
Impaired Glucose-Insulin Metabolism in Multisystem Inflammatory Syndrome Related to SARS-CoV-2 in Children

 , , ,
, , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects
2.2. Measurements and Statistical Analysis
- Homeostasis model analysis—insulin resistance (HOMA-IR) index, defined as ([fasting plasma insulin (mU/L) × fasting plasma glucose (mg/dL)]/405) [21]; the cutoff point for pathological IR was set at the 97.5th percentile of the HOMA-IR distribution in a representative group of Italian healthy children and adolescents grouped by sex and pubertal stage [22].
- Average glucose;
- Glucose standard deviation (SD);
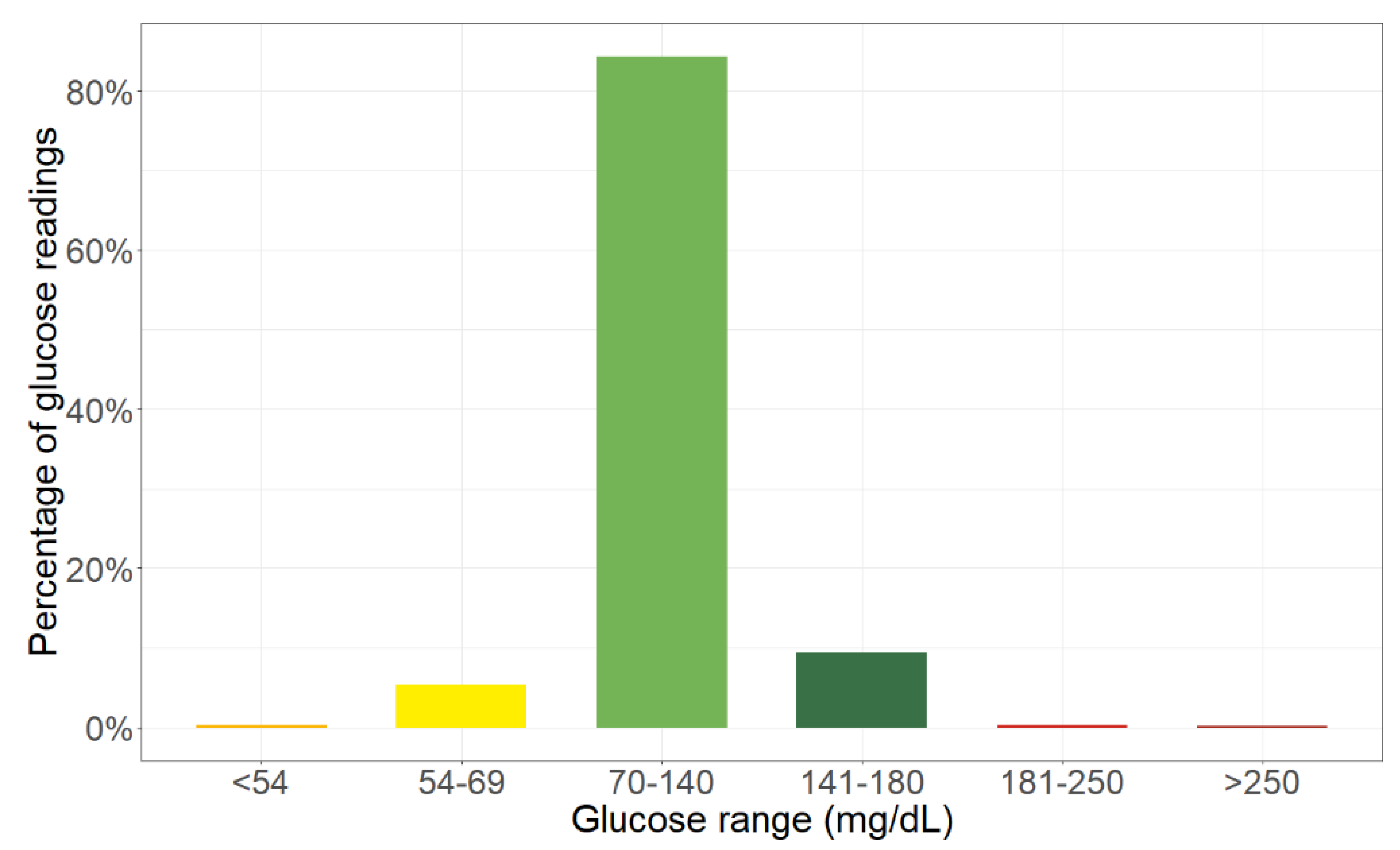
- Time below range (TBR), i.e., the percentage of glucose readings under 70 mg/dL, which can be further divided into time slightly below range in the 54–69 mg/dL range, and time severely below range under 54 mg/dL;
- Time in range (TIR), i.e., the percentage of glucose readings in the 70–180 mg/dL range, which can be further divided into time in the 70–140 mg/dL target range (TIT), and time in the 141–180 mg/dL range;
- Time above range (TAR), i.e., the percentage of glucose readings over 180 mg/dL, which can be further divided into Time slightly above range in the 181–250 mg/dL range, and time severely above range over 250 mg/dL.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Shrestha, E.; Charkviani, M.; Musurakis, C.; Kansakar, A.R.; Devkota, A.; Banjade, R.; Pudasainee, P.; Chitrakar, S.; Sharma, A.; Sous, M.; et al. Type 2 Diabetes Is Associated with Increased Risk of Critical Respiratory Illness in Patients COVID-19 in a Community Hospital. Obes. Med. 2020, 100316. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.-H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280.e8. [Google Scholar] [CrossRef]
- Adeyinka, A.; Bailey, K.; Pierre, L.; Kondamudi, N. COVID 19 Infection: Pediatric Perspectives. J. Am. Coll. Emerg. Physicians Open 2021, 2. [Google Scholar] [CrossRef]
