
Poor Glycemic Control Can Increase the Plasma Kidney Injury Molecule-1 Concentration in Normoalbuminuric Children and Adolescents with Diabetes Mellitus

 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Participants
2.2. Definition of Diagnosing DM
2.3. Clinical and Laboratory Data
2.4. Measurements of Renal Injury Markers
2.5. Statistical Analysis
3. Results
3.1. Baseline Characteristics and Biomarker Measurements
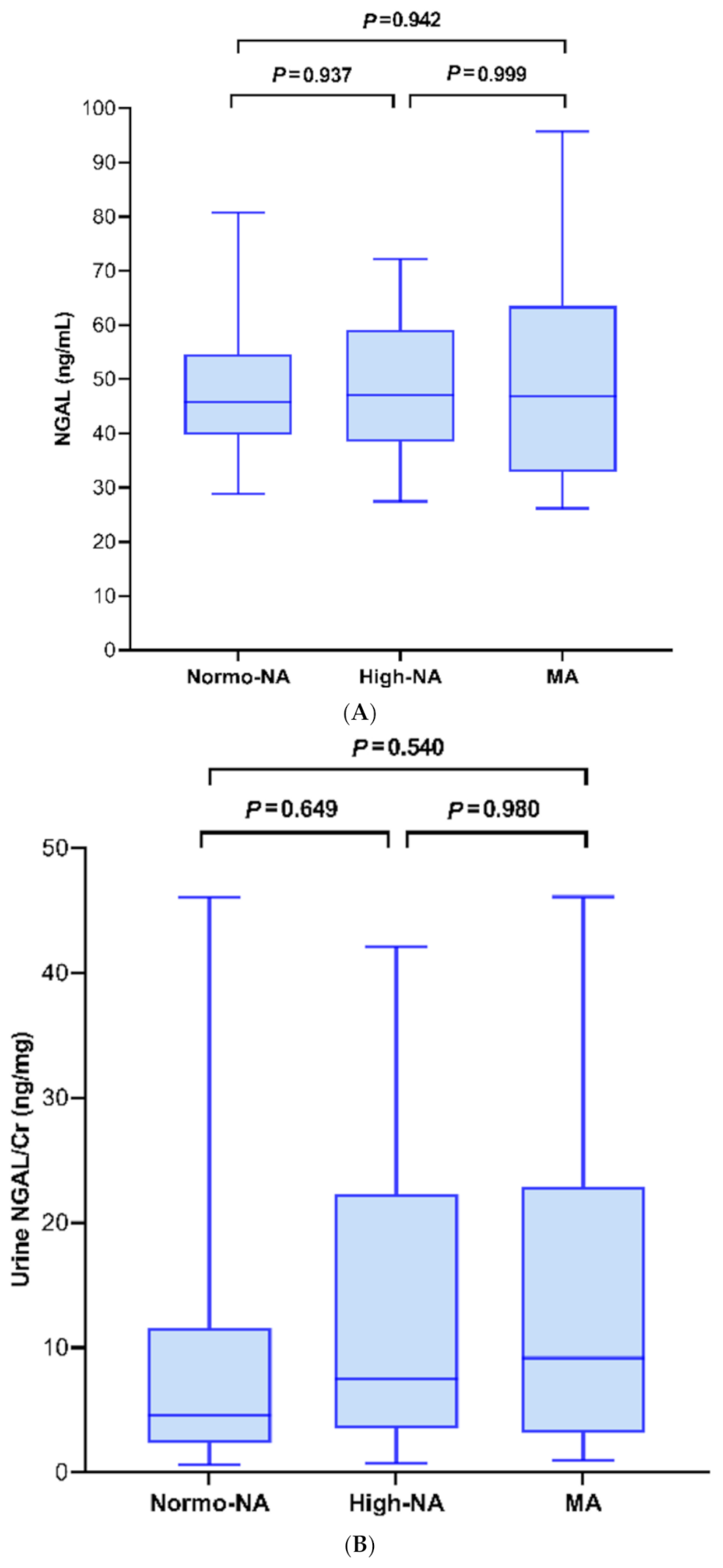
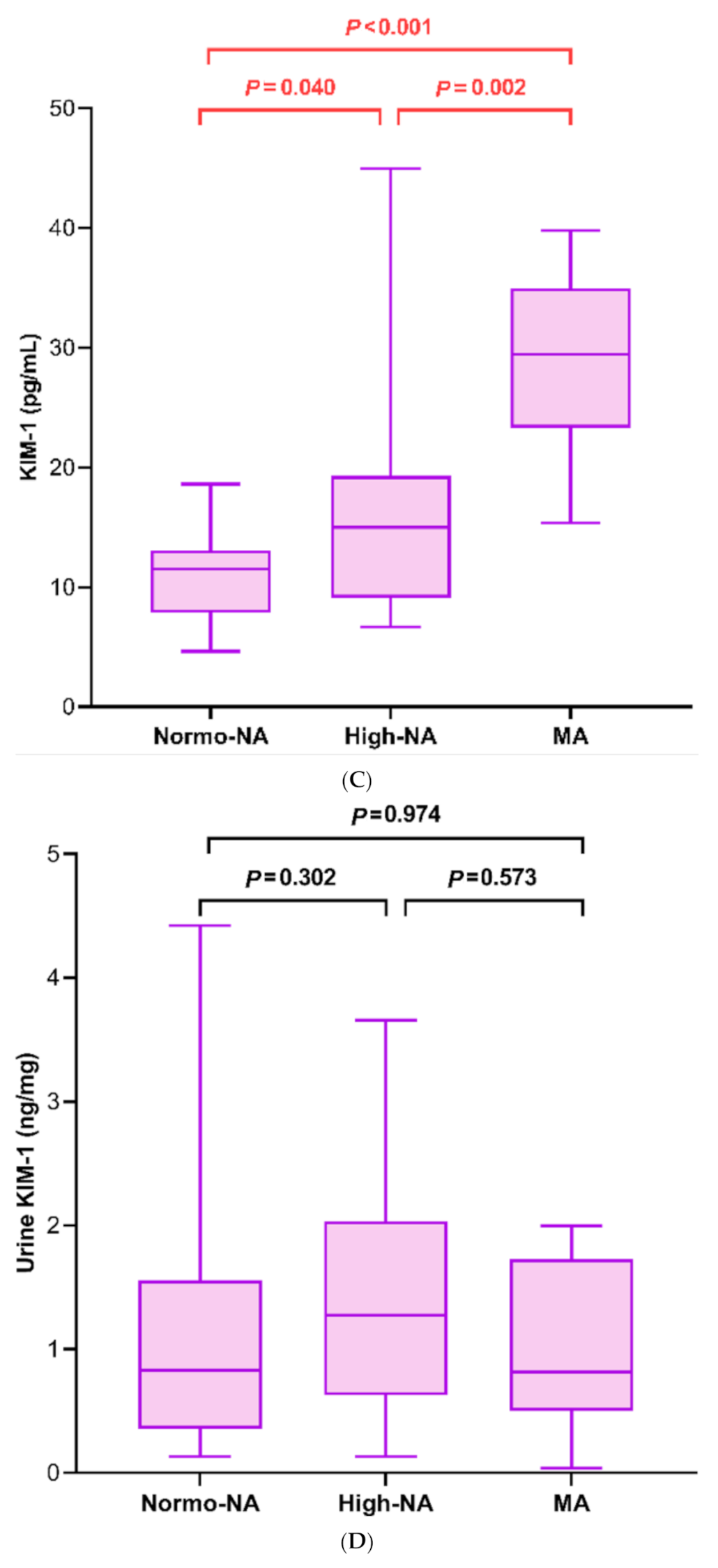
3.2. Renal Injury Markers in Association with the MA Status
3.3. Association of Plasma KIM-1 with the Clinical and Laboratory Data
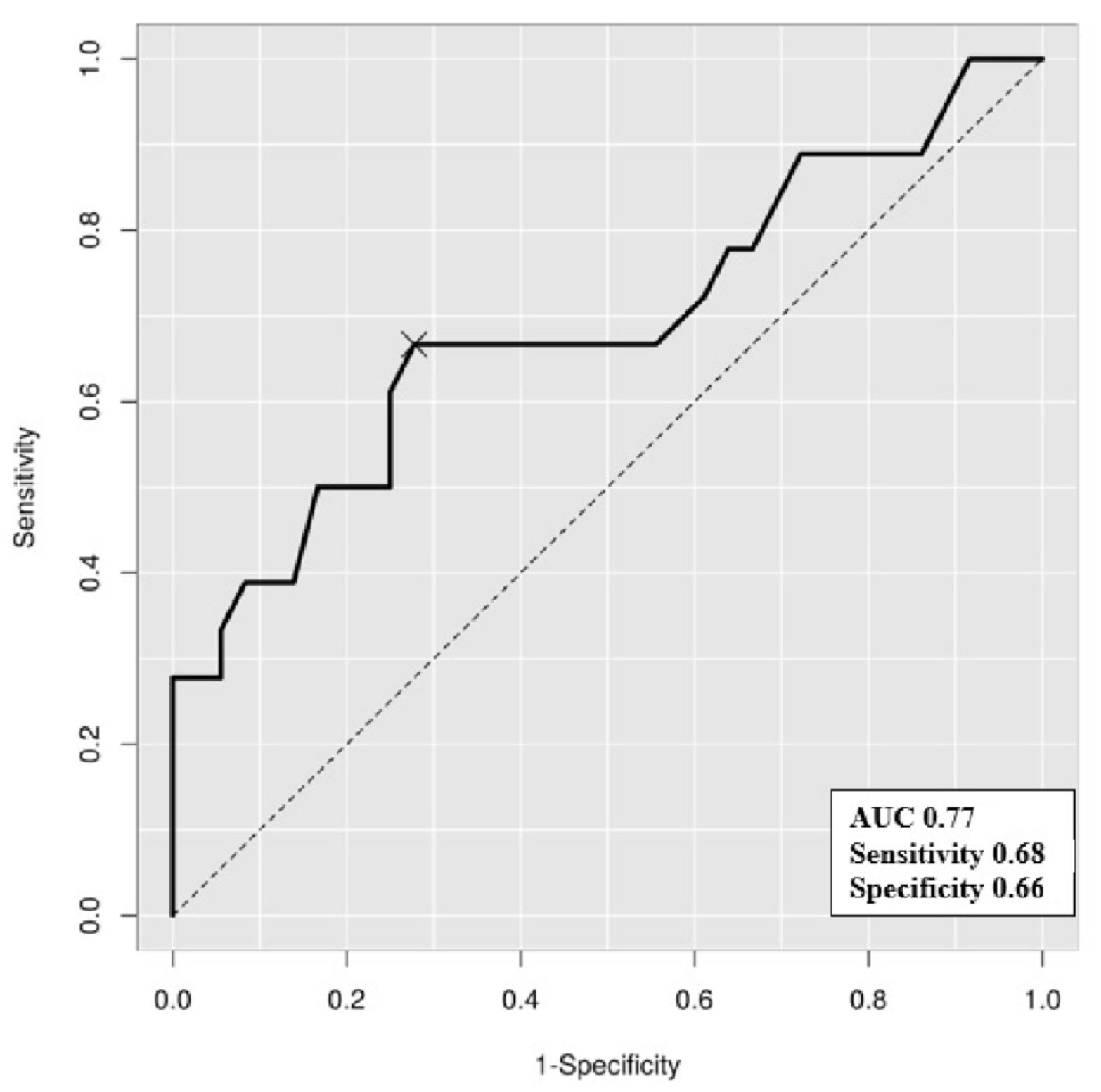
3.4. The HbA1c Cutoff Predicting a High Plasma KIM-1 Level
4. Discussions
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bogdanovic, R. Diabetic nephropathy in children and adolescents. Pediatr. Nephrol. 2008, 23, 507–525. [Google Scholar] [CrossRef]
- Klimontov, V.V.; Korbut, A.I. Albuminuric and non-albuminuric patterns of chronic kidney disease in type 2 diabetes. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 474–479. [Google Scholar] [CrossRef]
- Raja, P.; Maxwell, A.P.; Brazil, D.P. The Potential of Albuminuria as a Biomarker of Diabetic Complications. Cardiovasc. Drugs Ther. 2021, 35, 455–466. [Google Scholar] [CrossRef] [PubMed]
- Beisswenger, P.J. Glycation and biomarkers of vascular complications of diabetes. Amino Acids 2010, 42, 1171–1183. [Google Scholar] [CrossRef] [PubMed]
- Idowu, A.A.; Ajose, A.O.; Adedeji, A.T.; Adegoke, A.O.; Jimoh, K.A. Microalbuminuria, Other Markers of Nephropathy and Biochemical Derangementsin Type 2 Diabetes Mellitus: Relationships and Determinants. Ghana Med. J. 2017, 51, 56–63. [Google Scholar]
- Hayashi, Y. Detection of Lower Albuminuria Levels and Early Development of Diabetic Kidney Disease Using an Artificial Intelligence-Based Rule Extraction Approach. Diagnostics 2019, 9, 133. [Google Scholar] [CrossRef] [Green Version]
