
Neonates with Maternal Colonization of Carbapenemase-Producing, Carbapenem-Resistant Enterobacteriaceae: A Mini-Review and a Suggested Guide for Preventing Neonatal Infection


Abstract
:1. Introduction
1.1. Definition of Carbapenem-Resistant Enterobacteriaceae and Terminology
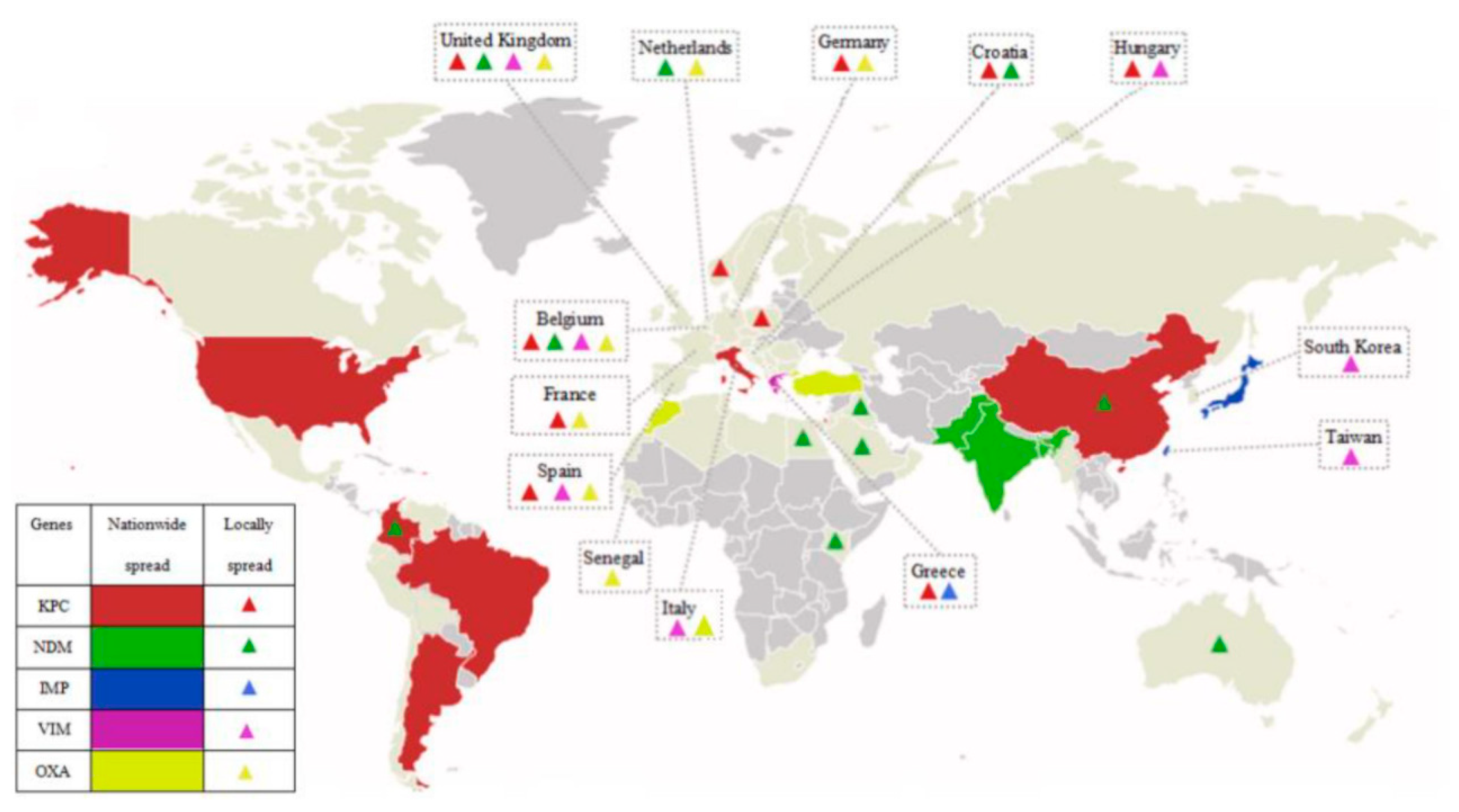
1.2. The Scope of the Problem Globally
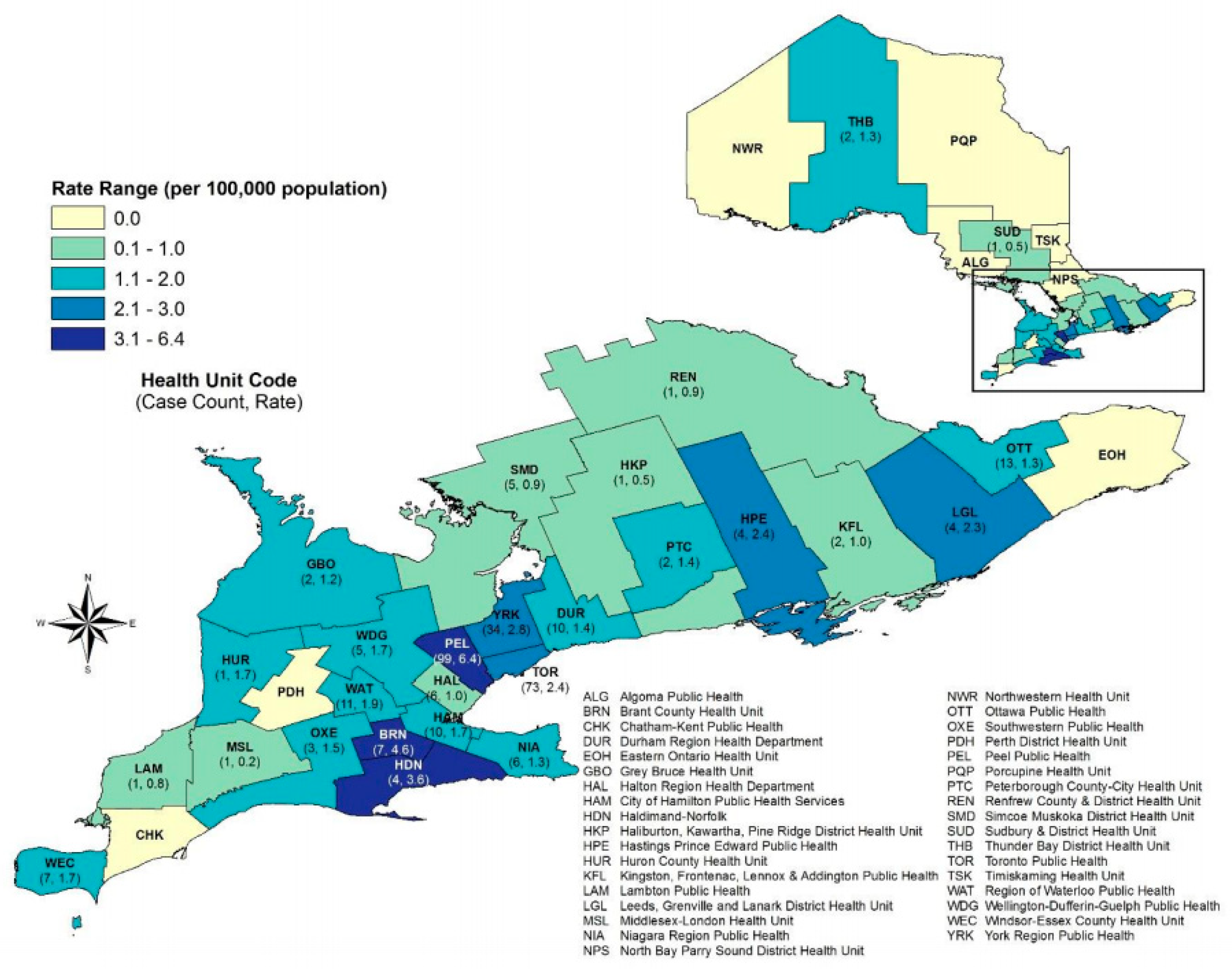
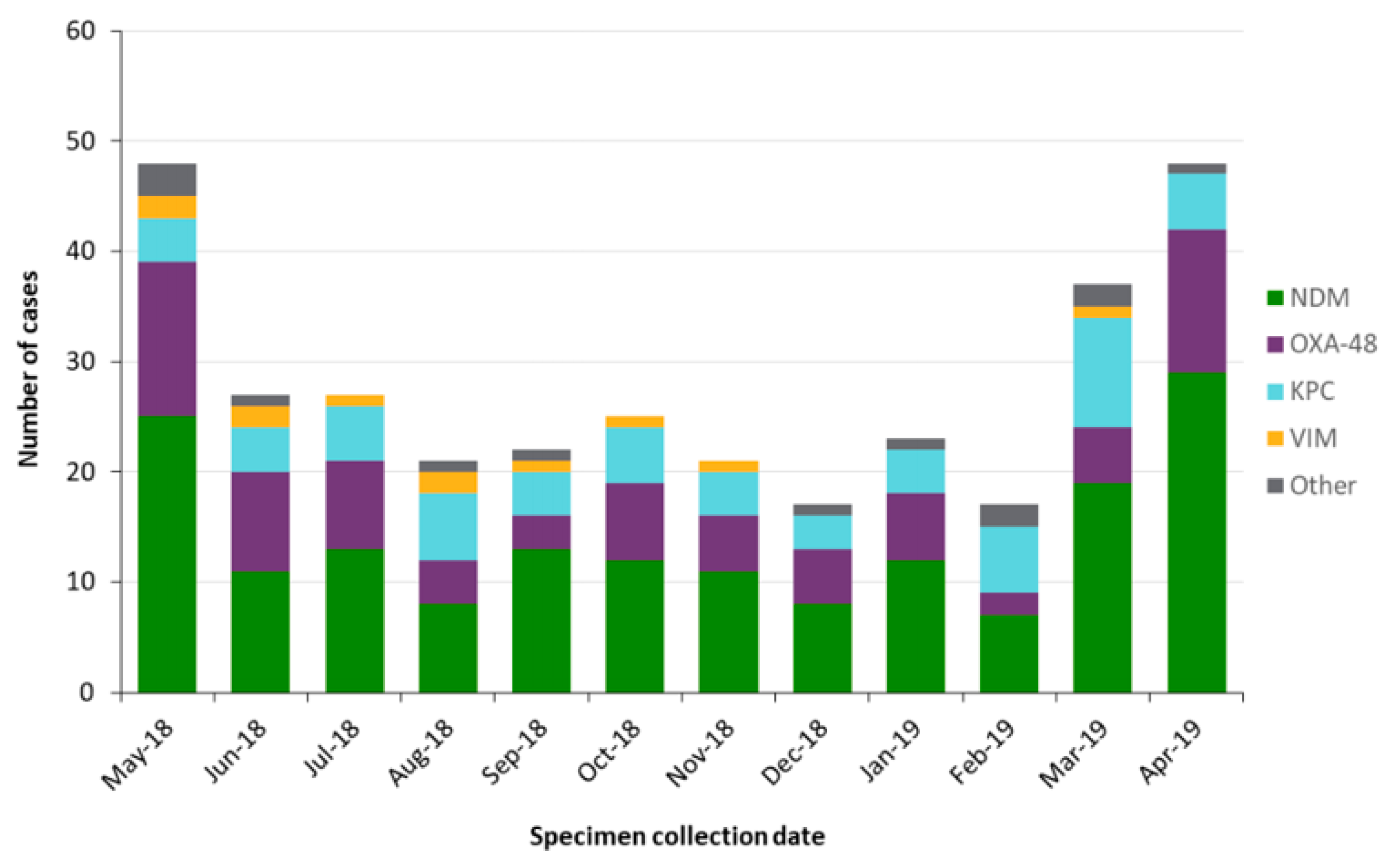
1.3. The Scope of the Problem in Canada
1.4. Risk Factors for CPE and Implications for Neonates Admitted to the Intensive Care Unit
1.5. Clinical Disease
2. Review of the Medical Literature of CPE in Neonates
Aim
3. A Glimpse into Our Local Experience
4. Discussion
- -
- Contact precautions were observed with the medical team using personal protective equipment of gloves and gown.
- -
- Dedicated equipment used with the neonates were kept in their isolation room and cleaned there. The incubators required two-step cleaning when they were changed. It was preferable to change the incubators during the workweek and not weekends to facilitate infection prevention and control inspection of the incubator units prior to and after they were cleaned. Environmental