
Impact of Perceived Social Support on the Relationship between ADHD and Depressive Symptoms among First Year Medical Students: A Structural Equation Model Approach

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Procedures
2.2. Instruments
2.2.1. General Demographic Data
2.2.2. Adult ADHD Self-Report Scale (ASRS) Screener V1.1
2.2.3. Patient Health Questionnaire (PHQ)-9
2.2.4. Revised-Thai Multidimensional Scale of Perceived Social Support (r-MSPSS)
2.3. Data Analysis
3. Results
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sadock, B.J.S.V.; Ruiz, P. (Eds.) Kaplan and Sadock’s Synopsis of Psychiatry: Behavioral Science/Clinical Psychiatry, 11th ed.; Wolters Kluwer: Philadelphia, PA, USA, 2015. [Google Scholar]
- Thapar, A.; Cooper, M. Attention deficit hyperactivity disorder. Lancet 2016, 387, 1240–1250. [Google Scholar] [CrossRef]
- Vasileva, M.; Graf, R.K.; Reinelt, T.; Petermann, U.; Petermann, F. Research review: A meta-analysis of the international prevalence and comorbidity of mental disorders in children between 1 and 7 years. J. Child. Psychol. Psychiatry 2021, 62, 372–381. [Google Scholar] [CrossRef]
- Kessler, R.C.; Adler, L.; Barkley, R.; Biederman, J.; Conners, C.K.; Demler, O.; Faraone, S.V.; Greenhill, L.L.; Howes, M.J.; Secnik, K.; et al. The Prevalence and Correlates of Adult ADHD in the United States: Results From the National Comorbidity Survey Replication. Am. J. Psychiatry 2006, 163, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Jung, Y.-E.; Kwak, Y.-S.; Kim, M.-D. Prevalence and correlates of attention-deficit hyperactivity disorder symptoms in Korean college students. Neuropsychiatr. Dis. Treat. 2015, 11, 797–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuttle, J.P.; Scheurich, N.E.; Ranseen, J. Prevalence of ADHD Diagnosis and Nonmedical Prescription Stimulant Use in Medical Students. Acad. Psychiatry 2010, 34, 220–223. [Google Scholar] [CrossRef] [PubMed]
- Atwoli, L.; Owiti, P.; Manguro, G.; Ndambuki, D. Attention deficit hyperactivity disorder symptom self-report among medical students in Eldoret, Kenya. Afr. J. Psychiatry 2011, 14, 286–289. [Google Scholar] [CrossRef] [Green Version]
- Shen, Y.; Chan, B.S.M.; Liu, J.; Meng, F.; Yang, T.; He, Y.; Lu, J.; Luo, X.; Zhang, X.Y. Estimated prevalence and associated risk factors of attention deficit hyperactivity disorder (ADHD) among medical college students in a Chinese population. J. Affect. Disord. 2018, 241, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Polanczyk, G.; De Lima, M.S.; Horta, B.L.; Biederman, J.; Rohde, L.A. The Worldwide Prevalence of ADHD: A Systematic Review and Metaregression Analysis. Am. J. Psychiatry 2007, 164, 942–948. [Google Scholar] [CrossRef]
- Faraone, S.V.; Banaschewski, T.; Coghill, D.; Zheng, Y.; Biederman, J.; Bellgrove, M.A.; Newcorn, J.H.; Gignac, M.; Al Saud, N.M.; Manor, I.; et al. The World Federation of ADHD International Consensus Statement: 208 Evidence-Based Conclusions about the Disorder. Available online: https://0-www-sciencedirect-com.brum.beds.ac.uk/science/article/pii/S014976342100049X (accessed on 1 April 2021).
