
Australian Foster Carers’ Views and Concerns Regarding Maternal Drug Use and the Safety of Breastmilk

Abstract
:1. Introduction
2. Materials and Methods
2.1. Survey
2.2. Participants
2.3. Ethical Considerations
2.4. Data Analysis and Management
3. Results
3.1. Demographics
3.2. Support of Breast Feeding in the Foster Care Community
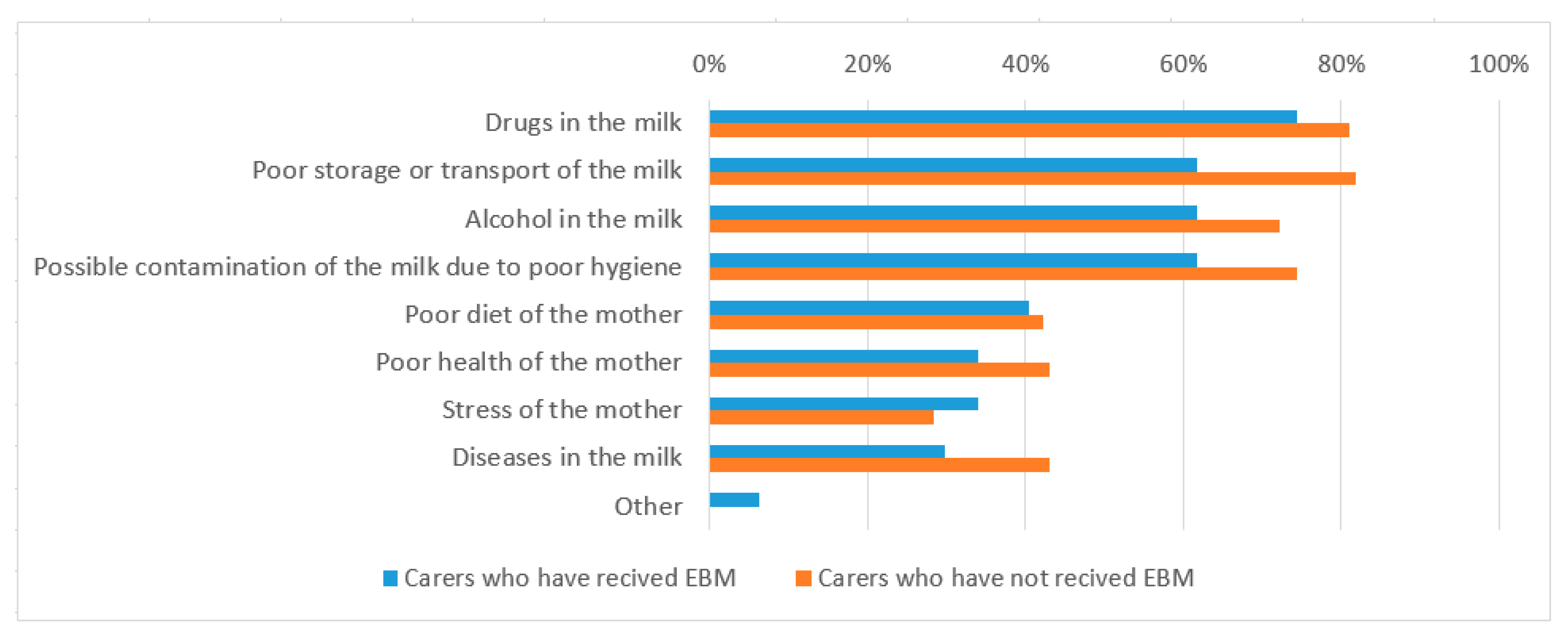
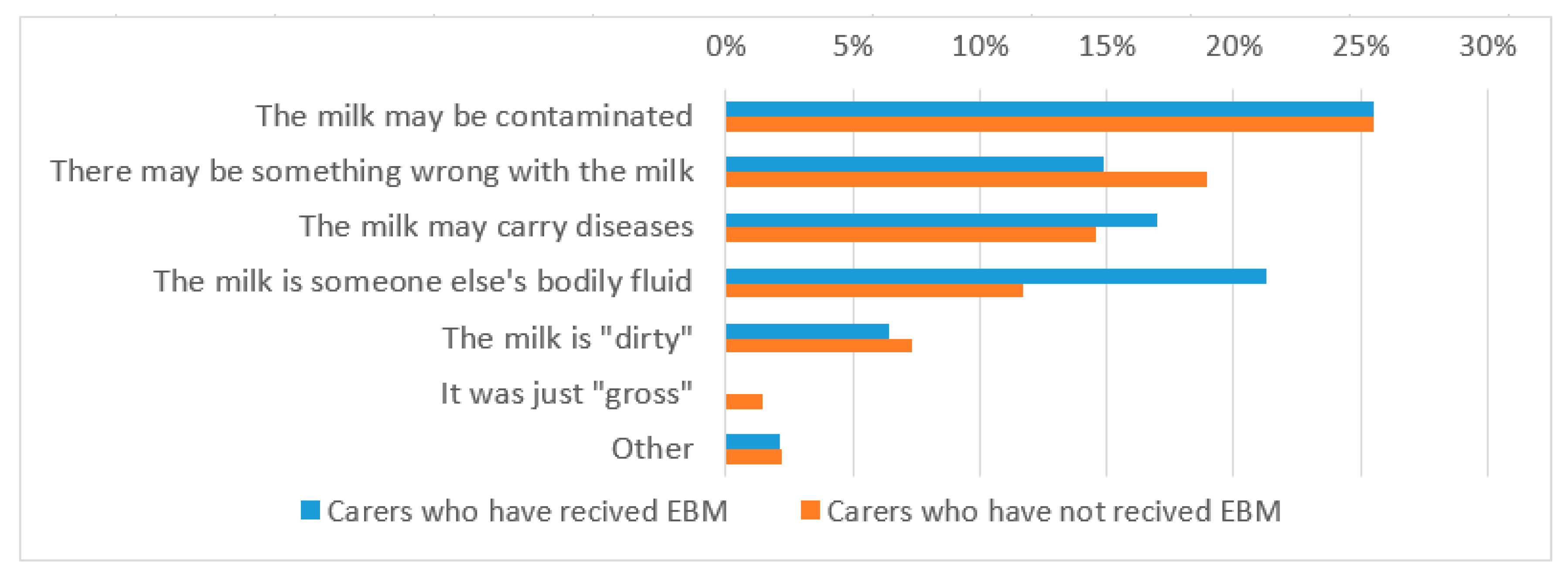
3.3. Breast Milk Safety
3.4. Behaviours as a Result of Breast Milk Saftey Concerns
3.5. Carer Training Regarding EBM
4. Discussion
4.1. Lack of Background Information
4.2. Knowledge Deficit Regarding Breast Milk Safety
4.3. Need for Integrated Care for Infants Entering OOHC
4.4. Limitations and Suggestions for Future Research
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Australian Institute of Health and Welfare. Child Protection Australia 2018–19; AIHW: Canberra, Australia, 2020.
- Boyd, R. Foster care outcomes and experiences of infants removed due to substance abuse. J. Public Child Welf. 2019, 13, 529–555. [Google Scholar] [CrossRef]
- Bunting, L.; McCartan, C.; McGhee, J.; Bywaters, P.; Daniel, B.; Featherstone, B.; Slater, T. Trends in child protection across the UK: A comparative analysis. Br. J. Soc. Work 2018, 48, 1154–1175. [Google Scholar] [CrossRef]
- Zhou, A.Z.; Chilvers, M. Infants in Australian Out-of-Home Care. Br. J. Soc. Work 2008, 40, 26–43. [Google Scholar] [CrossRef]
