
A Retrospective Analysis of Feeding Practices and Complications in Patients with Critical Bronchiolitis on Non-Invasive Respiratory Support

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Setting
2.2. Study Design
2.3. Eligibility
2.4. Variables
2.5. Definitions
2.6. Statistical Analyses
3. Results
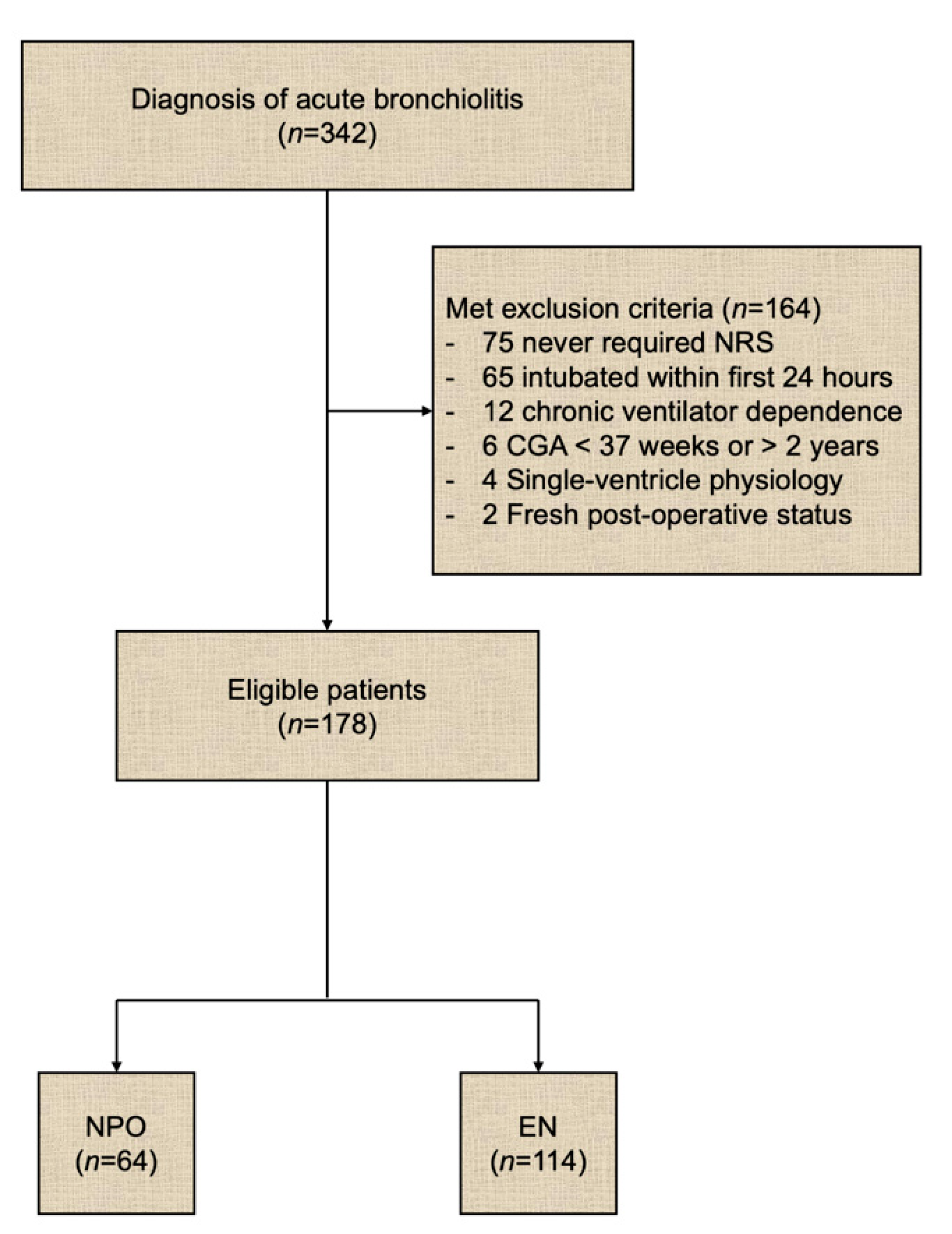
3.1. Eligibility
3.2. Patient Demographics
3.3. Clinical Characteristics
3.4. Enteral Nutrition Details
3.5. Physiometric Parameters and Enteral Nutrition
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. List of ICD-9 and ICD-10 Codes Associated with the Diagnoses Used to Select Patients for the Study
| Diagnosis | ICD-9 | ICD-10 |
|---|---|---|
| Acute bronchiolitis due to respiratory syncytial virus | 466.11 | J21.0 |
| Acute bronchiolitis due to human metapneumovirus | 466.19 | J21.1 |
| Acute bronchiolitis due to other specified organisms | 466.19 | J21.8 |
| Acute bronchiolitis, unspecified | 466.19 | J21.9 |
References
- Shay, D.K.; Holman, R.C.; Newman, R.D.; Liu, L.L.; Stout, J.W.; Anderson, L.J. Bronchiolitis-Associated Hospitalizations Among US Children, 1980-1996. JAMA 1999, 282, 1440–1446. [Google Scholar] [CrossRef] [Green Version]
- Yorita, K.L.; Holman, R.C.; Sejvar, J.J.; Steiner, C.A.; Schonberger, L.B. Infectious Disease Hospitalizations Among Infants in the United States. Pediatrics 2008, 121, 244–252. [Google Scholar] [CrossRef]
- Wright, M.; Mullett, C.J.; Piedimonte, G. Pharmacological management of acute bronchiolitis. Ther. Clin. Risk Manag. 2008, 4, 895–903. [Google Scholar]
- Bont, L.; Checchia, P.A.; Fauroux, B.; Figueras-Aloy, J.; Manzoni, P.; Paes, B.; Simões, E.A.F.; Carbonell-Estrany, X. Defining the Epidemiology and Burden of Severe Respiratory Syncytial Virus Infection Among Infants and Children in Western Countries. Infect. Dis. Ther. 2016, 5, 271–298. [Google Scholar] [CrossRef] [Green Version]
- Gupta, P.; Beam, B.W.; Rettiganti, M. Temporal Trends of Respiratory Syncytial Virus–Associated Hospital and ICU Admissions Across the United States. Pediatr. Crit. Care Med. 2016, 17, e343–e351. [Google Scholar] [CrossRef] [PubMed]
- Wang, E.E.; Law, B.J.; Stephens, D. Pediatric Investigators Collaborative Network on Infections in Canada (PICNIC) prospective study of risk factors and outcomes in patients hospitalized with respiratory syncytial viral lower respiratory tract infection. J. Pediatr. 1995, 126, 212–219. [Google Scholar] [CrossRef]
- Maamari, M.; Nino, G.; Bost, J.; Cheng, Y.; Sochet, A.; Sharron, M. Predicting Failure of Non-Invasive Ventilation With RAM Cannula in Bronchiolitis. J. Intensiv. Care Med. 2021, 885066620979642. [Google Scholar] [CrossRef]
- Javouhey, E.; Barats, A.; Richard, N.; Stamm, D.; Floret, D. Non-invasive ventilation as primary ventilatory support for infants with severe bronchiolitis. Intensiv. Care Med. 2008, 34, 1608–1614. [Google Scholar] [CrossRef]