- Rotenstein, L.S.; Ramos, M.A.; Torre, M.; Segal, J.B.; Peluso, M.J.; Guille, C.; Sen, S.; Mata, D.A. Prevalence of Depression, Depressive Symptoms, and Suicidal Ideation Among Medical Students: A Systematic Review and Meta-Analysis. JAMA 2016, 316, 2214–2236. [Google Scholar] [CrossRef] [Green Version]
- Pan, P.-Y.; Yeh, C.-B. Impact of depressive/anxiety symptoms on the quality of life of adolescents with ADHD: A community-based 1-year prospective follow-up study. Eur. Child. Adolesc. Psychiatry 2016, 26, 659–667. [Google Scholar] [CrossRef]
- Panevska, L.S.; Zafirova-Ivanovska, B.; Vasilevska, K.; Isjanovska, R.; Kadri, H. Relationship Between ADHD and Depression Among University Students in Macedonia. Mater. Socio-Med. 2015, 27, 18–21. [Google Scholar] [CrossRef] [Green Version]
- Cole, D.A.; Jacquez, F.M.; Maschman, T.L. Social Origins of Depressive Cognitions: A Longitudinal Study of Self-Perceived Competence in Children. Cogn. Ther. Res. 2001, 25, 377–395. [Google Scholar] [CrossRef]
- Cole, D.A.; Martin, J.M.; Powers, B. A Competency-based Model of Child Depression: A Longitudinal Study of Peer, Parent, Teacher, and Self-evaluations. J. Child. Psychol. Psychiatry 1997, 38, 505–514. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Adler, L.; Ames, M.; Barkley, R.A.; Birnbaum, H.; Greenberg, P.; Johnston, J.A.; Spencer, T.; Ustün, T.B. The Prevalence and Effects of Adult Attention Deficit/Hyperactivity Disorder on Work Performance in a Nationally Representative Sample of Workers. J. Occup. Environ. Med. 2005, 47, 565–572. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DuPaul, G.J.; Gormley, M.J.; Laracy, S.D. School-Based Interventions for Elementary School Students with ADHD. Child. Adolesc. Psychiatr. Clin. N. Am. 2014, 23, 687–697. [Google Scholar] [CrossRef]
- Sibley, M.H.; Graziano, P.A.; Ortiz, M.; Rodriguez, L.; Coxe, S. Academic impairment among high school students with ADHD: The role of motivation and goal-directed executive functions. J. Sch. Psychol. 2019, 77, 67–76. [Google Scholar] [CrossRef]
- Herman, K.C.; Lambert, S.F.; Ialongo, N.S.; Ostrander, R. Academic Pathways between Attention Problems and Depressive Symptoms Among Urban African American Children. J. Abnorm. Child. Psychol. 2007, 35, 265–274. [Google Scholar] [CrossRef] [Green Version]
- Milich, R.; Okazaki, M. An examination of learned helplessness among attention-deficit hyperactivity disordered boys. J. Abnorm. Child. Psychol. 1991, 19, 607–623. [Google Scholar] [CrossRef]
- Patterson, G.R.; Stoolmiller, M. Replications of a dual failure model for boys’ depressed mood. J. Consult. Clin. Psychol. 1991, 59, 491–498. [Google Scholar] [CrossRef]
- Powell, V.; Riglin, L.; Hammerton, G.; Eyre, O.; Martin, J.; Anney, R.; Thapar, A.; Rice, F. What explains the link between childhood ADHD and adolescent depression? Investigating the role of peer relationships and academic attainment. Eur. Child. Adolesc. Psychiatry 2020, 29, 1581–1591. [Google Scholar] [CrossRef] [Green Version]
- Hoza, B.; Mrug, S.; Gerdes, A.C.; Hinshaw, S.P.; Bukowski, W.M.; Gold, J.A.; Kraemer, H.C.; Pelham, W.E.; Wigal, T.; Arnold, L.E. What Aspects of Peer Relationships Are Impaired in Children with Attention-Deficit/Hyperactivity Disorder? J. Consult. Clin. Psychol. 2005, 73, 411–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humphreys, K.L.; Katz, S.J.; Lee, S.S.; Hammen, C.L.; Brennan, P.A.; Najman, J.M. The association of ADHD and depression: Mediation by peer problems and parent–child difficulties in two complementary samples. J. Abnorm. Psychol. 2013, 122, 854–867. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johnston, C.; Mash, E.J. Families of Children with Attention-Deficit/Hyperactivity Disorder: Review and Recommendations for Future Research. Clin. Child. Fam. Psychol. Rev. 2001, 4, 183–207. [Google Scholar] [CrossRef] [PubMed]
- Meinzer, M.C.; Hill, R.M.; Pettit, J.W.; Nichols-Lopez, K.A. Parental Support Partially Accounts for the Covariation Between ADHD and Depressive Symptoms in College Students. J. Psychopathol. Behav. Assess. 2015, 37, 247–255. [Google Scholar] [CrossRef]
- Meinzer, M.C.; Felton, J.W.; Oddo, L.E.; Rubin, K.H.; Chronis-Tuscano, A. Do ADHD Symptoms and Relationship Quality With Mothers and Best Friends Across High School Predict Depressive Symptoms for Adolescents? J. Atten. Disord. 2020, 2020. [Google Scholar] [CrossRef]