- Syangtan, G.; Bista, S.; Dawadi, P.; Rayamajhee, B.; Shrestha, L.B.; Tuladhar, R.; Joshi, D.R. Asymptomatic SARS-CoV-2 Carriers: A Systematic Review and Meta-Analysis. Front. Public Health 2021, 8. [Google Scholar] [CrossRef]
- Bernardino, F.B.S.; Alencastro, L.C.D.S.; da Silva, R.A.; Ribeiro, A.D.D.N.; Castilho, G.R.D.C.; Gaíva, M.A.M. Epidemiological Profile of Children and Adolescents with COVID-19: A Scoping Review. Rev. Bras. Enferm. 2021, 74. [Google Scholar] [CrossRef] [PubMed]
- Shahin, W.; Rabie, W.; Alyossof, O.; Alasiri, M.; Alfaki, M.; Mahmoud, E.; Hijazi, M.; Faraidi, H.E.; Alahmari, H. COVID-19 in Children Ranging from Asymptomatic to a Multi-System Inflammatory Disease: A Single-Center Study. Saudi Med. J. 2021, 42, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Vogel, T.P.; Top, K.A.; Karatzios, C.; Hilmers, D.C.; Tapia, L.I.; Moceri, P.; Giovannini-Chami, L.; Wood, N.; Chandler, R.E.; Klein, N.P.; et al. Multisystem Inflammatory Syndrome in Children and Adults (MIS-C/A): Case Definition & Guidelines for Data Collection, Analysis, and Presentation of Immunization Safety Data. Vaccine 2021. [Google Scholar] [CrossRef]
- Hoste, L.; Van Paemel, R.; Haerynck, F. Multisystem Inflammatory Syndrome in Children Related to COVID-19: A Systematic Review. Eur. J. Pediatr. 2021. [Google Scholar] [CrossRef]
- Cattalini, M.; Taddio, A.; Bracaglia, C.; Cimaz, R.; Paolera, S.D.; Filocamo, G.; La Torre, F.; Lattanzi, B.; Marchesi, A.; Simonini, G.; et al. Childhood Multisystem Inflammatory Syndrome Associated with COVID-19 (MIS-C): A Diagnostic and Treatment Guidance from the Rheumatology Study Group of the Italian Society of Pediatrics. Ital. J. Pediatr. 2021, 47, 24. [Google Scholar] [CrossRef]
- CDC Multisystem Inflammatory Syndrome in Children (MIS-C). Available online: https://www.cdc.gov/mis-c/hcp/ (accessed on 1 March 2021).
