
The Child Behavior Checklist as a Screening Instrument for PTSD in Refugee Children

Abstract
:1. Introduction
2. Methods
2.1. Assessment
2.2. Psychometric Testing and Statistical Analyses
2.3. Statistical Analysis
3. Results
3.1. Participants
3.2. Test Results
3.2.1. Item-Frequencies and Item/Criterion-Item/Total Correlations
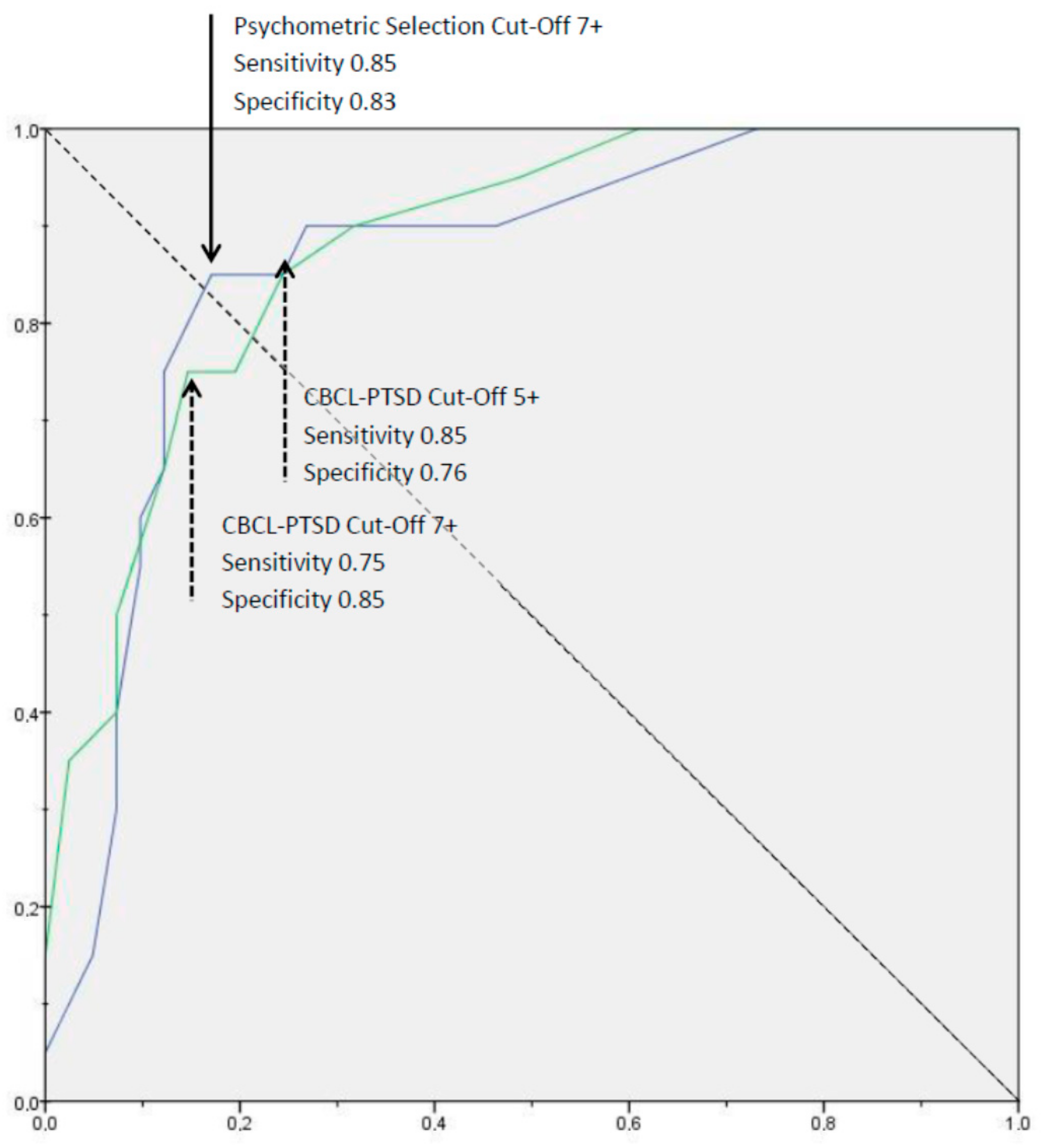
3.2.2. Internal Consistency and Proposed Cut-Offs
4. Discussion
Strengths & Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alberer, M.; Wendeborn, M.; Löscher, T.; Seilmaier, M. Spectrum of diseases occurring in refugees and asylum seekers: Data from three different medical institutions in the Munich area from 2014 and 2015. Dtsch. Med. Wochenschr. 2016, 141, e8–e15. [Google Scholar] [PubMed]
- van Berlaer, G.; Carbonell, F.B.; Manantsoa, S.; de Béthune, X.; Buyl, R.; Debacker, M.; Hubloue, I. A refugee camp in the centre of Europe: Clinical characteristics of asylum seekers arriving in Brussels. BMJ Open 2016, 6, e013963. [Google Scholar] [CrossRef] [Green Version]
- Alpak, G.; Unal, A.; Bulbul, F.; Sagaltici, E.; Bez, Y.; Altindag, A.; Dalkilic, A.; Savas, H.A. Post-traumatic stress disorder among Syrian refugees in Turkey: A cross-sectional study. Int. J. Psychiatry Clin. Pract. 2015, 19, 45–50. [Google Scholar] [CrossRef] [PubMed]
- Fazel, M.; Wheeler, J.; Danesh, J. Prevalence of serious mental disorder in 7000 refugees resettled in western countries: A systematic review. Lancet 2005, 365, 1309–1314. [Google Scholar] [CrossRef]
- Slone, M.; Mann, S. Effects of War, Terrorism and Armed Conflict on Young Children: A Systematic Review. Child Psychiatry Hum. Dev. 2016, 47, 950–965. [Google Scholar] [CrossRef] [PubMed]
- Soykoek, S.; Mall, V.; Nehring, I.; Henningsen, P.; Aberl, S. Post-traumatic stress disorder in Syrian children of a German refugee camp. Lancet 2017, 389, 903–904. [Google Scholar] [CrossRef] [Green Version]
- Gutermann, J.; Schreiber, F.; Matulis, S.; Schwartzkopff, L.; Deppe, J.; Steil, R. Psychological Treatments for Symptoms of Posttraumatic Stress Disorder in Children, Adolescents, and Young Adults: A Meta-Analysis. Clin. Child Fam. Psychol. Rev. 2016, 19, 77–93. [Google Scholar] [CrossRef] [PubMed]
