
Oral Diseases and Quality of Life between Obese and Normal Weight Adolescents: A Two-Year Observational Study

 , , , and
, , , and
Abstract
:
1. Introduction
2. Materials and Methods
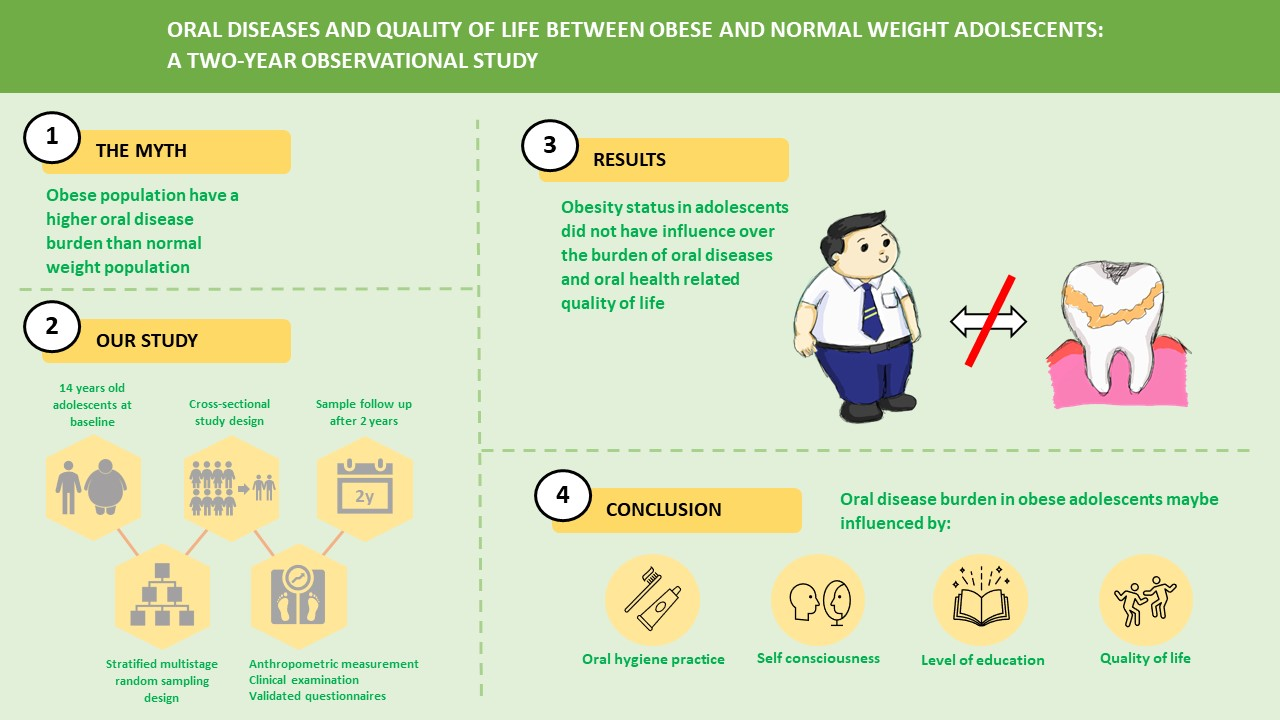
2.1. Study Design and Study Population
2.2. Ethics, Consents, and Permission
2.3. Anthropometric Measurement
2.4. Clinical Examinations
2.4.1. Caries Experiences
2.4.2. Periodontal Assessments
2.4.3. Training and Calibration
2.5. Questionnaires
2.6. Statistical Analysis
3. Results
3.1. Sociodemographic
3.2. Oral Health Practices
3.3. Caries and Periodontal Health
3.4. Oral Health Related Quality of Life
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organisation. World Health Organisation. Obesity-and-Overweight. Who.int. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 3 March 2021).
