
Magnetic Resonance Imaging as the Primary Imaging Modality in Children Presenting with Inflammatory Nontraumatic Atlantoaxial Rotatory Subluxation


Abstract
:1. Introduction
2. Materials and Methods
2.1. MR Imaging
2.2. MRI Protocol
3. Results
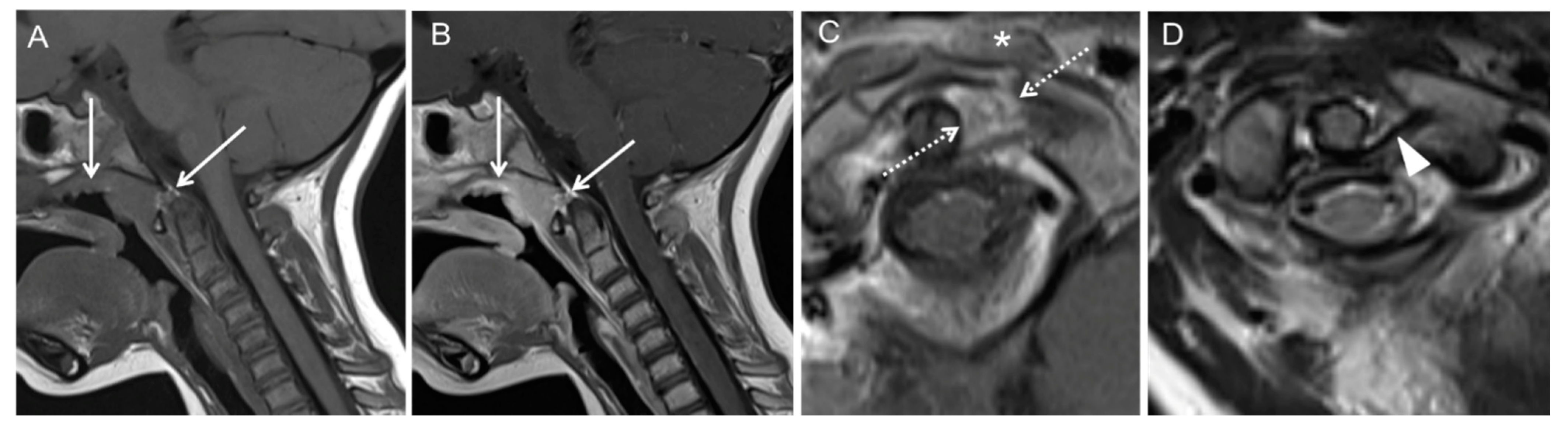
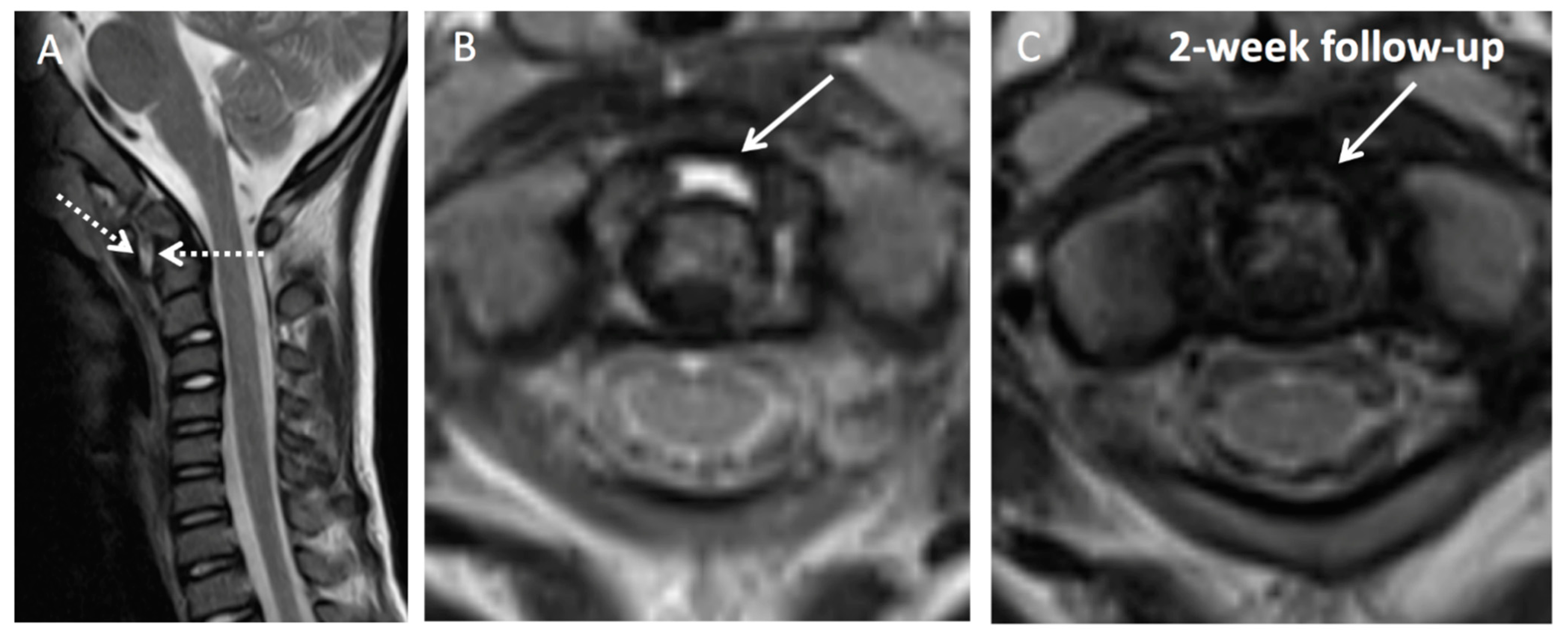
Illustration of Three Pediatric Cases of MRI in Inflammatory Nontraumatic Atlantoaxial Rotatory Subluxation
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Dirheimer, Y. The Craniovertebral Region in Chronic Inflammatory Rheumatic Diseases; Springer: Berlin/Heidelberg, Germany, 1977; ISBN 978-3-642-66605-6. [Google Scholar]
- Grisel, P. Enucleation de l’atlas et Torticollis Nasopharyngien. PresseMed 1930, 59, 1647–1648. [Google Scholar]
- Barcelos, A.C.E.S.; Patriota, G.C.; Netto, A.U. Nontraumatic Atlantoaxial Rotatory Subluxation: Grisel Syndrome. Case Report and Literature Review. Glob. Spine J. 2014, 4, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Spennato, P.; Nicosia, G.; Rapanà, A.; Cicala, D.; Donnianni, T.; Scala, S.; Aliberti, F.; Cinalli, G. Grisel Syndrome Following Adenoidectomy: Surgical Management in a Case with Delayed Diagnosis. World Neurosurg. 2015, 84, 1494.e7–1494.e12. [Google Scholar] [CrossRef]
- Pavlidis, E.; Copioli, C.; Spagnoli, C.; Mazzotta, S.; Ormitti, F.; Crisi, G.; Pisani, F. A Painful Stiff Neck Following an Ear, Nose, and Throat Surgical Procedure: Case Report. Neuropediatrics 2015, 46, 69–71. [Google Scholar] [CrossRef]
- Wood, A.J.; Singh-Grewal, D.; De, S.; Gunasekera, H. Kawasaki Disease Complicated by Subluxation of Cervical Vertebrae (Grisel Syndrome). Med. J. Aust. 2013, 199, 494–496. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, J.K.; Oh, C.H.; Park, H.-C.; Yoon, S.H. Grisel’s Syndrome Induced by Mycobacterium Tuberculosis. Korean J. Spine 2015, 12, 84–87. [Google Scholar] [CrossRef] [Green Version]
- Martins, J.; Almeida, S.; Nunes, P.; Prata, F.; Lobo, M.L.; Marques, J.G. Grisel Syndrome, Acute Otitis Media, and Temporo-Mandibular Reactive Arthritis: A Rare Association. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 1370–1373. [Google Scholar] [CrossRef] [Green Version]
- Gourin, C.G.; Kaper, B.; Abdu, W.A.; Donegan, J.O. Nontraumatic Atlanto-Axial Subluxation after Retropharyngeal Cellulitis: Grisel’s Syndrome. Am. J. Otolaryngol. 2002, 23, 60–65. [Google Scholar] [CrossRef]