swabs were taken. We left the cleaned incubators (the changed ones) aside until culture results were available. We ensured documentation of the incubator number in the baby’s chart.
- -
- All bodily fluids were secured in their isolation room and disposed of only after being placed in a closed bag.
- -
- Strict hand hygiene was observed for staff and parents with alcohol-based hand rub.
- -
- Breastfeeding was not contraindicated. The mother’s own milk was stored in the refrigerator in the babies’ room. Milk that required fortification (due to prematurity) was sent to the milk preparation room after education of the milk preparation staff for contact precautions as parents would have handled the bottles. Parental bathroom use was restricted to a single bathroom for the entire NICU stay, and no one else was allowed to use this bathroom. This washroom received daily cleaning, and hand sink drains were treated with RESCUETM disinfectant daily. This disinfectant cleaner is bactericidal to NDM-1 bacteria [39].
- -
- The family did not use the family room as this was a shared space with other families. The family was asked to inform NICU of any development of diarrhea. They were asked to not visit when experiencing diarrhea.
- -
- All relevant staff was aware of the need for the cleaning protocol for equipment and the room once discharged.
- -
- Neonates remained on contact precautions for the duration of their stay due to ongoing exposure.
- -
- Appointments were made towards the end of the workday, and so the chance of interaction with and the chance of spread to other families was reduced.
- -
- Once they arrived at the clinic, they were placed immediately in the identified room and not in the waiting area.
- -
- Rooms and equipment were identified specifically for the visit, and these were deep-cleaned with hospital-approved disinfectant. At our institution, we use an accelerated hydrogen-based product. Rooms were cleaned prior to the next day and before the next use.
- -
- Personal protective equipment was used by the staff directly in contact with the family.
- -
- A specified bathroom was identified for their use only and deep-cleaned prior to use again.
- -
- Education of staff as a multidisciplinary team and parents is an essential part of the process for compliance to policies.
Clinical Implications
- -
- Isolation of parents and bathroom restrictions.