- Lazner, M.R.; Basu, A.; Klonin, H. Non-invasive ventilation for severe bronchiolitis: Analysis and evidence. Pediatr. Pulmonol. 2012, 47, 909–916. [Google Scholar] [CrossRef] [PubMed]
- Meduri, G.U.; Turner, R.E.; Abou-Shala, N.; Wunderink, R.; Tolley, E. Noninvasive positive pressure ventilation via face mask. First-line intervention in patients with acute hypercapnic and hypoxemic respiratory failure. Chest 1996, 109, 179–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morris, J.V.; Ramnarayanm, P.; Parslow, R.C.; Fleming, S.J. Outcomes for Children Receiving Noninvasive Ventilation as the First-Line Mode of Mechanical Ventilation at Intensive Care Admission: A Propensity Score-Matched Cohort Study. Crit. Care Med. 2017, 45, 1045–1053. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, N.M.; Bechard, L.J.; Cahill, N.; Wang, M.; Day, A.; Duggan, C.P.; Heyland, D.K. Nutritional practices and their relationship to clinical outcomes in critically ill children—An international multicenter cohort study. Crit. Care Med. 2012, 40, 2204–2211. [Google Scholar] [CrossRef]
- Ng, G.Y.H.; Ong, C.; Wong, J.J.M.; Teoh, O.H.; Sultana, R.; Mok, Y.H.; Lee, J.H. Nutritional status, intake, and outcomes in critically ill children with bronchiolitis. Pediatr. Pulmonol. 2020, 55, 1199–1206. [Google Scholar] [CrossRef]
- Mehta, N.M.; Skillman, H.E.; Irving, S.Y.; Coss-Bu, J.A.; Vermilyea, S.; Farrington, E.A.; McKeever, L.; Hall, A.M.; Goday, P.S.; Braunschweig, C. Guidelines for the Provision and Assessment of Nutrition Support Therapy in the Pediatric Critically Ill Patient: Society of Critical Care Medicine and American Society for Parenteral and Enteral Nutrition. J. Parenter. Enter. Nutr. 2017, 41, 706–742. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canarie, M.F.; Barry, S.; Carroll, C.L.; Hassinger, A.; Kandil, S.; Li, S.; Pinto, M.; Valentine, S.L.; Faustino, E.V.S. Northeast Pediatric Critical Care Research Consortium. Risk Factors for Delayed Enteral Nutrition in Critically Ill Children. Pediatr. Crit. Care Med. 2015, 16, e283–e289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leroue, M.K.; Good, R.J.; Skillman, H.E.; Czaja, A.S. Enteral Nutrition Practices in Critically Ill Children Requiring Noninvasive Positive Pressure Ventilation. Pediatr. Crit. Care Med. 2017, 18, 1093–1098. [Google Scholar] [CrossRef]
- Casaer, M.P.; van den Berghe, G. Nutrition in the acute phase of critical illness. N. Engl. J. Med. 2014, 370, 2450–2451. [Google Scholar] [CrossRef]
- Hoffer, L.J.; Bistrian, B.R. Nutrition in critical illness: A current conundrum. F1000Research 2016, 5, 2531. [Google Scholar] [CrossRef] [Green Version]
- Singer, P.; Rattanachaiwong, S. To eat or to breathe? The answer is both! Nutritional management during noninvasive ventilation. Crit. Care 2018, 22, 1–3. [Google Scholar] [CrossRef] [Green Version]