- Duru, E.; Balkis, M.; Turkdoğan, T. Relational Violence, Social Support, Self-Esteem, Depression and Anxiety: A Moderated Mediation Model. J. Child. Fam. Stud. 2019, 28, 2404–2414. [Google Scholar] [CrossRef]
- Nam, E.J.; Lee, J.-E. Mediating Effects of Social Support on Depression and Suicidal Ideation in Older Korean Adults With Hypertension Who Live Alone. J. Nurs. Res. 2019, 27, e20. [Google Scholar] [CrossRef]
- Greenglass, E.; Fiksenbaum, L.; Eaton, J. The relationship between coping, social support, functional disability and depression in the elderly. Anxiety Stress. Coping 2006, 19, 15–31. [Google Scholar] [CrossRef]
- Talwar, P.; Othman, M.K.; Ghan, K.A.; Wah, T.K.; Aman, S.; Yusoff, N.F.M. The role of social support in mediating stress and depression. Online J. Health Allied. Scs 2017, 16, 4. [Google Scholar]
- Zimet, G.D.; Powell, S.S.; Farley, G.K.; Werkman, S.; Berkoff, K.A. Psychometric Characteristics of the Multidimensional Scale of Perceived Social Support. J. Pers. Assess. 1990, 55, 610–617. [Google Scholar] [CrossRef]
- Biederman, J.; Monuteaux, M.C.; Mick, E.; Spencer, T.; Wilens, T.E.; Silva, J.M.; Snyder, L.E.; Faraone, S.V. Young adult outcome of attention deficit hyperactivity disorder: A controlled 10-year follow-up study. Psychol. Med. 2006, 36, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Larsson, H.; Asherson, P.; Chang, Z.; Ljung, T.; Friedrichs, B.; Larsson, J.-O.; Lichtenstein, P. Genetic and environmental influences on adult attention deficit hyperactivity disorder symptoms: A large Swedish population-based study of twins. Psychol. Med. 2012, 43, 197–207. [Google Scholar] [CrossRef]
- Faraone, S.V.; Biederman, J.; Mick, E. The age-dependent decline of attention deficit hyperactivity disorder: A meta-analysis of follow-up studies. Psychol. Med. 2005, 36, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Verheul, I.; Rietdijk, W.; Block, J.; Franken, I.; Larsson, H.; Thurik, R. The association between attention-deficit/hyperactivity (ADHD) symptoms and self-employment. Eur. J. Epidemiol. 2016, 31, 793–801. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kooij, J.J.S.; Buitelaar, J.K.; Oord, E.J.V.D.; Furer, J.W.; Rijnders, C.A.T.; Hodiamont, P.P.G. Internal and external validity of Attention-Deficit Hyperactivity Disorder in a population-based sample of adults. Psychol. Med. 2005, 35, 817–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kessler, R.C.; Adler, L.; Ames, M.; Demler, O.; Faraone, S.; Hiripi, E.; Howes, M.J.; Jin, R.; Secnik, K.; Spencer, T.; et al. The World Health Organization adult ADHD self-report scale (ASRS): A short screening scale for use in the general population. Psychol. Med. 2005, 35, 245–256. [Google Scholar] [CrossRef] [Green Version]
- Bussaratid, S.; Atsariyasing, W.; Wannarit, K.; Pukrittayakami, P.; Hosiri, T.; Wiwatwararom, N.; Pornnoppadol, C. Reliability and Validity Study of Adult ADHD Self-Report Scale (ASRS) Screener v1.1 Thai Version. J. Psychiatr. Assoc. Thailand. 2016, 61, 145–154. [Google Scholar]
- Kiatrungrit, K.; Putthisri, S.; Hongsanguansri, S.; Wisajan, P.; Jullagate, S. Validity and Reliability of Adult ADHD Self-Report Scale Thai Version (ASRS-V1.1 TH). Shanghai Arch. Psychiatry 2017, 29, 218–227. [Google Scholar]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- Lotrakul, M.; Sumrithe, S.; Saipanish, R. Reliability and validity of the Thai version of the PHQ-9. BMC Psychiatry 2008, 8, 46. [Google Scholar] [CrossRef] [Green Version]
- Wongpakaran, T.; Wongpakaran, N.; Sirirak, T.; Arunpongpaisal, S.; Zimet, G. Confirmatory factor analysis of the revised version of the Thai multidimensional scale of perceived social support among the elderly with depression. Aging Ment. Health 2017, 22, 1149–1154. [Google Scholar] [CrossRef] [PubMed]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process. Analysis: A Regression-Based Approach, 2nd ed.; Guilford Press: New York, NY, USA, 2018; pp. 159–162. [Google Scholar]
- Soper, D.S. A-Priori Sample Size for Structural Equation Models References—Free Statistics Calculators. Available online: (https://www.danielsoper.com/statcalc/calculator.aspx?id=89) (accessed on 31 January 2021).
