
Ectopic Eruption of Maxillary First Permanent Molars: Preliminary Results of Prevalence and Dentoskeletal Characteristics in Spanish Paediatric Population

 , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design and Ethical Aspects
2.2. Study Population
2.3. Radiological Analysis
2.4. Statistical Analysis
3. Results
3.1. Ectopic Eruption and Gender
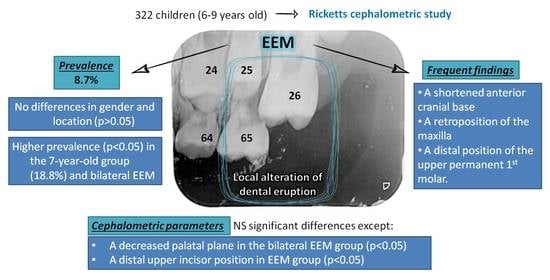
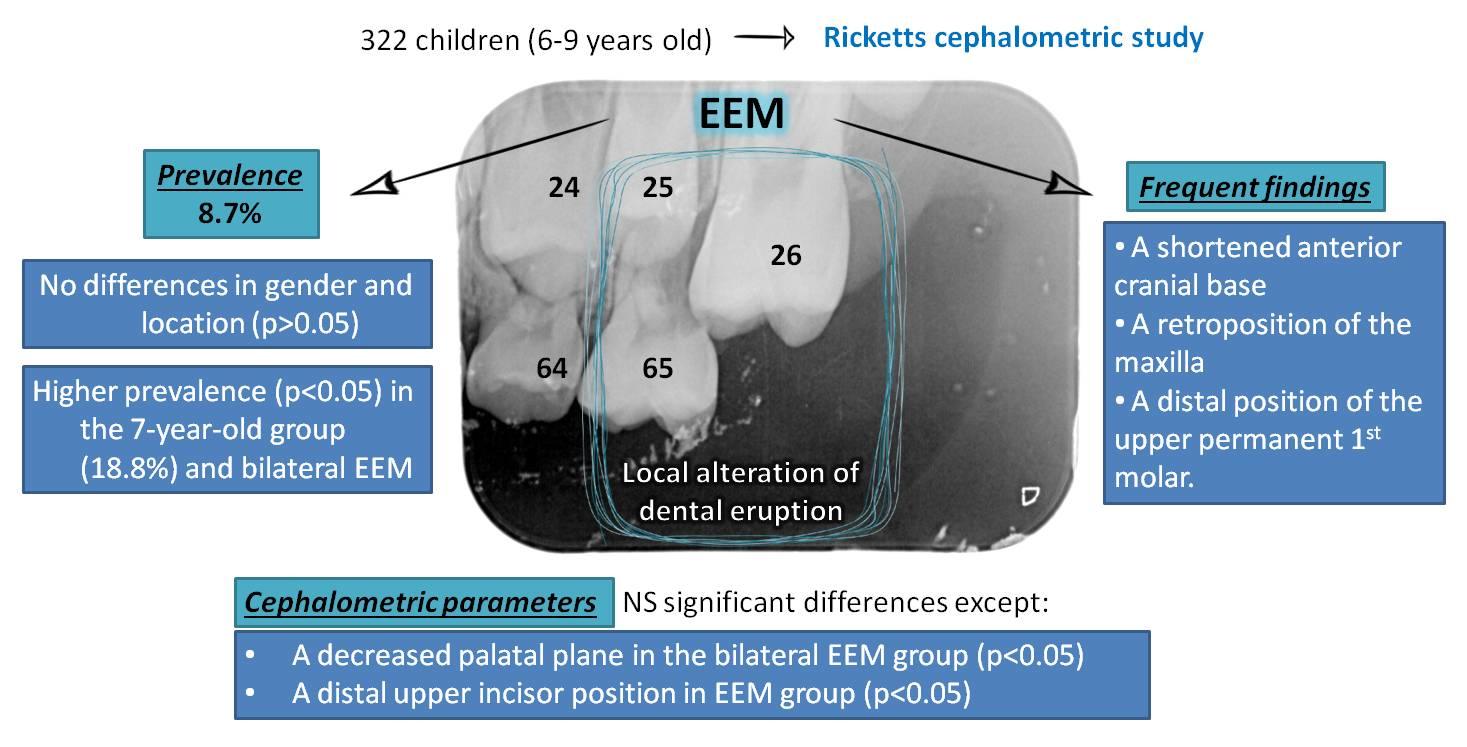
3.2. Ectopic Eruption and Age Group
3.3. Ectopic Eruption Location
3.4. Ectopic Eruption and Cephalometric Parameters
- The facial convexity values were slightly increased in the EEM group.
