
Perceptions of Family-Level Social Factors That Influence Health Behaviors in Latinx Adolescents and Young Adults at High Risk for Type 2 Diabetes

 , and
, and
Abstract
:1. Introduction
Familial Influences in Youth Health-Related Behaviors
2. Materials and Methods
2.1. Participants
2.2. Interview Procedures
2.3. Interview Guide
2.4. Qualitative Data Analysis
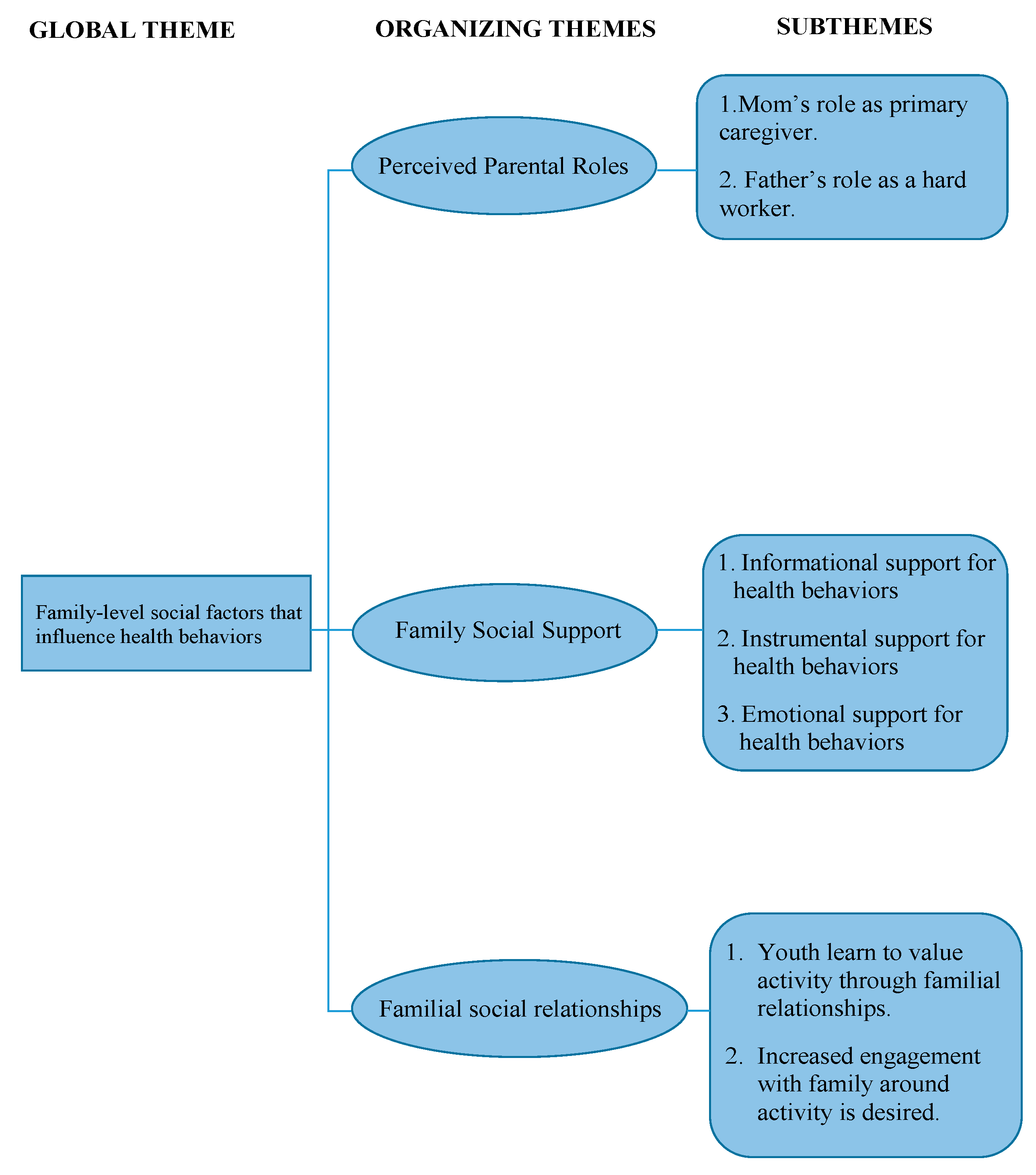
3. Results
3.1. Theme 1. The Influence of Perceived Parental Roles and Responsibilities on Health Behaviors
3.1.1. Subtheme 1: Mom’s Role as Primary Caregiver Influences Health Behaviors
“I’d say my mom definitely is a big one. She would always take us hiking, or ... She would try to do things with us.”—Adolescent female
“…having all these kids and then every day waking up early, making my dad food. At some point we had three uncles living with us, she’d wake up earlier just to get them food and then me and my sister would wake up and she gives us food and then we go to school. When we get back, she already has food prepared. Mothers are one of the hardest workers I think we have.”—Adolescent male
“My mom would either have to work late or work on the weekends...I barely even sometimes get to talk to her cause she has to take care of the kids, or run some errands, and clean the house.”—Adolescent female
“My mom, when we were in the program [health promotion program], she would go with us, and she would take us…but I feel like she has a lot of responsibilities around the house, and like, well, now that she has the baby, it’s different, ‘cause when she had the baby, we had to start going by ourselves to the program.”—Adolescent female
“She usually is the one that does the grocery shopping so we eat healthier. Yeah, she’s the cook.”—Young adult female
“Just putting more work on me, taking care of my brother and my sister or, “Go do this for me,” or, “Go do that for me.” That doesn’t give me time to do a bunch of what I would like to do, but just the fact that I have to help them [parents] out with most of the chores at the house, the driving here and there… It doesn’t give me enough time to do activities that I would like.”—Young adult female
3.1.2. Subtheme 2: Dad’s Role as a Hard Worker Influences Health Behaviors
“…he [dad] still does a pretty laborious job, like construction, he still does that to feed everyone in the house. And seeing that makes me want to work hard as well…instead of him always taking care of us, I could take care of them [participant’s family] as well.”—Adolescent male
“Well, my dad, I feel because he’s not really around the house, because he works a lot, and he gets home tired. I don’t spend a lot of time with him. My brother is maybe the one that spends a little bit more time with him, because either they do yard work, or something together…”—Adolescent female