- -
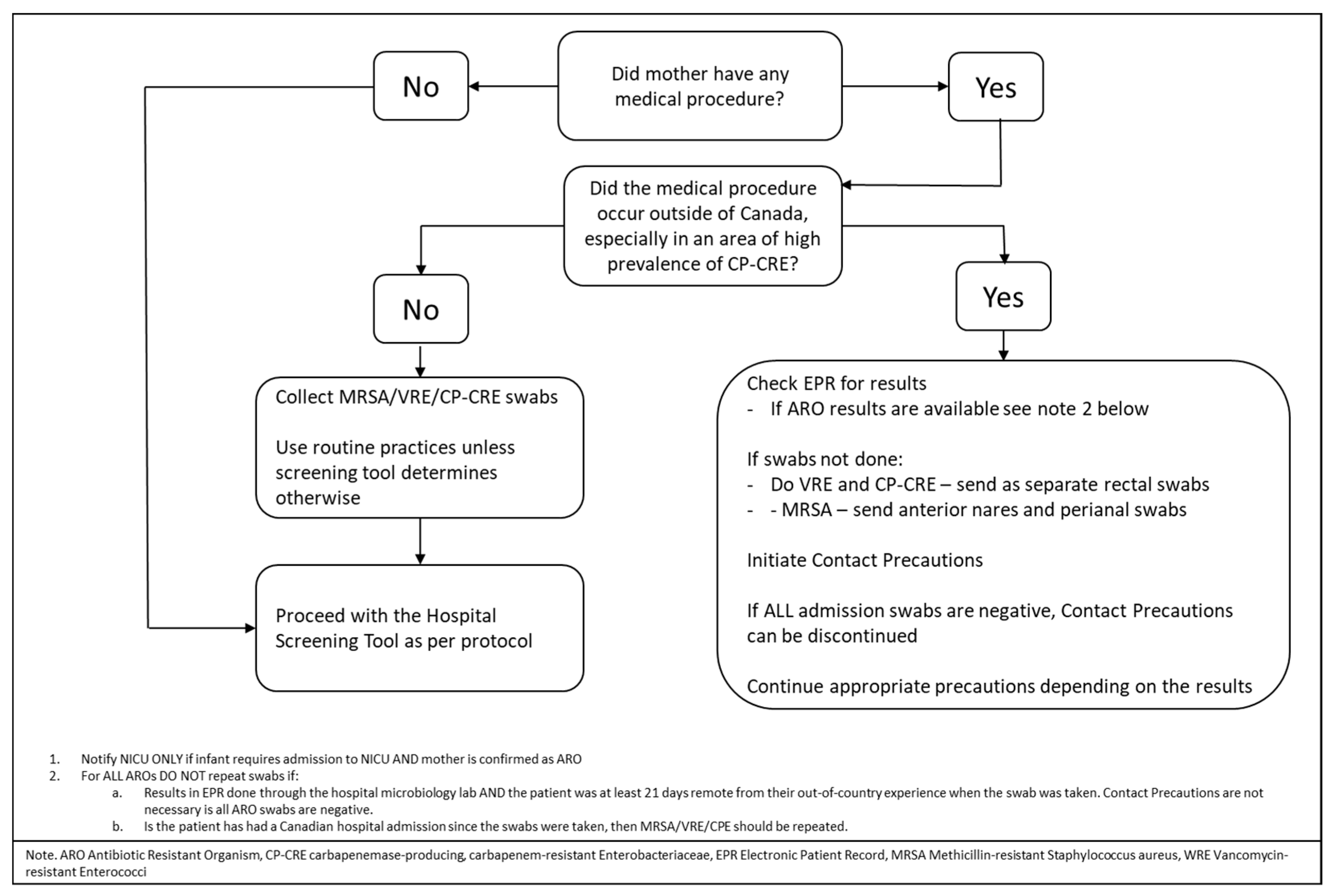
- Screening for CPE colonization, especially if there are identified risk factors as per Public Health Ontario, such as medical procedures or hospital admissions in or outside of Canada during the previous 12 months—for example, invitro fertilization or cervical cerclage.
- -
- The decision to treat or not for suspected or confirmed sepsis as the drugs for CP-CRE treatment are infrequently used in neonates. The safety profile, target drug range, length of treatment and dosage in this age group is unknown. An individualized approach to treatment should be considered in this population based on clinical presentation, cultures and sensitivity. The sensitivity of the maternal isolates should also be a factor in the decision process for antibiotic choice.
- -
- Management of infant contact with parents where colonization may occur—for example, attention to hand washing with kangaroo care.
- -
- Management of breastfeeding and human milk expression, handling and storage.
- -
- Limiting exposure to other parents with vulnerable children—no use of shared facilities.
