
ADHD Symptomatology, Executive Function and Cognitive Performance Differences between Family Foster Care and Control Group in ADHD-Diagnosed Children


Abstract
:
1. Introduction
2. Materials and Methods
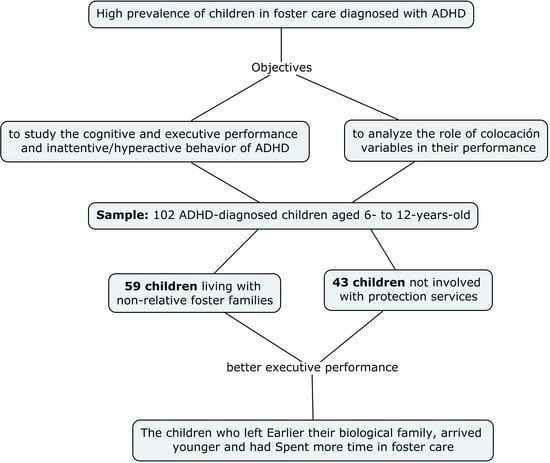
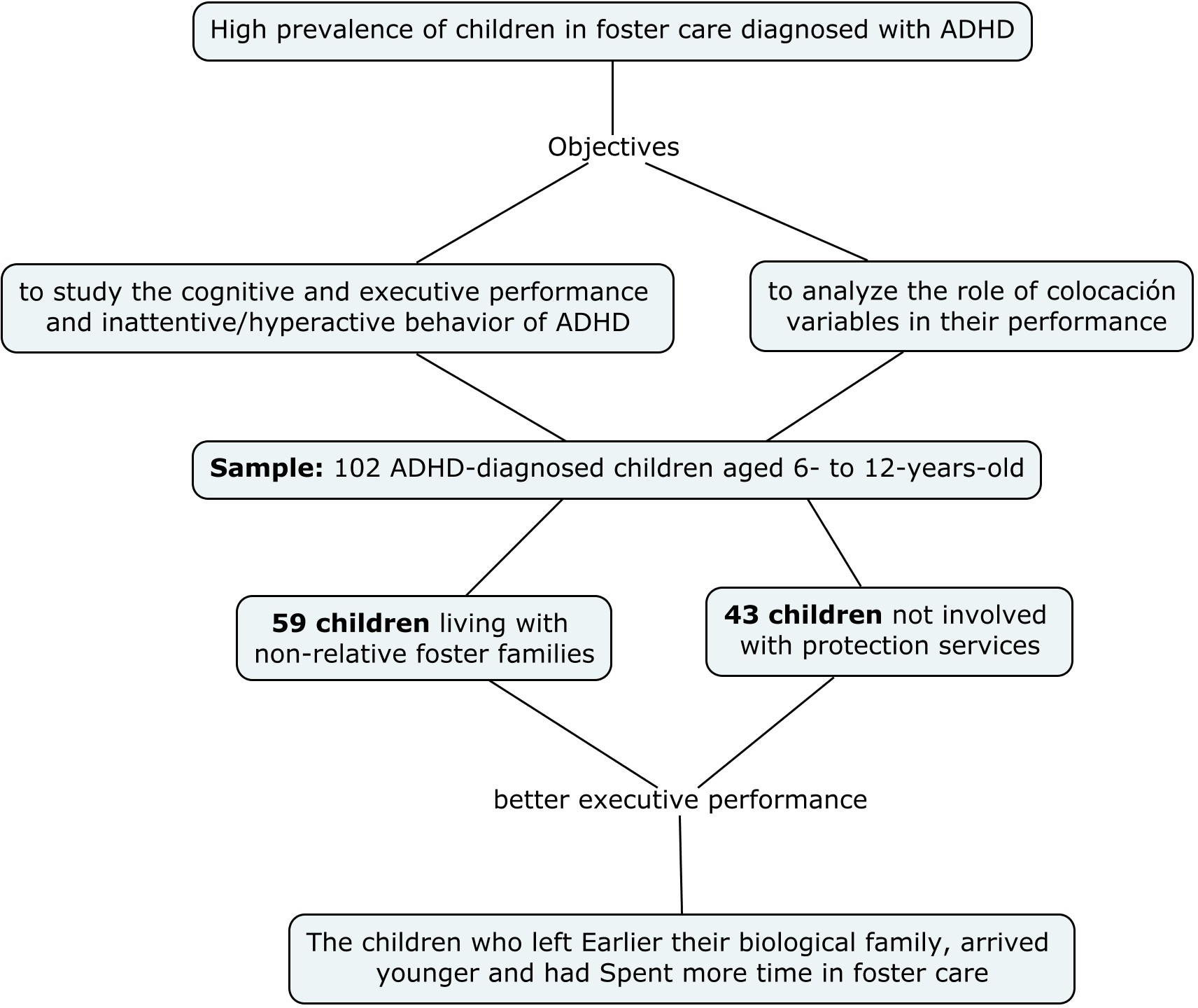
2.1. Participants
2.2. Measures
2.2.1. EF Performance
- Fluency task is an indirect measurement of working memory. The child has one minute to produce as many words as possible from both phonemic and semantic categories;
- Trail Making test assesses flexibility, inhibition, working memory and executive attention. In the gray trial, the child had to draw a line linking numbers from 20 to 1, which appeared randomly on a sheet of paper assessing working memory and executive attention. In the color version, the child must link numbers from 1 to 21, but he/she must switch between yellow and pink colors assessing to larger extent flexibility and inhibition;
- An inhibition task derived from the Stroop test assesses cognitive inhibition. A paper sheet shows three columns with 13 words in each. The words are color names printed with random color inks, but the color name and the color ink never match. The child must say the color ink of each word.
2.2.2. Intellectual Capacity