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Abera, S.F.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Institute of Public Health. National Health and Morbidity Survey 2019: Technical Report Volume I; Ministry of Health: Putrajaya, Malaysia, 2020. [Google Scholar]
- Simmonds, M.; Burch, J.; Llewellyn, A.; Griffiths, C.; Yang, H.; Owen, C.; Duffy, S.; Woolacott, N. The use of measures of obesity in childhood for predicting obesity and the development of obesity-related diseases in adulthood: A systematic review and meta-analysis. Health Technol. Assess. 2015, 19, 1–336. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaul, R.; Angrish, P.; Saha, S.; Halder, S.; Bhattacharya, B.; Mitra, M. Association between Obesity and Oral Health Status in Schoolchildren: A Survey in Five Districts of West Bengal, India. Int. J. Clin. Pediatr. Dent. 2018, 11, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Killedar, A.; Lung, T.; Petrou, S.; Teixeira-Pinto, A.; Tan, E.J.; Hayes, A. Weight status and health-related quality of life during childhood and adolescence: Effects of age and socioeconomic position. Int. J. Obes. 2020, 44, 637–645. [Google Scholar] [CrossRef] [PubMed]
- Drummond, B.K.; Brosnan, M.G.; Leichter, J.W. Management of periodontal health in children: Pediatric dentistry and periodontology interface. Periodontology 2000 2017, 74, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Franchini, R.; Petri, A.; Migliario, M.; Rimondini, L. Poor oral hygiene and gingivitis are associated with obesity and overweight status in paediatric subjects. J. Clin. Periodontol. 2011, 38, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- D’Avila, H.F.; Poll, F.A.; Reuter, C.P.; Burgos, M.S.; Mello, E.D. Health-related quality of life in adolescents with excess weight. J. Pediatr. (Versão em Português) 2019, 95, 495–501. [Google Scholar] [CrossRef]
- Listl, S.; Galloway, J.; Mossey, P.; Marcenes, W. Global Economic Impact of Dental Diseases. J. Dent. Res. 2015, 94, 1355–1361. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Baez, R.J. Oral Health Surveys: Basic Methods, 5th ed.; World Health Organization: Geneva, Switzerland, 2013; Available online: https://apps.who.int/iris/handle/10665/97035 (accessed on 3 March 2021).
- Nishi, M.; Bratthall, D.; Stjernswärd, J. How to Calculate the Significant Caries Index (SiC Index); WHO Collaborating Centre/Faculty of Odontology, University of Malmö: Malmö, Sweden, 2001. [Google Scholar]
- Ainamo, J.; Bay, I. Problems and proposals for recording gingivitis and plaque. Int. Dent. J. 1975, 25, 229–235. [Google Scholar] [CrossRef] [PubMed]
- Eckel, R.H.; Matsuzawa, Y.; Després, J.P. Waist circumference as a vital sign in clinical practice: A Consensus Statement from the IAS and ICCR Working Group on Visceral Obesity. Nat. Rev. Endocrinol. 2020, 16, 177–189. [Google Scholar] [CrossRef]
- Bahagian Pembangunan Kurikulum Kementerian Pendidikan Malaysia; Panduan Standard Kecergasan Fizikal Kebangsaan untuk Murid Sekolah Malaysia (SEGAK); Ministry of Education: Putrajaya, Malaysia, 2016.
- Li, L.-W.; Wong, H.M.; Gandhi, A.; McGrath, C.P. Caries-related risk factors of obesity among 18-year-old adolescents in Hong Kong: A cross-sectional study nested in a cohort study. BMC Oral Health 2018, 18, 188. [Google Scholar] [CrossRef] [PubMed]
- Hemmingsson, E. Early Childhood Obesity Risk Factors: Socioeconomic Adversity, Family Dysfunction, Offspring Distress, and Junk Food Self-Medication. Curr. Obes. Rep. 2018, 7, 204–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nihtila, A.; West, N.; Lussi, A.; Bouchard, P.; Ottolenghi, L.; Senekola, E.; Llodra, J.C.; Viennot, S.; Bourgeois, D. Oral Health Behavior and Lifestyle Factors among Overweight and Non-Overweight Young Adults in Europe: A Cross-Sectional Questionnaire Study. Health 2016, 4, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oral Health Division, Ministry of Health Malaysia. National Oral Health Survey of Schoolchildren 2007 (NOHSS 2007): 16-Year-olds. November 2010. Available online: http://ohd.moh.gov.my/images/pdf/nohp20112020.pdf (accessed on 3 March 2021).