“My dad works from 8:00 in the morning to 6:00… I don’t really care because I’m not as close to him, because I barely see him, and he doesn’t get me.”—Adolescent female
“My Dad, always on his feet, never stops… He just runs the restaurant, non-stop…For sure my dad can work and at times when he gets home, he might want to rest, most of the time. That’s when, he’s just exhausted…”—Young adult male
“He [participant’s dad] just works and goes to sleep. I don’t really see him throughout the week except for Saturday and Sunday. Throughout the week he works. He leaves early in the morning. He comes back mid-afternoon. He stays sleeping. I get home like at six. I don’t really see him.”—Young adult female
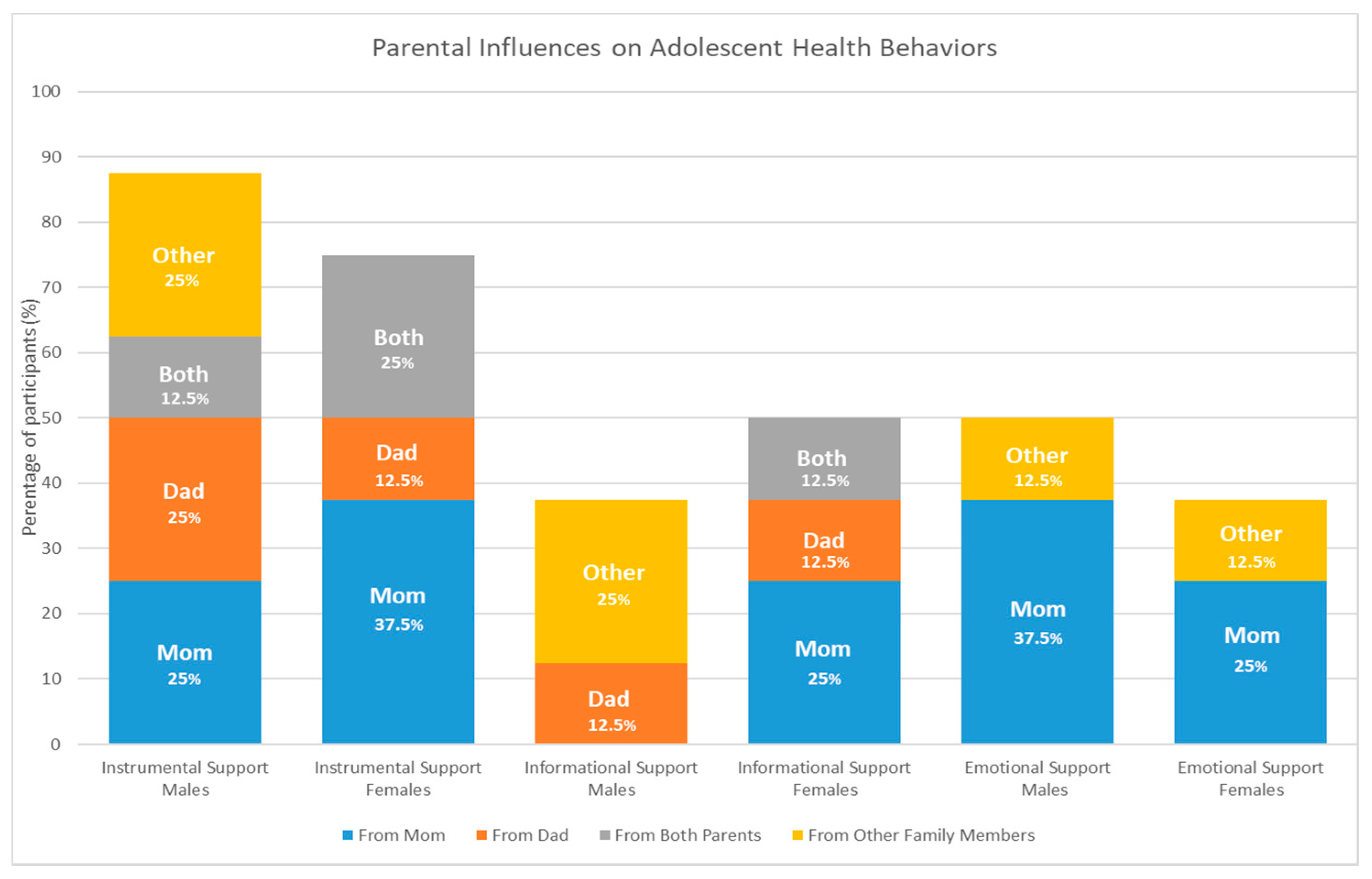
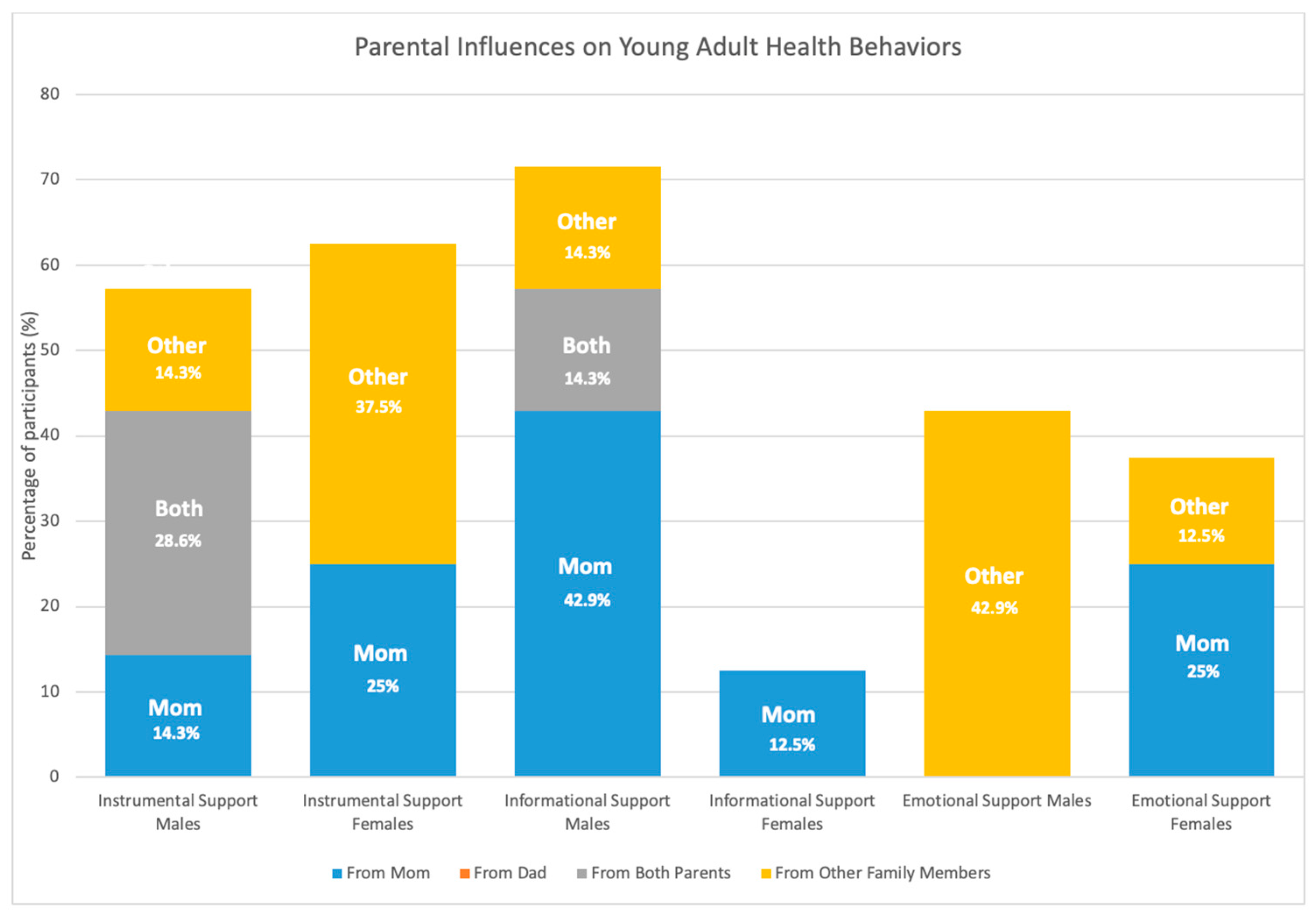
3.2. Theme 2: Perceived Family Social Support for Health Behaviors
3.2.1. Subtheme 1: Informational Social Support for Health Behaviors
“Also, my little brother, he would always tell me, ‘cause over there at school, there’s really bad breakfast so he would say, “Choose the best cereal and stuff. If there’s none that are good, then you better not get some…” On Fridays they always do cinnamon rolls and donuts or pop-tarts, he says, “Just get cereal” and I said, “Okay.”—Adolescent male
“My mom was always telling me to eat my fruits and vegetables, and she’s making us take vitamins… She always makes our food, so she puts like vegetables in there… She’s always telling me to exercise with her.”—Adolescent female
“My Mama. She’s the one who always like tells me to get up and do something [physically active].”—Young adult male
3.2.2. Subtheme 2: Instrumental Social Support for Health Behaviors
“We [participant and dad] play soccer together once or twice a week.”—Adolescent male
“I mean, my mom will go to the grocery store, and she lets me pick out the things that I wanna buy, like when it comes to like fruits or vegetables…or sometimes, she helps me prepare different meals. Definitely, my mom is one of the main people that helps me and encourages me to eat better and to exercise.”—Adolescent female
“She [participant’s mom] goes to the gym four times a week, so, yeah. She is a good example.”—Young adult male
“Usually we [participant and participant’s mom] take walks every afternoon. Probably that’s like the only time that I feel active…We just go to the park, walk around with the dogs.”—Young adult female
3.2.3. Subtheme 3: Emotional Social Support for Health Behaviors
“Recently, she [participant’s mom] talked to me, she’s like, “I know you don’t like being the way how you are,” Cause I tell her I don’t feel good, cause you can feel the weight difference. So yeah. And she was like, “You know, you should do it [lose the weight]. I know you can do it.”—Adolescent male
“Because she [participant’s mom] cares about me, and she cares about my health and my goals…Like, I tell her my goals, and she wants to help me to get where I wanna be.”—Adolescent female
