 20 March 2021
/
Published: 24 March 2021
(This article belongs to the Special Issue Advances in Pediatric Critical Care)
Abstract
:Advances in medical and surgical care for children in the pediatric intensive care unit (PICU) have led to vast reductions in mortality, but survivors often leave with newly acquired or worsened morbidity. Emerging evidence reveals that survivors of pediatric critical illness may experience a constellation of physical, emotional, cognitive, and social impairments, collectively known as the “post-intensive care syndrome in pediatrics” (PICs-P). The spectrum of PICs-P manifestations within each domain are heterogeneous. This is attributed to the wide age and developmental diversity of children admitted to PICUs and the high prevalence of chronic complex conditions. PICs-P recovery follows variable trajectories based on numerous patient, family, and environmental factors. Those who improve tend to do so within less than a year of discharge. A small proportion, however, may actually worsen over time. There are many gaps in our current understanding of PICs-P. A unified approach to screening, preventing, and treating PICs-P-related morbidity has been hindered by disparate research methodology. Initiatives are underway to harmonize clinical and research priorities, validate new and existing epidemiologic and patient-specific tools for the prediction or monitoring of outcomes, and define research priorities for investigators interested in long-term outcomes.
1. Introduction
The first dedicated pediatric intensive care unit (PICU) was established in Europe in 1955, and pediatric intensive care has only been established as a distinct specialty since 1981 [1]. Since then, advances in the care of critically ill children have resulted in significant improvements in mortality [2,3,4,5,6]. As the vast majority of children now survive critical illness, the focus has turned to newly acquired morbidities that affect their functional abilities, health-related quality of life, and post-discharge survival [7,8,9,10,11,12,13,14]. Subsequently, our definition of a good outcome in pediatric critical care has evolved from survival, to measures of survivorship [15,16].
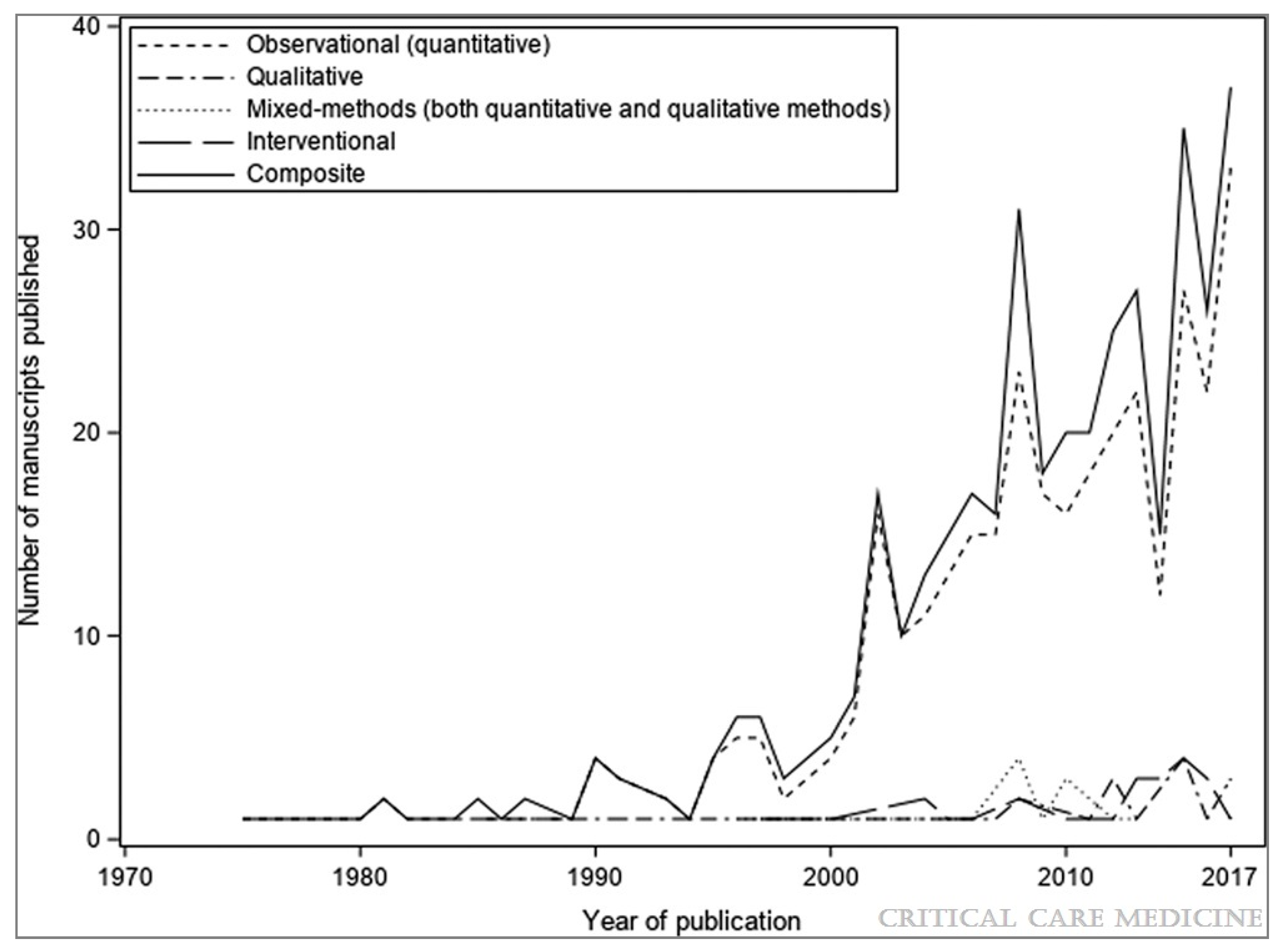
The evolving PICU landscape of rising morbidity and falling mortality has coincided with, and perhaps contributed to, an increasing proportion of critically ill children with underlying chronic conditions, and those with complex conditions who require prolonged PICU admissions [17,18,19]. Pediatric critical care research over the last 20 years has increasingly focused on understanding this evolving, diverse population and their outcomes beyond the PICU (Figure 1) [20]. This research has revealed that PICU survivors experience a constellation of post-intensive care morbidities that can significantly impact their long-term outcomes. In this narrative review, we describe the epidemiology of the post-intensive care syndrome in pediatrics (PICs-P), risk factors, and management strategies, how PICs affect caregivers and families, and long-term outcomes. We identify related research priorities including ongoing efforts to derive an internationally relevant core-outcome set for clinical research in the field of pediatric critical care.
2. Post-Intensive Care Syndrome in Pediatrics
In 2010, stakeholder meetings were held in North America with representatives from key professional organizations and groups, aiming to better define and address the lasting impairments experienced by adult intensive care unit (ICU) survivors [21]. One of the initial goals of these meetings was to establish a common nomenclature describing post-ICU morbidity to facilitate future collaboration, research, and education. It was recognized that many ICU survivors experienced co-morbidities affecting physical, cognitive, and psychiatric domains. This phenomenon was coined the “post-intensive care syndrome” (PICs) to identify the presence of one or more of these ICU-acquired sequelae [21]. The effect of intensive care hospitalization on family members was also recognized. The term “PICs-Family” emerged to recognize psychiatric sequelae such as post-traumatic stress disorder in relatives and caregivers [22].
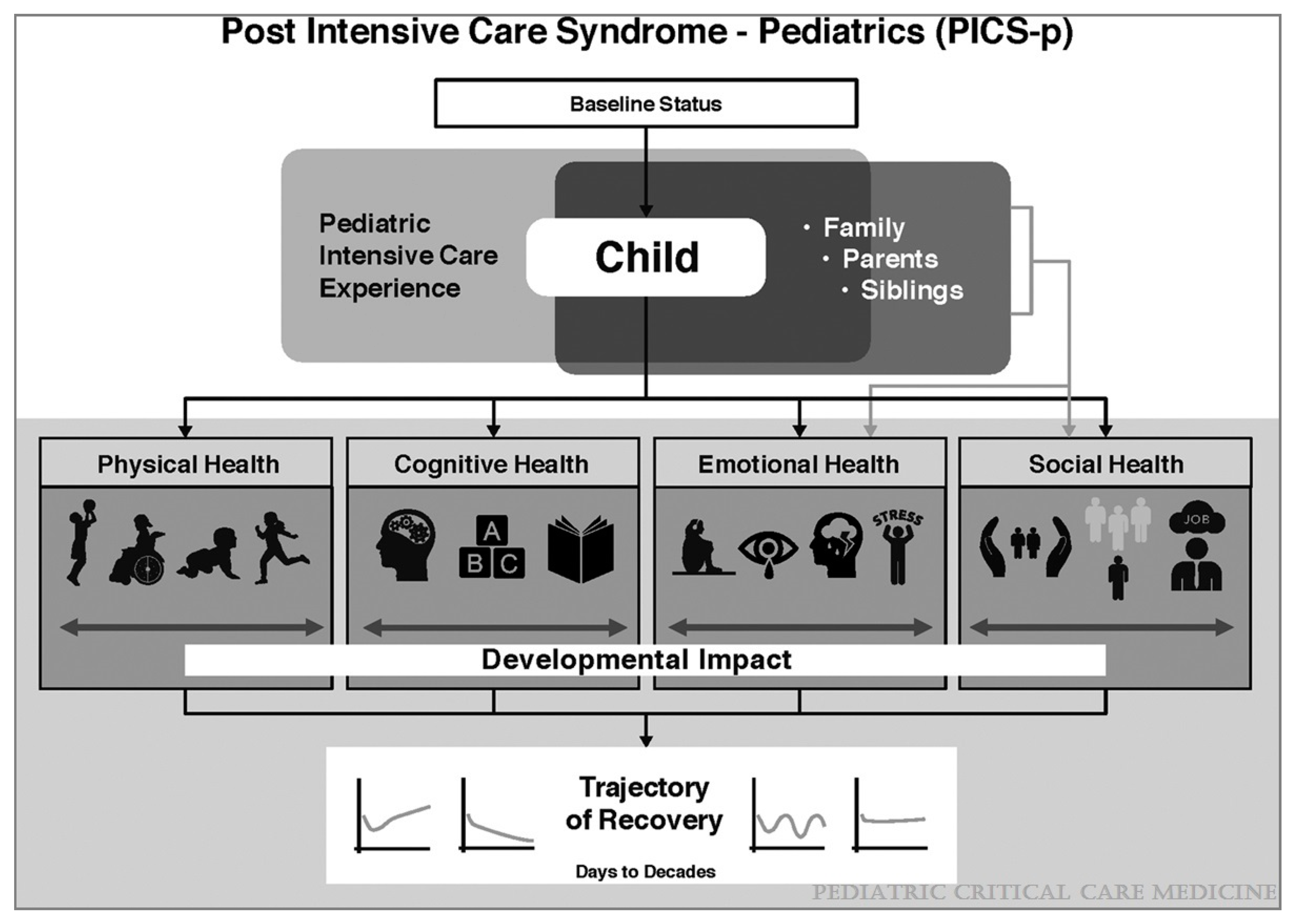
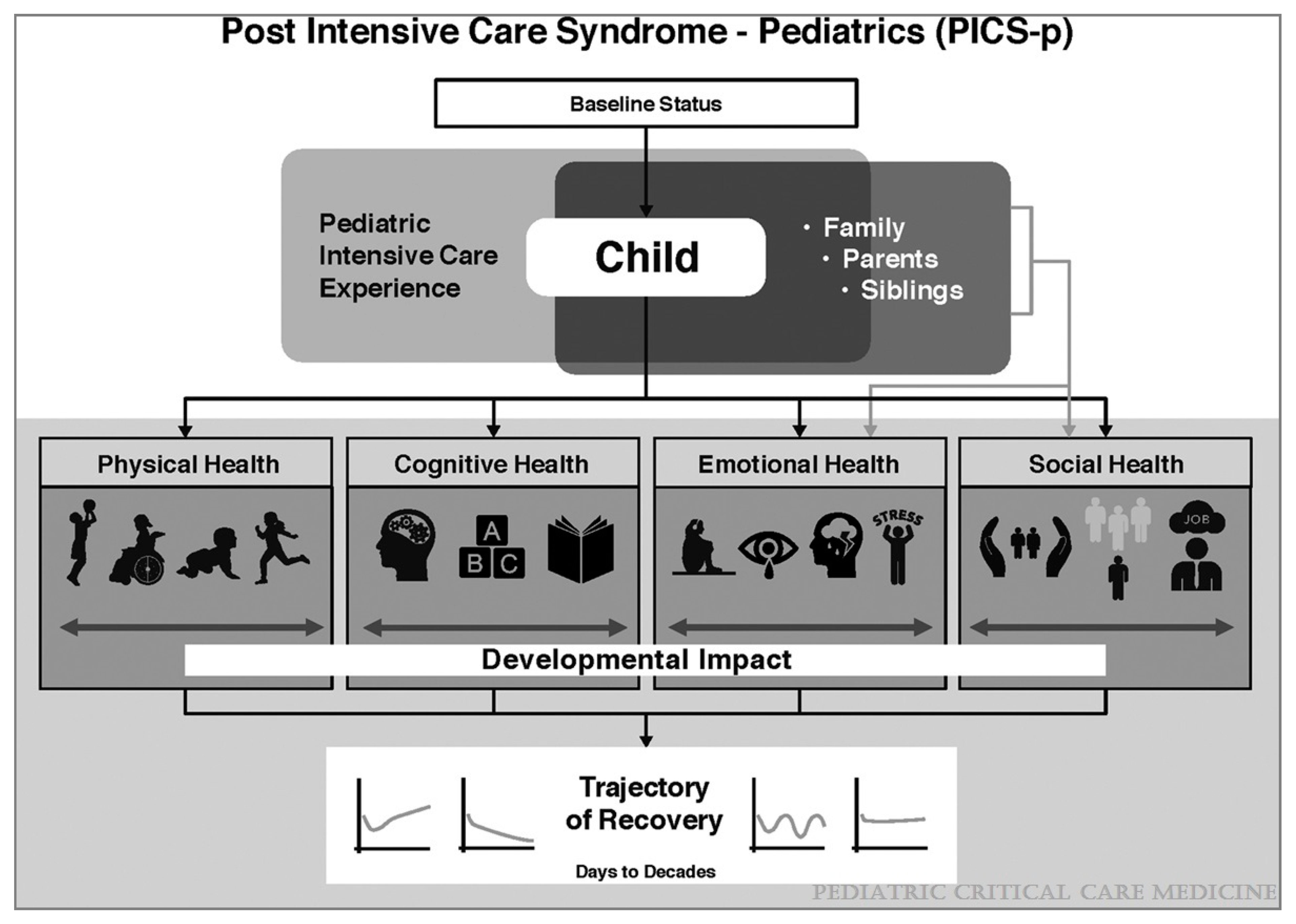
To address emerging evidence of post-PICU morbidity in children, Manning et al. adapted the PICs conceptual framework to pediatrics (PICs-P) (Figure 2) [23]. The pediatric model differs from that in adults in a number of ways. Residual morbidity in children following critical illness can affect four health domains: physical, cognitive, emotional, and social (examples in Table 1). These domains are influenced by the interplay of the child’s pre-morbid baseline status, the pediatric intensive care experience, and the caregiver or family unit. The social domain was added based on evidence that critical illness affects children’s post-discharge social functioning [24,25,26]. PICs may manifest differently in children due to dynamic states of growth and development, and the presence of pre-existing complex or chronic conditions. Critically ill children may therefore experience more heterogeneous trajectories of recovery than what is seen in adults [27,28].
3. Physical Manifestations
One of the earliest aspects of adult PICs described in the modern cannon of medicine was critical illness associated polyneuromyopathy, or “ICU-acquired weakness” [29,30,31,32]. ICU-acquired weakness is extremely challenging to ascertain in children and likely under-recognized [33]. Furthermore, weakness is not only a reflection of muscle function or power but is inextricably linked to neurologic function, pain, heart function, and lung function [28,34,35,36]. “Functional status” or “functional outcomes” are thus a more patient-centered means of conceptualizing the physical health domain than mobility or strength alone. Physical functioning assessments are now commonly measured as a part of multidimensional scales of movement, activity, endurance, abilities, and health-related quality of life [37]. This is of particular importance in a developmentally heterogeneous PICU population. Functional outcome has not only important implications for the patient, but for resource utilization [38]. Functional morbidity is associated with increased critical care resource utilization and prolonged length of hospital stay [35,39,40]. Poor functional outcomes at discharge, including technology dependence and complex chronic conditions, increase the risk of unplanned readmission and post-discharge mortality [41,42,43].