- -
- General measures for contact precautions.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Cailes, B.; Kortsalioudaki, C.; Buttery, J.; Pattnayak, S.; Greenough, A.; Matthes, J.; Russell, A.B.; Kennea, N.; Heath, P.T. Epidemiology of UK neonatal infections: The neonIN infection surveillance network. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F547–F553. [Google Scholar] [CrossRef] [PubMed]
- Potter, R.F.; D’Souza, A.W.; Dantas, G. The rapid spread of carbapenem-resistant Enterobacteriaceae. Drug Resist. Updat. 2016, 29, 30–46. [Google Scholar] [CrossRef] [Green Version]
- Laxminarayan, R.; Duse, A.; Wattal, C.; Zaidi, A.K.M.; Wertheim, H.F.L.; Sumpradit, N.; Vlieghe, E.; Hare, G.L.; Gould, I.M.; Goossens, H. Antibiotic resistance—the need for global solutions. Lancet Infect Dis. 2013, 13, 1057–1098. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tsai, M.-H.; Chu, S.-M.; Hsu, J.-F.; Lien, R.; Huang, H.-R.; Chiang, M.-C.; Fu, R.-H.; Lee, C.-W.; Huang, Y.-C. Risk Factors and Outcomes for Multidrug-Resistant Gram-Negative Bacteremia in the NICU. Pediatrics 2014, 133, e322–e329. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paterson, D.L.; Doi, Y. A Step Closer to Extreme Drug Resistance (XDR) in Gram-Negative Bacilli. Clin. Infect. Dis. 2007, 45, 1179–1181. [Google Scholar] [CrossRef] [PubMed]
- Guidance for Control of Infections with Carbapenem-Resistant or Car-Bapenemase-Producing Enterobacteriaceae in Acute Care Facilities. Available online: https://www-cdc-gov.myaccess.library.utoronto.ca/mmwr/preview/mmwrhtml/mm5810a4.htm (accessed on 17 January 2021).
- Righi, E.; Peri, A.M.; Harris, P.N.A.; Wailan, A.M.; Liborio, M.; Lane, S.W.; Paterson, D.L. Global prevalence of carbapenem resistance in neutropenic patients and association with mortality and carbapenem use: Systematic review and meta-analysis. J. Antimicrob. Chemother. 2016, 72, 668–677. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Durante-Mangoni, E.; Andini, R.; Zampino, R. Management of carbapenem-resistant Enterobacteriaceae infections. Clin. Microbiol. Infect. 2019, 25, 943–950. [Google Scholar] [CrossRef]
- Public Health Ontario. Ontario Agency for Health Protection and Promotion. Available online: https://www.publichealthontario.ca/en/health-topics/infection-prevention-control/routine-practices-additional-precautions (accessed on 6 March 2021).
- Carbapenemases in Enterobacteriaceae: Detection and Antimicrobial Therapy. Available online: https://www.frontiersin.org/article/10.3389/fmicb.2019.01823 (accessed on 29 April 2021).
- Infection Control. CDC Reports that CRE Are a Nightmare Bacteria in Healthcare Environments. Dow Jones Factiva, Life Science Weekly. Available online: https://global-factiva-com.myaccess.library.utoronto.ca/redir/default.aspx?P=sa&NS=16&AID=9UNI011000&an=LFSW000020130322e93q0011t&cat=a&ep=ASI (accessed on 28 February 2021).
- Mataseje, L.F.; Abdesselam, K.; Vachon, J.; Mitchel, R.; Bryce, E.; Roscoe, D.; Boyd, D.A.; Embree, J.; Katz, K.; Kibsey, P.; et al. Results from the Canadian Nosocomial Infection Surveillance Program on Carbapenemase-ProducingEnterobacteriaceae, 2010 to 2014. Antimicrob. Agents Chemother. 2016, 60, 6787–6794. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Public Health Ontario. Carbapenemase-Producing Enterobacteriaceae Frequently Asked Questions. Available online: https://www.publichealthontario.ca/-/media/documents/F/2019/faq-cpe.pdf?la=en (accessed on 17 January 2021).
- Surveillance Report: CPE in Ontario, 1 May 2018–30 April 2019. Available online: https://www.publichealthontario.ca/-/media/documents/surveillance-reports/cpe/surveillance-report-cpe-2019.pdf?la=en (accessed on 29 April 2021).
- De Geyter, D.; Blommaert, L.; Verbraeken, N.; Sevenois, M.; Huyghens, L.; Martini, H.; Covens, L.; Piérard, D.; Wybo, I. The sink as a potential source of transmission of carbapenemase-producing Enterobacteriaceae in the intensive care unit. Antimicrob. Resist. Infect. Control. 2017, 6, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Tang, L.; Tadros, M.; Matukas, L.; Taggart, L.; Muller, M. Sink and Drain Monitoring and Decontamination Protocol for Carbapenemase-producing Enterobacteriaceae (CPE). Am. J. Infect. Control. 2020, 48, S17. [Google Scholar] [CrossRef]
- Kohler, P.P.; Melano, R.G.; Patel, S.N.; Shafinaz, S.; Faheem, A.; Coleman, B.L.; Green, K.; Armstrong, I.; Almohri, H.; Borgia, S.; et al. Emergence of Carbapenemase-Producing Enterobacteriaceae, South-Central Ontario, Canada1. Emerg. Infect. Dis. 2018, 24, 1674–1682. [Google Scholar] [CrossRef] [Green Version]
- Centers for Disease Control and Prevention, National Center for Emerging and Zoonotic Infectious Diseases (NCEZID), Divi-sion of Healthcare Quality Promotion (DHQP) [Internet]. 2016. Available online: https://www-cdc-gov.myaccess.library.utoronto.ca/infectioncontrol/basics/transmission-based-precautions.html (accessed on 6 March 2021).