- Nowak, N.; Skupien, J.; Niewczas, M.A.; Yamanouchi, M.; Major, M.; Croall, S.; Smiles, A.; Warram, J.H.; Bonventre, J.V.; Krolewski, A.S. Increased plasma kidney injury molecule-1 suggests early progressive renal decline in non-proteinuric patients with type 1 diabetes. Kidney Int. 2016, 89, 459–467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wahab, M.A.K.A.; Saad, M.M.; Baraka, K.A.G. Microalbuminuria is a late event in patients with hypertension: Do we need a lower threshold? J. Saudi Heart Assoc. 2017, 29, 30–36. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.-K.; Han, K.-D.; Lee, J.-H.; Sohn, S.-Y.; Hong, O.-K.; Jeong, J.-S.; Kim, M.-K.; Baek, K.-H.; Song, K.-H.; Kwon, H.-S. Normal-to-mildly increased albuminuria predicts the risk for diabetic retinopathy in patients with type 2 diabetes. Sci. Rep. 2017, 7, 11757. [Google Scholar] [CrossRef] [Green Version]
- Cao, Z.; Cooper, M.E. Pathogenesis of diabetic nephropathy. J. Diabetes Investig. 2011, 2, 243–247. [Google Scholar] [CrossRef] [PubMed]
- Satirapoj, B. Tubulointerstitial Biomarkers for Diabetic Nephropathy. J. Diabetes Res. 2018, 2018, 1–6. [Google Scholar] [CrossRef]
- Nauta, F.L.; Scheven, L.; Meijer, E.; Van Oeveren, W.; De Jong, P.E.; Bakker, S.J.; Gansevoort, R.T. Glomerular and Tubular Damage Markers in Individuals with Progressive Albuminuria. Clin. J. Am. Soc. Nephrol. 2013, 8, 1106–1114. [Google Scholar] [CrossRef] [Green Version]
- Żyłka, A.; Dumnicka, P.; Kuśnierz-Cabala, B.; Gala-Błądzińska, A.; Ceranowicz, P.; Kucharz, J.; Ząbek-Adamska, A.; Maziarz, B.; Drozdz, R.; Kuźniewski, M. Markers of Glomerular and Tubular Damage in the Early Stage of Kidney Disease in Type 2 Diabetic Patients. Mediat. Inflamm. 2018, 2018, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Gluhovschi, C.; Gluhovschi, G.; Petrica, L.; Timar, R.; Velciov, S.; Ionita, I.; Kaycsa, A.; Timar, B. Urinary Biomarkers in the Assessment of Early Diabetic Nephropathy. J. Diabetes Res. 2016, 2016, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Lee, S.-Y.; Choi, M.E. Urinary biomarkers for early diabetic nephropathy: Beyond albuminuria. Pediatr. Nephrol. 2015, 30, 1063–1075. [Google Scholar] [CrossRef] [Green Version]