“For sure, they [participant’s family members] tell me, as well, ‘Keep it up, you’re doing good’…I have their support, as well. So that’s a good thing that I get to have to motivate me to go to the gym every day.”—Young adult male
“I think it’s just my mom, she tells me like, when I was working out, she’s like ‘oh I like seeing you be active, I like seeing you drink more water’, and stuff like that.”—Young adult female
3.3. Theme 3: Familial Social Relationships Are Central to Health Behaviors
3.3.1. Subtheme 1: The Value of Activity Is Learned through Familial Relationships
“My dad, he thinks that it [physical activity] was so important that he made a soccer team with me...He’s the coach.”—Adolescent male
“I think they see it already. I think they’re always active, and they motivate me to be active with them…so then I’m going to be active too…and I get two things at the same time, spending time and then being active”—Adolescent female
“Now that we’re a little older, we’re not all together… My brother goes to school and my sister goes to school. My brother gets home at like six because of his sports. My sister gets home at like five because she stays after school for something. Then my dad, he gets home from work but he goes straight to sleep… so we’re not always together during the weekdays. I think the only day that we are all together is on a Sunday. Changing that to being together the whole week and trying to figure out, “Hey, what are we going to eat all together? What should we make, something different, something a little more healthier?” Just not doing our own thing all the time.”—Young adult female
“For sure, when I was younger, I was way more active with my family. Walking around, going places and things like that….”—Young adult male
3.3.2. Subtheme 2: Increased Engagement with Family around Activity Is Desired
“I wish we could just have more time to be with each other... a little less time working and more time focusing on what activity we should do together as a family.”—Adolescent female
“I wish we would do more active things. I wish I could go with them to the zoo, walk around, hang out at the mall. It’s just our conflicting lives and schedules.”—Young adult male
4. Discussion
4.1. Influence of Traditional Gender Roles
4.2. Effects of Social Support
4.3. Effects of Familial Social Relationships
4.4. Directions for Future Research with Latinx Families
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Narayan, K.M.V.; Boyle, J.P.; Thompson, T.J.; Sorensen, S.W.; Williamson, D.F. Lifetime Risk for Diabetes Mellitus in the United States. JAMA 2003, 290, 1884–1890. [Google Scholar] [CrossRef] [Green Version]
- Skinner, A.C.; Ravanbakht, S.N.; Skelton, J.A.; Perrin, E.M.; Armstrong, S.C. Prevalence of obesity and severe obesity in US children, 1999–2016. Pediatrics 2018, 141, e20173459. [Google Scholar] [CrossRef] [Green Version]