2.2.3. ADHD Symptomatology and Diagnosis
2.3. Procedure
2.4. Analytic Strategy
3. Results
3.1. Differences between Foster Care and Control Groups for ADHD Symptoms, EF Performance and Cognitive Profile
3.2. Relationship between ADHD Symptoms, EF Performance and Cognitive Profile
3.3. Relationship between ADHD Symptoms, EF Performance and Cognitive Profile with Placement History
4. Discussion and Conclusions
5. Limitations, Future Lines of Research and Practical Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- van Ijzendoorn, M.H.; Bakermans-Kranenburg, M.J.; Duschinsky, R.; Fox, N.A.; Goldman, P.S.; Gunnar, M.R.; Johnson, D.E.; Nelson, C.A.; Reijman, S.; Skinner, G.C.M.; et al. Institutionalisation and deinstitutionalisation of children 1: A systematic and integrative review of evidence regarding effects on development. Lancet Psychiatry 2020, 7, 703–720. [Google Scholar] [CrossRef]
- Observatorio de la Infancia. Boletín de datos estadísticos de medidas de protección a la infancia. In Boletín Número 22. Datos 2019; Ministerio de Sanidad, Servicios Sociales e Igualdad, Gobierno de España: Madrid, Spain, 2020. Available online: https://observatoriodelainfancia.vpsocial.gob.es/productos/pdf/BOLETIN_22_final.pdf (accessed on 13 May 2021).