- Bolignano, D.; Lacquaniti, A.; Coppolino, G.; Donato, V.; Campo, S.; Fazio, M.R.; Nicocia, G.; Buemi, M. Neutrophil Gelatinase-Associated Lipocalin (NGAL) and Progression of Chronic Kidney Disease. Clin. J. Am. Soc. Nephrol. 2009, 4, 337–344. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Li, Y.; Liu, Y.; Zang, C.; Wu, M.; Xu, Z. Diagnostic value of neutrophil gelatinase-associated lipocalin in diabetic nephropathy: A meta-analysis. Ren. Fail. 2019, 41, 489–496. [Google Scholar] [CrossRef]
- Van Donge, T.; Welzel, T.; Atkinson, A.; Anker, J.D.; Pfister, M. Age-Dependent Changes of Kidney Injury Biomarkers in Pediatrics. J. Clin. Pharmacol. 2019, 59, S21–S32. [Google Scholar] [CrossRef] [Green Version]
- Van Timmeren, M.M.; Bakker, S.J.L.; Vaidya, V.S.; Bailly, V.; Schuurs, T.A.; Damman, J.; Stegeman, C.A.; Bonventre, J.V.; Van Goor, H. Tubular kidney injury molecule-1 in protein-overload nephropathy. Am. J. Physiol. Physiol. 2006, 291, F456–F464. [Google Scholar] [CrossRef]
- Kapoula, G.V.; Kontou, P.I.; Bagos, P.G. Diagnostic Performance of Biomarkers Urinary KIM-1 and YKL-40 for Early Diabetic Nephropathy, in Patients with Type 2 Diabetes: A Systematic Review and Meta-Analysis. Diagnostics 2020, 10, 909. [Google Scholar] [CrossRef]
- Mayer-Davis, E.J.; Kahkoska, A.R.; Jefferies, C.; Dabelea, D.; Balde, N.; Gong, C.X.; Aschner, P.; Craig, M.E. ISPAD Clinical Practice Consensus Guidelines 2018: Definition, epidemiology, and classification of diabetes in children and adolescents. Pediatr. Diabetes 2018, 19, 7–19. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Yun, S.; Hwang, S.-S.; Shim, J.O.; Chae, H.W.; Lee, Y.J.; Lee, J.H.; Kim, S.C.; Lim, D.; Yang, S.W.; et al. The 2017 Korean National Growth Charts for children and adolescents: Development, improvement, and prospects. Korean J. Pediatr. 2018, 61, 135–149. [Google Scholar] [CrossRef]