- Morina, N.; Koerssen, R.; Pollet, T.V. Interventions for children and adolescents with posttraumatic stress disorder: A meta-analysis of comparative outcome studies. Clin. Psychol. Rev. 2016, 47, 41–54. [Google Scholar] [CrossRef] [PubMed]
- AACAP. Practice Parameter for the Assessment and Treatment of Children and Adolescents with Posttraumatic Stress Disorder. J. Am. Acad. Child Adolesc. Psychiatry 2010, 49, 414–430. [Google Scholar]
- Gadeberg, A.; Montgomery, E.; Frederiksen, H.; Norredam, M. Assessing trauma and mental health in refugee children and youth: A systematic review of validated screening and measurement tools. Eur. J. Public Health 2017, 27, 439–446. [Google Scholar] [CrossRef] [Green Version]
- Foa, E.B.; Johnson, K.M.; Feeny, N.C.; Treadwell, K.R.H. The child PTSD Symptom Scale: A preliminary examination of its psychometric properties. J. Clin. Child. Psychol. 2001, 30, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Steinberg, A.M.; Brymer, M.J.; Decker, K.B.; Pynoos, R.S. The UCLA PTSD Reaction Index. Curr. Psychiatry Rep. 2004, 6, 96–100. [Google Scholar] [CrossRef]
- Tagay, S.; Düllmann, S.; Hermans, E.; Repic, N.; Hiller, R.; Senf, W. Das Essener Trauma-Inventar für Kinder und Jugendliche (ETI-KJ). 2007. Available online: https://www.uni-due.de/rke-pp/essenertraumainventareti.php (accessed on 15 May 2017).
- Levendosky, A.A.; Huth-Bocks, A.C.; Semel, M.A.; Shapiro, D.L. Trauma symptoms in preschool-age children exposed to domestic violence. J. Interpers. Violence 2002, 17, 150–164. [Google Scholar] [CrossRef]
- Dehon, C.; Scheeringa, M.S. Screening for Preschool Posttraumatic Stress Disorder with the Child Behavior Checklist. J. Pediatric. Psychol. 2006, 31, 431–435. [Google Scholar] [CrossRef]
- Wolfe, V.V.; Gentile, C.; Wolfe, D.A. The Impact of Sexual Abuse on Children: A PTSD Formulation. Behav. Ther. 1989, 20, 215–228. [Google Scholar] [CrossRef]
- Ruggiero, K.J.; McLeer, S.V. PTSD scale of the Child Behavior Checklist: Concurrent and discriminant validity with non-clinic-referred sexually abused children. J. Trauma. Stress 2000, 13, 287–299. [Google Scholar] [CrossRef]
- Adler, N.; Stewart, J. The MacArthur Scale of Subjective Social Status. 2007. Available online: http://www.macses.ucsf.edu/research/psychosocial/subjective.php (accessed on 15 May 2017).