- Kline, R. Principles and Practice of Structural Equation Modeling; The Guilford Press: New York, NY, USA; London, UK, 2011. [Google Scholar]
- Shahar, G.; Cohen, G.; Grogan, K.E.; Barile, J.P.; Henrich, C.C. Terrorism-Related Perceived Stress, Adolescent Depression, and Social Support from Friends. Pediatrics 2009, 124, e235–e240. [Google Scholar] [CrossRef] [PubMed]
- Little, T.D.; Cunningham, W.A.; Shahar, G.; Widaman, K.F. To Parcel or Not to Parcel: Exploring the Question, Weighing the Merits. Struct. Equ. Model. A Multidiscip. J. 2002, 9, 151–173. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Knutson, T.J.; Komolsevin, R.; Chatiketu, P.; Smith, V.R. A cross-cultural comparison of Thai and US American rhetorical sensitivity: Implications for intercultural communication effectiveness. Int. J. Intercult. Relat. 2003, 27, 63–78. [Google Scholar] [CrossRef]
- Zheng, Y.; Pingault, J.-B.; Unger, J.B.; Rijsdijk, F. Genetic and environmental influences on attention-deficit/hyperactivity disorder symptoms in Chinese adolescents: A longitudinal twin study. Eur. Child. Adolesc. Psychiatry 2019, 29, 205–216. [Google Scholar] [CrossRef]
- Yaman, A.; Mesman, J.; Van Ijzendoorn, M.H.; Bakermans-Kranenburg, M.J.; Linting, M. Parenting in an Individualistic Culture with a Collectivistic Cultural Background: The Case of Turkish Immigrant Families with Toddlers in the Netherlands. J. Child. Fam. Stud. 2010, 19, 617–628. [Google Scholar] [CrossRef] [Green Version]
- Griffin, B.; Hu, W. Parental career expectations: Effect on medical students’ career attitudes over time. Med. Educ. 2019, 53, 584–592. [Google Scholar] [CrossRef]