- Menke, A.; Casagrande, S.; Cowie, C.C. Prevalence of diabetes in adolescents aged 12 to 19 years in the United States, 2005–2014. JAMA 2016, 316, 344–345. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goran, M.I.; Ball, G.D.C.; Cruz, M.L. Obesity and Risk of Type 2 Diabetes and Cardiovascular Disease in Children and Adolescents. J. Clin. Endocrinol. Metab. 2003, 88, 1417–1427. [Google Scholar] [CrossRef] [Green Version]
- Hagman, E.; Danielsson, P.; Brandt, L.; Ekbom, A.; Marcus, C. Association between impaired fasting glycaemia in pediatric obesity and type 2 diabetes in young adulthood. Nutr. Diabetes 2016, 6, e227. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Constantino, M.I.; Molyneaux, L.; Limacher-Gisler, F.; Al-Saeed, A.; Luo, C.; Wu, T.; Twigg, S.M.; Yue, D.K.; Wong, J. Long-term complications and mortality in young-onset diabetes: Type 2 diabetes is more hazardous and lethal than type 1 diabetes. Diabetes Care 2013, 36, 3863–3869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cha, E.; Umpierrez, G.; Kim, K.H.; Bello, M.K.; Dunbar, S.B. Characteristics of American young adults with increased risk for type 2 diabetes: A pilot study. Diabetes Educ. 2013, 39, 454–463. [Google Scholar] [CrossRef] [PubMed]
- American Association of Diabetes Educators. The Art and Science of Diabetes Self-Management Education Desk Reference, 2nd ed.; American Association of Diabetes Educators: Chicago, IL, USA, 2011. [Google Scholar]
- McCurley, J.L.; Crawford, M.A.; Gallo, L.C. Prevention of type 2 diabetes in U.S. Hispanic youth: A systematic review of lifestyle interventions. Am. J. Prev. Med. 2017, 53, 519–532. [Google Scholar] [CrossRef] [PubMed]
- McCurley, J.L.; Gutierrez, A.P.; Gallo, L.C. Diabetes prevention in U.S. Hispanic adults: A systematic review of culturally tailored interventions. Am. J. Prev. Med. 2017, 52, 519–529. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, J.O.; Galloway, J.M.; Goley, A.; Marrero, D.G.; Minners, R.; Montgomery, B.; Peterson, G.E.; Ratner, R.E.; Sanchez, E.; Aroda, V.R. Scientific statement: Socioecological determinants of prediabetes and type 2 diabetes. Diabetes Care 2013, 36, 2430–2439. [Google Scholar] [CrossRef] [Green Version]
- Wilson, D.K. New perspectives on health disparities and obesity interventions in youth. J. Pediatr. Psychol. 2009, 34, 231–244. [Google Scholar] [CrossRef] [PubMed]
- Castro, F.G.; Shaibi, G.Q.; Boehm-Smith, E. Ecodevelopmental contexts for preventing type 2 diabetes in Latino and other racial/ethnic minority populations. J. Behav. Med. 2009, 32, 89–105. [Google Scholar] [CrossRef] [Green Version]
- McWayne, C.M.; Melzi, G.; Limlingan, M.C.; Schick, A. Ecocultural patterns of family engagement among low-income Latino families of preschool children. Dev. Psychol. 2016, 52, 1088–1102. [Google Scholar] [CrossRef] [PubMed]