- There was a slight increase in lower facial height in the EEM group.
- The upper first molar was on average 0.3 mm more posterior with respect to the vertical pterygoid in children without EEM.
- The upper incisor had a position 0.7 mm more anterior in the group of children without EEM, with significant differences with respect to patients with EEM (p < 0.05), and there was a variability of almost 1 mm regarding its inclination.
- Facial depth tended to be negative in patients with EEM, while in patients without this pathology it was positive, with a mean difference greater than 1 mm.
- The facial axis was 1 mm increased in the EEM group.
- The maxillary depth is increased compared to the control group.
- Maxillary height presented a higher mean value in children without EEM.
- The palatal plane presented similar values between patients with and without EEM (p < 0.05). Intergroup differences were found (p = 0.017), determining that the difference was significant in the bilateral EEM group with respect to the unilateral EEM and control groups, finding lower values in the bilateral EEM in comparison to the other groups studied.
- Cranial deflection had a higher mean value in the group with EEM.
- The anterior cranial length was higher in the group without EEM, with a difference greater than 1 mm.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Young, D.H. Ectopic eruption of the first permanent molar. J. Dent. Child. 1957, 24, 153–162. [Google Scholar]
- Kupietzky, A. Correction of ectopic eruption of permanent molars utilizing the brass wire technique. Pediatr. Dent. 2000, 22, 408–412. [Google Scholar]
- Yeung, C.Y.; Chu, C.H. A review of the eruption of primary teeth. OA Dent. 2014, 2, 7. [Google Scholar]
- Ge, C. Ectopic eruption of the first permanent maxillary molar in cleft lip and cleft palate children. J. Dent. Child. 1965, 32, 179–188. [Google Scholar]
- Bjerklin, K.; Kurol, J. Prevalence of ectopic eruption of the maxillary first permanent molar. Swed Dent. J. 1981, 5, 29–34. [Google Scholar]
- Kurol, J.; Bjerklin, K. Resorption of maxillary second primary molars caused by ectopic eruption of the maxillary first permanent molar: A longitudinal and histological study. ASDC J. Dent. Child. 1982, 49, 273–279. [Google Scholar]
- Chintakanon, K.; Boonpinon, P. Ectopic eruption of the first permanent molars: Prevalence and etiologic factors. Angle Orthod. 1998, 68, 153–160. [Google Scholar]
- Kimmel, N.A.; Gellin, M.E.; Bohannan, H.M.; Kaplan, A.L. Ectopic eruption of maxillary first permanent molars in different areas of the United States. ASDC J. Dent. Child. 1982, 49, 294–299. [Google Scholar]
- Pulver, F. The etiology and prevalence of ectopic eruption of the maxillary first permanent molar. ASDC J. Dent. Child. 1968, 35, 138–146. [Google Scholar]
- Chapman, H. First upper permanent molars partially impacted against second deciduous molars. Int. J. Ortho. Oral Surg. Radio. 1923, 9, 339–345. [Google Scholar] [CrossRef]
- Cheyne, V.D.; Wessels, K.E. Impaction of permanent first molar with resorption and space loss in region of deciduous second molar. J. Am. Dent. Assoc. 1947, 35, 774–787. [Google Scholar] [CrossRef]