- Marcovecchio, M.L.; Chiesa, S.T.; Armitage, J.; Daneman, D.; Donaghue, K.C.; Jones, T.W.; Mahmud, F.H.; Marshall, S.M.; Neil, H.A.W.; Dalton, R.N.; et al. Renal and Cardiovascular Risk According to Tertiles of Urinary Albumin-to-Creatinine Ratio: The Adolescent Type 1 Diabetes Cardio-Renal Intervention Trial (AdDIT). Diabetes Care 2018, 41, 1963–1969. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef] [Green Version]
- de Carvalho, J.A.M.; Tatsch, E.; Hausen, B.S.; Bollick, Y.S.; Moretto, M.B.; Duarte, T.; Duarte, M.M.; Londero, S.W.; Premaor, M.O.; Comim, F.V.; et al. Urinary kidney injury molecule-1 and neutrophil gelatinase-associated lipocalin as indicators of tubular damage in normoalbuminuric patients with type 2 diabetes. Clin. Biochem. 2016, 49, 232–236. [Google Scholar] [CrossRef]
- Rivera, P.; Miranda, C.; Roldán, N.; Guerrero, A.; Olave, J.; Cárdenas, P.; Nguyen, Q.M.; Kassan, M.; Gonzalez, A.A. Augmented transcripts of kidney injury markers and renin angiotensin system in urine samples of overweight young adults. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Sabbisetti, V.S.; Waikar, S.S.; Antoine, D.J.; Smiles, A.; Wang, C.; Ravisankar, A.; Ito, K.; Sharma, S.; Ramadesikan, S.; Lee, M.; et al. Blood Kidney Injury Molecule-1 Is a Biomarker of Acute and Chronic Kidney Injury and Predicts Progression to ESRD in Type I Diabetes. J. Am. Soc. Nephrol. 2014, 25, 2177–2186. [Google Scholar] [CrossRef]
- Greenberg, J.H.; Abraham, A.G.; Xu, Y.; Schelling, J.R.; Feldman, H.I.; Sabbisetti, V.S.; Gonzalez, M.C.; Coca, S.; Schrauben, S.J.; Waikar, S.S.; et al. Plasma Biomarkers of Tubular Injury and Inflammation Are Associated with CKD Progression in Children. J. Am. Soc. Nephrol. 2020, 31, 1067–1077. [Google Scholar] [CrossRef]
- Colombo, M.; on behalf of the Scottish Diabetes Research Network (SDRN) Type 1 Bioresource Investigators; McGurnaghan, S.J.; Blackbourn, L.; Dalton, R.N.; Dunger, D.; Bell, S.; Petrie, J.R.; Green, F.; MacRury, S.; McKnight, J.A.; et al. Comparison of serum and urinary biomarker panels with albumin/creatinine ratio in the prediction of renal function decline in type 1 diabetes. Diabetologia 2020, 63, 788–798. [Google Scholar] [CrossRef] [Green Version]