- Oral Health Division, Ministry of Health Malaysia. National Health Morbidity Survey 2017: Oral Health Status of Schoolchildren in Malaysia: National Oral Health Survey of Schoolchildren (NOHSS) 2017 Survey Findings; Ministry of Health: Putrajaya, Malaysia, 2019. [Google Scholar]
- Chen, D.; Zhi, Q.; Zhou, Y.; Tao, Y.; Wu, L.; Lin, H. Association between dental caries and BMI in Children: A systematic review and meta-analysis. Caries Res. 2018, 52. [Google Scholar] [CrossRef] [PubMed]
- Zandoná, A.F.; Santiago, E.; Eckert, G.; Katz, B.; De Oliveira, S.P.; Capin, O.; Mau, M.; Zero, D. The Natural History of Dental Caries Lesions. J. Dent. Res. 2012, 91, 841–846. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alshihri, A.A.; Rogers, H.J.; Alqahtani, M.A.; Aldossary, M.S. Association between Dental Caries and Obesity in Children and Young People: A Narrative Review. Int. J. Dent. 2019, 2019, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Banu, A.; Șerban, C.; Pricop, M.; Urechescu, H.; Vlaicu, B. Dental health between self-perception, clinical evaluation and body image dissatisfaction—A cross-sectional study in mixed dentition pre-pubertal children. BMC Oral Health 2018, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Van Vuuren, C.L.; Wachter, G.G.; Veenstra, R.; Rijnhart, J.J.M.; Van Der Wal, M.F.; Chinapaw, M.J.M.; Busch, V. Associations between overweight and mental health problems among adolescents, and the mediating role of victimization. BMC Public Health 2019, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Characteristics | Baseline n (%) | Follow-Up n (%) | p Value | Cohen’s Effect Size | ||
|---|---|---|---|---|---|---|
| OW/OB n = 195 | NW n = 202 | OW/OB n = 122 | NW n = 116 | |||
| Gender | ||||||
| Male | 124 (31.2) | 118 (29.7) | 73 (30.7) | 73 (30.7) | 0.03 1 | |
| Female | 71 (17.9) | 84 (21.2) | 49 (20.6) | 43 (18.1) | 0.81 | |
| Ethnicity | ||||||
| Malays | 117 (29.5) | 105 (26.4) | 72 (30.3) | 68 (28.6) | 0.05 * | 0.05 1 |
| Non-Malays | 78 (19.7) | 97 (24.5) | 50 (21.0) | 48 (20.2) | ||
| Mother level of education | ||||||
| High | 57 (14.4) | 67 (16.9) | 32 (13.4) | 35 (14.7) | 0.79 | 0.02 1 |
| Low | 138 (34.8) | 135 (34.1) | 90 (37.8) | 81 (34.0) | ||
| BMI (kg/m2) (Mean) (SD) | 28.5 (4.01) | 19.2 (1.84) | 29.6 (4.30) | 19.6 (1.67) | 0.02 1 | |
| Baseline n (%) | Follow-Up n (%) | |||||
|---|---|---|---|---|---|---|
| OW/OB n = 122 | NW n = 116 | SIC n = 79 | OW/OB n = 122 | NW n = 116 | SIC n = 79 | |
| Frequency of tooth brushing | X2 = 0.26, p = 0.87 | X2 = 0.49, p = 0.77 | ||||
| 2x/day | 89 (37.0) | 95 (39.9) | 64 (81.0) | 91 (38.4) | 91 (38.4) | 65 (82.3) |
| ≤1x/day | 33 (14.2) | 21 (8.8) | 15 (19.0) | 31 (12.6) | 25 (10.5) | 13 (16.5) |
| Used fluoride toothpaste | X2 = 2.28, p = 0.13 | X2 = 0.26, p = 0.87 | ||||
| Yes | 120 (50.4) | 110 (46.2) | 76 (96.2) | 78 (35.5) | 69 (29.5) | 55 (69.6) |