- McCall, R. Research, practice, and policy perspectives on issues of children without permanent parental care. Monogr. Soc. Res. Child Dev. 2011, 76, 223–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeanah, C.; Nelson, C.; Fox, N.; Smyke, A.; Marshall, P.; Parker, S.; Koga, S. Designing research to study the effects of institutionalization on brain and behavioral development: The Bucharest Early Intervention Project. Dev. Psychopathol. 2003, 15, 885–907. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juffer, F.; Van Ijzendoorn, M.H.; Palacios, J. Recuperación de niños y niñas tras su adopción. Infanc. Aprendiz. 2011, 34, 3–18. [Google Scholar] [CrossRef]
- Amorós, P.; Palacios, J. Acogimiento Familiar; Alianza Editorial: Barcelona, Spain, 2004. [Google Scholar]
- Morago, J.M.J.; León, E.; Román, M. Adversity and Adjustment in Children in Institutions, Family Foster Care, and Adoption. Span. J. Psychol. 2015, 18. [Google Scholar] [CrossRef]
- Pollak, S.; Nelson, C.; Schlaak, M.; Roeber, B.; Wewerka, S.; Wiik, K.; Frenn, K.; Loman, M.; Gunnar, M. Neurodevelopmental Effects of Early Deprivation in Postinstitutionalized Children. Child Dev. 2010, 81, 224–236. [Google Scholar] [CrossRef] [Green Version]
- Esposito, E.; Gunnar, M. Early Deprivation and Developmental Psychopathology. In Handbook of Developmental Psychopathology; Lewis, M., Rudolph, K., Eds.; Springer: London, UK, 2014; pp. 371–388. [Google Scholar]
- Loman, M.; Gunnar, M.; The Early Experience, Stress and Neurobehavioral Development Center. Early experience and the development of stress reactivity and regulation in children. Neurosci. Biobehav. Rev. 2010, 34, 867–876. [Google Scholar] [CrossRef] [Green Version]
- Bruce, J.; Fisher, P.; Pears, K.; Levine, S. Morning cortisol Levels in preschool-aged foster children: Differential effects of maltreatment type. Dev. Psychobiol. 2009, 51, 14–23. [Google Scholar] [CrossRef] [Green Version]
- McLaughlin, K.; Fox, N.; Zeanah, C.; Sheridan, M.; Marshall, P.; Nelson, C. Delayed Maturation in Brain Electrical Activity Partially Explains the Association Between Early Environmental Deprivation and Symptoms of Attention-Deficit/Hyperactivity Disorder. Biol. Psychiatry 2010, 68, 329–336. [Google Scholar] [CrossRef] [Green Version]
- Mehta, M.; Golembo, N.; Nosarti, C.; Colvert, E.; Mota, A.; Williams, S.; Rutter, M.; Sonuga-Barke, E. Amygdala, hippocampal and corpus callosum size following severe early institutional deprivation: The English and Romanian Adoptees Study Pilot. J. Child Psychol. Psychiatry 2009, 50, 943–951. [Google Scholar] [CrossRef]
- Navarro-Soria, I.; Fenollar-Cortés, J.; Carbonell, J.; Real, M. Memoria de trabajo y velocidad de procesamiento evaluado mediante WISC-IV como claves en la evaluación del TDAH. Rev. Psicol. Clín. Niños Adolesc. 2019, 7, 23–29. [Google Scholar] [CrossRef]
- Tarren-Sweeney, M. An Investigation of Complex Attachment- and Trauma-Related Symptomatology Among Children in Foster and Kinship Care. Child Psychiatry Hum. Dev. 2013, 44, 727–741. [Google Scholar] [CrossRef]
- Tibu, F.; Sheridan, M.; McLaughlin, K.; Nelson, C.; Fox, N.; Zeanah, C. Reduced Working Memory Mediates the Link between Early Institutional Rearing and Symptoms of ADHD at 12 Years. Front. Psychol. 2016, 7, 1850. [Google Scholar] [CrossRef] [Green Version]
- Stevens, S.; Sonuga-Barke, E.; Kreppner, J.; Beckett, C.; Castle, J.; Colvert, E.; Groothues, C.; Hawkins, A.; Rutter, M. Inattention/Overactivity Following Early Severe Institutional Deprivation: Presentation and Associations in Early Adolescence. J. Abnorm. Child Psychol. 2008, 36, 385–398. [Google Scholar] [CrossRef] [Green Version]