- Sletta, C.; Tyssen, R.; Løvseth, L.T. Change in subjective well-being over 20 years at two Norwegian medical schools and factors linked to well-being today: A survey. BMC Med. Educ. 2019, 19, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Kunanitthaworn, N.; Wongpakaran, T.; Wongpakaran, N.; Paiboonsithiwong, S.; Songtrijuck, N.; Kuntawong, P.; Wedding, D. Factors associated with motivation in medical education: A path analysis. BMC Med. Educ. 2018, 18, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Semeijn, E.; Comijs, H.; Kooij, J.; Michielsen, M.; Beekman, A.; Deeg, D. The role of adverse life events on depression in older adults with ADHD. J. Affect. Disord. 2015, 174, 574–579. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, E.; McNeill, K.G.; Mavor, K.I.; Anderson, K. Looking Beyond Personal Stressors: An Examination of How Academic Stressors Contribute to Depression in Australian Graduate Medical Students. Teach. Learn. Med. 2014, 26, 56–63. [Google Scholar] [CrossRef] [PubMed]



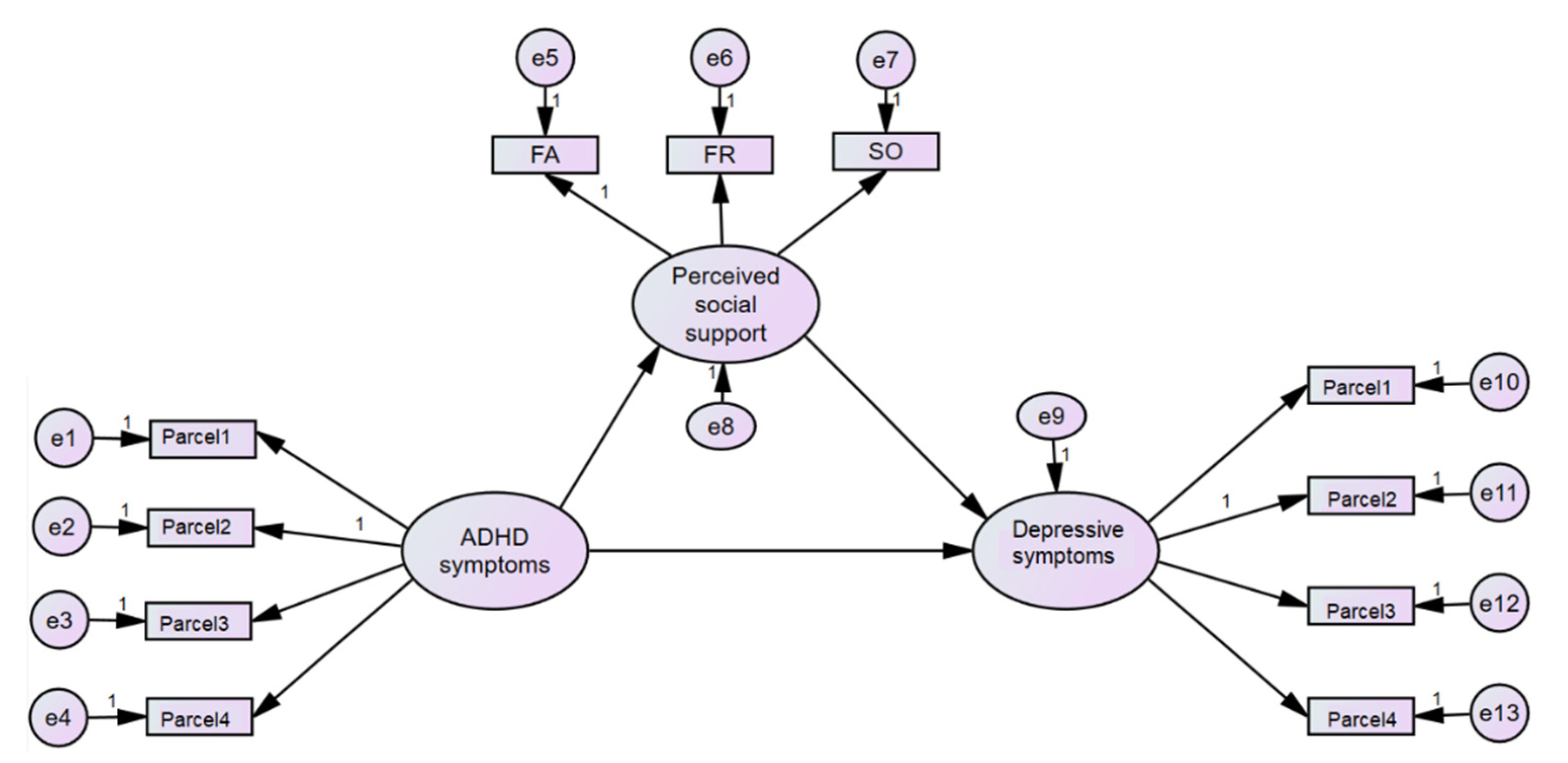{kind=link}
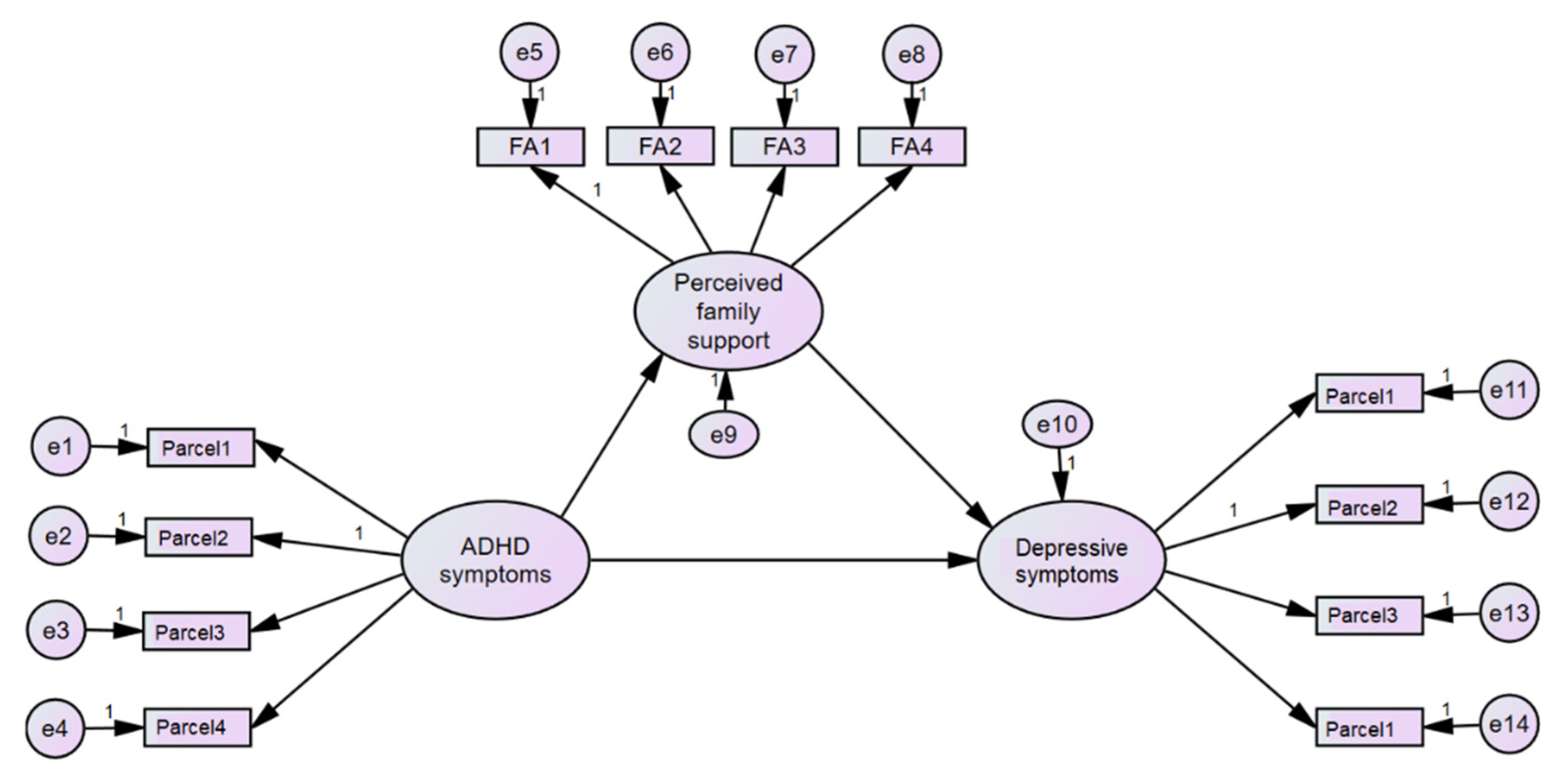{kind=link}
| All (n = 124) | ADHD Symptoms (n = 31) | Non-ADHD Symptoms (n = 93) | p-Value | |
|---|---|---|---|---|
| Variable | n (%) or Mean ± SD | n (%) or Mean ± SD | n (%) or Mean ± SD | |
| Male sex, n (%) | 46 (37.1) | 10 (32.3) | 36 (38.7) | 0.520 |
| Age (years old), mean ± SD | 18.78 ± 0.74 | 18.55 ± 0.64 | 18.75 ± 0.77 | 0.186 |
| Underlying illness, n (%) | ||||
| Allergy | 39 (31.5) | 8 (25.8) | 23 (24.7) | 0.905 |
| Mental health problem or psychiatric disorder | 0 (0) | 0 (0) | 0 (0) | - |
| Father’s years of education, SD Mean ± SD | 14.98 ± 5.6 | 14.85 ± 6.0 | 15.03 ± 5.4 | 0.887 |
| Father’s mental illness, n (%) | 1(0.8) | 1(3.3) | 0(0) | 0.080 |