- Peleg, A.Y.; Franklin, C.; Bell, J.M.; Spelman, D.W. Dissemination of the Metallo—Lactamase Gene blaIMP-4 among Gram-Negative Pathogens in a Clinical Setting in Australia. Clin. Infect. Dis. 2005, 41, 1549–1556. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zheng, R.; Zhang, Q.; Guo, Y.; Feng, Y.; Liu, L.; Zhang, A.; Zhao, Y.; Yang, X.; Xia, X. Outbreak of plasmid-mediated NDM-1-producing Klebsiella pneumoniae ST105 among neonatal patients in Yunnan, China. Ann. Clin. Microbiol. Antimicrob. 2016, 15, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mairi, A.; Touati, A.; Bessai, S.A.; Boutabtoub, Y.; Khelifi, F.; Sotto, A.; Lavigne, J.-P.; Pantel, A. Carbapenemase-producing Enterobacteriaceae among pregnant women and newborns in Algeria: Prevalence, molecular characterization, maternal-neonatal transmission, and risk factors for carriage. Am. J. Infect. Control. 2019, 47, 105–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arhoune, B.; Oumokhtar, B.; Hmami, F.; Barguigua, A.; Timinouni, M.; El Fakir, S.; Bouharrou, A. Rectal carriage of extended-spectrum β-lactamase- and carbapenemase-producing Enterobacteriaceae among hospitalised neonates in a neonatal intensive care unit in Fez, Morocco. J. Glob. Antimicrob. Resist. 2017, 8, 90–96. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Rámila, C.; López-Cerero, L.; Martín, M.V.A.; Martín, C.V.; Serrano, L.; Pascual, Á.; Rodríguez-Baño, J. Vagino-rectal colonization and maternal–neonatal transmission of Enterobacteriaceae producing extended-spectrum β-lactamases or carbapenemases: A cross-sectional study. J. Hosp. Infect. 2019, 101, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Mougkou, K.; Michos, A.; Spyridopoulou, K.; Daikos, G.L.; Siahanidou, T.; Spyridis, N.; Kapetanakis, J.; Korkas, A.; Anagnostakou, C.; Papagaroufalis, G.; et al. Colonization of neonates with carbapenemase-producing Enterobacteriaceae (CPE). In Proceedings of the 30th Annual Meeting of the European Society for Paediatric Infectious Diseases (ESPID 2012), Thessalonike, Greece, 8–12 May 2012. [Google Scholar]
- Singh, N.P.; Das Choudhury, D.; Gupta, K.; Rai, S.; Batra, P.; Manchanda, V.; Saha, R.; Kaur, I. Predictors for gut colonization of carbapenem-resistant Enterobacteriaceae in neonates in a neonatal intensive care unit. Am. J. Infect. Control. 2018, 46, e31–e35. [Google Scholar] [CrossRef] [PubMed]
- Ballot, D.E.; Bandini, R.; Nana, T.; Bosman, N.; Thomas, T.; Davies, V.A.; Cooper, P.A.; Mer, M.; Lipman, J. A review of -multidrug-resistant Enterobacteriaceae in a neonatal unit in Johannesburg, South Africa. BMC Pediatr. 2019, 19, 1–9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magiorakos, A.P.; Burns, K.; Baño, J.R.; Borg, M.; Daikos, G.; Dumpis, U.; Lucet, J.C.; Moro, M.L.; Tacconelli, E.; Simonsen, G.S.; et al. Infection prevention and control measures and tools for the prevention of entry of carbapenem-resistant Enterobacteriaceae into healthcare settings: Guidance from the European Centre for Disease Prevention and Control. Antimicrob. Resist. Infect. Control. 2017, 6, 113. [Google Scholar] [CrossRef] [PubMed]
- Schneider, A.; Coope, C.; Michie, S.; Puleston, R.; Hopkins, S.; Oliver, I. Implementing a toolkit for the prevention, management and control of carbapenemase-producing Enterobacteriaceae in English acute hospitals trusts: A qualitative evaluation. BMC Health Serv. Res. 2019, 19, 1–20. [Google Scholar] [CrossRef] [PubMed]
- Fournier, S.; Monteil, C.; Lepainteur, M.; Richard, C.; Brun-Buisson, C.; Jarlier, V.; Collective AP-HP Outbreaks Control Group. Long-term control of carbapenemase-producing Enterobacteriaceae at the scale of a large French multihospital institution: A nine-year experience, France, 2004 to 2012. Eurosurveillance 2014, 19, 20802. [Google Scholar] [CrossRef] [Green Version]
- Chair, M.R.; Cruickshank, M.; Cheng, A.; Gandossi, S.; Quoyle, C.; Stuart, R.; Sutton, B.; Turnidge, J.; Bennett, N.; Buising, K.; et al. Recommendations for the control of carbapenemase-producing Enterobacteriaceae (CPE): A guide for acute care health facilities. Infect. Dis. Health 2017, 22, 159–186. [Google Scholar] [CrossRef] [Green Version]
- Jamal, A.J.; Garcia-Jeldes, F.; Baqi, M.; Borgia, S.; Johnstone, J.; Katz, K.; Kohler, P.; Muller, M.P.; McGeer, A.J.; for the CPE Investigators of the Toronto Invasive Bacterial Diseases Network. Infection prevention and control practices related to carbapenemase-producing Enterobacteriaceae (CPE) in acute-care hospitals in Ontario, Canada. Infect. Control. Hosp. Epidemiol. 2019, 40, 1006–1012. [Google Scholar] [CrossRef] [PubMed]