- Oswald, S.; Heil, K.; Goldbeck, L. History of Maltreatment and Mental Health Problems in Foster Children: A Review of the Literature. J. Pediatr. Psychol. 2010, 35, 462–472. [Google Scholar] [CrossRef] [Green Version]
- Polanczyk, G.; Salum, G.; Sugaya, L.; Caye, A.; Rohde, L. Annual Research Review: A meta-analysis of the worldwide prevalence of mental disorders in children and adolescents. J. Child Psychol. Psychiatry 2015, 56, 345–365. [Google Scholar] [CrossRef]
- Vargas, M.; Martínez-Montoro, J.; Martínez, S.; Fernández-López, L.; Checa, A.; Molina-Carballo, A.; Muñoz-Hoyos, A. Estudio de prevalencia del trastorno por déficit de atención e hiperactividad en niños en régimen de acogimiento residencial. Rev. Psiquiatr. Infanto Juv. 2017, 34, 332–350. [Google Scholar] [CrossRef] [Green Version]
- Rubin, D.; Matone, M.; Huang, Y.; Dosreis, S.; Feudtner, C.; Localio, R. Interstate variation in trends of psychotropic medication use among Medicaid-enrolled children in foster care. Child. Youth Serv. Rev. 2012, 34, 1492–1499. [Google Scholar] [CrossRef] [Green Version]
- Dosreis, S.; Zito, J.; Safer, D.; Soeken, K. Mental health services for youths in foster care and disabled youths. Am. J. Public Health 2001, 91, 1094–1099. [Google Scholar] [CrossRef] [Green Version]
- Thapar, A.; Cooper, M.; Eyre, O.; Langley, K. What have we learnt about the causes of ADHD? J. Child Psychol. Psychiatry 2012, 54, 3–16. [Google Scholar] [CrossRef] [Green Version]
- Klein, B.; Damiani-Taraba, G.; Koster, A.; Campbell, J.; Scholz, C. Diagnosing attention-deficit hyperactivity disorder (ADHD) in children involved with child protection services: Are current diagnostic guidelines acceptable for vulnerable populations? Child Care Health Dev. 2015, 41, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Lewis-Morrarty, E.; Dozier, M.; Bernard, K.; Terracciano, S.; Moore, S. Cognitive Flexibility and Theory of Mind Outcomes Among Foster Children: Preschool Follow-Up Results of a Randomized Clinical Trial. J. Adolesc. Health 2012, 51, S17–S22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pears, K.; Fisher, P. Developmental, Cognitive, and Neuropsychological Functioning in Preschool-aged Foster Children. J. Dev. Behav. Pediatr. 2005, 26, 112–122. [Google Scholar] [CrossRef] [PubMed]
- Gioia, G.A.; Isquith, P.K.; Guy, S.C.; Kenworthy, L. Test Review Behavior Rating Inventory of Executive Function. Child Neuropsychol. 2000, 6, 235–238. [Google Scholar] [CrossRef]
- Carrera, P.; Jiménez-Morago, J.; Román, M.; León, E. Caregiver ratings of executive functions among foster children in middle childhood: Associations with early adversity and school adjustment. Child. Youth Serv. Rev. 2019, 106, 104495. [Google Scholar] [CrossRef]
- Leslie, L.; Gordon, J.; Meneken, L.; Premji, K.; Michelmore, K.; Ganger, W. The Physical, Developmental, and Mental Health Needs of Young Children in Child Welfare by Initial Placement Type. J. Dev. Behav. Pediatr. 2005, 26, 177–185. [Google Scholar] [CrossRef] [Green Version]
- Tarren-Sweeney, M. Predictors of Problematic Sexual Behavior Among Children With Complex Maltreatment Histories. Child Maltreat. 2008, 13, 182–198. [Google Scholar] [CrossRef]
- Viezel, K.; Freer, B.; Lowell, A.; Castillo, J. Cognitive abilities of maltreated children. Psychol. Sch. 2015, 52, 92–106. [Google Scholar] [CrossRef]