- Behnke, M.; Smith, V.C. Prenatal Substance Abuse: Short- and Long-term Effects on the Exposed Fetus. Pediatrics 2013, 131, e1009–e1024. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maguire, D. Care of the Infant with Neonatal Abstinence Syndrome: Strength of the Evidence. J. Perinat. Neonatal Nurs. 2014, 28, 204–211. [Google Scholar] [CrossRef]
- Vaiserman, A. Long-term health consequences of early-life exposure to substance abuse: An epigenetic perspective. J. Dev. Orig. Health Dis. 2013, 4, 269–279. [Google Scholar] [CrossRef]
- Oei, J.L. Adult consequences of prenatal drug exposure. Intern. Med. J. 2018, 48, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Oei, J.L. After NAS. In Seminars in Fetal and Neonatal Medicine; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Bagley, S.M.; Wachman, E.M.; Holland, E.; Brogly, S.B. Review of the assessment and management of neonatal abstinence syndrome. Addict. Sci. Clin. Pract. 2014, 9, 19. [Google Scholar] [CrossRef] [Green Version]
- Shannon, J.; Blythe, S.; Peters, K. The Complexities Associated with Caring for Hospitalised Infants with Neonatal Abstinence Syndrome: The Perspectives of Nurses and Midwives. Children 2021, 8, 152. [Google Scholar] [CrossRef]
- COAG Health Council. Australian National Breastfeeding Strategy: 2019 and Beyond; Department of Health: Canberra, Australia, 2019.