- Bjerklin, K.; Kurol, J. Ectopic eruption of the maxillary first permanent molar: Etiologic factors. Am. J. Orthod. 1983, 84, 147–155. [Google Scholar] [CrossRef]
- Salzmann, J.A. Orthodontics: Principles and Prevention; Lippincott: New York, NY, USA, 1957. [Google Scholar]
- Harrison, L.M., Jr.; Michal, B.C. Treatment of ectopically erupting permanent molars. Dent. Clin. N. Am. 1984, 28, 57–67. [Google Scholar]
- Yuen, S.; Chan, J.; Tay, F. Ectopic eruption of the maxillary permanent first molar: The effect of increased mesial angulation on arch length. JADA (1939) 1985, 111, 447–451. [Google Scholar] [CrossRef]
- Canut, J.A.; Raga, C. Morphological analysis of cases with ectopic eruption of the maxillary first permanent molar. Eur. J. Orthod. 1983, 5, 249–253. [Google Scholar] [CrossRef] [Green Version]
- Ricketts, R.M. Cephalometric analysis and synthesis. Angle Orthod. 1961, 31, 141–156. [Google Scholar]
- Kurol, J.; Bjerklin, K. Ectopic eruption of maxillary first permanent molars: A review. ASDC J. Dent. Child. 1986, 53, 209–214. [Google Scholar]
- Mucedero, M.; Rozzi, M.; Cardoni, G.; Ricchiuti, M.R.; Cozza, P. Dentoskeletal features in individuals with ectopic eruption of the permanent maxillary first molar. Korean J. Orthod. 2015, 45, 190. [Google Scholar] [CrossRef] [Green Version]
- Rah, Y.; Lee, J.; Ra, J. Association between Ectopic Eruption of the Maxillary First Permanent Molar and Skeletal Malocclusion. J. Korean Acad. Pediatr. Dent. 2017, 44, 147–153. [Google Scholar] [CrossRef]
- Barberia-Leache, E.; Suarez-Clúa, M.C.; Saavedra-Ontiveros, D. Ectopic eruption of the maxillary first permanent molar: Characteristics and occurrence in growing children. Angle Orthod. 2005, 75, 610–615. [Google Scholar]
- O’Meara, W.F. Ectopic eruption pattern in selected permanent teeth. J. Dent. Res. 1962, 41, 607–616. [Google Scholar] [CrossRef]
- Sweet, C.A. Ectopic eruption of permanent teeth. J. Am. Dent. Assoc. 1939, 26, 574–579. [Google Scholar] [CrossRef]
- Lower, D.J. Ectopic Eruption of Teeth. Chron. Omaha. Dist. D. Soc. 1960, 23, 270. [Google Scholar]
- Niliforuk, G. Ectopic Eruption. J. Ontario DA 1948, 25, 241. [Google Scholar]
- Bjork, A. The face in profile. Sven. Tidskr. 1947, 40, 30–50. [Google Scholar]
- Solow, B. The pattern of craniofacial associations. Acta Odontol. Scand. 1966, 24. [Google Scholar]

{kind=link}
| Orthopantomography 1 | Lateral Teleradiography 2 |
|---|---|
| Nominal voltage: 208/220/230/240 V | Nominal voltage: 380 V |
| Rated current: 12 A | Tube: Comet, rotating anode |
| Frequency: 50/60 Hz | Tube voltage: 50–125 kV |
| Tube stream: 9–16 mA | Tube stream: 25–300 mA |
| Aluminum equivalent filter 2.5 mm | Focus-midline distance: 152 cm |
| Focal size 0.5 × 0.5 mm | Focal size: 0.3 × 0.3 mm |
| Medium technique used: 65 kV y 12 mA | Medium technique used: 80 kV y 20 mA |
| Fixed time: 12 s | Midline-image receptor distance: 12 cm |
| EEM | Total | ||||
|---|---|---|---|---|---|
| No | Yes | ||||
| Gender | Male | N (%) | 146 (90.1) | 16 (9.9) | 162 (100) |
| Female | N (%) | 148 (92.5) | 12 (7.5) | 160 (100) | |