Functional sequelae following critical illness are widely dependent on the developmental stage and baseline function of the patient in question [36]. For infants or children with severe neuromuscular problems at baseline, movement may be very poor, and more salient indicators of overall function may be a decline in respiratory status ranging from subjective dyspnea or difficulty with secretion clearance to the need for positive pressure ventilation. Similarly, feeding issues might arise ranging from normal intake to mild dysphagia to dependence on parenteral nutrition. This wide variety of problems composing functional outcomes is apparent in newer tools used to measure them [44].
The prevalence of physical functional decline after critical illness is variable depending on the methods of and timing of assessment [12,34,40]. Functional status decline is reported in 4.6–10.3% of children at PICU discharge when assessed by objective, provider-completed instruments [34,35,45,46,47]. Interestingly, when disability inventories were completed by parents and caregivers at discharge, a striking 81.5% of children were identified as having had functional decline compared with their baseline prior to intensive care [40]. This finding suggests that parent perception of disability may be higher than what is uncovered with brief clinician-applied scoring tools. Functional recovery trajectories in children with acquired disability vary according to study and methods of functional assessment. Choong et al. found that approximately two-thirds of affected children demonstrated some functional recovery by 6 months post-PICU discharge [40]. In a large clinical trial population followed for a median of 4 years, 56% demonstrated functional improvement, with nearly 82% recovered to baseline function or mild dysfunction from baseline [12,36]. Conversely, some studies have shown accumulation of disability over time [47,48]. Telephone follow-up with patients consecutively admitted to a PICU demonstrated that functional morbidity continued to accumulate over a 3-year follow-up period, increasing from 5.2% to 10.4% of patients [35]. Subpopulations can have much higher rates of functional decline. In sepsis and traumatic brain injury survivors, 34% and 51% had functional decline, respectively [49,50]. However, both groups showed favorable recovery in 47% and 95% of patients, respectively, after 1 year [51,52]. Despite longer median lengths of stay in the PICU and more preceding medical complexity, children with preceding feeding or respiratory technology dependence have similar likelihood of functional decline to their less medically complex peers, 4.5 vs. 4.6% [53].
4. Cognitive Manifestations
Cognitive manifestations following critical illness include deficits in attention, memory, or processing speed. The true prevalence of cognitive decline following critical illness in children is challenging, as baseline neurocognitive testing is often not available nor feasible [20]. Assessments are often by basic objective scoring, caregiver recall, teacher survey, or the use of age-matched controls [54,55,56,57], and hence, measurement of cognitive decline may be prone to recall bias [46,58]. Non-verbal children and those with neurocognitive disabilities present additional challenges and are under-represented in the existing literature [59].
Based on United States database data, the overall rate of newly acquired cognitive disability following critical illness is 3.4% [46]. A recent systematic review covering cognitive outcomes in critically ill children reports considerable heterogeneity [59]. Subpopulations at highest risk are children with sepsis and meningitis, with 22.5–42% reported as having cognitive or neurodevelopmental delays following their illness [59]; among children with post-cardiac extracorporeal membrane oxygenation (ECMO), 46.8% are reported as having learning difficulties and 29.2% requiring some form of special education [55], and 24% of young children surviving extracorporeal cardiopulmonary resuscitation (E-CPR) have intellectual disability [60].
Longer-term follow-up of cognitive outcomes in children following PICU admission has demonstrated concerning findings that these deficits may persist. In children demonstrating neurocognitive impairment at 3–6 months, deficits were found to persist at 12-month follow-up [61]. Neurocognitive follow-up in pediatric survivors of meningococcal sepsis treated from 1988 to 2001 at a median 13 years following index intensive care admission demonstrated that measured intelligence quotient was comparable to the general population but had lower scores on verbal and numerical fluency subtests with effect sizes of 10–20% [57]. The effects of these cognitive changes on school performance, educational attainment, and health-related quality of life are unknown, and additional studies are needed. The importance of even minor cognitive decline should not be overlooked as it is thought to be one of the most salient factors determining health-related quality of life in PICU survivors [62].
5. Emotional and Psychological Manifestations
Emotional sequelae of PICs-P can manifest as mood, psychological, or psychiatric disorders acquired during ICU hospitalization that persist following discharge [24]. The majority of existing literature on emotional health has focused on school-aged children due to available diagnostic and reporting tools [63]. Therefore, a significant proportion of emotional morbidity might be missed in younger children. Specific mental health diagnoses, such as post-traumatic stress disorder (PTSD), depression [64,65], changes in self-esteem, delusional memories or fears, and sleep disturbances, have been reported in children following PICU discharge [64,65,66,67,68,69].