- Castagnola, E.; Tatarelli, P.; Mesini, A.; Baldelli, I.; La Masa, D.; Biassoni, R.; Bandettini, R. Epidemiology of carbapenemase-producing Enterobacteriaceae in a pediatric hospital in a country with high endemicity. J. Infect. Public Health 2019, 12, 270–274. [Google Scholar] [CrossRef]
- Wangchinda, W.; Pati, N.; Maknakhon, N.; Seenama, C.; Tiengrim, S.; Thamlikitkul, V. Collateral damage of using Colistin in hos-pitalized patients on emergence of colistin-resistant Escherichia coli and Klebsiella pneumoniae colonization and infection. Antimicrob. Resist. Infect. Control 2018, 7, 84. [Google Scholar] [CrossRef] [PubMed]
- Jajoo, M.; Kumar, V.; Jain, M.; Kumari, S.; Manchanda, V. Intravenous Colistin Administration in Neonates. Pediatr. Infect. Dis. J. 2011, 30, 218–221. [Google Scholar] [CrossRef] [PubMed]
- Çağan, E.; Baş, E.K.; Asker, H.S. Use of Colistin in a Neonatal Intensive Care Unit: A Cohort Study of 65 Patients. Med Sci. Monit. 2017, 23, 548–554. [Google Scholar] [CrossRef] [Green Version]
- Kimberlin, D.W. Red Book: 2018–2021 Report of The Committee on Infectious Diseases; American Academy of Pediatrics: Itasca, IL, USA, 2018. [Google Scholar]
- Borer, A.; Saidel-Odes, L.; Eskira, S.; Nativ, R.; Riesenberg, K.; Livshiz-Riven, I.; Schlaeffer, F.; Sherf, M.; Peled, N. Risk factors for developing clinical infection with carbapenem-resistant Klebsiella pneumoniae in hospital patients initially only colonized with carbapenem-resistant K pneumoniae. Am. J. Infect. Control. 2012, 40, 421–425. [Google Scholar] [CrossRef]
- Schechner, V.; Kotlovsky, T.; Kazma, M.; Mishali, H.; Schwartz, D.; Navon-Venezia, S.; Schwaber, M.; Carmeli, Y. Asymptomatic rectal carriage of blaKPC producing carbapenem-resistant Enterobacteriaceae: Who is prone to become clinically infected? Clin. Microbiol. Infect. 2013, 19, 451–456. [Google Scholar] [CrossRef] [Green Version]
- Virox Technologies Incorporated. RescueTM Ready to Use One Step Disinfectant Cleaner & Deodorizer. [Internet]. Available online: https://rescuedisinfectants.com/wp-content/uploads/2017/07/REF067_Rescue-RTU-Ref-Sheet_17-069-2.pdf (accessed on 3 April 2021).






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Risk Factors | Cases | Proportion (%) | Maternal Scenarios/Considerations | Neonatal Scenarios/Considerations |
|---|---|---|---|---|
| Chronic illness/underlying medical conditions | 241 | 83.4 | ||
| Inpatient hospitalization in Canada in the last 12 months | 155 | 53.6 | Admission for obstetrics reasons such as preterm labor, rupture of membranes | Neonates’ risk of admission to the NICU increases, especially with prematurity |
| Travel outside of Canada in the last 12 months | 151 | 52.2 | Travel especially to endemic countries in preconception period or during pregnancy | |
| Medical/surgical procedure in Canada in the last 12 months | 102 | 35.3 | In vitro fertilization, cervical cerclage etcetera | |
| Healthcare received outside of Canada in last 12 months | 92 | 31.8 | Maternal obstetric care in higher-risk countries or contacts from these countries such as India and Pakistan as per Public Health Ontario [14] | |
| ICU admission in Canada in the last 12 months | 55 | 19.0 | Multiple potential reasons in the NICU including respiratory procedures (ventilation, suctioning), breast feeding, or human milk expression and handling | |
| Endoscopic procedure in Canada in the last 12 months | 41 | 14.2 | ||
| Previous colonization with CPE | 31 | 10.7 | Maternal obstetric care in higher-risk countries or contacts from these countries such as India and Pakistan as per Public Health Ontario [14] | |
| Known contact with a confirmed case | 15 | 5.2 | Maternal obstetric care in higher-risk countries or contacts from these countries such as India and Pakistan as per Public Health Ontario (ref Surveillance report) | Kangaroo care, breast milk expression and breast feeding |
| Other | 84 | 29.1 |
| Author | Country | Population | Findings |
|---|---|---|---|
| Zheng et al., 2016 | China | NICU admissions in a tertiary care health facility | Eighteen carbapenem-resistant Klebsiella pneumoniae strains were isolated from 17 patients in various specimens, including sputum, stool, and blood, and one carbapenem-resistant Klebsiella pneumoniae was detected in incubator water. |