- Wilson, B.C.; Jarvis, B.L.; Haydon, R.C. Nontraumatic Subluxation of the Atlantoaxial Joint: Grisel’s Syndrome. Ann. Otol. Rhinol. Laryngol. 1987, 96, 705–708. [Google Scholar] [CrossRef] [PubMed]
- Battiata, A.P.; Pazos, G. Grisel’s Syndrome: The Two-Hit Hypothesis—A Case Report and Literature Review. Ear Nose Throat J. 2004, 83, 553–555. [Google Scholar] [CrossRef] [Green Version]
- Kraft, M.; Tschopp, K. Evaluation of Persistent Torticollis Following Adenoidectomy. J. Laryngol. Otol. 2001, 115, 669–672. [Google Scholar] [CrossRef]
- Yu, K.K.; White, D.R.; Weissler, M.C.; Pillsbury, H.C. Nontraumatic Atlantoaxial Subluxation (Grisel Syndrome): A Rare Complication of Otolaryngological Procedures. Laryngoscope 2003, 113, 1047–1049. [Google Scholar] [CrossRef]
- Gray’s Anatomy: The Anatomical Basis of Clinical Practice, 39th ed.; Gray, H.; Standring, S.; Ellis, H.; Berkovitz, B.K.B. (Eds.) Elsevier Churchill Livingstone: Edinburgh, NY, USA, 2005; ISBN 978-0-443-07168-3. [Google Scholar]
- Park, S.-H.; Park, S.-H.; Lee, S.-H. Grisel Syndrome: Pathophysiological Evidence from Magnetic Resonance Imaging Findings. Ann. Rehabil. Med. 2013, 37, 713–716. [Google Scholar] [CrossRef] [PubMed]
- Harth, M.; Mayer, M.; Marzi, I.; Vogl, T.J. Lateral Torticollis on Plain Radiographs and MRI: Grisel Syndrome. Eur. Radiol. 2004, 14, 1713–1715. [Google Scholar] [CrossRef] [PubMed]
- Fielding, J.W.; Hawkins, R.J. Atlanto-Axial Rotatory Fixation. (Fixed Rotatory Subluxation of the Atlanto-Axial Joint). J. Bone Jt. Surg. Am. 1977, 59, 37–44. [Google Scholar] [CrossRef]
- Hannonen, J.; Perhomaa, M.; Salokorpi, N.; Serlo, W.; Sequeiros, R.B.; Sinikumpu, J. Interventional Magnetic Resonance Imaging as a Diagnostic and Therapeutic Method in Treating Acute Pediatric Atlantoaxial Rotatory Subluxation. Exp. Ther. Med. 2019, 18, 18–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ugur, H.C.; Cağlar, S.; Unlu, A.; Erdem, A.; Kanpolat, Y. Infection-Related Atlantoaxial Subluxation in Two Adults: Grisel Syndrome or Not? Acta Neurochir. 2003, 145, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Wurm, G.; Aichholzer, M.; Nussbaumer, K. Acquired Torticollis Due to Grisel’s Syndrome: Case Report and Follow-up of Non-Traumatic Atlantoaxial Rotatory Subluxation. Neuropediatrics 2004, 35, 134–138. [Google Scholar] [CrossRef]