PTSD is particularly common amongst critically ill children [70]. As many as 84.6% of PICU survivors compared to 6.2% of ward survivors met criteria for probable PTSD or actual Diagnosis and Statistics Manual of Mental Disorders 5th edition (DSM5) criteria, according to an Egyptian study [71], while other studies report that 13–32% of children screen positive for PTSD within a year of discharge [27,72]. PTSD symptoms are thought to improve over time [72]. However, Colville et al. observed higher trauma scale scores at 12 months compared to 3 months in 40% of children. This suggests that for some children, peak symptom severity may not be captured with short follow-up periods [27].
Additional post-PICU psychiatric morbidities include hyperactivity or conduct issues, which have been reported to affect up to 20% [61]. Depressive symptoms are also common, with 83.1% of children self-identified as having symptoms of depression [71]. Sleep disturbances have been reported in up to 80% of PICU survivors, and 38% are at risk for fatigue disorder [61]. Cognitive fatigue, a term differentiating poor sustained attention and motivation, is significantly higher in PICU survivors compared to age-matched controls [73].
The impact of emotional decline following PICU is not yet fully understood. Nevertheless, early recognition and referral of PICU patients who are high-risk for adverse emotional outcomes, particularly those with high levels of medical traumatic stress, may improve outcomes including health-related quality of life [15,25,74,75,76]. The downstream effects of adverse emotional outcomes on trajectory of PICs-P recovery have not been well elucidated, but there is evidence to suggest that more children with psychiatric morbidity after discharge are re-admitted with physical complaints in the following 6-12 months [70].
6. Social Manifestations and PICs-Family
As their main social support, PICs affect not just the patient, but also the family. In turn, family wellbeing and functioning can significantly impact child outcomes. Issues ranging from social isolation of children to parental stress and loss of employment are all critical outcomes that may be predictive of the child’s recovery [24]. Qualitative studies in PICU survivors have shown themes related to living disrupted lives, experiencing social stigma, and having to rebuild social identities, particularly in older children [26,66]. Similarly, recent qualitative studies of parents of children who experienced critical illness identified themes related to prolonged adjustment periods following intensive care where they get used to a “new normal” [77,78,79]. The breadth of issues is reflected in the diversity and depth of literature on this topic. A recent scoping review on post-discharge outcomes in children found more studies related to social outcomes than any other PICs domain [20].
School attendance is an important objective measure of the impact of pediatric critical illness on a child’s social health [80]. Kastner et al. noted that among children admitted to an urban PICU, 43% of children followed up at 3 months had missed 7 or more days of school and 14% had missed more than 30 days of school [81]. The implementation of educational supports was also inadequate, with over half of absentee children not receiving homebound services and over a quarter having falling grades post-PICU. Chronic critical illness likely only exacerbates school absenteeism and social isolation [82,83].
Parental psychological health is closely linked to their child’s psychosocial wellbeing and their ability to support their child’s recovery [72,75]. In total, 21% of parents experience moderate to severe anxiety, and 9% reported moderate–severe depression [84]. Parent medical traumatic stress outcomes following pediatric critical illness are not uncommon [42], occurring in the range of 10.5% to 21% [85]. A study in the United States revealed that 9.5% received a new mental health diagnosis in the 6 months following their child’s PICU hospitalization, a 110% increase from the baseline rate of mental health diagnoses in this group prior their child’s PICU admission [86].
Studies assessing children’s peer relationships are notably lacking in the literature. Similarly, social determinates of health such as parental age, employment status, educational attainment, food and housing security, and support networks are known as predictors of parental resilience but have not been studied themselves as outcomes [84,87,88].
7. Patient Centered Outcomes in PICs-P
Outcomes research in the PICU has historically focused on clinician-important measures, tending to focus on short-term physiologic or laboratory markers [89]. In recent years, PICU research has increasingly focused on patient-centered outcomes, which require longer follow-up and prioritize measures that incorporate patient or family perceptions of wellness [8,90,91].
Health-related quality of life (HRQoL) is a uniquely patient-centered outcome and does not fall easily into any one PICs domains but rather spans them all. High-quality measures of HRQoL in children contain subscores for the physical, emotional, or social wellbeing of a child. Certain measures have also been validated for children with chronic complex disease with additional normative data and may therefore be highly useful in measuring outcomes across diverse PICU populations [90].
In consecutively admitted PICU patients tested following discharge, global scores on HRQoL measures have been very low [75,92]. Key determinates of poor HRQoL in children post-PICU include diagnoses such as sepsis, meningitis, trauma, and antecedent chronic comorbidities [49,54,93,94,95]. Treatments including prolonged cardiopulmonary resuscitation, prolonged length of stay, and use of invasive technology may also decrease post-discharge HRQoL [15,96,97]. However, longer-term follow-up has been more reassuring, showing that HRQoL generally improves after discharge for up to a year and in many children may recover to a point where children with histories of critical illness are not easily discernable from their healthy peers [25].
However, to date, there remains little uniformity in the specific measures used to assess PICU outcomes. A recent scoping review of the literature from 1970 to 2017 describes an exceptionally high number of instruments available for testing [20]. The unique article to unique measurement ratio reported in this review was 1.11, suggesting that, taken on average, for nearly every publication on this area, a new instrument was used. Consensus on ideal measures in each domain does not exist, but efforts to do so are underway. Fink et al. have initiated an effort to provide a core outcomes set which will direct clinicians and researchers to a smaller number of ideal tools that will screen for risk factors and measure outcomes which are important to patients and clinicians [98,99]. These efforts will improve the ability to measure outcomes of survivorship in a more cohesive manner.
8. Screening and Identification of At-Risk Patients
Evidence on potential risk factors for adverse long-term outcomes and PICs-P has only recently begun to emerge. Numerous interacting and collinear illness severity variables appear predictive of poor outcomes in all domains [56]. Severity of illness has been demonstrated in multiple studies to mediate the risk of all PICs domains [40,46,49]. Similarly, studies have recently described the use of objective organ dysfunction scoring to accurately predict trichotomous outcomes of mortality, survival with morbidity, and survival without new morbidity [100,101]. Perhaps counterintuitively, children with preceding chronic complex comorbid disease may have similar decline in function to previously healthy children or even be more likely to return to their pre-ICU baseline [40,53,102]. However, these children have high rates of PICU readmission, and the cumulative impact of recurrent or chronic critical illness is not well described [43]. Intensive care providers should therefore consider additional testing of patients with high severity of disease and chronic complex comorbid disease.
Screening patients for PICU-related iatrogenic and environmental risk factors is also important, as evidence suggests that these are independent predictors of poor post-PICU outcomes [40,103]. Excessive sedation, inadequate pain control, delirium, and immobility are classic risk factors associated with poor outcomes in adult ICU patients [104]. However, these factors can be difficult to disentangle from disease-related risks, since the intensity and duration of these therapies is related to disease severity and need for mechanical support [105]. Duration of sedation, use of certain opioid medications, and presence of withdrawal symptoms may be associated with worse functional and neuropsychiatric outcomes [47,106]. Despite strong evidence in the adult literature showing delirium as a risk factor for cognitive decline, the pediatric literature has yet to show a strong association of delirium with cognitive decline [107,108]. However, there appears to be a weak association of delirium with functional decline [47,103]. A prospective randomized trial of early vs. late parenteral nutrition (PN) in the PICU demonstrated that the use of PN in the first week of admission may contribute to limited, adverse neurocognitive outcomes at 2 years follow-up and adverse emotional and behavioral outcomes at 4 years follow-up [109,110]. Other treatments, such as glycemic control, do not appear to modify risk [111].
Demographic and social factors are also thought to mediate risk. A recent modified Delphi consensus of PICU and pediatric palliative care providers identified a number of candidate risk factors for adverse psychosocial outcomes following pediatric critical illness. The panel identified demographic factors including young caregivers and caregiver language barriers as highly predictive of poor outcome. Consensus was also reached regarding the importance of a variety of social determinates including the presence of social supports, involvement of child protective services, transportation challenges, and caregiver intellectual disability. Clinical factors considered most important were new technology or tracheostomy dependence and recurrent hospitalizations over the past year [88]. This may also negatively impact caregivers who are taking on a new, higher level of caregiver burden [112].
Our understanding of the epidemiology and risk factors of PICs-P remains nascent. Improved screening tests are needed to help to identify children at highest risk. Long-term follow-up of patients by PICU teams is rare, and the use of multidisciplinary follow-up programs, even more so [113]. Until better screening tools exist to reliably identify high risk patients, providers should have a low threshold for referral to available outpatient therapy and psychology.
9. Management and Prevention of PICs-P
Prioritization of reversal of organ dysfunction and survival is of foundational importance in critical care but cannot be viewed in isolation if one is to take a holistic view of patient outcomes [114]. Recognizing the potential role of iatrogenic harm in contributing to post-intensive care morbidities across PICs domains, care bundles have been proposed to mitigate the risks that accompany life-saving treatments. The most widely accepted in recent years has been the ABCDEF bundle [115].
The ABCDEF bundle is a harm-reduction tool initially used in adults to promote ICU liberation and limit chronic morbidity ([116]. This bundle of interventions includes assessing, preventing, and managing pain, both spontaneous breathing and awakening trials, choice of analgesia and sedation, assessing preventing and managing delirium, early mobility and exercise, and family engagement and empowerment. In adults, implementation of this bundle has reduced early mortality, duration of mechanical ventilation, duration of coma, incidence of delirium, physical restraint use, ICU readmission, and has increased the percentage of patients that return to their home versus chronic treatment facilities [116]. In pediatrics, evidence for this bundle is accumulating, and several recent and ongoing studies evaluating early mobilization, delirium prevention, and sedation protocols reveal promising results [117,118]. This and other research evidence has prompted emerging practice recommendations for the routine assessment of pain, sedation, withdrawal, and delirium in the PICU [119,120].
Other promising interventions that have shown benefits in adults and are planned for study in children include the use of “PICU Diaries” [121]. This intervention involves partnering with families to provide a lay narrative, comprising daily entries, drawings, and/or photographs about their child’s condition and care while in the ICU [122]. Diaries fill in memory gaps, provide a means for coherent recall of events, and may help children to make meaning out of their experience. In adults, ICU diaries have been shown to improve HRQoL and decrease PTSD, anxiety, and depression following critical illness recovery [123]. New data show the feasibility and acceptance of this intervention among families of critically ill children, and it is ripe for further study [121,122].
Multidisciplinary follow-up clinics have been proposed as a way of testing for PICU-acquired morbidities and providing comprehensive support and intervention to high-risk patients. Ongoing support after PICU and hospital discharge has been shown to be an important protective factor in prevention of psychiatric morbidity of parents and children [76]. Parents of critically ill children have indicated support for such clinics; however, when given the opportunity, only 37% choose to attend [124]. Early efforts to provide outpatient follow-up after pediatric intensive care were collaborations between pediatric neurology and pediatric intensivists caring for neurocritical care survivors [125]. These clinics have expanded to include neuropsychiatric professionals and allied health professional support [124,126]. Currently, a minority of PICUs have these types of clinics [127]. Inadequate data exist to recommend specific timing, frequency, or specialty mix of these clinics, and the limited data available have yet to show effectiveness as an intervention [124]. Additional research is needed to understand whether such care provides any significant protection or improved recovery for PICU-acquired co-morbidity.