- World Health Organization; UNICEF. Global Strategy for Infant and Young Child Feeding; WHO: Geneva, Switzerland, 2003. [Google Scholar]
- NHMRC. Infant Feeding Guidelines for Health Workers; Commonwealth of Australia: Canberra, Australia, 2013.
- Payne, S.; Quigley, M.A. Breastfeeding and infant hospitalisation: Analysis of the UK 2010 Infant Feeding Survey. Matern. Child Nutr. 2016, 13, e12263. [Google Scholar] [CrossRef]
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; França, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C. Breastfeeding in the 21st century: Epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef] [Green Version]
- Goemans, A.; van Geel, M.; van Beem, M.; Vedder, P. Developmental outcomes of foster children: A meta-analytic comparison with children from the general population and children at risk who remained at home. Child. Maltreatment 2016, 21, 198–217. [Google Scholar] [CrossRef] [PubMed]
- Monson, K.; Moeller-Saxone, K.; Humphreys, C.; Harvey, C.; Herrman, H. Promoting mental health in out of home care in Australia. Health Promot. Int. 2019. [Google Scholar] [CrossRef]
- Turney, K.; Wildeman, C. Mental and Physical Health of Children in Foster Care. Pediatrics 2016, 138, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gribble, K.D.; Gallagher, M. Rights of children in relation to breastfeeding in child protection cases. Br. J. Soc. Work 2014, 44, 434–450. [Google Scholar] [CrossRef]
- Strathearn, L.; Mamun, A.A.; Najman, J.M.; O’Callaghan, M.J. Does breastfeeding protect against substantiated child abuse and neglect? A 15-year cohort study. Pediatrics 2009, 123, 483–493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gribble, K.D.; McGrath, M.; MacLaine, A.; Lhotska, L. Supporting breastfeeding in emergencies: Protecting women’s reproductive rights and maternal and infant health. Disasters 2011, 35, 720–738. [Google Scholar] [CrossRef]
- Goel, N.; Beasley, D.; Rajkumar, V.; Banerjee, S. Perinatal outcome of illicit substance use in pregnancy—Comparative and contemporary socio-clinical profile in the UK. Eur. J. Pediatrics 2011, 170, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Welle-Strand, G.K.; Skurtveit, S.; Jansson, L.M.; Bakstad, B.; Bjarkø, L.; Ravndal, E. Breastfeeding reduces the need for withdrawal treatment in opioid-exposed infants. Acta Paediatr. 2013, 102, 1060–1066. [Google Scholar] [CrossRef]
- ABM Clinical Protocol #21: Guidelines for Breastfeeding and Substance Use or Substance Use Disorder, Revised 2015. Breastfeed. Med. 2015, 10, 135–141. [CrossRef] [Green Version]
- McGlothen, K.S.; Cleveland, L.M. The right to mother’s milk: A call for social justice that encourages breastfeeding for women receiving medication-assisted treatment for opioid use disorder. J. Hum. Lact. 2018, 34, 799–803. [Google Scholar] [CrossRef] [PubMed]
- McGlothen, K.S.; Gill, S.; Cleveland, L.M. Infant feeding decisions among mothers who receive medication-assisted treatment for opioid use disorder. J. Obstet. Gynecol. Neonatal Nurs. 2017, 46, S49–S50. [Google Scholar] [CrossRef] [Green Version]
- Köhler, M.; Emmelin, M.; Hjern, A.; Rosvall, M. Children in family foster care have greater health risks and less involvement in Child Health Services. Acta Paediatr. 2015, 104, 508–513. [Google Scholar] [CrossRef]
- Alliance for Family Preservation and Restoration. Cases of Removals of Babies at Birth by FACS NSW; 2015. Available online: https://www.parliament.nsw.gov.au/lcdocs/other/10425/Answers%20to%20Questions%20on%20Notice%20-%20Alliance%20for%20Family%20Preservation%20and%20Restoration.pdf (accessed on 31 March 2021).