- Vélez-Agosto, N.M.; Soto-Crespo, J.G.; Vizcarrondo-Oppenheimer, M.; Vega-Molina, S.; Coll, C.G. Bronfenbrenner’s bioecological theory revision: Moving culture from the macro Into the micro. Perspect. Psychol. Sci. 2017, 12, 900–910. [Google Scholar] [CrossRef] [PubMed]
- Davison, K.K.; Jurkowski, J.M.; Lawson, H.A. Reframing family-centred obesity prevention using the Family Ecological Model. Public Health Nutr. 2013, 16, 1861–1869. [Google Scholar] [CrossRef] [Green Version]
- Wilson, D.K.; Sweeney, A.M.; Kitzman-Ulrich, H.; Gause, H.; St George, S.M. Promoting social nurturance and positive social environments to reduce obesity in high-risk youth. Clin. Child. Fam. Psychol. Rev. 2017, 20, 64–77. [Google Scholar] [CrossRef] [Green Version]
- Lebron, C.N.; Lee, T.K.; Park, S.E.; St George, S.M.; Messiah, S.E.; Prado, G. Effects of parent-adolescent reported family functioning discrepancy on physical activity and diet among Hispanic youth. J. Fam. Psychol. 2018, 32, 333–342. [Google Scholar] [CrossRef]
- Ochoa, A.; Berge, J.M. Home environmental influences on childhood obesity in the Latino population: A decade review of literature. J. Immigr. Minor. Health 2017, 19, 430–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindsay, A.C.; Wasserman, M.; Muñoz, M.A.; Wallington, S.F.; Greaney, M.L. Examining influences of parenting styles and practices on physical activity and sedentary behaviors in Latino children in the United States: Integrative review. JMIR Public Health Surveill. 2018, 4, e14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beets, M.W.; Cardinal, B.J.; Alderman, B.L. Parental social support and the physical activity-related behaviors of youth: A review. Health Educ. Behav. 2010, 37, 621–644. [Google Scholar] [CrossRef]
- Donnelly, R.; Springer, A. Parental social support, ethnicity, and energy balance-related behaviors in ethnically diverse, low-income, urban elementary schoolchildren. J. Nutr. Educ. Behav. 2015, 47, 10–18. [Google Scholar] [CrossRef] [Green Version]
- Thompson, R.A.; Flood, M.F.; Goodvin, R. Social support and developmental psychopathology. In Developmental Psychopathology: Volume Three: Risk, Disorder, and Adaptation; Cicchetti, D., Cohen, D.J., Eds.; John Wiley & Sons: Hoboken, NJ, USA, 2006; pp. 1–37. [Google Scholar]
- Langer, S.L.; Crain, A.L.; Senso, M.M.; Levy, R.L.; Sherwood, N.E. Predicting child physical activity and screen time: Parental support for physical activity and general parenting styles. J. Pediatr. Psychol. 2014, 39, 633–642. [Google Scholar] [CrossRef] [Green Version]
- Patrick, H.; Hennessy, E.; McSpadden, K.; Oh, A. Parenting styles and practices in children’s obesogenic behaviors: Scientific gaps and future research directions. Child. Obes. 2013, 9 (Suppl. S1), S73–S86. [Google Scholar] [CrossRef] [Green Version]