- Ahmad, T.; Ulhaq, I.; Mawani, M.; Islam, N. Microalbuminuria in Type-2 Diabetes Mellitus; the tip of iceberg of diabetic complications. Pak. J. Med. Sci. 2017, 33, 519–523. [Google Scholar] [CrossRef]
- Harindhanavudhi, T.; Parks, A.; Mauer, M.; Caramori, M.L. Podocyte structural parameters do not predict progression to diabetic nephropathy in normoalbuminuric type 1 diabetic patients. Am. J. Nephrol. 2015, 41, 277–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeitler, P.; Arslanian, S.; Fu, J.; Pinhas-Hamiel, O.; Reinehr, T.; Tandon, N.; Urakami, T.; Wong, J.; Maahs, D.M. ISPAD Clinical Practice Consensus Guidelines 2018: Type 2 diabetes mellitus in youth. Pediatr. Diabetes 2018, 19, 28–46. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Total (n = 98) | |||
|---|---|---|---|
| Control (n = 44) | Diabetic Children (n = 54) | p | |
| Gender, male/female, n | 27/17 | 28/26 | 0.415 |
| Age (years) | 9.92 (8.67–11.58) | 15.83 (13.46–17.69) | <0.001 |
| BMI SDS | 2.22 (0.78–2.92) | 1.64 (−0.65–3.08) | 0.389 |
| Hemoglobin (g/dL) | 13.6 (13.1–14.2) | 14.1 (13.28–15.60) | 0.059 |
| CRP (mg/dL) | 0.07 (0.03–0.14) | 0.30 (0.08–1.46) | <0.001 |
| Glucose (mg/dL) | 94.00 (90.75–97.25) | 118.00 (104.25–185.25) | <0.001 |
| Cr (mg/dL) | 0.47 (0.43–0.55) | 0.56 (0.48–0.70) | <0.001 |
| eGFR (mL/min/1.73 m2) | 121.18 (107.21–129.78) | 118.15 (99.79–133.13) | 0.337 |
| Protein (mg/dL) | 7.40 (7.10–7.70) | 7.30 (7.10–7.60) | 0.435 |
| Albumin (g/dL) | 4.70 (4.60–4.90) | 4.70 (4.50–4.90) | 0.311 |
| AST (U/L) | 22.50 (18.75–28.25) | 18.50 (13.75–34.75) | 0.080 |
| ALT (U/L) | 15 (11.75–22.50) | 14.00 (10.00–56.25) | 0.689 |
| TC (mg/dL) | 173.50 (155.75–203.75) | 179.00 (156.75–202.50) | 0.898 |
| TG (mg/dL) | 97.00 (58.75–133.50) | 110.50 (58.00–171.75) | 0.530 |
| HDL-C (mg/dL) | 50.00 (44.00–60.25) | 52.00 (44.00–633.25) | 0.825 |
| LDL-C (mg/dL) | 106.00 (90.75–127.00) | 106.10 (78.75–124.00) | 0.328 |