| Mother’s years of education, Mean ± SD | 14.71 ± 5.7 | 15.46 ± 5.8 | 14.45 ± 5.6 | 0.437 |
| Mother’s mental illness, n (%) | 0(0) | 0(0) | 0(0) | - |
| Single child, n (%) | 18 (14.5) | 2 (6.5) | 16 (17.2) | 0.141 |
| Firstborn, n (%) | 65 (52.4) | 14 (45.2) | 51 (54.8) | 0.350 |
| Lastborn, n (%) | 46 (37.4) | 11 (36.7) | 35 (37.6) | 0.924 |
| Number of siblings, Mean ± SD | 2.1 ± 0.79 | 2.37 ± 0.85 * | 2.01 ± 0.76 | 0.036 |
| ASRS total score | 10.11 ± 3.54 | 14.45 ± 1.8 | 8.67 ± 2.7 | <0.0001 |
| rMSPSS-total | 5.49 ± 0.9 | 5.38 ± 0.9 | 5.53 ± 0.9 | 0.458 |
| rMSPSS-SO | 4.98 ± 1.4 | 4.92 ± 1.6 | 5.00 ± 1.4 | 0.800 |
| rMSPSS-FA | 6.07 ± 1.0 | 5.82 ±1.2 | 6.15 ± 0.9 | 0.117 |
| rMSPSS-FR | 5.43 ± 1.0 | 5.41 ± 0.9 | 5.43 ± 1.0 | 0.931 |
| PHQ-9 | 7.19± 3.86 | 7.87 ± 4.0 | 6.97 ± 3.8 | 0.261 |
| Variable | ASRS | rMSPSS-SO | rMSPSS-FR | rMSPSS-FA | PHQ-9 |
|---|---|---|---|---|---|
| ASRS | − | ||||
| rMSPSS−SO | −0.183 * | − | |||
| rMSPSS−FR | −0.164 | 0.469 ** | − | ||
| rMSPSS−FA | −0.238 ** | 0.335 ** | 0.338 ** | − | |
| PHQ−9 | 0.264 ** | −0.199 * | −0.320 ** | 0.368 ** | − |
| Variable | Coefficient | S.E. | LLCI | ULCI | p-Value | R Square |
|---|---|---|---|---|---|---|
| Model 1. Mediator: Overall Perceived Social Support | ||||||
| Total effect | 0.313 | 0.119 | 0.109 | 0.505 | 0.011 | 0.352 |
| Total indirect | 0.168 | 0.103 | 0.039 | 0.367 | 0.029 | |
| Direct effect | 0.145 | 0.128 | −0.079 | 0.340 | 0.292 | |
| Model 2. Mediator: Perceived Family Members’ Support | ||||||
| Total effect | 0.312 | 0.119 | 0.103 | 0.499 | 0.012 | 0.244 |
| Total indirect | 0.116 | 0.063 | 0.037 | 0.256 | 0.008 | |
| Direct effect | 0.196 | 0.111 | 0.030 | 0.381 | 0.044 | |