10. Research Priorities
The need to better understand patient-centered outcomes and PICs-P has led researchers to prioritize how to best measure outcomes in critically ill children. PICU core outcome set (COS) investigators, in conjunction with the Pediatric Acute Lung Injury And Sepsis Investigators (PALISI) Network and the Collaborative Pediatric Critical Care Network (CPCCRN), are currently working with clinical and family stakeholders to determine ideal outcomes and associated measurement tools to evaluate PICU and long-term outcomes of children and their families [98,99]. The resulting core outcomes set and measures will serve as a guideline and resource for clinicians and potentially family caregivers and patients to track their own recovery. Researchers can also draw on ideal outcome tools to assess the efficacy of interventions targeted at optimizing PICU and long-term functional and HRQoL outcomes.
Ongoing research targeted at early rehabilitation and reducing PICU-acquired morbidities will provide increasing evidence on the efficacy of these interventions on clinical, patient-centered, as well as process of care outcomes, and how best to implement these multi-prong bundles in the PICU setting [128,129,130].
Discovery of means for improved patient retention including the use of multidisciplinary ICU follow-up clinics and other forms of post-discharge family support are critical to improving the retention of patients and validity of findings in outcomes research. As in any field, data sharing and outcomes registries will be an important component of retrospective analysis. Additionally, the continued funding of studies with aims related to long-term outcomes in large PICU trials will add to our detailed understanding of specific interventions and populations.
11. Conclusions
The post-intensive care syndrome in pediatrics is marked by poor outcomes across multiple domains of health, functioning and HRQoL. Pediatric intensivist, acute care clinicians, outpatient physicians, and allied health professionals should be increasingly aware of critical illness sequelae and how they affect both patient and family. Clinicians need to be able to identify patients at risk early in their critical illness course and minimize the risk of PICU-acquired complications and institute early rehabilitation. Ward clinicians, subspecialists, rehabilitation specialists, and outpatient primary care physicians should be educated on how best to screen for PICs-p symptoms and ensure adequate ongoing rehabilitation and follow-up to optimize long-term outcomes and recovery.
The current legacy of pediatric critical care is one of great historical success in improving survival. The future of pediatric critical care is one of great promise of improving survivorship. Pediatric intensivists are looking toward a future where an increased understanding of outcomes epidemiology, risk factors, and interventions leads to reduction in PICs-P frequency and severity.
Author Contributions
A.G.W. and K.C. both share responsibility for manuscript preparation, editing, and submission. Both authors have read and agreed to the published version of the manuscript.
Funding
No relevant funding.
Conflicts of Interest
The authors have no conflict of interest relevant to this work.
Abbreviations/Acronyms
| ABCDEF | Bundle of Care to improve ICU outcomes further defined in text |
| COS | Core Outcome Set |
| CPCCRN | Collaborative Pediatric Critical Care Research Network |
| DSM5 | Diagnostics and Statistics Manual 5th Edition |
| ECMO | Extracorporeal Membrane Oxygenation |
| E-CPR | Extracorporeal Cardiopulmonary Resuscitation |
| HRQoL | Health-Related Quality of Life |
| ICU | Intensive Care Unit |
| PALISI | Pediatric Acute Lung Injury and Sepsis Investigators Network |
| PICs | Post-intensive Care Syndrome |
| PICs-P | Post-intensive Care Syndrome in Pediatrics |
| PICU | Pediatric Intensive Care Unit |
| PTSD | Post-traumatic Stress Disorder |
| PN | Parenteral Nutrition |
References
- Epstein, D.; Brill, J.E. A history of pediatric critical care medicine. Pediatr. Res. 2005, 58, 987–996. [Google Scholar] [CrossRef] [Green Version]
- Wilkinson, J.D.; Pollack, M.M.; Ruttimann, U.E.; Glass, N.L.; Yeh, T.S. Outcome of pediatric patients with multiple organ system failure. Crit. Care Med. 1986, 14, 271–274. [Google Scholar] [CrossRef]
- Pollack, M.M.; Ruttimann, U.E.; Getson, P.R. Accurate prediction of the outcome of pediatric intensive care. A new quantitative method. N. Engl. J. Med. 1987, 316, 134–139. [Google Scholar] [CrossRef]
- Stoll, B.J.; Holman, R.C.; Schuchat, A. Decline in sepsis-associated neonatal and infant deaths in the United States, 1979 through 1994. Pediatrics 1998, 102, e18. [Google Scholar] [CrossRef] [Green Version]
- Namachivayam, P.; Shann, F.; Shekerdemian, L.; Taylor, A.; van Sloten, I.; Delzoppo, C.; Daffey, C.; Butt, W. Three decades of pediatric intensive care: Who was admitted, what happened in intensive care, and what happened afterward. Pediatr. Crit. Care Med. 2010, 11, 549–555. [Google Scholar] [CrossRef]
- Tan, B.; Wong, J.J.; Sultana, R.; Koh, J.; Jit, M.; Mok, Y.H.; Lee, J.H. Global Case-Fatality Rates in Pediatric Severe Sepsis and Septic Shock: A Systematic Review and Meta-analysis. JAMA Pediatr. 2019, 173, 352–362. [Google Scholar] [CrossRef]
- Watson, R.S.; Crow, S.S.; Hartman, M.E.; Lacroix, J.; Odetola, F.O. Epidemiology and Outcomes of Pediatric Multiple Organ Dysfunction Syndrome. Pediatr. Crit. Care Med. 2017, 18, S4–S16. [Google Scholar] [CrossRef] [Green Version]
- Merritt, C.; Menon, K.; Agus, M.S.D.; Choong, K.; McNally, D.; O’Hearn, K.; Watson, R.S.; Wong, H.R.; Duffett, M.; Wypij, D.; et al. Beyond Survival: Pediatric Critical Care Interventional Trial Outcome Measure Preferences of Families and Healthcare Professionals. Pediatr. Crit. Care Med. 2018, 19, e105–e111. [Google Scholar] [CrossRef]
- Pollack, M.M.; Holubkov, R.; Funai, T.; Dean, J.M.; Berger, J.T.; Wessel, D.L.; Meert, K.; Berg, R.A.; Newth, C.J.; Harrison, R.E.; et al. The Pediatric Risk of Mortality Score: Update 2015. Pediatr. Crit. Care Med. 2016, 17, 2–9. [Google Scholar] [CrossRef] [Green Version]
- Wolfler, A.; Osello, R.; Gualino, J.; Calderini, E.; Vigna, G.; Santuz, P.; Amigoni, A.; Savron, F.; Caramelli, F.; Rossetti, E.; et al. The Importance of Mortality Risk Assessment: Validation of the Pediatric Index of Mortality 3 Score. Pediatr. Crit. Care Med. 2016, 17, 251–256. [Google Scholar] [CrossRef]
- Burns, J.P.; Sellers, D.E.; Meyer, E.C.; Lewis-Newby, M.; Truog, R.D. Epidemiology of death in the PICU at five U.S. teaching hospitals*. Crit. Care Med. 2014, 42, 2101–2108. [Google Scholar] [CrossRef] [Green Version]
- Pollack, M.M.; Holubkov, R.; Funai, T.; Clark, A.; Berger, J.T.; Meert, K.; Newth, C.J.; Shanley, T.; Moler, F.; Carcillo, J.; et al. Pediatric intensive care outcomes: Development of new morbidities during pediatric critical care. Pediatr. Crit. Care Med. 2014, 15, 821–827. [Google Scholar] [CrossRef] [PubMed]
- Traube, C.; Silver, G.; Gerber, L.M.; Kaur, S.; Mauer, E.A.; Kerson, A.; Joyce, C.; Greenwald, B.M. Delirium and Mortality in Critically Ill Children: Epidemiology and Outcomes of Pediatric Delirium. Crit. Care Med. 2017, 45, 891–898. [Google Scholar] [CrossRef] [PubMed]
- Creten, C.; Van Der Zwaan, S.; Blankespoor, R.J.; Leroy, P.L.; Schieveld, J.N. Pediatric delirium in the pediatric intensive care unit: A systematic review and an update on key issues and research questions. Minerva Anestesiol. 2011, 77, 1099–1107. [Google Scholar]
- Aspesberro, F.; Mangione-Smith, R.; Zimmerman, J.J. Health-related quality of life following pediatric critical illness. Intensive Care Med. 2015, 41, 1235–1246. [Google Scholar] [CrossRef]
- Rennick, J.E.; Childerhose, J.E. Redefining success in the PICU: New patient populations shift targets of care. Pediatrics 2015, 135, e289–e291. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanthimathinathan, H.K.; Plunkett, A.; Scholefield, B.R.; Pearson, G.A.; Morris, K.P. Trends in long-stay admissions to a UK paediatric intensive care unit. Arch. Dis. Child. 2020, 105, 558–562. [Google Scholar] [CrossRef]
- Odetola, F.O.; Gebremariam, A.; Davis, M.M. Comorbid illnesses among critically ill hospitalized children: Impact on hospital resource use and mortality, 1997–2006. Pediatr. Crit. Care Med. 2010, 11, 457–463. [Google Scholar] [CrossRef]
- Edwards, J.D.; Houtrow, A.J.; Vasilevskis, E.E.; Rehm, R.S.; Markovitz, B.P.; Graham, R.J.; Dudley, R.A. Chronic conditions among children admitted to U.S. pediatric intensive care units: Their prevalence and impact on risk for mortality and prolonged length of stay*. Crit. Care Med. 2012, 40, 2196–2203. [Google Scholar] [CrossRef] [Green Version]
- Maddux, A.B.; Pinto, N.; Fink, E.L.; Hartman, M.E.; Nett, S.; Biagas, K.; Killien, E.Y.; Dervan, L.A.; Christie, L.M.; Luckett, P.M.; et al. Postdischarge Outcome Domains in Pediatric Critical Care and the Instruments Used to Evaluate Them: A Scoping Review. Crit. Care Med. 2020, 48, e1313–e1321. [Google Scholar] [CrossRef]
- Needham, D.M.; Davidson, J.; Cohen, H.; Hopkins, R.O.; Weinert, C.; Wunsch, H.; Zawistowski, C.; Bemis-Dougherty, A.; Berney, S.C.; Bienvenu, O.J.; et al. Improving long-term outcomes after discharge from intensive care unit: Report from a stakeholders’ conference. Crit. Care Med. 2012, 40, 502–509. [Google Scholar] [CrossRef]
- Davidson, J.E.; Jones, C.; Bienvenu, O.J. Family response to critical illness: Postintensive care syndrome-family. Crit. Care Med. 2012, 40, 618–624. [Google Scholar] [CrossRef]
- Manning, J.C.; Pinto, N.P.; Rennick, J.E.; Colville, G.; Curley, M.A.Q. Conceptualizing Post Intensive Care Syndrome in Children-The PICS-p Framework. Pediatr. Crit. Care Med. 2018, 19, 298–300. [Google Scholar] [CrossRef]
- Rennick, J.E.; Dougherty, G.; Chambers, C.; Stremler, R.; Childerhose, J.E.; Stack, D.M.; Harrison, D.; Campbell-Yeo, M.; Dryden-Palmer, K.; Zhang, X.; et al. Children’s psychological and behavioral responses following pediatric intensive care unit hospitalization: The caring intensively study. BMC Pediatr. 2014, 14, 276. [Google Scholar] [CrossRef] [Green Version]