| [20] | Period: in 2014 | Nosocomial surveillance systems should play a more important role in the infection control to limit the spread of NDM1-producing pathogens. | |
| Mairi et al., 2019 | Algeria | All mothers and their newborns managed in two maternity units | 414 mothers and 422 newborns were included. |
| 836 rectal swabs and 221 vaginal swabs were collected. | |||
| [21] | Period: January 2016 to April 2016 | A total of 28 CPE isolates were obtained from mothers (n = 19) (with two different isolated from the same mother), newborns (n = 7), and the environment (n = 1). | |
| Low birth weight was significantly associated with CPE carriage in the newborn. | |||
| No carriers were premature, suggesting that CPE had no direct role on a premature delivery and could not represent a high risk for infections encountered frequently in preterm newborns but could influence birth weight. | |||
| Focused interventions to reduce this cross-transmission in settings of high endemicity are required. | |||
| Arhoune et al., 2017 | Morocco | All neonates hospitalized in the NICU | A high rate of multi-resistance ESBLE was noted. The prevalence of carbapenemase-producing Enterobacteriaceae was 1.8%. It was proposed a screening policy be developed |
| [22] | Period: February 2013 to July 2013 | ||
| Jimenez Ramila et al., 2018 | Spain | All pregnant women at the time of delivery and their newborns | A total of 815 women and 800 neonates were studied; 59 were found to be colonized by ESBLE at delivery (prevalence, 7.2%; 95% CI: 5.6–9.2) but no CPE were found. |
| [23] | Period: August 2014 to June 2015 | ||
| Mougkou et al., 2012 [24] | Greece | Multi-center, eight NICUs in five public hospitals. | Rectal and umbilical swabs from infants in 8 NICUs. |
| (Abstract) | Period: November 2011 to January 2012. | One outborn neonate was colonized. The study showed a very low prevalence of colonization with CPE in NICU patients. Factors associated with this phenomenon need to be further determined. | |
| Singh et al., 2018 | India | Three rectal swabs were collected from hospital-delivered and NICU-admitted neonates | From 300 neonates, 26 cases of CRE were isolated. |
| Statistically, significant risk factors were NG tube, breastfeeding, NG feeding, top feeding, expressed breastmilk, ventilation, antibiotic administration, and hospitalization duration. | |||
| [25] | Top feeding and antibiotics administration were identified as two independent risk factors by multiple logistic regression. | ||
| Active surveillance of cultures from hospitalized patients and implementation of preventive efforts can reduce the risk of CRE. | |||
| Ballot et al., 2019 | South Africa | A cross-sectional retrospective review of multidrug-resistant organisms in neonates admitted to a tertiary neonatal unit. | A total of 465 infections in 291 neonates. Very low birth weight was record in 68.6% of cases. |
| [26] | Period:1 January 2013 to December 2015. | The median age of infection was 14.0 days. Risk factors for MDRE included prematurity (p = 0.01), lower birth weight (p = 0.04), maternal HIV infection (p = 0.02) and oxygen on day 28 (p < 0.001). | |
| There was an increase in CRE from 2.6% in 2013 to 8.9% in 2015 (p = 0.06). | |||
| There was an increase in CRE from 2.6% in 2013 to 8.9% in 2015 (p = 0.06). Most of the CRE were NDM producers. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Seesahai, J.; Church, P.T.; Asztalos, E.; Eng-Chong, M.; Arbus, J.; Banihani, R. Neonates with Maternal Colonization of Carbapenemase-Producing, Carbapenem-Resistant Enterobacteriaceae: A Mini-Review and a Suggested Guide for Preventing Neonatal Infection. Children 2021, 8, 399. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050399
Seesahai J, Church PT, Asztalos E, Eng-Chong M, Arbus J, Banihani R. Neonates with Maternal Colonization of Carbapenemase-Producing, Carbapenem-Resistant Enterobacteriaceae: A Mini-Review and a Suggested Guide for Preventing Neonatal Infection. Children. 2021; 8(5):399. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050399
Chicago/Turabian StyleSeesahai, Judy, Paige Terrien Church, Elizabeth Asztalos, Melanee Eng-Chong, Jo Arbus, and Rudaina Banihani. 2021. "Neonates with Maternal Colonization of Carbapenemase-Producing, Carbapenem-Resistant Enterobacteriaceae: A Mini-Review and a Suggested Guide for Preventing Neonatal Infection" Children 8, no. 5: 399. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050399