- Arredondo, E.M.; Elder, J.P.; Ayala, G.X.; Campbell, N.; Baquero, B.; Duerksen, S. Is parenting style related to children’s healthy eating and physical activity in Latino families? Health Educ. Res. 2006, 21, 862–871. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hennessy, E.; Hughes, S.O.; Goldberg, J.P.; Hyatt, R.R.; Economos, C.D. Parent-child interactions and objectively measured child physical activity: A cross-sectional study. Int. J. Behav. Nutr. Phys. Act. 2010, 7, 71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray-Johnson, L.; Witte, K.; Liu, W.Y.; Hubbell, A.P.; Sampson, J.; Morrison, K. Addressing cultural orientations in fear appeals: Promoting AIDS-protective behaviors among Mexican immigrant and African American adolescents and American and Taiwanese college students. J. Health Commun. 2001, 6, 335–358. [Google Scholar] [CrossRef]
- Marquez, B.; Elder, J.P.; Arredondo, E.M.; Madanat, H.; Ji, M.; Ayala, G.X. Social network characteristics associated with health promoting behaviors among Latinos. Health Psychol. 2014, 33, 544–553. [Google Scholar] [CrossRef] [Green Version]
- Brunet, J.; Sabiston, C.M.; O’Loughlin, J.; Mathieu, M.E.; Tremblay, A.; Barnett, T.A.; Lambert, M. Perceived parental social support and moderate-to-vigorous physical activity in children at risk of obesity. Res. Q. Exerc. Sport 2014, 85, 198–207. [Google Scholar] [CrossRef] [PubMed]
- Grieser, M.; Neumark-Sztainer, D.; Saksvig, B.I.; Lee, J.S.; Felton, G.M.; Kubik, M.Y. Black, Hispanic, and White girls’ perceptions of environmental and social support and enjoyment of physical activity. J. Sch. Health 2008, 78, 314–320. [Google Scholar] [CrossRef] [PubMed]
- Shen, B.; Centeio, E.; Garn, A.; Martin, J.; Kulik, N.; Somers, C.; McCaughtry, N. Parental social support, perceived competence and enjoyment in school physical activity. J. Sport Health Sci. 2018, 7, 346–352. [Google Scholar] [CrossRef] [Green Version]
- Flouri, E.; Buchanan, A. The role of father involvement and mother involvement in adolescents’ psychological well-being. Br. J. Soc. Work 2003, 33, 399–406. [Google Scholar] [CrossRef]
- Davison, K.K.; Jago, R. Change in parent and peer support across ages 9 to 15 yr and adolescent girls’ physical activity. Med. Sci. Sports Exerc. 2009, 41, 1816–1825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, H.F.; Shannon, S.E. Three approaches to qualitative content analysis. Qual. Health Res. 2005, 15, 1277–1288. [Google Scholar] [CrossRef]
- Bernard, H.R.; Ryan, G.W. Analyzing Qualitative Data: Systematic Approaches; Sage Publications: Thousand Oaks, CA, USA, 2009. [Google Scholar]
- Passel, J.; Cohn, D.U.S. Population Projections: 2005–2050. Available online: https://www.pewresearch.org/hispanic/2008/02/11/us-population-projections-2005-2050/ (accessed on 24 August 2020).