- Colville, G.A.; Pierce, C.M. Children’s self-reported quality of life after intensive care treatment. Pediatr. Crit. Care Med. 2013, 14, e85–e92. [Google Scholar] [CrossRef]
- Manning, J.C.; Hemingway, P.; Redsell, S.A. Stories of survival: Children’s narratives of psychosocial well-being following paediatric critical illness or injury. J. Child Health Care 2017, 21, 236–252. [Google Scholar] [CrossRef]
- Colville, G.; Pierce, C. Patterns of post-traumatic stress symptoms in families after paediatric intensive care. Intensive Care Med. 2012, 38, 1523–1531. [Google Scholar] [CrossRef] [PubMed]
- Ong, C.; Lee, J.H.; Leow, M.K.; Puthucheary, Z.A. Functional Outcomes and Physical Impairments in Pediatric Critical Care Survivors: A Scoping Review. Pediatr. Crit. Care Med. 2016, 17, e247–e259. [Google Scholar] [CrossRef] [PubMed]
- Osler, W.; McCrae, T. The Principles and Practice of Medicine: Designed for the Use of Practitioners and Students of Medicine, 8th ed.; D. Appleton: New York, NY, USA, 1915; p. 1225. [Google Scholar]
- Olsen, C.W. Lesions of peripheral nerves developing during coma. J. Am. Med. Assoc. 1956, 160, 39–41. [Google Scholar] [CrossRef]
- MacFarlane, I.A.; Rosenthal, F.D. Severe myopathy after status asthmaticus. Lancet 1977, 2, 615. [Google Scholar] [CrossRef]
- Bolton, C.F.; Gilbert, J.J.; Hahn, A.F.; Sibbald, W.J. Polyneuropathy in critically ill patients. J. Neurol. Neurosurg. Psychiatry 1984, 47, 1223–1231. [Google Scholar] [CrossRef]
- Siu, K.; Al-Harbi, S.; Clark, H.; Thabane, L.; Cheng, J.; Tarnopolsky, M.; Meaney, B.; Choong, K. Feasibility and Reliability of Muscle Strength Testing in Critically Ill Children. J. Pediatr. Intensive Care 2015, 4, 218–224. [Google Scholar] [CrossRef]
- Pollack, M.M.; Holubkov, R.; Funai, T.; Clark, A.; Moler, F.; Shanley, T.; Meert, K.; Newth, C.J.; Carcillo, J.; Berger, J.T.; et al. Relationship between the functional status scale and the pediatric overall performance category and pediatric cerebral performance category scales. JAMA Pediatr. 2014, 168, 671–676. [Google Scholar] [CrossRef] [Green Version]
- Pinto, N.P.; Rhinesmith, E.W.; Kim, T.Y.; Ladner, P.H.; Pollack, M.M. Long-Term Function After Pediatric Critical Illness: Results From the Survivor Outcomes Study. Pediatr. Crit. Care Med. 2017, 18, e122–e130. [Google Scholar] [CrossRef]
- Pollack, M.M.; Banks, R.; Holubkov, R.; Meert, K.L.; the Eunice Kennedy Shriver National Institute of Child Health and Human Development Collaborative Pediatric Critical Care Research Network. Long-Term Outcome of PICU Patients Discharged with New, Functional Status Morbidity. Pediatr. Crit. Care Med. 2021, 22, 27–39. [Google Scholar] [CrossRef]
- World Health Organization. International Classification of Functioning, Disability, and Health: Children & Youth Version: ICF-CY; World Health Organization: Geneva, Switzerland, 2007; p. 322. [Google Scholar]
- Ward, S.L.; Turpin, A.; Spicer, A.C.; Treadwell, M.J.; Church, G.D.; Flori, H.R. Long-Term Pulmonary Function and Quality of Life in Children After Acute Respiratory Distress Syndrome: A Feasibility Investigation. Pediatr. Crit. Care Med. 2017, 18, e48–e55. [Google Scholar] [CrossRef] [Green Version]
- Field-Ridley, A.; Dharmar, M.; Steinhorn, D.; McDonald, C.; Marcin, J.P. ICU-Acquired Weakness Is Associated With Differences in Clinical Outcomes in Critically Ill Children. Pediatr. Crit. Care Med. 2016, 17, 53–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Choong, K.; Fraser, D.; Al-Harbi, S.; Borham, A.; Cameron, J.; Cameron, S.; Cheng, J.; Clark, H.; Doherty, T.; Fayed, N.; et al. Functional Recovery in Critically Ill Children, the "WeeCover" Multicenter Study. Pediatr. Crit. Care Med. 2018, 19, 145–154. [Google Scholar] [CrossRef]
- Edwards, J.D.; Lucas, A.R.; Stone, P.W.; Boscardin, W.J.; Dudley, R.A. Frequency, risk factors, and outcomes of early unplanned readmissions to PICUs. Crit. Care Med. 2013, 41, 2773–2783. [Google Scholar] [CrossRef] [Green Version]
- Yagiela, L.M.; Barbaro, R.P.; Quasney, M.W.; Pfarr, M.A.; Ursu, D.C.; Prosser, L.A.; Odetola, F.O. Outcomes and Patterns of Healthcare Utilization After Hospitalization for Pediatric Critical Illness Due to Respiratory Failure. Pediatr. Crit. Care Med. 2019, 20, 120–127. [Google Scholar] [CrossRef] [PubMed]
- Edwards, J.D.; Lucas, A.R.; Boscardin, W.J.; Dudley, R.A. Repeated Critical Illness and Unplanned Readmissions Within 1 Year to PICUs. Crit. Care Med. 2017, 45, 1276–1284. [Google Scholar] [CrossRef]
- Pollack, M.M.; Holubkov, R.; Glass, P.; Dean, J.M.; Meert, K.L.; Zimmerman, J.; Anand, K.J.; Carcillo, J.; Newth, C.J.; Harrison, R.; et al. Functional Status Scale: New pediatric outcome measure. Pediatrics 2009, 124, e18–e28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pollack, M.M.; Holubkov, R.; Funai, T.; Berger, J.T.; Clark, A.E.; Meert, K.; Berg, R.A.; Carcillo, J.; Wessel, D.L.; Moler, F.; et al. Simultaneous Prediction of New Morbidity, Mortality, and Survival Without New Morbidity From Pediatric Intensive Care: A New Paradigm for Outcomes Assessment. Crit. Care Med. 2015, 43, 1699–1709. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bone, M.F.; Feinglass, J.M.; Goodman, D.M. Risk factors for acquiring functional and cognitive disabilities during admission to a PICU*. Pediatr. Crit. Care Med. 2014, 15, 640–648. [Google Scholar] [CrossRef]
- Watson, R.S.; Asaro, L.A.; Hutchins, L.; Bysani, G.K.; Killien, E.Y.; Angus, D.C.; Wypij, D.; Curley, M.A.Q. Risk Factors for Functional Decline and Impaired Quality of Life after Pediatric Respiratory Failure. Am. J. Respir. Crit. Care Med. 2019, 200, 900–909. [Google Scholar] [CrossRef]
- Watson, R.S.; Asaro, L.A.; Hertzog, J.H.; Sorce, L.R.; Kachmar, A.G.; Dervan, L.A.; Angus, D.C.; Wypij, D.; Curley, M.A.Q.; Investigators, R.S.; et al. Long-Term Outcomes after Protocolized Sedation versus Usual Care in Ventilated Pediatric Patients. Am. J. Respir. Crit. Care Med. 2018, 197, 1457–1467. [Google Scholar] [CrossRef]
- Farris, R.W.; Weiss, N.S.; Zimmerman, J.J. Functional outcomes in pediatric severe sepsis: Further analysis of the researching severe sepsis and organ dysfunction in children: A global perspective trial. Pediatr. Crit. Care Med. 2013, 14, 835–842. [Google Scholar] [CrossRef] [Green Version]
- Bennett, T.D.; Dixon, R.R.; Kartchner, C.; DeWitt, P.E.; Sierra, Y.; Ladell, D.; Kempe, A.; Runyan, D.K.; Dean, J.M.; Keenan, H.T. Functional Status Scale in Children With Traumatic Brain Injury: A Prospective Cohort Study. Pediatr. Crit. Care Med. 2016, 17, 1147–1156. [Google Scholar] [CrossRef] [Green Version]
- Sankar, J.; Moodu, S.; Kumar, K.; Sankar, M.J.; Kabra, S.K.; Lodha, R. Functional Outcomes at 1 Year After PICU Discharge in Critically Ill Children With Severe Sepsis. Pediatr. Crit. Care Med. 2021, 22, 40–49. [Google Scholar] [CrossRef] [PubMed]
- Slovis, J.C.; Gupta, N.; Li, N.Y.; Kernie, S.G.; Miles, D.K. Assessment of Recovery Following Pediatric Traumatic Brain Injury. Pediatr. Crit. Care Med. 2018, 19, 353–360. [Google Scholar] [CrossRef]
- Heneghan, J.A.; Reeder, R.W.; Dean, J.M.; Meert, K.L.; Berg, R.A.; Carcillo, J.; Newth, C.J.L.; Dalton, H.; Tamburro, R.; Pollack, M.M. Characteristics and Outcomes of Critical Illness in Children With Feeding and Respiratory Technology Dependence. Pediatr. Crit. Care Med. 2019, 20, 417–425. [Google Scholar] [CrossRef] [PubMed]
- Als, L.C.; Nadel, S.; Cooper, M.; Pierce, C.M.; Sahakian, B.J.; Garralda, M.E. Neuropsychologic function three to six months following admission to the PICU with meningoencephalitis, sepsis, and other disorders: A prospective study of school-aged children. Crit. Care Med. 2013, 41, 1094–1103. [Google Scholar] [CrossRef] [PubMed]
- Elias, M.D.; Achuff, B.J.; Ittenbach, R.F.; Ravishankar, C.; Spray, T.L.; Fuller, S.; Montenegro, L.M.; Gaynor, J.W.; O’Connor, M.J. Long-Term Outcomes of Pediatric Cardiac Patients Supported by Extracorporeal Membrane Oxygenation. Pediatr. Crit. Care Med. 2017, 18, 787–794. [Google Scholar] [CrossRef] [PubMed]
- Watson, R.S.; Choong, K.; Colville, G.; Crow, S.; Dervan, L.A.; Hopkins, R.O.; Knoester, H.; Pollack, M.M.; Rennick, J.; Curley, M.A.Q. Life after Critical Illness in Children-Toward an Understanding of Pediatric Post-intensive Care Syndrome. J. Pediatr. 2018, 198, 16–24. [Google Scholar] [CrossRef]
- Vermunt, L.C.; Buysse, C.M.; Joosten, K.F.; Duivenvoorden, H.J.; Hazelzet, J.A.; Verhulst, F.C.; Utens, E.M. Survivors of septic shock caused by Neisseria meningitidis in childhood: Psychosocial outcomes in young adulthood. Pediatr. Crit. Care Med. 2011, 12, e302–e309. [Google Scholar] [CrossRef]
- Elison, S.; Shears, D.; Nadel, S.; Sahakian, B.; Garralda, M.E. Neuropsychological function in children following admission to paediatric intensive care: A pilot investigation. Intensive Care Med. 2008, 34, 1289–1293. [Google Scholar] [CrossRef]
- Kachmar, A.G.; Irving, S.Y.; Connolly, C.A.; Curley, M.A.Q. A Systematic Review of Risk Factors Associated With Cognitive Impairment After Pediatric Critical Illness. Pediatr. Crit. Care Med. 2018, 19, e164–e171. [Google Scholar] [CrossRef]
- Garcia Guerra, G.; Zorzela, L.; Robertson, C.M.; Alton, G.Y.; Joffe, A.R.; Moez, E.K.; Dinu, I.A.; Ross, D.B.; Rebeyka, I.M.; Lequier, L.; et al. Survival and neurocognitive outcomes in pediatric extracorporeal-cardiopulmonary resuscitation. Resuscitation 2015, 96, 208–213. [Google Scholar] [CrossRef]
- Als, L.C.; Picouto, M.D.; Hau, S.M.; Nadel, S.; Cooper, M.; Pierce, C.M.; Kramer, T.; Garralda, M.E. Mental and physical well-being following admission to pediatric intensive care. Pediatr. Crit. Care Med. 2015, 16, e141–e149. [Google Scholar] [CrossRef] [PubMed]
- Mestrovic, J.; Kardum, G.; Sustic, A.; Polic, B.; Mestrovic, M.; Markic, J.; Zanchi, J. Neurodevelopmental disabilities and quality of life after intensive care treatment. J. Paediatr. Child Health 2007, 43, 673–676. [Google Scholar] [CrossRef]
- Diagnostic and Statistics Manual of Mental Disorders, 5th ed.; American Psychatic Association: Arlington, VA, USA, 2013.