- Berger, L.; Bruch, S.; Johnson, E.; James, S.; Rubin, D. Estimating the “Impact” of Out-of-Home Placement on Child Well-Being: Approaching the Problem of Selection Bias. Child Dev. 2009, 80, 1856–1876. [Google Scholar] [CrossRef] [Green Version]
- Teicher, M.; Andersen, S.; Polcari, A.; Anderson, C.; Navalta, C.; Kim, D. The neurobiological consequences of early stress and childhood maltreatment. Neurosci. Biobehav. Rev. 2003, 27, 33–44. [Google Scholar] [CrossRef]
- Nelson, C.; Bos, K.; Gunnar, M.; Sonuga-Barke, E. The neurobiological toll of early human deprivation. Monogr. Soc. Res. Child Dev. 2011, 76, 127–146. [Google Scholar] [CrossRef] [Green Version]
- Peñarrubia, M. Función Ejecutiva en Niños y Niñas Adoptados Internacionalmente y su Relación con el Desarrollo Socioemocional. Master’s Thesis, University of Seville, Sevilla, Spain, 2015. [Google Scholar]
- Navarro-Soria, I.; Servera, M.; Burns, L. Association of Foster Care and its Duration with Clinical Symptoms and Impairment: Foster Care versus Non-Foster Care Comparisons with Spanish Children. J. Child Fam. Stud. 2019, 29, 526–533. [Google Scholar] [CrossRef] [Green Version]
- Wretham, A.E.; Woolgar, M. Do children adopted from British foster care show difficulties in executive functioning and social communication? Adopt. Foster. 2017, 41, 331–345. [Google Scholar] [CrossRef]
- Li, M.; Shrout, P.; Ramirez-Gaite, M.; Hope, S.; Albert, A.; Linares, L.; Castellanos, F. The Course of Inattention and Hyperactivity/Impulsivity Symptoms After Foster Placement. Pediatrics 2010, 125, e489–e498. [Google Scholar] [CrossRef]
- Willcutt, E.; Nigg, J.; Pennington, B.; Solanto, M.; Rohde, L.; Tannock, R.; Loo, S.; Carlson, C.; McBurnett, K.; Lahey, B. Validity of DSM-IV attention deficit/hyperactivity disorder symptom dimensions and subtypes. J. Abnorm. Psychol. 2012, 121, 991–1010. [Google Scholar] [CrossRef]
- DuPaul, G.; Power, T.; Anastopoulos, A.; Reid, R. ADHD Rating Scale-IV: Checklists, Norms, and Clinical Interpretation; Guilford: New York, NY, USA, 1998. [Google Scholar]
- Cianchetti, C.; Pittau, A.; Carta, V.; Campus, G.; Littarru, R.; Ledda, M.G.; Zuddas, A.; Fancello, G.S. Child and Adolescent Behavior Inventory (CABI): A New Instrument for Epidemiological Studies and Pre-Clinical Evaluation. Clin. Pract. Epidemiol. Ment. Health 2013, 9, 51–61. [Google Scholar] [CrossRef]
- Fenollar-Cortés, J.; Navarro-Soria, I.; González-Gómez, C.; García-Sevilla, J. Cognitive Profile for Children with ADHD by Using WISC-IV: Subtype Differences? Detección de perfiles cognitivos mediante WISC-IV en niños diagnosticados de TDAH: ¿Existen diferencias entre subtipos? Rev. Psicodidáct. 2015, 20, 157–176. [Google Scholar] [CrossRef] [Green Version]
- Portellano, J.A.; Martínez-Arias, R.; Zumárraga, L. ENFEN: Evaluación Neuropsicológica de las Funciones Ejecutivas en Niños; TEA Ediciones: Madrid, Spain, 2009. [Google Scholar]
- Baddeley, A. Working memory. Science 1992, 255, 556–559. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.; Emerson, M.; Witzki, A.; Howerter, A.; Wager, T. The Unity and Diversity of Executive Functions and Their Contributions to Complex “Frontal Lobe” Tasks: A Latent Variable Analysis. Cogn. Psychol. 2000, 41, 49–100. [Google Scholar] [CrossRef] [Green Version]
- Anderson, P. Assessment and Development of Executive Function (EF) During Childhood. Child Neuropsychol. 2020, 8, 71–82. [Google Scholar] [CrossRef]
- Scott, W. Cognitive Complexity and Cognitive Flexibility. Sociometry 1962, 25, 405. [Google Scholar] [CrossRef]