| HbA1c (%) | 5.40 (5.20–5.60) | 8.20 (6.70–9.70) | <0.001 |
| C-peptide (ng/mL) | 2.45 (1.83–3.42) | 0.78 (0.11–2.88) | <0.001 |
| HOMA-IR | 3.87 (2.26–5.72) | 2.02 (0.76–6.91) | 0.070 |
| HOMA-β | 200.35 (136.19–292.07) | 40.49 (14.00–111.01) | <0.001 |
| Uric acid (mg/dL) | 5.25 (4.30–6.85) | 4.85 (4.08–5.60) | 0.011 |
| UPCR (mg/g Cr) | 0.09 (0.08–0.12) | 0.09 (0.06–0.13) | 0.749 |
| UACR (mg/g Cr) | 4.72 (3.49–8.81) | 11.57 (6.75–22.68) | <0.001 |
| NGAL (ng/mL) | 46.42 (37.63–53.71) | 45.96 (38.60–55.95) | 0.828 |
| Urine NGAL/Cr (ng/mg Cr) | 2.78 (1.23–5.83) | 5.91 (2.83–14.70) | <0.001 |
| KIM-1 (pg/mL) | 11.25 (9.06–14.62) | 16.89 (9.10–29.27) | 0.007 |
| Urine KIM-1/Cr (ng/mg Cr) | 0.61 (0.41–0.81) | 1.01 (0.49–1.64) | 0.005 |
| Total (n = 98) | |||
|---|---|---|---|
| T1DM (n = 31) | T2DM (n = 23) | p | |
| Gender, male/female, n | 18/13 | 10/13 | 0.409 |
| Age (years) | 14.67 (10.08–16.42) | 17.58 (15.75–18.25) | <0.001 |
| Duration of known DM (years) | 2.00 (0.75–4.50) | 1.33 (1.17–3.42) | 0.353 |
| BMI SDS | 0.15 (−1.16–1.59) | 3.19 (1.99–4.66) | <0.001 |
| Hemoglobin (g/dL) | 13.70 (13.10–15.50) | 14.30 (13.60–15.60) | 0.244 |
| CRP (mg/dL) | 0.30 (0.03–0.73) | 0.87 (0.12–2.60) | 0.062 |
| Glucose (mg/dL) | 113.00 (101.00–161.00) | 122.00 (112.00–219.00) | 0.124 |
| Cr (mg/dL) | 0.53 (0.45–0.70) | 0.60 (0.54–0.72) | 0.050 |
| eGFR (mL/min/1.73 m2) | 123.90 (102.06–138.79) | 116.60 (94.36–131.70) | 0.340 |
| Protein (mg/dL) | 7.20 (7.00–7.40) | 7.50 (7.30–7.80) | <0.001 |
| Albumin (g/dL) | 4.60 (4.50–4.90) | 4.70 (4.50–4.90) | 0.487 |
| AST (U/L) | 17.00 (14.00–21.00) | 34.00 (13.00–59.00) | 0.038 |
| ALT (U/L) | 12.00 (9.00–15.00) | 57.00 (12.00–103.00) | <0.001 |
| TC (mg/dL) | 170.00 (149.00–204.00) | 181.00 (159.00–202.00) | 0.903 |
| TG (mg/dL) | 79.00 (50.00–156.00) | 127.00 (99.00–230.00) | 0.013 |
| HDL-C (mg/dL) | 59.00 (52.00–71.00) | 44.00 (39.00–49.00) | <0.001 |
| LDL-C (mg/dL) | 90.40 (74.00–124.00) | 116.60 (90.00–123.20) | 0.128 |