| No | 2 (0.8) | 6 (2.5) | 3 (3.8) | 14 (5.9) | 15 (6.3) | 24 (30.4) |
| Used mouth rinse | X2 = 0.00, p = 0.94 | X2 = 0.49, p = 0.77 | ||||
| Yes | 120 (50.4) | 110 (46.2) | 21 (26.6) | 25 (10.5) | 22 (9.3) | 15 (19.0) |
| No | 2 (0.8) | 6 (2.5) | 58 (73.4) | 97 (40.9) | 93 (39.2) | 64 (81.0) |
| Perception of health | X2 = 5.46, p = 0.17 | X2 = 2.98, p = 0.08 | ||||
| Poor | 43 (18.1) | 25 (10.5) | 24 (30.4) | 61 (26.1) | 46 (19.7) | 32 (40.5) |
| Good | 79 (33.2) | 91 (38.2) | 55 (69.6) | 58 (24.8) | 69 (29.5) | 46 (58.2) |
| Perception of oral health | X2 = 0.00, p = 0.97 | X2 = 3.13, p = 0.77 | ||||
| Poor | 45 (18.9) | 43 (18.1) | 33 (41.8) | 65 (27.9) | 50 (21.5) | 36 (45.6) |
| Good | 77 (32.4) | 73 (30.7) | 46 (58.2) | 53 (22.7) | 65 (27.9) | 41 (51.9) |
| Visited dentist for the past 1 year | X2 = 1.14, p = 0.56 | X2 = 0.56, p = 0.45 | ||||
| Yes | 16 (6.7) | 26 (10.9) | 12 (15.2) | 17 (7.2) | 17 (7.2) | 8 (10.1) |
| No | 106 (44.5) | 90 (37.8) | 67 (84.8) | 104 (43.9) | 99 (41.8) | 71 (89.9) |
| Total Participants, n = 238 | Baseline * M ± SD | Follow-Up ** M ± SD | p Value | ||
|---|---|---|---|---|---|
| OW/OB | NW | OW/OB | NW | ||
| Caries experience | 1.80 (3.16) | 1.84 (2.62) | 2.37 (3.30) | 2.47 (3.05) | 0.91 *, 0.79 ** |
| Based on teeth | |||||
| Decayed (D) | 1.66 (3.10) | 1.53 (2.35) | 2.11 (3.16) | 2.07 (2.70) | 0.71 *, 0.92 ** |
| Missing (M) | 0 | 0.03 (0.18) | 0.01 (0.09) | 0.06 (0.24) | 0.03 *, 0.02 ** |
| Filled (F) | 0.13 (0.48) | 0.27 (0.92) | 0.25 (0.72) | 0.34 (1.10) | 0.57 *, 0.45 ** |
| Sound dentition n (%) | 73 (59.8) | 60 (51.7) | 56 (45.9) | 42 (36.2) | |
| Periodontal status n (%) | |||||
| BPE screening | |||||
| Code 0 | 8 (6.6) | 6 (5.2) | 7 (6.0) | 10 (8.2) | |
| Code 1 | 20 (16.4) | 15 (12.9) | 49 (42.2) | 39 (32.0) | |
| Code 2 | 94 (77.0) | 95 (81.9) | 60 (51.7) | 73 (59.8) | |
| Gingival bleeding n (%) | >0.05 + | ||||
| Yes | 118 (96.7) | 112 (96.6) | 111 (91.0) | 106 (91.4) | |
| No | 4 (3.3) | 4 (3.4) | 11 (9.0) | 10 (8.6) | |
| Significant Caries Index (SiC) n =79 | 5.22 (3.90) | 4.48 (2.70) | 6.49 (3.08) | 5.80 (2.73) | 0.32 *, 0.28 ** |
| Based on teeth | |||||
| Decayed (D) | |||||
| Missing (M) | 4.89 (4.0) | 3.70 (2.70) | 5.80 (3.46) | 4.83 (2.67) | 0.11 *, 0.17 ** |
| Filled (F) | 0 | 0.07 (0.26) | 0.03 (0.16) | 0.12 (0.33) | 0.10 *, 0.12 ** |
| 0.32 (0.75) | 0.71 (1.42) | 0.68 (1.13) | 0.83 (1.68) | 0.12 *, 0.63 ** | |
| Periodontal status n (%) | |||||
| BPE screening | |||||
| Code 0 | 0 | ||||
| Code 1 | 5 (13.5) | 1 (2.4) | 3 (8.1) | 2 (4.8) | |
| Code 2 | 32 (86.5) | 5 (11.9) | 19 (51.4) | 18 (42.9) | |
| 36 (85.7) | 15 (40.5) | 22 (52.4) | |||
| Gingival bleeding n (%) | |||||
| Yes | 37 (100) | ||||
| No | 0 | 41 (97.6) | 34 (91.9) | 38 (90.5) | >0.05 + |
| 1 (2.4) | 3 (8.1) | 4 (9.5) | |||
| Baseline * M ± SD | Follow-Up ** M ± SD | p Value | |||||