- Brown, J.D.; Bednar, L.M. Foster parent perceptions of placement breakdown. Child. Youth Serv. Rev. 2006, 28, 1497–1511. [Google Scholar] [CrossRef]
- Miller, L.; Randle, M.; Dolnicar, S. Carer factors associated with foster-placement success and breakdown. Br. J. Soc. Work 2019, 49, 503–522. [Google Scholar] [CrossRef]
- Randle, M.; Miller, L.; Dolnicar, S. What can agencies do to increase foster carer satisfaction? Child Fam. Soc. Work 2018, 23, 212–221. [Google Scholar] [CrossRef] [Green Version]
- Geiger, J.M.; Piel, M.H.; Julien-Chinn, F.J. Improving relationships in child welfare practice: Perspectives of foster care providers. Child Adolesc. Soc. Work J. 2017, 34, 23–33. [Google Scholar] [CrossRef]
- Burns, E.; Triandafilidis, Z. Taking the path of least resistance: A qualitative analysis of return to work or study while breastfeeding. Int. Breastfeed. J. 2019, 14, 15. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schafer, E.J.; Livingston, T.A.; Roig-Romero, R.M.; Wachira, M.; Louis-Jacques, A.F.; Marhefka, S.L. “Breast Is Best, But…” According to Childcare Administrators, Not Best for the Childcare Environment. Breastfeed. Med. 2021, 16, 21–28. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.P.; Javanparast, S.; McIntyre, E.; Craig, L.; Mortensen, K.; Koh, C. Discrimination against breastfeeding mothers in childcare. Aust. J. Labour Econ. 2013, 16, 65–90. [Google Scholar]
- MMWR. Perspectives in Disease Prevention and Health Promotion Update: Universal Precautions for Prevention of Transmission of Human Immunodeficiency Virus, Hepatitis B Virus, and Other Bloodborne Pathogens in Health-Care Settings. Morb. Mortal. Wkly. Rep. 1988, 37, 377–388. [Google Scholar]
- Lee, D.L.; Gurzo, K.; Nhan, L.; Homel Vitale, E.; Yoshida, S.; Ritchie, L.D. Nutrition Provided to Infants in Licensed Childcare Centers and Homes: A Descriptive Study. Matern. Child Health J. 2020, 24, 932–942. [Google Scholar] [CrossRef]
- Lucas, A.; McMahon, P.M.; Asling, M.B.; Knobloch, A.; Kosh, E.; Sims, K. Assessing Child Care Providers’ Knowledge and Attitudes Regarding Support of Breastfeeding in a Region with Low Breastfeeding Prevalence. J. Hum. Lact. 2013, 29, 556–563. [Google Scholar] [CrossRef] [PubMed]
- Batan, M.; Li, R.; Scanlon, K. Association of child care providers breastfeeding support with breastfeeding duration at 6 months. Matern. Child Health J. 2013, 17, 708–713. [Google Scholar] [CrossRef] [PubMed]
- Gribble, K.D.; Hausman, B.L. Milk Sharing and formula feeding: Infant feeding risks in comparative perspective? Australas. Med. J. 2012, 5, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Hotham, N.; Hotham, E. Drugs in breastfeeding. Aust. Prescr. 2015, 38, 156–159. [Google Scholar] [CrossRef] [Green Version]
- Datta, P.; Baker, T.; Hale, T.W. Balancing the Use of Medications While Maintaining Breastfeeding. Clin. Perinatol. 2019, 46, 367–382. [Google Scholar] [CrossRef]
- Blandthorn, J.; James, K.; Bowman, E.; Bonomo, Y.; Amir, L.H. Two Case Studies Illustrating a Shared Decision-Making Approach to Illicit Methamphetamine Use and Breastfeeding. Breastfeed. Med. 2017, 12, 381–385. [Google Scholar] [CrossRef]
- Rowe, H.; Baker, T.; Hale, T.W. Maternal medication, drug use, and breastfeeding. Child Adolesc. Psychiatr. Clin. N. Am. 2015, 24, 1–20. [Google Scholar] [CrossRef]
- Holmes, A.P.; Schmidlin, H.N.; Kurzum, E.N. Breastfeeding Considerations for Mothers of Infants with Neonatal Abstinence Syndrome. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2017, 37, 861–869. [Google Scholar] [CrossRef]
- Tsai, L.C.; Doan, T.J. Breastfeeding among mothers on opioid maintenance treatment: A literature review. J. Hum. Lact. 2016, 32, 521–529. [Google Scholar] [CrossRef] [PubMed]
- Taylor, K.; Maguire, D. A Review of Feeding Practices in Infants with Neonatal Abstinence Syndrome. Adv. Neonatal Care 2020, 20, 430–439. [Google Scholar] [CrossRef]