- Davis, R.E.; Cole, S.M.; Blake, C.E.; McKenney-Shubert, S.J.; Peterson, K.E. Eat, play, view, sleep: Exploring Mexican American mothers’ perceptions of decision making for four behaviors associated with childhood obesity risk. Appetite 2016, 101, 104–113. [Google Scholar] [CrossRef] [Green Version]
- Pharr, J.R.; Dodge Francis, C.; Terry, C.; Clark, M.C. Culture, caregiving, and health: Exploring the influence of culture on family caregiver experiences. ISRN Public Health 2014, 2014, 689826. [Google Scholar] [CrossRef] [Green Version]
- Tamez, E.G. Familism, machismo and child rearing practices among Mexican Americans. J. Psychosoc. Nurs. Ment. Health Serv. 1981, 19, 21–25. [Google Scholar] [CrossRef] [PubMed]
- Bautista, L.; Reininger, B.; Gay, J.L.; Barroso, C.S.; McCormick, J.B. Perceived barriers to exercise in Hispanic adults by level of activity. J. Phys. Act. Health 2011, 8, 916–925. [Google Scholar] [CrossRef]
- Garcia, D.O.; Valdez, L.A.; Hooker, S.P. Hispanic male’s perspectives of health behaviors related to weight management. Am. J. Men’s Health 2017, 11, 1547–1559. [Google Scholar] [CrossRef] [Green Version]
- Valdez, L.A.; Morrill, K.E.; Griffith, D.M.; Lindberg, N.M.; Hooker, S.P.; Garcia, D.O. Mexican origin Hispanic men’s perspectives of physical activity-related health behaviors. Am. J. Men’s Health 2019, 13, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Davey, C.; Larson, N.; Reicks, M. Influence of parenting styles in the context of adolescents’ energy balance-related behaviors: Findings from the FLASHE study. Appetite 2019, 142, 104364. [Google Scholar] [CrossRef]
- U.S. Bureau of Labor Statistics. Labor Force Characteristics by Race and Ethnicity. 2018. Available online: https://www.bls.gov/opub/reports/race-and-ethnicity/2018/home.htm (accessed on 24 August 2020).
- Pager, D.; Western, B.; Pedulla, D. Employment discrimination and the changing landscape of low-wage labor markets. Univ. Chic. Leg Forum 2009, 2009, 9. [Google Scholar]
- Taylor, P.; Lopez, M.H.; Martínez, J.H.; Velasco, G. When Labels Don’t Fit: Hispanics and Their Views of Identity. Available online: https://www.pewresearch.org/hispanic/2012/04/04/when-labels-dont-fit-hispanics-and-their-views-of-identity/ (accessed on 24 August 2020).
- Davison, K.K.; Cutting, T.M.; Birch, L.L. Parents’ activity-related parenting practices predict girls’ physical activity. Med. Sci. Sports Exerc. 2003, 35, 1589–1595. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laird, Y.; Fawkner, S.; Kelly, P.; McNamee, L.; Niven, A. The role of social support on physical activity behaviour in adolescent girls: A systematic review and meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2016, 13, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peterson, M.S.; Lawman, H.G.; Wilson, D.K.; Fairchild, A.; Van Horn, M.L. The association of self-efficacy and parent social support on physical activity in male and female adolescents. Health Psychol. 2013, 32, 666–674. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Updegraff, K.A.; Delgado, M.Y.; Wheeler, L.A. Exploring mothers’ and fathers’ relationships with sons versus daughters: Links to adolescent adjustment in Mexican immigrant families. Sex. Roles 2009, 60, 559–574. [Google Scholar] [CrossRef] [Green Version]
- Cruz, P.; Granados, A. Type 2 diabetes in Latino youth: A clinical update and current challenges. Curr. Probl. Pediatr. Adolesc. Health Care 2019, 49, 16–22. [Google Scholar] [CrossRef]
- Ash, T.; Agaronov, A.; Young, T.; Aftosmes-Tobio, A.; Davison, K.K. Family-based childhood obesity prevention interventions: A systematic review and quantitative content analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 113. [Google Scholar] [CrossRef]
- Lei, L.; South, S.J. Racial and ethnic differences in leaving and returning to the parental home: The role of life course transitions, socioeconomic resources, and family connectivity. Demogr. Res. 2016, 34, 109–142. [Google Scholar] [CrossRef] [Green Version]