| HbA1c (%) | 8.50 (6.80–9.60) | 7.90 (6.50–10.30) | 0.759 |
| C-peptide (ng/mL) | 0.13 (0.02–0.66) | 3.26 (1.96–4.61) | <0.001 |
| HOMA-IR | 0.95 (0.38–1.82) | 6.59 (4.27–12.84) | <0.001 |
| HOMA-β | 22.76 (9.53–42.45) | 107.92 (60–04–209.39) | <0.001 |
| Uric acid (mg/dL) | 4.40 (3.80–5.30) | 5.40 (4.70–6.40) | 0.002 |
| UPCR (mg/g Cr) | 0.10 (0.08–0.16) | 0.08 (0.06–0.11) | 0.098 |
| UACR (mg/g Cr) | 9.43 (6.51–20.99) | 14.98 (6.99–25.32) | 0.535 |
| NGAL (ng/mL) | 41.77 (37.05–49.87) | 51.11 (45.76–62.71) | 0.051 |
| Urine NGAL/Cr (ng/mg Cr) | 4.68 (3.16–23.72) | 6.61 (2.05–13.67) | 0.588 |
| KIM-1 (pg/mL) | 14.84 (8.00–20.67) | 22.64 (12.36–33.65) | 0.051 |
| Urine KIM-1/Cr (ng/mg Cr) | 1.00 (0.55–1.68) | 0.97 (0.39–1.60) | 0.601 |
| KIM-1 | ||
|---|---|---|
| Spearman’s ρ | P | |
| Age at DM diagnosis | 0.356 | 0.008 |
| Duration of known DM | −0.152 | 0.272 |
| Age | 0.163 | 0.238 |
| BMI SDS | 0.643 | <0.001 |
| Hemoglobin | 0.140 | 0.314 |
| CRP | 0.243 | 0.077 |
| Glucose | 0.380 | 0.005 |
| Cr | −0.078 | 0.577 |
| eGFR | 0.141 | 0.309 |
| Protein | 0.324 | 0.017 |
| Albumin | 0.003 | 0.980 |
| AST | 0.431 | 0.001 |
| ALT | 0.542 | <0.001 |
| TC | 0.466 | <0.001 |
| TG | 0.639 | 0.079 |
| HDL-C | −0.393 | 0.003 |
| LDL-C | 0.360 | 0.007 |
| HbA1c | 0.368 | 0.006 |
| C-peptide | 0.293 | 0.032 |
| HOMA-IR | 0.377 | 0.005 |
| HOMA-β | 0.122 | 0.378 |
| Uric acid | 0.360 | 0.008 |
| UPCR | 0.316 | 0.020 |
| UACR | 0.398 | 0.003 |
| Risk Factors | Univariate | Multivariate | ||||
|---|---|---|---|---|---|---|
| OR (95% CI) | SE | P | OR (95% CI) | SE | p | |
| DM type | 7.89 (−2.77–18.6) | 5.31 | 0.143 | |||
| Age at DM diagnosis | 1.98 (0.47–3.49) | 0.75 | 0.011 | 1.16 (–0.74–3.06) | 0.94 | 0.226 |
| DM duration | −0.93 (−2.98–1.12) | 1.02 | 0.367 | |||
| BMI SDS | 4.63 (2.51–6.75) | 1.06 | <0.001 | 1.72 (–1.62–5.06) | 1.66 | 0.305 |
| Hb | 1.21 (−2.30–4.73) | 1.75 | 0.492 | |||
| CRP | 0.25 (−1.13–1.63) | 0.69 | 0.721 | |||
| Glucose | 0.09 (<0.01–0.17) | 0.04 | 0.039 | −0.03 (−0.13–0.06) | 0.05 | 0.460 |