- Tume, L.N.; Eveleens, R.D.; Mayordomo-Colunga, J.; López, J.; Verbruggen, S.C.A.T.; Fricaudet, M.; Smith, C.; Cusco, M.G.G.; Latten, L.; Valla, F.V. Enteral Feeding of Children on Noninvasive Respiratory Support: A Four-Center European Study. Pediatr. Crit. Care Med. 2021, 22, e192–e202. [Google Scholar] [CrossRef]
- Buck, M.L. Dexmedetomidine Use in Pediatric Intensive Care and Procedural Sedation. J. Pediatr. Pharmacol. Ther. 2010, 15, 17–29. [Google Scholar] [CrossRef] [PubMed]
- Carroll, C.L.; Krieger, D.; Campbell, M.; Fisher, D.G.; Comeau, L.L.; Zucker, A.R. Use of dexmedetomidine for sedation of children hospitalized in the intensive care unit. J. Hosp. Med. 2008, 3, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Yehya, N.; Harhay, M.O.; Curley, M.A.Q.; Schoenfeld, D.A.; Reeder, R.W. Reappraisal of Ventilator-Free Days in Critical Care Research. Am. J. Respir. Crit. Care Med. 2019, 200, 828–836. [Google Scholar] [CrossRef]
- Tume, L.N.; Valla, F.V.; Joosten, K.; Chaparro, C.J.; Latten, L.; Marino, L.V.; MacLeod, I.; Moullet, C.; Pathan, N.; Rooze, S.; et al. Nutritional support for children during critical illness: European Society of Pediatric and Neonatal Intensive Care (ESPNIC) metabolism, endocrine and nutrition section position statement and clinical recommendations. Intensiv. Care Med. 2020, 46, 411–425. [Google Scholar] [CrossRef] [Green Version]
- Terzi, N.; Darmon, M.; Reignier, J.; Ruckly, S.; Garrouste-Orgeas, M.; Lautrette, A.; Azoulay, E.; Mourvillier, B.; Argaud, L.; Papazian, L.; et al. Initial nutritional management during noninvasive ventilation and outcomes: A retrospective cohort study. Crit. Care 2017, 21, 293. [Google Scholar] [CrossRef] [Green Version]
- Mikhailov, T.A.; Kuhn, E.M.; Manzi, J.; Christensen, M.; Collins, M.; Brown, A.-M.; Dechert, R.; Scanlon, M.; Wakeham, M.K.; Goday, P.S. Early Enteral Nutrition Is Associated With Lower Mortality in Critically Ill Children. J. Parenter. Enter. Nutr. 2014, 38, 459–466. [Google Scholar] [CrossRef]
- Kogo, M.; Nagata, K.; Morimoto, T.; Ito, J.; Sato, Y.; Teraoka, S.; Fujimoto, D.; Nakagawa, A.; Otsuka, K.; Tomii, K. Enteral Nutrition Is a Risk Factor for Airway Complications in Subjects Undergoing Noninvasive Ventilation for Acute Respiratory Failure. Respir. Care 2016, 62, 459–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Srinivasan, V.; Hasbani, N.R.; Mehta, N.M.; Irving, S.Y.; Kandil, S.B.; Allen, H.C.; Typpo, K.V.; Cvijanovich, N.Z.; Faustino, E.V.S.; Wypij, D.; et al. Early Enteral Nutrition Is Associated With Improved Clinical Outcomes in Critically Ill Children: A Secondary Analysis of Nutrition Support in the Heart and Lung Failure-Pediatric Insulin Titration Trial. Pediatr. Crit. Care Med. 2020, 21, 213–221. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| NPO (64) | EN (114) | p | |
|---|---|---|---|
| Sex, n (%) | |||
| Male | 39 (61%) | 70 (61%) | 1.0 |