- Panopalis, P.; Christopoulos, S.; Churchill-Smith, M.; Chankowsky, J.; Ménard, H.A. Grisel’s Syndrome: Non-Traumatic Subluxation of the Atlantoaxial Joint. J. Rheumatol. 2005, 32, 1619. [Google Scholar]
- Yamazaki, M.; Someya, Y.; Aramomi, M.; Masaki, Y.; Okawa, A.; Koda, M. Infection-Related Atlantoaxial Subluxation (Grisel Syndrome) in an Adult with Down Syndrome. Spine 2008, 33, E156–E160. [Google Scholar] [CrossRef]
- Salpietro, V.; Polizzi, A.; Granata, F.; Briuglia, S.; Mankad, K.; Ruggieri, M. Upper Respiratory Tract Infection and Torticollis in Children: Differential Diagnosis of Grisel’s Syndrome. Clin. Neuroradiol. 2012, 22, 351–353. [Google Scholar] [CrossRef]
- Di Cola, F.; Cutilli, T.; Paulis, D.D.; Galzio, R.J. Image-Guided Transoral Biopsy in a Boy with Grisel’s Syndrome. J. Clin. Neurosci. 2013, 20, 901–903. [Google Scholar] [CrossRef]
- Reichman, E.F.; Shah, J. Grisel Syndrome: An Unusual and Often Unrecognized Cause of Torticollis. Pediatr. Emerg. Care 2015, 31, 577–580. [Google Scholar] [CrossRef]
- Kourelis, K.; Haronis, V.; Konandreas, I.; Kontrafouri, A.; Asimakopoulos, A. Atypical Post-Adenoidectomy Grisel’s Syndrome in Crouzon Child with Kyphotic Skull Base. Auris Nasus Larynx 2015, 42, 416–418. [Google Scholar] [CrossRef]
- Allegrini, D.; Autelitano, A.; Nocerino, E.; Fogagnolo, P.; De Cillà, S.; Rossetti, L. Grisel’s Syndrome, a Rare Cause of Anomalous Head Posture in Children: A Case Report. BMC Ophthalmol. 2016, 16, 21. [Google Scholar] [CrossRef] [Green Version]
- Ozalp, H.; Hamzaoglu, V.; Avci, E.; Karatas, D.; Ismi, O.; Talas, D.U.; Bagdatoglu, C.; Dagtekin, A. Early Diagnosis of Grisel’s Syndrome in Children with Favorable Outcome. Childs Nerv. Syst. 2019, 35, 113–118. [Google Scholar] [CrossRef] [PubMed]
- Fath, L.; Cebula, H.; Santin, M.N.; Coca, A.; Debry, C.; Proust, F. The Grisel’s Syndrome: A Non-Traumatic Subluxation of the Atlantoaxial Joint. Neurochirurgie 2018, 64, 327–330. [Google Scholar] [CrossRef]
- Chua, A.J.K.; Tan, B.W.S.; Tan, T.Y.; Heah, H.H.W. Grisel’s Syndrome in an Adult after Endoscopic Nasopharyngectomy. Laryngoscope Investig. Otolaryngol. 2019, 4, 504–507. [Google Scholar] [CrossRef] [PubMed]
- Spinnato, P.; Aparisi Gomez, M.P.; Molinari, M.; Mercatelli, D.; Bazzocchi, A. Torticollis After a Somersault: A Case of Grisel’s Syndrome. Indian J. Pediatr. 2019, 86, 198–199. [Google Scholar] [CrossRef] [PubMed]