- Montori, V.M.; Bistrian, B.R.; McMahon, M.M. Hyperglycemia in Acutely Ill Patients. JAMA 2002, 288, 2167–2169. [Google Scholar] [CrossRef]
- Annane, D.; Melchior, J.C. Hormone Replacement Therapy for the Critically Ill. Crit. Care Med. 2003, 31, 634–635. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Li, T.; Fang, F.; Zhang, Y.; Faramand, A. Tight Glycemic Control in Critically Ill Pediatric Patients: A Systematic Review and Meta-Analysis. Crit. Care 2018, 22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elkon, B.; Cambrin, J.R.; Hirshberg, E.; Bratton, S.L. Hyperglycemia: An Independent Risk Factor for Poor Outcome in Children With Traumatic Brain Injury*. Pediatr. Crit. Care Med. 2014, 15, 623–631. [Google Scholar] [CrossRef]
- Naranje, K.M.; Poddar, B.; Bhriguvanshi, A.; Lal, R.; Azim, A.; Singh, R.K.; Gurjar, M.; Baronia, A.K. Blood Glucose Variability and Outcomes in Critically Ill Children. Indian J. Crit. Care Med. 2017, 21, 122–126. [Google Scholar] [CrossRef] [PubMed]
- FreeStyle Libre 14-day System|Glucose Sensor & Reader|FreeStyleLibre.us. Available online: https://www.freestylelibre.us/ (accessed on 29 September 2020).
- Marshall, W.A.; Tanner, J.M. Variations in Pattern of Pubertal Changes in Girls. Arch. Dis. Child 1969, 44, 291–303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marshall, W.A.; Tanner, J.M. Variations in the Pattern of Pubertal Changes in Boys. Arch. Dis. Child 1970, 45, 13–23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Onis, M.; Onyango, A.W.; Borghi, E.; Siyam, A.; Nishida, C.; Siekmann, J. Development of a WHO Growth Reference for School-Aged Children and Adolescents. Bull. World Health Organ. 2007, 85, 660–667. [Google Scholar] [CrossRef] [PubMed]
- Calcaterra, V.; Montalbano, C.; de Silvestri, A.; Pelizzo, G.; Regalbuto, C.; Paganelli, V.; Albertini, R.; Cave, F.D.; Larizza, D.; Cena, H. Triglyceride Glucose Index as a Surrogate Measure of Insulin Sensitivity in a Caucasian Pediatric Population. J. Clin. Res. Pediatr. Endocrinol. 2019. [Google Scholar] [CrossRef] [PubMed]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis Model Assessment: Insulin Resistance and Beta-Cell Function from Fasting Plasma Glucose and Insulin Concentrations in Man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- d’Annunzio, G.; Vanelli, M.; Pistorio, A.; Minuto, N.; Bergamino, L.; Iafusco, D.; Lorini, R. Diabetes Study Group of the Italian Society for Pediatric Endocrinology and Diabetes Insulin Resistance and Secretion Indexes in Healthy Italian Children and Adolescents: A Multicentre Study. Acta Biomed. 2009, 80, 21–28. [Google Scholar] [PubMed]
- Simental-Mendía, L.E.; Rodríguez-Morán, M.; Guerrero-Romero, F. The Product of Fasting Glucose and Triglycerides As Surrogate for Identifying Insulin Resistance in Apparently Healthy Subjects. Metab. Syndr. Relat. Disord. 2008, 6, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Navarro-González, D.; Sánchez-Íñigo, L.; Pastrana-Delgado, J.; Fernández-Montero, A.; Martinez, J.A. Triglyceride–Glucose Index (TyG Index) in Comparison with Fasting Plasma Glucose Improved Diabetes Prediction in Patients with Normal Fasting Glucose: The Vascular-Metabolic CUN Cohort. Prev. Med. 2016, 86, 99–105. [Google Scholar] [CrossRef]