- Davydow, D.S.; Richardson, L.P.; Zatzick, D.F.; Katon, W.J. Psychiatric morbidity in pediatric critical illness survivors: A comprehensive review of the literature. Arch. Pediatr. Adolesc. Med. 2010, 164, 377–385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rennick, J.E.; Rashotte, J. Psychological outcomes in children following pediatric intensive care unit hospitalization: A systematic review of the research. J. Child Health Care 2009, 13, 128–149. [Google Scholar] [CrossRef]
- Carnevale, F.A. The experience of critically ill children: Narratives of unmaking. Intensive Crit. Care Nurs. 1997, 13, 49–52. [Google Scholar] [CrossRef]
- Colville, G.; Kerry, S.; Pierce, C. Children’s factual and delusional memories of intensive care. Am. J. Respir. Crit. Care Med. 2008, 177, 976–982. [Google Scholar] [CrossRef] [PubMed]
- Rennick, J.E.; McHarg, L.F.; Dell’Api, M.; Johnston, C.C.; Stevens, B. Developing the Children’s Critical Illness Impact Scale: Capturing stories from children, parents, and staff. Pediatr. Crit. Care Med. 2008, 9, 252–260. [Google Scholar] [CrossRef]
- Lopes-Junior, L.C.; Rosa, M.; Lima, R.A.G. Psychological and Psychiatric Outcomes Following PICU Admission: A Systematic Review of Cohort Studies. Pediatr. Crit. Care Med. 2018, 19, e58–e67. [Google Scholar] [CrossRef]
- Rees, G.; Gledhill, J.; Garralda, M.E.; Nadel, S. Psychiatric outcome following paediatric intensive care unit (PICU) admission: A cohort study. Intensive Care Med. 2004, 30, 1607–1614. [Google Scholar] [CrossRef]
- Rady, H.I.; Ismail, O.R.; Abdelkader, M.S.; Abdelgalil, A.A. Increased Psychiatric Risk in Children After Pediatric Intensive Care Unit Admission. J. Nerv. Ment. Dis. 2020, 208, 147–151. [Google Scholar] [CrossRef]
- Nelson, L.P.; Lachman, S.E.; Li, S.W.; Gold, J.I. The Effects of Family Functioning on the Development of Posttraumatic Stress in Children and Their Parents Following Admission to the PICU. Pediatr. Crit. Care Med. 2019, 20, e208–e215. [Google Scholar] [CrossRef]
- Colville, G.A.; Pierce, C.M.; Peters, M.J. Self-Reported Fatigue in Children Following Intensive Care Treatment. Pediatr. Crit. Care Med. 2019, 20, e98–e101. [Google Scholar] [CrossRef]
- Hordijk, J.; Verbruggen, S.; Vanhorebeek, I.; Guiza, F.; Wouters, P.; Van den Berghe, G.; Joosten, K.; Dulfer, K. Health-related quality of life of children and their parents 2 years after critical illness: Pre-planned follow-up of the PEPaNIC international, randomized, controlled trial. Crit. Care 2020, 24, 347. [Google Scholar] [CrossRef] [PubMed]
- Hordijk, J.; Verbruggen, S.; Vanhorebeek, I.; Van den Berghe, G.; Utens, E.; Joosten, K.; Dulfer, K. Health-related quality of life of children and their parents 6 months after children’s critical illness. Qual. Life Res. 2020, 29, 179–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baker, S.C.; Gledhill, J.A. Systematic Review of Interventions to Reduce Psychiatric Morbidity in Parents and Children After PICU Admissions. Pediatr. Crit. Care Med. 2017, 18, 343–348. [Google Scholar] [CrossRef]
- Atkins, E.K.; John, M.; Colville, G. Families’ Experiences of Life in the Year after a Child’s Critical Illness: Navigating the Road to a “New Normal”. J. Pediatr. Intensive Care 2020, 9, 188–195. [Google Scholar] [CrossRef]
- Foster, K.; Mitchell, R.; Van, C.; Young, A.; McCloughen, A.; Curtis, K. Resilient, recovering, distressed: A longitudinal qualitative study of parent psychosocial trajectories following child critical injury. Injury 2019, 50, 1605–1611. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Foster, K.; Mitchell, R.; Young, A.; Van, C.; Curtis, K. Parent experiences and psychosocial support needs 6 months following paediatric critical injury: A qualitative study. Injury 2019, 50, 1082–1088. [Google Scholar] [CrossRef]
- Allison, M.A.; Attisha, E.; Council On School, H. The Link Between School Attendance and Good Health. Pediatrics 2019, 143. [Google Scholar] [CrossRef] [Green Version]
- Kastner, K.; Pinto, N.; Msall, M.E.; Sobotka, S. PICU Follow-Up: The Impact of Missed School in a Cohort of Children Following PICU Admission. Crit. Care Explor. 2019, 1, e0033. [Google Scholar] [CrossRef]
- Emerson, N.D.; Distelberg, B.; Morrell, H.E.; Williams-Reade, J.; Tapanes, D.; Montgomery, S. Quality of Life and School Absenteeism in Children With Chronic Illness. J. Sch. Nurs. 2016, 32, 258–266. [Google Scholar] [CrossRef] [Green Version]
- Shapiro, M.C.; Henderson, C.M.; Hutton, N.; Boss, R.D. Defining Pediatric Chronic Critical Illness for Clinical Care, Research, and Policy. Hosp. Pediatr. 2017, 7, 236–244. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Rey, R.; Alonso-Tapia, J.; Colville, G. Prediction of parental posttraumatic stress, anxiety and depression after a child’s critical hospitalization. J. Crit. Care 2018, 45, 149–155. [Google Scholar] [CrossRef]
- Nelson, L.P.; Gold, J.I. Posttraumatic stress disorder in children and their parents following admission to the pediatric intensive care unit: A review. Pediatr. Crit. Care Med. 2012, 13, 338–347. [Google Scholar] [CrossRef]
- Logan, G.E.; Sahrmann, J.M.; Gu, H.; Harman, M. Parental Mental Health Care After Their Child’s Pediatric Intesnive Care Hospitaliation. Pediatr. Crit. Care Med. 2020, 21, 941–948. [Google Scholar] [CrossRef] [PubMed]
- Bronner, M.B.; Peek, N.; Knoester, H.; Bos, A.P.; Last, B.F.; Grootenhuis, M.A. Course and predictors of posttraumatic stress disorder in parents after pediatric intensive care treatment of their child. J. Pediatr. Psychol. 2010, 35, 966–974. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.S.P.; Grossoehme, D.H.; Forbes, M.L.; Friebert, S. Provider Consensus on Candidate Protective and Risk Factors for Adverse Psychosocial Outcomes Following Discharge From a PICU: A Modified Delphi Study. Pediatr. Crit. Care Med. 2020, 21, e1–e7. [Google Scholar] [CrossRef]
- Duffett, M.; Choong, K.; Hartling, L.; Menon, K.; Thabane, L.; Cook, D.J. Randomized controlled trials in pediatric critical care: A scoping review. Crit. Care 2013, 17, R256. [Google Scholar] [CrossRef] [Green Version]
- Aspesberro, F.; Fesinmeyer, M.D.; Zhou, C.; Zimmerman, J.J.; Mangione-Smith, R. Construct Validity and Responsiveness of the Pediatric Quality of Life Inventory 4.0 Generic Core Scales and Infant Scales in the PICU. Pediatr. Crit. Care Med. 2016, 17, e272–e279. [Google Scholar] [CrossRef]
- Fayed, N.; Cameron, S.; Fraser, D.; Cameron, J.I.; Al-Harbi, S.; Simpson, R.; Wakim, M.; Chiu, L.; Choong, K. Priority Outcomes in Critically Ill Children: A Patient and Parent Perspective. Am. J. Crit. Care 2020, 29, e94–e103. [Google Scholar] [CrossRef] [PubMed]
- Ebrahim, S.; Singh, S.; Hutchison, J.S.; Kulkarni, A.V.; Sananes, R.; Bowman, K.W.; Parshuram, C.S. Adaptive behavior, functional outcomes, and quality of life outcomes of children requiring urgent ICU admission. Pediatr. Crit. Care Med. 2013, 14, 10–18. [Google Scholar] [CrossRef]
- Buysse, C.M.; Vermunt, L.C.; Raat, H.; Hazelzet, J.A.; Hop, W.C.; Utens, E.M.; Joosten, K.F. Surviving meningococcal septic shock in childhood: Long-term overall outcome and the effect on health-related quality of life. Crit. Care 2010, 14, R124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Edmond, K.; Dieye, Y.; Griffiths, U.K.; Fleming, J.; Ba, O.; Diallo, N.; Mulholland, K. Prospective cohort study of disabling sequelae and quality of life in children with bacterial meningitis in urban Senegal. Pediatr. Infect. Dis. J. 2010, 29, 1023–1029. [Google Scholar] [CrossRef]
- Martin-Herz, S.P.; Zatzick, D.F.; McMahon, R.J. Health-related quality of life in children and adolescents following traumatic injury: A review. Clin. Child Fam. Psychol. Rev. 2012, 15, 192–214. [Google Scholar] [CrossRef] [Green Version]
- Polic, B.; Mestrovic, J.; Markic, J.; Mestrovic, M.; Capkun, V.; Utrobicic, I.; Jukica, M.; Radonic, M. Long-term quality of life of patients treated in paediatric intensive care unit. Eur. J. Pediatr. 2013, 172, 85–90. [Google Scholar] [CrossRef]
- Namachivayam, P.; Taylor, A.; Montague, T.; Moran, K.; Barrie, J.; Delzoppo, C.; Butt, W. Long-stay children in intensive care: Long-term functional outcome and quality of life from a 20-yr institutional study. Pediatr. Crit. Care Med. 2012, 13, 520–528. [Google Scholar] [CrossRef] [Green Version]
- Fink, E.L.; Jarvis, J.M.; Maddux, A.B.; Pinto, N.; Galyean, P.; Olson, L.M.; Zickmund, S.; Ringwood, M.; Sorenson, S.; Dean, J.M.; et al. Development of a core outcome set for pediatric critical care outcomes research. Contemp. Clin. Trials 2020, 91, 105968. [Google Scholar] [CrossRef] [PubMed]