| Total | N (%) | 294 (91.3) | 28 (8.7) | 322 (100) | |
| EEM | Total | ||||
|---|---|---|---|---|---|
| No | Yes | ||||
| Age group (years) | 6 | N (%) | 71(88.8%) | 9 (11.3%) | 80 (100%) |
| 7 | N (%) | 65 (81.3%) | 15 (18.8%) * | 80 (100%) | |
| 8 | N (%) | 78 (97.5%) | 2 (2.5%) | 80 (100%) | |
| 9 | N (%) | 80 (97.6%) | 2 (2.4%) | 82 (100%) | |
| Total | N (%) | 294 (91.3%) | 28 (8.7%) | 322 (100%) | |
| Non EEM | Unilateral EEM | Bilateral EEM | Chi-Square (sig +) | ANOVA (sig) | |
|---|---|---|---|---|---|
| Facial convexity | 1.00 ± 2.52 | 1.20 ± 2.71 | 1.27 ± 2.38 | 0.357 | 0.886 |
| Inferior facial height | −3.15 ± 4.32 | −2.70 ± 2.42 | −3.55 ± 4.37 | 0.363 | 0.875 |
| Upper molar to TPV | 1.66 ± 2.95 | 0.79 ± 1.84 | 0.76 ± 2.12 | 0.281 | 0.304 |
| Upper incisor position | 2.10 ± 3.08 * | 1.02 ± 1.97 | 0.95 ± 1.92 | 0.046 * | 0.167 |
| Upper incisor angulation | 0.81 ± 9.05 | 1.74 ± 6.47 | −0.01 ± 5.96 | 0.145 | 0.876 |
| Facial depth | 0.59 ± 3.36 | −0.52 ± 1.98 | −0.92 ± 3.51 | 0.494 | 0.114 |
| Facial axis | −1.14 ± 4.35 | −2.42 ± 3.76 | −1.75 ± 4.82 | 0.343 | 0.569 |
| Maxillar depth | −0.01 ± 3.87 | −0.03 ± 3.05 | −0.36 ± 2.74 | 0.660 | 0.926 |
| Maxillar height | 4.30 ± 3.46 | 3.97 ± 3.72 | 3.51 ± 3.88 | 0.525 | 0.622 |
| Palatal plane | 1.77 ± 3.15 | 2.28 ± 1.76 | −0.32 ± 2.14 * | 0.145 | 0.017 * |
| Cranial deflection | 1.18 ± 2.09 | 1.86 ± 2.26 | 0.94 ± 2.15 | 0.494 | 0.526 |
| Anterior cranial length | 1.19 ± 3.14 | −0.05 ± 3.00 | 0.14 ± 3.02 | 0.406 | 0.193 |
| Author, Year | Sample Size | Cases (%) |
|---|---|---|
| Cheyne, 1947 | 500 | 9 (1.8) |
| Young, 1957 | 1619 | 52 (3.2) |
| O’Meara, 1961 | 315 | 6 (2.0) |
| Pulver, 1968 | 831 | 26 (3.1) |
| Bjerklin, 1981 | 2903 | 126 (4.3) |
| Kimmel, 1982 | 5277 | 202 (3.8) |
| Canut, 1983 | 800 | 26 (3.3) |
| Chintakanon, 1998 | 3612 | 27 (0.8) |
| Barberia-Leache, 2005 | 509 | 22 (4.3) |
| Mucedero, 2005 | 1052 | 26 (2.5) |
| Rah, 2017 | 786 | 93 (11.8) |
| Present study | 322 | 28 (8.7%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Helm, A.; Martín-Vacas, A.; Molinero-Mourelle, P.; Caleya, A.M.; Gallardo, N.E.; Mourelle-Martínez, M.R. Ectopic Eruption of Maxillary First Permanent Molars: Preliminary Results of Prevalence and Dentoskeletal Characteristics in Spanish Paediatric Population. Children 2021, 8, 479. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060479
Helm A, Martín-Vacas A, Molinero-Mourelle P, Caleya AM, Gallardo NE, Mourelle-Martínez MR. Ectopic Eruption of Maxillary First Permanent Molars: Preliminary Results of Prevalence and Dentoskeletal Characteristics in Spanish Paediatric Population. Children. 2021; 8(6):479. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060479
Chicago/Turabian StyleHelm, Alexandra, Andrea Martín-Vacas, Pedro Molinero-Mourelle, Antonia M. Caleya, Nuria E. Gallardo, and María Rosa Mourelle-Martínez. 2021. "Ectopic Eruption of Maxillary First Permanent Molars: Preliminary Results of Prevalence and Dentoskeletal Characteristics in Spanish Paediatric Population" Children 8, no. 6: 479. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060479