| Weight (kg), median (IQR) | 8.4 (5.4–10.5) | 5.7 (4.7–7.4) | <0.001 |
| Age (months), median (IQR) | 10 (3–16) | 3 (2–6) | <0.001 |
| Age, n (%) | |||
| ≤1 month | 7 (11) | 13 (11) | <0.001 |
| 2–12 months | 31 (48) | 94 (82) | |
| 13–24 months | 26 (41) | 7 (6) | |
| Maturity, n (%) | |||
| Full-term at birth | 41 (64) | 68 (60) | 0.56 |
| Pre-term at birth | 23 (36) | 46 (40) | |
| Late (33 to <37 weeks) | 15 (23) | 33 (29) | 0.79 |
| Very (28 to <32 weeks) | 5 (8) | 7 (6) | |
| Extreme (<28 weeks) | 3 (5) | 6 (5) | |
| Genetic abnormalities, n (%) | 12 (19) | 12 (11) | 0.12 |
| Neurology abnormalities, n (%) | 7 (11) | 9 (8) | 0.50 |
| PRISM-III ROM, % (IQR) | 0.5 (0.5–0.8) | 0.5 (0.3–0.6) | 0.57 |
| Mortality, n (%) | 0 (0) | 0 (0) | - |
| NPO (64) | EN (114) | p | |
|---|---|---|---|
| NRS duration (days), median (IQR) | 1 (0.8–2) | 3 (2–4) | <0.001 |
| Type of NRS, n (%) | |||
| RAM | 52 (95) | 108 (99) | 0.34 |
| CPAP | 0 (0) | 1 (1) | |
| BiPAP | 3 (5) | 2 (2) | |
| Intubation #, n (%) | 9 (14) | 5 (4) | 0.016 |
| Pathogen f (#), median (IQR) | 1 (1–2) | 1 (1–1) | 0.21 |
| Pathogen positive, n (%) | 57 (89) | 105 (92) | 0.5 |
| Single | 41 (72) | 81 (77) | 0.53 |
| Multiple | 16 (28) | 25 (24) | |
| Virus only | 53 (93) | 99 (94) | 0.74 |
| Virus + Bacteria | 4 (7) | 6 (6) | |
| PICU LOS (days), median (IQR) | 2 (1–3) | 3 (2–5) | <0.001 |
| EN (109) | |
|---|---|
| Route, n (%) | |
| PO | 11 (10) |
| NG | 69 (63) |
| NJ | 14 (13) |
| GT/JT | 15 (14) |
| Mode, n (%) | |
| Bolus | 24 (22) |
| Continuous | 85 (78) |
| Time to initiation (h) *, median (IQR) | 19 (11–37) |
| n (%) | |
| ≤48 h | 98 (90) |
| >48 h | 11 (10) |
| Reached full EN (h) *, median (IQR) | 40 (24–58) |
| n (%) | |
| ≤7 days | 103 (94) |
| >7 days | 6 (6) |
| Complications #, n (%) | |
| Yes | 9 (8) |
| No | 100 (92) |
| Evidence of aspiration, n (%) | |
| Yes | 1 (1) |
| No | 108 (99) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lenihan, A.; Ramos, V.; Nemec, N.; Lukowski, J.; Lee, J.; Kendall, K.M.; Mahapatra, S. A Retrospective Analysis of Feeding Practices and Complications in Patients with Critical Bronchiolitis on Non-Invasive Respiratory Support. Children 2021, 8, 410. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050410
Lenihan A, Ramos V, Nemec N, Lukowski J, Lee J, Kendall KM, Mahapatra S. A Retrospective Analysis of Feeding Practices and Complications in Patients with Critical Bronchiolitis on Non-Invasive Respiratory Support. Children. 2021; 8(5):410. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050410
Chicago/Turabian StyleLenihan, Ariann, Vannessa Ramos, Nichole Nemec, Joseph Lukowski, Junghyae Lee, K M. Kendall, and Sidharth Mahapatra. 2021. "A Retrospective Analysis of Feeding Practices and Complications in Patients with Critical Bronchiolitis on Non-Invasive Respiratory Support" Children 8, no. 5: 410. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050410