- Vieira-Ribeiro, S.A.; Fonseca, P.C.A.; Andreoli, C.S.; Ribeiro, A.Q.; Hermsdorff, H.H.M.; Pereira, P.F.; Priore, S.E.; Franceschini, S.C.C.; Vieira-Ribeiro, S.A.; Fonseca, P.C.A.; et al. The TyG Index Cutoff Point and Its Association with Body Adiposity and Lifestyle in Children. J. Pediatr. 2019, 95, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Croux, C.; Dehon, C. Influence Functions of the Spearman and Kendall Correlation Measures. Stat. Methods Appl. 2010, 19, 497–515. [Google Scholar] [CrossRef] [Green Version]
- Battelino, T.; Danne, T.; Bergenstal, R.M.; Amiel, S.A.; Beck, R.; Biester, T.; Bosi, E.; Buckingham, B.A.; Cefalu, W.T.; Close, K.L.; et al. Clinical Targets for Continuous Glucose Monitoring Data Interpretation: Recommendations From the International Consensus on Time in Range. Diabetes Care 2019. [Google Scholar] [CrossRef] [Green Version]
- Limonta, A.; Gastaldi, G.; Heidegger, C.P.; Pichard, C. Insulin therapy and parenteral nutrition in intensive care: Practical aspects. Rev. Med. Suisse 2015, 11, 728–730, 732. [Google Scholar]
- Shrestha, G.S.; Khanal, S.; Sharma, S.; Nepal, G. COVID-19: Current Understanding of Pathophysiology. J. Nepal Health Res. Counc. 2020, 18, 351–359. [Google Scholar] [CrossRef]
- Mishra, D.; Dey, C.S. Type-2 Diabetes, a Co-Morbidity in Covid-19: Does Insulin Signaling Matter? Biochem. Soc. Trans. 2021. [Google Scholar] [CrossRef] [PubMed]
- Jia, X.; Gesualdo, P.; Rasmussen, C.G.; Alkanani, A.A.; He, L.; Dong, F.; Rewers, M.J.; Michels, A.W.; Yu, L. Prevalence of SARS-CoV-2 Antibodies in Children and Adults with Type 1 Diabetes. Diabetes Technol. Ther. 2021. [Google Scholar] [CrossRef]
- Bello, B.; Useh, U. COVID-19: Are Non-Communicable Diseases Risk Factors for Its Severity? Am. J. Health Promot. 2021, 0890117121990518. [Google Scholar] [CrossRef]
- Vargas-Vázquez, A.; Bello-Chavolla, O.Y.; Ortiz-Brizuela, E.; Campos-Muñoz, A.; Mehta, R.; Villanueva-Reza, M.; Bahena-López, J.P.; Antonio-Villa, N.E.; González-Lara, M.F.; Ponce de León, A.; et al. Impact of Undiagnosed Type 2 Diabetes and Pre-Diabetes on Severity and Mortality for SARS-CoV-2 Infection. BMJ Open Diabetes Res. Care 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Roberts, J.; Pritchard, A.L.; Treweeke, A.T.; Rossi, A.G.; Brace, N.; Cahill, P.; MacRury, S.M.; Wei, J.; Megson, I.L. Why Is COVID-19 More Severe in Patients With Diabetes? The Role of Angiotensin-Converting Enzyme 2, Endothelial Dysfunction and the Immunoinflammatory System. Front. Cardiovasc. Med. 2021, 7. [Google Scholar] [CrossRef]
- Nielsen-Saines, K.; Li, E.; Olivera, A.M.; Martin-Blais, R.; Bulut, Y. Case Report: Insulin-Dependent Diabetes Mellitus and Diabetic Keto-Acidosis in a Child With COVID-19. Front. Pediatr. 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Beliard, K.; Ebekozien, O.; Demeterco-Berggren, C.; Alonso, G.T.; Gallagher, M.P.; Clements, M.; Rapaport, R. Increased DKA at Presentation among Newly Diagnosed Type 1 Diabetes Patients with or without COVID-19: Data from a Multi-Site Surveillance Registry. J. Diabetes 2021, 13, 270–272. [Google Scholar] [CrossRef]