- Hill, M. The MotherSafe experience: Demystifying perceptions regarding treating pregnant or breastfeeding mothers. J. Pharm. Pract. Res. 2015, 45, 72–75. [Google Scholar] [CrossRef]
- Australian College of Midwives. Scope of Practice for Midwives in Australia; ACM: New York, NY, USA, 2016. [Google Scholar]
- Madhoun, L.L.; Crerand, C.E.; Keim, S.; Baylis, A.L. Breast Milk Feeding Practices and Barriers and Supports Experienced by Mother–Infant Dyads with Cleft Lip and/or Palate. Cleft Palate Craniofac. J. 2019, 57, 477–486. [Google Scholar] [CrossRef] [PubMed]
- Douglas, T.; Redley, B.; Ottmann, G. The need to know: The information needs of parents of infants with an intellectual disability—A qualitative study. J. Adv. Nurs. 2017, 73, 2600–2608. [Google Scholar] [CrossRef]
- Casper, T.; Arbour, M.W. Identification of the Pregnant Woman Who Is Using Drugs: Implications for Perinatal and Neonatal Care. J. Midwifery Women’s Health 2013, 58, 697–701. [Google Scholar] [CrossRef] [PubMed]
- Newman, A.; Davies, G.A.; Dow, K.; Holmes, B.; Macdonald, J.; McKnight, S.; Newton, L. Rooming-in care for infants of opioid-dependent mothers: Implementation and evaluation at a tertiary care hospital. Can. Fam. Phys. 2015, 61, e555–e561. [Google Scholar]
- Holmes, A.V.; Atwood, E.C.; Whalen, B.; Beliveau, J.; Jarvis, J.D.; Matulis, J.C.; Ralston, S.L. Rooming-in to treat neonatal abstinence syndrome: Improved family-centered care at lower cost. Pediatrics 2016, 137, 137. [Google Scholar] [CrossRef] [Green Version]
- Shannon, J.; Peters, K.; Blythe, S. The Challenges to Promoting Attachment for Hospitalised Infants with NAS. Children 2021, 8, 167. [Google Scholar] [CrossRef]
- Williams, V.N.; Ayele, R.; Shimasaki, S.; Tung, G.J.; Olds, D. Risk assessment practices among home visiting nurses and child protection caseworkers in Colorado, United States: A qualitative investigation. Health Soc. Care Community 2019, 27, 1344–1352. [Google Scholar] [CrossRef]
- Kuluski, K.; Ho, J.W.; Hans, P.K.; Nelson, M.L. Community care for people with complex care needs: Bridging the gap between health and social care. Int. J. Integr. Care 2017, 17, 2. [Google Scholar] [CrossRef] [PubMed]
- Maruthappu, M.; Hasan, A.; Zeltner, T. Enablers and barriers in implementing integrated care. Health Syst. Reform 2015, 1, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Australian Government Department of Health. Australia’s Long Term National Health Plan; Australian Government Department of Health: Canberra, Australia, 2019.
- Trankle, S.A.; Usherwood, T.; Abbott, P.; Roberts, M.; Crampton, M.; Girgis, C.M.; Riskallah, J.; Chang, Y.; Saini, J.; Reath, J. Integrating health care in Australia: A qualitative evaluation. BMC Health Serv. Res. 2019, 19, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marks, A.; Wilkes, L.; Blythe, S.; Griffiths, R. A novice researcher’s reflection on recruiting participants for qualitative research. Nurse Res. 2017, 25, 34. [Google Scholar] [CrossRef]
- Filteau, J.; Coo, H.; Dow, K. Trends in incidence of neonatal abstinence syndrome in Canada and associated healthcare resource utilization. Drug Alcohol Depend. 2018, 185, 313–321. [Google Scholar] [CrossRef] [PubMed]
- Leech, A.A.; Cooper, W.O.; McNeer, E.; Scott, T.A.; Patrick, S.W. Neonatal Abstinence Syndrome In The United States, 2004–16: An examination of neonatal abstinence syndrome trends and incidence patterns across US census regions in the period 2004–16. Health Aff. 2020, 39, 764–767. [Google Scholar] [CrossRef]
- Representative for Children and Youth, British Columbia Ministry of Children and Family Development. Promoting Access to Breastfeeding in Child Welfare Matters; Representative for Children and Youth, British Columbia Ministry of Children and Family Development: Victoria, BC, Canada, 2018.