| Model 3. Mediator: Perceived Friends’ Support | ||||||
| Total effect | 0.312 | 0.119 | 0.106 | 0.504 | 0.012 | 0.253 |
| Total indirect | 0.068 | 0.046 | 0.000 | 0.084 | 0.102 | |
| Direct effect | 0.243 | 0.120 | 0.021 | 0.259 | 0.045 | |
| Model 4. Mediator: Perceived Significant Others’ Support | ||||||
| Total effect | 0.310 | 0.119 | 0.137 | 0.475 | 0.003 | 0.198 |
| Total indirect | 0.050 | 0.032 | 0.000 | 0.110 | 0.085 | |
| Direct effect | 0.261 | 0.104 | 0.087 | 0.430 | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karawekpanyawong, N.; Wongpakaran, T.; Wongpakaran, N.; Boonnag, C.; Siritikul, S.; Chalanunt, S.; Kuntawong, P. Impact of Perceived Social Support on the Relationship between ADHD and Depressive Symptoms among First Year Medical Students: A Structural Equation Model Approach. Children 2021, 8, 401. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050401
Karawekpanyawong N, Wongpakaran T, Wongpakaran N, Boonnag C, Siritikul S, Chalanunt S, Kuntawong P. Impact of Perceived Social Support on the Relationship between ADHD and Depressive Symptoms among First Year Medical Students: A Structural Equation Model Approach. Children. 2021; 8(5):401. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050401
Chicago/Turabian StyleKarawekpanyawong, Nuntaporn, Tinakon Wongpakaran, Nahathai Wongpakaran, Chiraphat Boonnag, Sirinut Siritikul, Sirikorn Chalanunt, and Pimolpun Kuntawong. 2021. "Impact of Perceived Social Support on the Relationship between ADHD and Depressive Symptoms among First Year Medical Students: A Structural Equation Model Approach" Children 8, no. 5: 401. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050401