- Chryssikos, T.; Pratt, N.; Howie, B.; Mushlin, H.; Sansur, C. Open Reduction and Decompression of Atlantoaxial Subluxation with Basilar Impression Due to Grisel Syndrome Using the Cervical Management Base Unit. World Neurosurg. 2020, 138, 129–136. [Google Scholar] [CrossRef]
- Saunders, D.E.; Thompson, C.; Gunny, R.; Jones, R.; Cox, T.; Chong, W.K. Magnetic Resonance Imaging Protocols for Paediatric Neuroradiology. Pediatr. Radiol. 2007, 37, 789–797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Z.; Chen, Y.A.; Chow, D.; Talbott, J.; Glastonbury, C.; Shah, V. Practical Applications of CISS MRI in Spine Imaging. Eur. J. Radiol. Open 2019, 6, 231–242. [Google Scholar] [CrossRef] [Green Version]
- Bissonnette, B. (Ed.) Syndromes: Rapid Recognition and Perioperative Implications, 2nd ed.; McGraw-Hill Education: New York, NY, USA, 2019; ISBN 978-1-259-86178-9. [Google Scholar]
- Banerjee, P.; Thomas, M. CT Scans to Exclude Spine Fractures in Children after Negative Radiographs May Lead to Increase in Future Cancer Risk. Eur. J. Orthop. Surg. Traumatol. 2019, 29, 983–988. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.; Elliston, C.; Hall, E.; Berdon, W. Estimated Risks of Radiation-Induced Fatal Cancer from Pediatric CT. AJR Am. J. Roentgenol. 2001, 176, 289–296. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, S.-Z.; Zhu, M.; Bulas, D. Techniques for Minimizing Sedation in Pediatric MRI. J. Magn. Reson. Imaging 2019, 50, 1047–1054. [Google Scholar] [CrossRef] [PubMed]
- Benedetti, P.F.; Fahr, L.M.; Kuhns, L.R.; Hayman, L.A. MR Imaging Findings in Spinal Ligamentous Injury. Am. J. Roentgenol. 2000, 175, 661–665. [Google Scholar] [CrossRef] [Green Version]
- Debnam, J.M.; Guha-Thakurta, N. Retropharyngeal and Prevertebral Spaces: Anatomic Imaging and Diagnosis. Otolaryngol. Clin. N. Am. 2012, 45, 1293–1310. [Google Scholar] [CrossRef] [Green Version]
- Eid, M.; Abougabal, A. Subtraction Images: A Really Helpful Tool in Non-Vascular MRI. Egypt. J. Radiol. Nucl. Med. 2014, 45, 909–919. [Google Scholar] [CrossRef] [Green Version]
- Delfaut, E.M.; Beltran, J.; Johnson, G.; Rousseau, J.; Marchandise, X.; Cotten, A. Fat Suppression in MR Imaging: Techniques and Pitfalls. RadioGraphics 1999, 19, 373–382. [Google Scholar] [CrossRef] [PubMed]