{kind=link}
{kind=link}
| Characteristic | n (%) | |
|---|---|---|
| (a) | ||
| Gender | Female | 178 (96.7%) |
| Male | 6 (3.3%) | |
| Age | 20–29 years | 12 (6.5%) |
| 30–39 years | 50 (27.2%) | |
| 40–49 years | 75 (41.3%) | |
| 50–59 years | 34 (18.5%) | |
| 60–69 years | 10 (5.4%) | |
| 70+ years | 2 (1.1%) | |
| Highest level of education completed | Primary School | 3 (1.6%) |
| Secondary School | 29 (15.8%) | |
| TAFE Qualification * | 67 (36.4%) | |
| Bachelor’s Degree | 61 (33.2%) | |
| Master’s Degree | 7 (3.8%) | |
| Doctoral Degree | 3 (1.6%) | |
| Other | 14 (7.6%) | |
| Duration of fostering experience | 1–3 years | 60 (32.6%) |
| 4–5 years | 38 (20.7%) | |
| 5–10 years | 46 (25.0%) | |
| 10–15 years | 18 (9.8%) | |
| 15+ years | 22 (12.0%) | |
| State or territory where fostered ^ | New South Wales | 49 (26.6%) |
| Western Australia | 42 (22.8%) | |
| Victoria | 29 (15.8%) | |
| South Australia | 26 (14.1%) | |
| Queensland | 20 (10.9%) | |
| Australian Capital Territory | 12 (6.5%) | |
| Northern Territory | 8 (4.3%) | |
| Tasmania | 4 (2.2%) | |
| Type/s of foster care authorization ^ | Long term | 148 (80.4%) |
| Short Term | 154 (83.7%) | |
| Crisis/Emergency | 130 (70.7%) | |
| Respite | 115 (62.5%) | |
| Specialised care of infants | 44 (23.9%) | |
| Other | 20 (10.9%) | |
| (b) & | ||
| Number of children under 12 months ever fostered | One | 43 (23.2%) |
| Two | 27 (14.6%) | |
| 3 or 4 | 39 (21.1%) | |
| 5 to 9 | 42 (22.7%) | |
| 10 to 19 | 15 (8.1%) | |
| 20 or more | 13 (7%) | |
| Number of infants placed with foster carers as newborns directly from hospital | None | 50 (27%) |
| One | 56 (30.3%) | |
| Two | 29 (15.7%) | |
| 3 or 4 | 22 (11.9%) | |
| 5 to 9 | 13 (7%) | |
| 10 to 19 | 5 (2.7%) | |
| 20 or more | 4 (2.2%) | |
| Number of infants under six months of age at placement with foster carers | None | 10 (5.4%) |
| One | 52 (28.1%) | |
| Two | 27 (14.6%) | |
| 3 or 4 | 37 (20%) | |
| 5 to 9 | 35 (18.9%) | |
| 10 to 19 | 11 (5.9%) | |
| 20 or more | 7 (3.8%) | |
| Total | 179 (96.8%) | |
| Concerned Foster Carers Who Had Received EBM (n = 47) | Concerned Foster Carers Who Had Not Received EBM (n = 137) | |
|---|---|---|
| Feed it to the infant anyway | 9 (23%) | 2 (5%) |
| Keep the milk, but do not give it to the infant | 6 (15%) | 41 (35%) |
| Discard the milk | 31 (80%) | 57 (48%) |
| Other | 2 (5%) | 28 (24%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blythe, S.; Peters, K.; Elcombe, E.; Burns, E.; Gribble, K. Australian Foster Carers’ Views and Concerns Regarding Maternal Drug Use and the Safety of Breastmilk. Children 2021, 8, 284. https://0-doi-org.brum.beds.ac.uk/10.3390/children8040284
Blythe S, Peters K, Elcombe E, Burns E, Gribble K. Australian Foster Carers’ Views and Concerns Regarding Maternal Drug Use and the Safety of Breastmilk. Children. 2021; 8(4):284. https://0-doi-org.brum.beds.ac.uk/10.3390/children8040284
Chicago/Turabian StyleBlythe, Stacy, Kath Peters, Emma Elcombe, Elaine Burns, and Karleen Gribble. 2021. "Australian Foster Carers’ Views and Concerns Regarding Maternal Drug Use and the Safety of Breastmilk" Children 8, no. 4: 284. https://0-doi-org.brum.beds.ac.uk/10.3390/children8040284