- Fink, E.L.; Maddux, A.B.; Pinto, N.; Sorenson, S.; Notterman, D.; Dean, J.M.; Carcillo, J.A.; Berg, R.A.; Zuppa, A.; Pollack, M.M.; et al. A Core Outcome Set for Pediatric Critical Care. Crit. Care Med. 2020, 48, 1819–1828. [Google Scholar] [CrossRef]
- Matics, T.J.; Pinto, N.P.; Sanchez-Pinto, L.N. Association of Organ Dysfunction Scores and Functional Outcomes Following Pediatric Critical Illness. Pediatr. Crit. Care Med. 2019, 20, 722–727. [Google Scholar] [CrossRef]
- Senna, S.; Ong, C.; Wong, J.J.; Allen, J.C., Jr.; Sultana, R.; Lee, J.H. Prediction of Acquired Morbidity Using Illness Severity Indices in Pediatric Intensive Care Patients. Pediatr. Crit. Care Med. 2020, 21, e972–e980. [Google Scholar] [CrossRef] [PubMed]
- Meert, K.L.; Reeder, R.; Maddux, A.B.; Banks, R.; Berg, R.A.; Zuppa, A.; Newth, C.J.; Wessel, D.; Pollack, M.M.; Hall, M.W.; et al. Trajectories and Risk Factors for Altered Physical and Psychosocial Health-Related Quality of Life After Pediatric Community-Acquired Septic Shock. Pediatr. Crit. Care Med. 2020, 21, 869–878. [Google Scholar] [CrossRef] [PubMed]
- Silver, G.; Doyle, H.; Hegel, E.; Kaur, S.; Mauer, E.A.; Gerber, L.M.; Traube, C. Association Between Pediatric Delirium and Quality of Life After Discharge. Crit. Care Med. 2020, 48, 1829–1834. [Google Scholar] [CrossRef]
- Devlin, J.W.; Skrobik, Y.; Gelinas, C.; Needham, D.M.; Slooter, A.J.C.; Pandharipande, P.P.; Watson, P.L.; Weinhouse, G.L.; Nunnally, M.E.; Rochwerg, B.; et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU. Crit. Care Med. 2018, 46, e825–e873. [Google Scholar] [CrossRef] [Green Version]
- Choong, K.; Tran, N.; Clark, H.; Cupido, C.; Corsi, D.J. Acute rehabilitation in critically ill children. J. Pediatr. Intensive Care 2012, 1, 183–192. [Google Scholar] [CrossRef]
- van Zellem, L.; Utens, E.M.; de Wildt, S.N.; Vet, N.J.; Tibboel, D.; Buysse, C. Analgesia-sedation in PICU and neurological outcome: A secondary analysis of long-term neuropsychological follow-up in meningococcal septic shock survivors*. Pediatr. Crit. Care Med. 2014, 15, 189–196. [Google Scholar] [CrossRef]
- Dervan, L.A.; Di Gennaro, J.L.; Farris, R.W.D.; Watson, R.S. Delirium in a Tertiary PICU: Risk Factors and Outcomes. Pediatr. Crit. Care Med. 2020, 21, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Meyburg, J.; Ries, M.; Zielonka, M.; Koch, K.; Sander, A.; von Haken, R.; Reuner, G. Cognitive and Behavioral Consequences of Pediatric Delirium: A Pilot Study. Pediatr. Crit. Care Med. 2018, 19, e531–e537. [Google Scholar] [CrossRef] [PubMed]
- Verstraete, S.; Verbruggen, S.C.; Hordijk, J.A.; Vanhorebeek, I.; Dulfer, K.; Guiza, F.; van Puffelen, E.; Jacobs, A.; Leys, S.; Durt, A.; et al. Long-term developmental effects of withholding parenteral nutrition for 1 week in the paediatric intensive care unit: A 2-year follow-up of the PEPaNIC international, randomised, controlled trial. Lancet Respir. Med. 2019, 7, 141–153. [Google Scholar] [CrossRef]
- Jacobs, A.; Dulfer, K.; Eveleens, R.D.; Hordijk, J.; Van Cleemput, H.; Verlinden, I.; Wouters, P.J.; Mebis, L.; Guerra, G.G.; Joosten, K.; et al. Long-term developmental effect of withholding parenteral nutrition in paediatric intensive care units: A 4-year follow-up of the PEPaNIC randomised controlled trial. Lancet Child Adolesc. Health 2020, 4, 503–514. [Google Scholar] [CrossRef]
- Biagas, K.V.; Hinton, V.J.; Hasbani, N.R.; Luckett, P.M.; Wypij, D.; Nadkarni, V.M.; Agus, M.S.D.; HALF-PINT Trial Study Investigators; Network, P. Long-Term Neurobehavioral and Quality of Life Outcomes of Critically Ill Children after Glycemic Control. J. Pediatr. 2020, 218, 57–63.e55. [Google Scholar] [CrossRef] [Green Version]
- Meert, K.; Slomine, B.S.; Christensen, J.R.; Telford, R.; Holubkov, R.; Dean, J.M.; Moler, F.W. Burden of caregiving after a child’s in-hospital cardiac arrest. Resuscitation 2018, 127, 44–50. [Google Scholar] [CrossRef]
- Treble-Barna, A.; Beers, S.R.; Houtrow, A.J.; Ortiz-Aguayo, R.; Valenta, C.; Stanger, M.; Chrisman, M.; Orringer, M.; Smith, C.M.; Pollon, D.; et al. PICU-Based Rehabilitation and Outcomes Assessment: A Survey of Pediatric Critical Care Physicians. Pediatr. Crit. Care Med. 2019, 20, e274–e282. [Google Scholar] [CrossRef]
- Jackson, J.C.; Santoro, M.J.; Ely, T.M.; Boehm, L.; Kiehl, A.L.; Anderson, L.S.; Ely, E.W. Improving patient care through the prism of psychology: Application of Maslow’s hierarchy to sedation, delirium, and early mobility in the intensive care unit. J. Crit. Care 2014, 29, 438–444. [Google Scholar] [CrossRef] [Green Version]
- Morandi, A.; Piva, S.; Ely, E.W.; Myatra, S.N.; Salluh, J.I.F.; Amare, D.; Azoulay, E.; Bellelli, G.; Csomos, A.; Fan, E.; et al. Worldwide Survey of the “Assessing Pain, Both Spontaneous Awakening and Breathing Trials, Choice of Drugs, Delirium Monitoring/Management, Early Exercise/Mobility, and Family Empowerment” (ABCDEF) Bundle. Crit. Care Med. 2017, 45, e1111–e1122. [Google Scholar] [CrossRef] [PubMed]
- Pun, B.T.; Balas, M.C.; Barnes-Daly, M.A.; Thompson, J.L.; Aldrich, J.M.; Barr, J.; Byrum, D.; Carson, S.S.; Devlin, J.W.; Engel, H.J.; et al. Caring for Critically Ill Patients with the ABCDEF Bundle: Results of the ICU Liberation Collaborative in Over 15,000 Adults. Crit. Care Med. 2019, 47, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Cuello-Garcia, C.A.; Mai, S.H.C.; Simpson, R.; Al-Harbi, S.; Choong, K. Early Mobilization in Critically Ill Children: A Systematic Review. J. Pediatr. 2018, 203, 25–33.e26. [Google Scholar] [CrossRef] [Green Version]
- Curley, M.A.; Wypij, D.; Watson, R.S.; Grant, M.J.; Asaro, L.A.; Cheifetz, I.M.; Dodson, B.L.; Franck, L.S.; Gedeit, R.G.; Angus, D.C.; et al. Protocolized sedation vs usual care in pediatric patients mechanically ventilated for acute respiratory failure: A randomized clinical trial. JAMA 2015, 313, 379–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harris, J.; Ramelet, A.S.; van Dijk, M.; Pokorna, P.; Wielenga, J.; Tume, L.; Tibboel, D.; Ista, E. Clinical recommendations for pain, sedation, withdrawal and delirium assessment in critically ill infants and children: An ESPNIC position statement for healthcare professionals. Intensive Care Med. 2016, 42, 972–986. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simone, S.; Edwards, S.; Lardieri, A.; Walker, L.K.; Graciano, A.L.; Kishk, O.A.; Custer, J.W. Implementation of an ICU Bundle: An Interprofessional Quality Improvement Project to Enhance Delirium Management and Monitor Delirium Prevalence in a Single PICU. Pediatr. Crit. Care Med. 2017, 18, 531–540. [Google Scholar] [CrossRef] [PubMed]
- Herrup, E.A.; Wieczorek, B.; Kudchadkar, S.R. Feasibility and Perceptions of PICU Diaries. Pediatr. Crit. Care Med. 2019, 20, e83–e90. [Google Scholar] [CrossRef]
- Lynch, F.; Endacott, R.; Latour, J.M. Patient diaries: Survey of paediatric intensive care units in the United Kingdom and Ireland. Nurs. Crit. Care 2020, 25, 31–36. [Google Scholar] [CrossRef] [Green Version]
- McIlroy, P.A.; King, R.S.; Garrouste-Orgeas, M.; Tabah, A.; Ramanan, M. The Effect of ICU Diaries on Psychological Outcomes and Quality of Life of Survivors of Critical Illness and Their Relatives: A Systematic Review and Meta-Analysis. Crit. Care Med. 2019, 47, 273–279. [Google Scholar] [CrossRef]
- Samuel, V.M.; Colville, G.A.; Goodwin, S.; Ryninks, K.; Dean, S. The Value of Screening Parents for Their Risk of Developing Psychological Symptoms After PICU: A Feasibility Study Evaluating a Pediatric Intensive Care Follow-Up Clinic. Pediatr. Crit. Care Med. 2015, 16, 808–813. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.N.; Kirby, A.; Piantino, J. If You Build It, They Will Come: Initial Experience with a Multi-Disciplinary Pediatric Neurocritical Care Follow-Up Clinic. Children 2017, 4, 83. [Google Scholar] [CrossRef] [Green Version]
- Colville, G.A.; Cream, P.R.; Kerry, S.M. Do parents benefit from the offer of a follow-up appointment after their child’s admission to intensive care?: An exploratory randomised controlled trial. Intensive Crit. Care Nurs. 2010, 26, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Manning, J.C.; Scholefield, B.R.; Popejoy, E.; Dodds, E.; Latour, J.M. Paediatric intensive care follow-up provision in the United Kingdom and Republic of Ireland. Nurs. Crit. Care 2021, 26, 128–134. [Google Scholar] [CrossRef]
- Choong, K. Early Rehabilitation in Critically Ill Children-The PICU Liber8 Study (PICULiber8); NCT03573479; U.S. National Library of Medicine: Bethesda, MD, USA, 2019. Available online: www.clinicaltrials.gov (accessed on 2 February 2021).