- Maldonado, E.; Nislin, M.; Marín, L.; Martín-Escribano, A.; Enguix, A.; López, C.; Magarín, A.; Álamo, A.; Ortíz, P.; Muñoz, M.; et al. Association between Salivary Alpha-Amylase and Executive Functioning in Healthy Children. Span. J. Psychol. 2019, 22, E24. [Google Scholar] [CrossRef]
- Wechsler, D. Escala de Inteligencia de Wechsler Para Niños-IV (WISC-IV); Pearson: Barcelona, Spain, 2003. [Google Scholar]
- Wechsler, D. Manual Técnico y de Interpretación. In Escala de Inteligencia de Wechsler Para Niños–IV (WISC-IV); Pearson: Barcelona, Spain, 2005. [Google Scholar]
- Fenollar-Cortés, J.; López-Pinar, C.; Watkins, M.W. Structural validity of the Spanish Wechsler Intelligence Scale for Children—Fourth Edition in a large sample of Spanish children with attention-deficit hyperactivity disorder. Int. J. Sch. Educ. Psychol. 2019, 7 (Suppl. 1), 2–14. [Google Scholar] [CrossRef]
- Barceló, M.S.; Jalón, E.C. ADHD Rating Scale-IV en una muestra escolar española: Datos normativos y consistencia interna para maestros, padres y madres. Rev. Neurol. 2007, 45, 393. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: New York, NY, USA, 1994. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum: London, UK, 1998. [Google Scholar]
- Cohen, J.; Cohen, P.; West, S.; Aiken, L. Applied Multiple Regression/Correlation Analysis for the Behavioral Science, 3rd ed.; Lawrence Erlbaum Associates: London, UK, 2003. [Google Scholar]
- Sattler, J. Assessment of Children: Cognitive Foundations, 5th ed.; Jerome, M., Ed.; Sattler: London, UK, 2008. [Google Scholar]
- Devena, S.; Watkins, M. Diagnostic Utility of WISC-IV General Abilities Index and Cognitive Proficiency Index Difference Scores Among Children With ADHD. J. Appl. Sch. Psychol. 2012, 28, 133–154. [Google Scholar] [CrossRef] [Green Version]
- Moura, O.; Costa, P.; Simões, M. WISC-III Cognitive Profiles in Children with ADHD: Specific Cognitive Impairments and Diagnostic Utility. J. Gen. Psychol. 2019, 146, 258–282. [Google Scholar] [CrossRef] [PubMed]
- Durbeej, N.; Hellner, C. Improving school performance among Swedish foster children: A quasi-experimental study exploring outcomes of the Skolfam model. Child. Youth Serv. Rev. 2017, 82, 466–476. [Google Scholar] [CrossRef]
- Fox, N.; Almas, A.; Degnan, K.; Nelson, C.; Zeanah, C. The effects of severe psychosocial deprivation and foster care intervention on cognitive development at 8 years of age: Findings from the Bucharest Early Intervention Project. J. Child Psychol. Psychiatry 2011, 52, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Soria, I.; De Mier, R.J.-R.; García-Fernández, J.; González-Gómez, C.; Real-Fernández, M.; De León, M.S.-M.; Lavigne-Cervan, R. Detection of Executive Performance Profiles Using the ENFEN Battery in Children Diagnosed with Attention-Deficit Hyperactivity Disorder. Front. Psychol. 2020, 11, 552322. [Google Scholar] [CrossRef]
- Hurks, P.; Hendriksen, J.; Vles, J.; Kalff, A.; Feron, F.; Kroes, M.; van Zeben, T.; Steyaert, J.; Jolles, J. Verbal fluency over time as a measure of automatic and controlled processing in children with ADHD. Brain Cogn. 2004, 55, 535–544. [Google Scholar] [CrossRef]
- Pennington, B.; Ozonoff, S. Executive Functions and Developmental Psychopathology. J. Child Psychol. Psychiatry 1996, 37, 51–87. [Google Scholar] [CrossRef]
- Martel, M.; Nikolas, M.; Nigg, J. Executive Function in Adolescents With ADHD. J. Am. Acad. Child Adolesc. Psychiatry 2007, 46, 1437–1444. [Google Scholar] [CrossRef]
- McAuley, T.; Chen, S.; Goos, L.; Schachar, R.; Crosbie, J. Is the behavior rating inventory of executive function more strongly associated with measures of impairment or executive function? J. Int. Neuropsychol. Soc. 2010, 16, 495–505. [Google Scholar] [CrossRef]