- Larsen, B.A.; Pekmezi, D.; Marquez, B.; Benitez, T.J.; Marcus, B.H. Physical activity in Latinas: Social and environmental influences. Women’s Health (Lond.) 2013, 9, 201–210. [Google Scholar] [CrossRef] [Green Version]
- Vollmer, R.L.; Mobley, A.R. A pilot study to explore how low-income mothers of different ethnic/racial backgrounds perceive and implement recommended childhood obesity prevention messages. Child. Obes. 2013, 9, 261–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, A.; de Vlieger, N.; Young, M.; Jensen, M.E.; Burrows, T.L.; Morgan, P.J.; Collins, C.E. Dietary outcomes of overweight fathers and their children in the Healthy Dads, Healthy Kids community randomised controlled trial. J. Hum. Nutr. Diet. 2018, 31, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Lloyd, A.B.; Lubans, D.R.; Plotnikoff, R.C.; Morgan, P.J. Paternal lifestyle-related parenting practices mediate changes in children’s dietary and physical activity behaviors: Findings from the Healthy Dads, Healthy Kids community randomized controlled trial. J. Phys. Act. Health 2015, 12, 1327–1335. [Google Scholar] [CrossRef] [PubMed]
- Soltero, E.G.; Ramos, C.; Williams, A.N.; Hooker, E.; Mendez, J.; Wildy, H.; Davis, K.; Hernandez, V.; Contreras, O.A.; Silva, M.; et al. ¡Viva Maryvale!: A multilevel, multisector model to community-based diabetes prevention. Am. J. Prev. Med. 2019, 56, 58–65. [Google Scholar] [CrossRef]
- Williams, A.N.; Konopken, Y.P.; Keller, C.S.; Castro, F.G.; Arcoleo, K.J.; Barraza, E.; Patrick, D.L.; Olson, M.L.; Shaibi, G.Q. Culturally-grounded diabetes prevention program for obese Latino youth: Rationale, design, and methods. Contemp. Clin. Trials 2017, 54, 68–76. [Google Scholar] [CrossRef] [Green Version]
- Herzer, M.; Zeller, M.H.; Rausch, J.R.; Modi, A.C. Perceived social support and its association with obesity-specific health-related quality of life. J. Dev. Behav. Pediatr. 2011, 32, 188–195. [Google Scholar] [CrossRef]
- Teufel-Shone, N.I.; Drummond, R.; Rawiel, U. Developing and adapting a family-based diabetes program at the U.S.-Mexico border. Prev. Chronic. Dis. 2005, 2, A20. [Google Scholar]
- Soltero, E.G.; Olson, M.L.; Williams, A.N.; Konopken, Y.P.; Castro, F.G.; Arcoleo, K.J.; Keller, C.S.; Patrick, D.L.; Ayers, S.L.; Barraza, E.; et al. Effects of a community-based diabetes prevention program for Latino youth with obesity: A randomized controlled trial. Obesity (Silver Spring) 2018, 26, 1856–1865. [Google Scholar] [CrossRef]
- O’Connor, T.; Perez, O.; Garcia, I.C.; Gallagher, M. Engaging Latino fathers in children’s eating and other obesity-related behaviors: A review. Curr. Nutr. Rep. 2018, 7, 29–38. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
|
|
|
| Variable | Adolescent (N = 16) | Young Adults (N = 15) |
|---|---|---|
| Sex (N) | ||
| Male | 8 | 7 |
| Female | 8 | 8 |
| Age (years) | 14.6 ± 1.5 | 20.7 ± 1.1 |
| Mean BMI (kg/m2) | 37.2 ± 5.6 | 41.8 ± 9.0 |
| Living Status (%) | ||
| Two-parent household | 62.5 | 73.3 |
| Female-headed household | 18.8 | 6.7 |
| Separated parents | 12.5 | 6.7 |
| Blended Family | 6.3 | 13.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Soltero, E.G.; Navabi, N.; Castro, F.G.; Ayers, S.L.; Mendez, J.; Thompson, D.I.; Shaibi, G.Q. Perceptions of Family-Level Social Factors That Influence Health Behaviors in Latinx Adolescents and Young Adults at High Risk for Type 2 Diabetes. Children 2021, 8, 406. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050406
Soltero EG, Navabi N, Castro FG, Ayers SL, Mendez J, Thompson DI, Shaibi GQ. Perceptions of Family-Level Social Factors That Influence Health Behaviors in Latinx Adolescents and Young Adults at High Risk for Type 2 Diabetes. Children. 2021; 8(5):406. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050406
Chicago/Turabian StyleSoltero, Erica G., Neeku Navabi, Felipe G. Castro, Stephanie L. Ayers, Jenny Mendez, Deborah I. Thompson, and Gabriel Q. Shaibi. 2021. "Perceptions of Family-Level Social Factors That Influence Health Behaviors in Latinx Adolescents and Young Adults at High Risk for Type 2 Diabetes" Children 8, no. 5: 406. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050406