- Blackwood, B.; Agus, A.; Boyle, R.; Clarke, M.; Hemming, K.; Jordan, J.; Macrae, D.; McAuley, D.F.; McDowell, C.; McIlmurray, L.; et al. Sedation AND Weaning In Children (SANDWICH): Protocol for a cluster randomised stepped wedge trial. BMJ Open 2019, 9, e031630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kudchadkar, S.R. PICU Up! A Pilot Stepped-Wedge Trial of a Multicomponent Early Mobility Intervention for Critically Ill Children (PICU Up!); NCT03860168; U.S. National Library of Medicine: Bethesda, MD, USA, 2019. Available online: www.clinicaltrials.gov (accessed on 2 February 2021).
Figure 1.
Number of manuscripts evaluating post-discharge outcomes after pediatric critical illness and study designs. Composite in the legend refers to the additive total number of articles. Original figure by Maddux et al. [20]. Graph generated using a comprehensive search strategy outlined in Table S2 of the Supplemental Digital Content in the original article, title and abstract exclusion, and dual full-text screening of the remaining articles [20]. Reprinted with appropriate permission from Wolters Kluwer. Original Copyright © 2021 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Figure 1.
Number of manuscripts evaluating post-discharge outcomes after pediatric critical illness and study designs. Composite in the legend refers to the additive total number of articles. Original figure by Maddux et al. [20]. Graph generated using a comprehensive search strategy outlined in Table S2 of the Supplemental Digital Content in the original article, title and abstract exclusion, and dual full-text screening of the remaining articles [20]. Reprinted with appropriate permission from Wolters Kluwer. Original Copyright © 2021 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
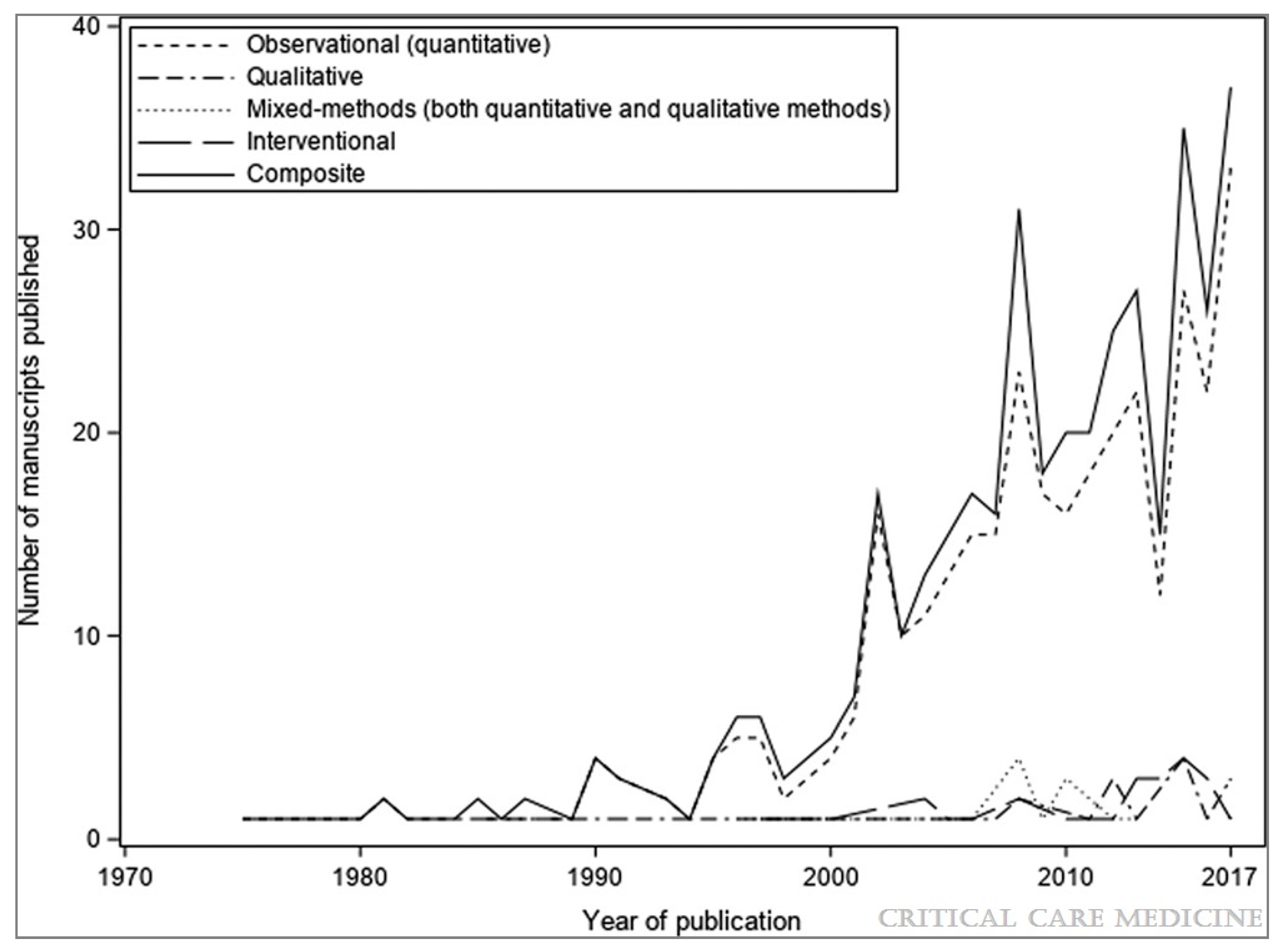
Figure 2.
A framework for the post-intensive care syndrome—pediatrics (PICS-p). Original figure by Manning et al. [23]. Reprinted with appropriate permission from Wolters Kluwer. Original Copyright © 2021 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.
Figure 2.
A framework for the post-intensive care syndrome—pediatrics (PICS-p). Original figure by Manning et al. [23]. Reprinted with appropriate permission from Wolters Kluwer. Original Copyright © 2021 by the Society of Critical Care Medicine and the World Federation of Pediatric Intensive and Critical Care Societies.

{kind=link}
{kind=link}
Table 1.
PICs-P domains and selected examples of adverse outcomes in each domain. Listed examples are not comprehensive, and some examples can span multiple domains.
Table 1.
PICs-P domains and selected examples of adverse outcomes in each domain. Listed examples are not comprehensive, and some examples can span multiple domains.
| PICs-P Domains | Examples | ||
|---|---|---|---|
| Physical Health | Chronic organ dysfunction or failure Technology dependence Chronic pain Feeding problems or malnutrition Fatigue or weakness Sleep disturbances. |  | Health-Related Quality of Life |
| Cognitive Health | Reduced attention Memory problems Decreased communication abilities Decreased school achievement. | ||
| Emotional Health | Depression Post-traumatic stress symptoms and disorder Anxiety Delusional memories and fears Behavioral problems Sleep disturbances. | ||
| Social Health | Loss of peer relationships Loss of social identity School absenteeism Decreased participation Strained family relationships Social anxiety. | ||
| PICs-F (Family) | Parent, caretaker or sibling psychiatric complications Job loss Food or housing insecurity Strained family relationships Family financial strain | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Woodruff, A.G.; Choong, K. Long-Term Outcomes and the Post-Intensive Care Syndrome in Critically Ill Children: A North American Perspective. Children 2021, 8, 254. https://0-doi-org.brum.beds.ac.uk/10.3390/children8040254
AMA Style
Woodruff AG, Choong K. Long-Term Outcomes and the Post-Intensive Care Syndrome in Critically Ill Children: A North American Perspective. Children. 2021; 8(4):254. https://0-doi-org.brum.beds.ac.uk/10.3390/children8040254
Chicago/Turabian StyleWoodruff, Alan G., and Karen Choong. 2021. "Long-Term Outcomes and the Post-Intensive Care Syndrome in Critically Ill Children: A North American Perspective" Children 8, no. 4: 254. https://0-doi-org.brum.beds.ac.uk/10.3390/children8040254
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.