|---|---|---|---|---|---|---|---|
| OW/O | NW | SiC + | OW/OB | NW | SiC + | ||
| OHIP severity | 9.14 (6.37) | 8.63 (5.97) | 9.83 (6.68) | 6.80 (7.49) | 7.52 (6.65) | 8.18 (7.47) | 0.53 *, 0.75 *+, 0.45 **, 0.57 **+ |
| OHIP Impact based on items (n, %) | |||||||
| Functional limitation | |||||||
| (trouble pronouncing words) | 0 | 1 (1.3) | 1 (1.3) | 1 (0.4) | 2 (0.8) | 3 (3.8) | |
| Functional limitation | |||||||
| (worsened sense of taste) | 1 (1.3) | 0 | 1 (1.3) | 4 (1.7) | 1 (0.4) | 8 (10.1) | |
| Physical pain | |||||||
| (painful aching in the mouth) | 1 (1.3) | 1 (1.3) | 2 (2.5) | 2 (0.8) | 2 (0.8) | 6 (7.6) | |
| Physical pain | |||||||
| (uncomfortable eating) | 2 (2.5) | 0 | 2 (2.5) | 6 (2.5) | 1 (0.4) | 6 (7.6) | |
| Psychological discomfort | |||||||
| (self-consciousness) | 5 (6.3) | 8 (10.1) | 13 (16.5) | 12 (5.0) | 16 (6.7) | 15 (19.0) | |
| Psychological discomfort | |||||||
| (felt tense) | 4 (5.1) | 2 (2.5) | 6 (7.6) | 7 (2.9) | 9 (3.8) | 8 (10.1) | >0.05 *** |
| Physical disability | |||||||
| (diet has been unsatisfactory) | 2 (2.5) | 2 (2.5) | 4 (5.1) | 5 (2.1) | 5 (2.1) | 7 (8.9) | |
| Physical disability | |||||||
| (meals interrupted) | 1 (1.3) | 1 (1.3) | 2 (2.5) | 5 (2.1) | 8 (3.4) | 6 (7.6) | |
| Psychological disability | |||||||
| (difficult to relax) | 0 | 1 (1.3) | 4 (5.1) | 3 (1.3) | 1 (0.4) | 3 (3.8) | |
| Psychological disability | |||||||
| (been embarrassed) | 3 (3.8) | 1 (1.3) | 1 (1.3) | 0 | 2 (0.8) | 4 (5.1) | |
| Social disability | |||||||
| (been irritable with others) | 8 (10.1) | 1 (1.3) | 9 (11.4) | 17 (7.1) | 6 (2.5) | 2 (2.5) | |
| Social disability | |||||||
| (difficulty doing schoolwork) | 0 | 1 (1.3) | 1 (1.3) | 0 | 2 (0.8) | 2 (2.5) | |
| Handicap (felt life is less satisfying) | 0 | 0 | 0 | 0 | 1 (0.4) | 2 (2.5) | |
| Handicap | |||||||
| (unable to perform usual function) | 1 (1.3) | 2 (2.5) | 3 (3.8) | 3 (1.3) | 4 (1.7) | 5 (6.3) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tengku H, T.N.N.; Peh, W.Y.; Shoaib, L.A.; Baharuddin, N.A.; Vaithilingam, R.D.; Saub, R. Oral Diseases and Quality of Life between Obese and Normal Weight Adolescents: A Two-Year Observational Study. Children 2021, 8, 435. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060435
Tengku H TNN, Peh WY, Shoaib LA, Baharuddin NA, Vaithilingam RD, Saub R. Oral Diseases and Quality of Life between Obese and Normal Weight Adolescents: A Two-Year Observational Study. Children. 2021; 8(6):435. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060435
Chicago/Turabian StyleTengku H, Tengku Nurfarhana Nadirah, Wei Ying Peh, Lily Azura Shoaib, Nor Adinar Baharuddin, Rathna Devi Vaithilingam, and Roslan Saub. 2021. "Oral Diseases and Quality of Life between Obese and Normal Weight Adolescents: A Two-Year Observational Study" Children 8, no. 6: 435. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060435