- Chen, X.; Chen, Z.; Azman, A.S.; Deng, X.; Sun, R.; Zhao, Z.; Zheng, N.; Chen, X.; Lu, W.; Zhuang, T.; et al. Serological Evidence of Human Infection with SARS-CoV-2: A Systematic Review and Meta-Analysis. Lancet Glob. Health 2021, 9, e598–e609. [Google Scholar] [CrossRef]
- Yang, H.; Lyu, Y.; Hou, F. SARS-CoV-2 Infection and the Antiviral Innate Immune Response. J. Mol. Cell Biol. 2020. [Google Scholar] [CrossRef]
- Mazori, A.Y.; Bass, I.R.; Chan, L.; Mathews, K.S.; Altman, D.R.; Saha, A.; Soh, H.; Wen, H.H.; Bose, S.; Leven, E.; et al. Hyperglycemia Is Associated With Increased Mortality in Critically Ill Patients With COVID-19. Endocr. Pract. 2021, 27, 95–100. [Google Scholar] [CrossRef] [PubMed]
- Krinsley, J.S.; Rule, P.; Pappy, L.; Ahmed, A.; Huley-Rodrigues, C.; Prevedello, D.; Preiser, J.-C. The Interaction of Acute and Chronic Glycemia on the Relationship of Hyperglycemia, Hypoglycemia, and Glucose Variability to Mortality in the Critically Ill. Crit. Care Med. 2020, 48, 1744–1751. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Liu, Z. Effect of Hyperglycemia on All-Cause Mortality from Pediatric Brain Injury: A Systematic Review and Meta-Analysis. Medicine 2020, 99, e23307. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Summary Statistics |
|---|---|
| Sex | Female: 7 (23.33%) Male: 23 (76.67%) |
| Age (years) | 10.68 ± 7.25 |
| BMI (Kg/m2) | 17.70 ± 3.99 |
| BMI z-score | 0.03 ± 1.49 |
| HbA1c (%) | 5.20 ± 0.20 |
| HbA1c (mmol/mol) | 33.00 ± 2.25 |
| FPG (mg/dL) | 111.00 ± 31.00 |
| FPI (µU/mL) | 21.95 ± 11.50 |
| TG (mg/dL) | 190.00 ± 177.25 |
| HOMA-IR index | 5.15 ± 5.69 |
| TyG index | 9.20 ± 0.73 |
| Total cholesterol (mg/dL) | 118.00 ± 72.00 |
| HDL cholesterol (mg/dL) | 17.00 ± 21.00 |
| TSH (mIU/L) | 2.16 ± 1.81 |
| GGT (IU/L) | 26.50 ± 38.75 |
| ALT (IU/L) | 31.00 ± 45.50 |
| Creatine kinase (IU/L) | 68.00 ± 102.00 |
| Albumin (g/L) | 25.50 ± 7.50 |
| Sodium (mEq/L) | 132.00 ± 5.00 |
| Potassium (mEq/L) | 3.50 ± 0.90 |
| Ferritin (µg/L) | 745.00 ± 1259.25 |
| IL-6 (ng/L) | 83.00 ± 208.50 |
| C-reactive protein (mg/dL) | 236.50 ± 176.00 |
| Procalcitonin (µg/L) | 6.2 ± 11.20 |
| NT-proBNP (ng/L) | 7554.00 ± 11,143.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Calcaterra, V.; Bosoni, P.; Dilillo, D.; Mannarino, S.; Fiori, L.; Fabiano, V.; Carlucci, P.; Di Profio, E.; Verduci, E.; Mameli, C.; et al. Impaired Glucose-Insulin Metabolism in Multisystem Inflammatory Syndrome Related to SARS-CoV-2 in Children. Children 2021, 8, 384. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050384
Calcaterra V, Bosoni P, Dilillo D, Mannarino S, Fiori L, Fabiano V, Carlucci P, Di Profio E, Verduci E, Mameli C, et al. Impaired Glucose-Insulin Metabolism in Multisystem Inflammatory Syndrome Related to SARS-CoV-2 in Children. Children. 2021; 8(5):384. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050384
Chicago/Turabian StyleCalcaterra, Valeria, Pietro Bosoni, Dario Dilillo, Savina Mannarino, Laura Fiori, Valentina Fabiano, Patrizia Carlucci, Elisabetta Di Profio, Elvira Verduci, Chiara Mameli, and et al. 2021. "Impaired Glucose-Insulin Metabolism in Multisystem Inflammatory Syndrome Related to SARS-CoV-2 in Children" Children 8, no. 5: 384. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050384