- Ma, J. Dixon Techniques for Water and Fat Imaging. J. Magn. Reson. Imaging 2008, 28, 543–558. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sequence | Plane | Slice Thickness | Pixel Size | TR; TE; Number of Averages | Trans-mitting Coil | Receiving Coil | Comment |
|---|---|---|---|---|---|---|---|
| 2D T2w TSE | sagittal | 3 mm | 1 mm | 3800; 84; 2 | body | neck | Aim to include nasopharyngeal and upper neck soft tissue, mastoid air cells and if possible paranasal sinus FOV |
| 2D TIRM | coronal; planning on sagittal plane, block position angled parallel to cervical spine | 3 mm | 1 mm | 3800; 33; 2 | body | neck | Short inversion time (160 ms) for fat suppression of bone marrow |
| 2D T1w TSE | sagittal | 3 mm | 1 mm | 550; 9.5; 3 | body | neck | |
| 2D T2w TSE | axial; planning on sagittal plane, block position angled perpendicular to cervical spine | 3 mm | 1 mm | 4500; 84; 2 | body | neck | Include at least craniocervical transition to C3 and any pathological region on sagittal plane |
| 2D T1w TSE post CA | sagittal | 3 mm | 1 mm | 550; 9.5; 3 | body | neck | |
| 2D T1w TSE post CA | axial; planning on sagittal plane, block position angled perpendicular to cervical spine | 3 mm | 1 mm | 550; 9.9; 2 | body | neck | include at least craniocervical transition to C3 and any pathological region on sagittal plane |
| 2D T1w TSE post CA | coronal; planning on sagittal plane, block position angled parallel to cervical spine | 3 mm | 1 mm | 524; 17; 2 | body | neck |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wenger, K.J.; Hattingen, E.; Porto, L. Magnetic Resonance Imaging as the Primary Imaging Modality in Children Presenting with Inflammatory Nontraumatic Atlantoaxial Rotatory Subluxation. Children 2021, 8, 329. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050329
Wenger KJ, Hattingen E, Porto L. Magnetic Resonance Imaging as the Primary Imaging Modality in Children Presenting with Inflammatory Nontraumatic Atlantoaxial Rotatory Subluxation. Children. 2021; 8(5):329. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050329
Chicago/Turabian StyleWenger, Katharina J., Elke Hattingen, and Luciana Porto. 2021. "Magnetic Resonance Imaging as the Primary Imaging Modality in Children Presenting with Inflammatory Nontraumatic Atlantoaxial Rotatory Subluxation" Children 8, no. 5: 329. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050329