| Cr | 18.6 (−14.12–51.30) | 16.30 | 0.259 | |||
| eGFR | −0.07 (−0.30–0.16) | 0.11 | 0.542 | |||
| Protein | 7.02 (−3.17–17.20) | 5.08 | 0.173 | |||
| Albumin | −2.33 (−16.60–12.00) | 7.13 | 0.745 | |||
| AST | 0.45 (0.24–0.67) | 0.11 | <0.001 | 0.25 (−0.37–0.87) | 0.31 | 0.415 |
| ALT | 0.24 (0.14–0.35) | 0.05 | <0.001 | 0.02 (−0.33–0.37) | 0.17 | 0.906 |
| TC | 0.19 (0.02–0.35) | 0.08 | 0.090 | |||
| TG | 0.12 (0.07–0.17) | 0.02 | 0.061 | |||
| HDL-C | −0.40 (−0.77–0.03) | 0.19 | 0.035 | 0.08 (−0.34–0.51) | 0.21 | 0.700 |
| LDL-C | 0.16 (−0.03–0.34) | 0.09 | 0.102 | |||
| HbA1c | 2.99 (0.60–5.38) | 1.19 | 0.015 | 2.96 (0.35–5.56) | 1.29 | 0.027 |
| C-peptide | 2.73 (−0.33–5.80) | 1.53 | 0.079 | |||
| HOMA-IR | 0.37 (−0.11–0.85) | 0.24 | 0.127 | |||
| HOMA-β | −0.01 (−0.06–0.05) | 0.03 | 0.813 | |||
| Uric acid | 5.21 (0.86–9.56) | 2.17 | 0.020 | 1.38 (−4.45–7.22) | 2.89 | 0.636 |
| UPCR | 5.16 (−25.40–35.80) | 15.25 | 0.736 | |||
| UACR | 0.03 (−0.05–0.09) | 0.04 | 0.461 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ahn, M.B.; Cho, K.S.; Kim, S.K.; Kim, S.H.; Cho, W.K.; Jung, M.H.; Suh, J.-S.; Suh, B.-K. Poor Glycemic Control Can Increase the Plasma Kidney Injury Molecule-1 Concentration in Normoalbuminuric Children and Adolescents with Diabetes Mellitus. Children 2021, 8, 417. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050417
Ahn MB, Cho KS, Kim SK, Kim SH, Cho WK, Jung MH, Suh J-S, Suh B-K. Poor Glycemic Control Can Increase the Plasma Kidney Injury Molecule-1 Concentration in Normoalbuminuric Children and Adolescents with Diabetes Mellitus. Children. 2021; 8(5):417. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050417
Chicago/Turabian StyleAhn, Moon Bae, Kyoung Soon Cho, Seul Ki Kim, Shin Hee Kim, Won Kyoung Cho, Min Ho Jung, Jin-Soon Suh, and Byung-Kyu Suh. 2021. "Poor Glycemic Control Can Increase the Plasma Kidney Injury Molecule-1 Concentration in Normoalbuminuric Children and Adolescents with Diabetes Mellitus" Children 8, no. 5: 417. https://0-doi-org.brum.beds.ac.uk/10.3390/children8050417