- Gunnar, M.; Quevedo, K. The Neurobiology of Stress and Development. Annu. Rev. Psychol. 2007, 58, 145–173. [Google Scholar] [CrossRef] [Green Version]
- Coker, T.; Elliott, M.; Toomey, S.; Schwebel, D.; Cuccaro, P.; Emery, S.; Davies, S.; Visser, S.; Schuster, M. Racial and Ethnic Disparities in ADHD Diagnosis and Treatment. Pediatrics 2016, 138, e20160407. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
| Variables M (SD) | Foster Group | Control Group | χ2/t/U † | p | Effect Size | |
|---|---|---|---|---|---|---|
| n | 59 | 43 | ||||
| Gender n (% male) | 47 (79.7) | 34 (79.1) | 0.005 | 0.566 | ||
| Age (years) | 8.29 (1.92) | 8.30 (2.0) | 0.04 | 0.971 | ||
| ADHD combined presentation n (%) | 37 (62.7) | 22 (51.2) | 1.36 | 0.311 | ||
| ADHD predominantly inattentive presentation n (%) | 22 (37.3) | 21 (48.8) | ||||
| ADHD symptomatology (ADHD-RS-IV) | ||||||
| Teacher form (raw scores) | ||||||
| Inattention | 7.64 (1.41) | 7.00 (1.23) | 1.600 | 0.018 | 0.26 ‡ | |
| Hyp/imp | 4.78 (3.55) | 3.51 (3.21) | 1.527 | 0.077 | ||
| Family form (raw scores) | ||||||
| Inattention | 7.76 (1.36) | 7.42 (1.50) | 1.427 | 0.265 | ||
| Hyp/imp | 4.92 (3.30) | 4.35 (3.09) | 1.390 | 0.411 | ||
| Cognitive performance (WISC-IV; IQ scores) | ||||||
| Verbal comprehension | 104.0 (11.2) | 108.8 (13.6) | 1.959 | 0.053 | ||
| Perceptual reasoning | 98.9 (12.6) | 101.3 (12.2) | 0.987 | 0.330 | ||
| Working memory | 86.2 (11.8) | 91.2 (14.5) | 1.925 | 0.057 | ||
| Processing speed | 91.7 (12.6) | 93.9 (12.8) | 0.858 | 0.393 | ||
| General ability index | 99.7 (12.2) | 105.0 (12.5) | 2.126 | 0.036 | 0.43 § | |
| Cognitive proficiency index | 86.4 (12.6) | 89.0 (13.9) | 0.970 | 0.334 | ||
| Full Scale IQ | 94.3 (10.8) | 98.4 (12.2) | 1.762 | 0.081 | ||
| Executive performance (ENFEN; sten scores) | ||||||
| Phonemic fluency | 3.78 (1.86) | 4.40 (1.94) | 1.021 | 0.090 | ||
| Semantic fluency | 5.64 (2.02) | 6.44 (2.18) | 0.984 | 0.051 | ||
| Gray trail | 4.53 (2.56) | 4.91 (2.55) | 1.155 | 0.438 | ||
| Color trail | 2.92 (1.97) | 3.12 (1.88) | 1.170 | 0.494 | ||
| Interference | 3.70 (1.94) | 3.70 (1.70) | 1.218 | 0.731 | ||
| EF Outcomes | Time with Biological Family | Age at Entry into Residential Care | Age at Placement into Foster Family | Time with Foster Family |
|---|---|---|---|---|
| Gray Trail | −0.33 * | −0.32 * | −0.36 * | 0.36 ** |
| Color Trail | −0.34 ** | −0.34 ** | −0.44 *** | 0.43 *** |
| Interference | −0.27 * | −0.05 | −0.04 | 0.26 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Peñarrubia, M.; Navarro-Soria, I.; Palacios, J.; Fenollar-Cortés, J. ADHD Symptomatology, Executive Function and Cognitive Performance Differences between Family Foster Care and Control Group in ADHD-Diagnosed Children. Children 2021, 8, 405. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050405
Peñarrubia M, Navarro-Soria I, Palacios J, Fenollar-Cortés J. ADHD Symptomatology, Executive Function and Cognitive Performance Differences between Family Foster Care and Control Group in ADHD-Diagnosed Children. Children. 2021; 8(5):405. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050405
Chicago/Turabian StylePeñarrubia, María, Ignasi Navarro-Soria, Jesús Palacios, and Javier Fenollar-Cortés. 2021. "ADHD Symptomatology, Executive Function and Cognitive Performance Differences between Family Foster Care and Control Group in ADHD-Diagnosed Children" Children 8, no. 5: 405. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050405