- Nehring, I.; Schlag, E.; Qirjako, E.; Büyükyaglioglu, C.; Mall, V.; Sattel, H.; Sack, M.; Henningsen, P.; Aberl, S. Health State of Syrian Children and Their Parents in a German Refugee Camp. J. Refug. Stud. 2019, 29. [Google Scholar] [CrossRef]
- Unnewehr, S.; Schneider, S.; Margraf, J. Kinder-DIPS: Diagnostisches Interview bei Psychischen Störungen im Kindes- und Jugendalter; Springer: Berlin/Heidelberg, Germany, 2009. [Google Scholar]
- Irblich, A.G.D.; Landhold, M.A. Posttraumatische Belastungsstörungen bei Säuglingen und Kleinkindern [Posttraumatic Stress Disorder in Infants and Toddlers]. Praxis der Kinderpsychologie und Kinderpsychiatrie 2008, 57, 247–263. [Google Scholar]
- Scheeringa, M.S.; Zeanah, C.H. PTSD Semi-Structured Interview and Observation Record for Infants and Young Children; T.U.H.S.C. Department of Psychiatry and Neurology: New Orleans, LA, USA, 1994. [Google Scholar]
- Achenbach, T.M. Manual for the Child Behavior Checklist 4-18 and 1991 Profile; University of Vermont, Department of Psychiatry: Burlington, VT, USA, 1991. [Google Scholar]
- Döpfner, M.U.A. Elternfragebogen Über das Verhalten von Kindern und Jugendlichen: Deutsche Beabeitung der Child Behavior Checklist (CBCL/4-18). 1998. Available online: www.testzentrale.de (accessed on 1 June 2013).
- Achenbach, T.M.; Rescorla, L.A. Chapter 9 Reliability, Internal Consistency, Cross-Informant Agreement, and Stability in Manual for the ASEBA School-Age Forms and Profiles; University of Vermont, Research Center for Children, Youth, & Families: Burlington, VT, USA, 2001. [Google Scholar]
- Clark, L.A.; Watson, D. Constructing validity: Basic issues in objective scale development. Psychol. Assess. 1995, 7, 309–319. [Google Scholar] [CrossRef]
- Lienert, G.A.; Raatz, U. Testaufbau und Testanalyse; Beltz PVU: Weinheim, Germany, 1998. [Google Scholar]
- Moosbrugger, H.; Kelava, A. (Eds.) Deskriptivstatistische Evaluation von Items (Itemanalyse) und Testwertverteilungen, in Testtheorie und Fragebogenkonstruktion; Springer: Berlin/Heidelberg, Germany, 2007. [Google Scholar]
- Fan, J.; Upadhye, S.; Worster, A. Understanding receiver operating characteristic (ROC) curves. CJEM 2006, 8, 19–20. [Google Scholar] [CrossRef] [PubMed]
- McLeer, S.V.; Callaghan, M.; Henry, D.; Wallen, J. Psychiatric disorders in sexually abused children. J. Am. Acad. Child Adolesc. Psychiatry 1994, 33, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Ozbaran, B.; Erermis, S.; Bukusoglu, N.; Bildik, T.; Tamar, M.; Ercan, E.S.; Aydin, C.; Cetin, S.K. Social and emotional outcomes of child sexual abuse: A clinical sample in Turkey. J. Interpers Violence 2009, 24, 1478–1493. [Google Scholar] [CrossRef] [PubMed]
- Hecker, T.; Maerker, A. Komplexe posttraumatische Belastungsstörung nach ICD-11. Psychotherapeut 2015, 60, 547. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| PTSD (n = 20) | No PTSD (n = 41) | |
|---|---|---|
| Children 4–14 years | ||
| Age (years (SD)) | 8.2 (2.5) | 9.3 (2.9) |
| Boys (n) | 12 | 24 |
| Religion (n) | ||
| Islam | 19 | 39 |
| Other | 1 | 2 |
| In Germany since, months (SD) | 1.1 (1.1) | 1.1 (1.0) |
| n (%) | |
|---|---|
| Interview partner (n = 38) | |
| mother | 27 (71.1) |
| father | 11 (28.9) |
| Country of birth | |
| Syria | 35 (92.1) |
| other (Iraq, Jordan, Libya) | 3 (7.9) |
| Religion | |
| Islam | 36 (94.7) |
| other | 2 (5.3) |
| Mother tongue | |
| Arabic | 30 (78.9) |
| Kurdish | 5 (13.2) |
| other | 3 (7.9) |
| Communication (language) problems in Germany 1 | 29 (76.3) |
| Feels socially isolated 2 | 17 (44.7) |
| Community-based subjective sociodemographic status in Germany above the median 3 | 19 (51.3) |
| Society-based subjective sociodemographic status in Germany above the median 3 | 12 (35.3) |
| CBCL Item Selections | Coincidence of Item with PTSD Diagnosis 1 | Occurrence/Frequency 2 [%] | Item—Total Correlation 1 (CBCL-PTSD-Scale) | Item—Total Correlation 1 (Psycho-Metrically Guided Item Selection) |
|---|---|---|---|---|
| Frequent Behaviors, Well Associated with a PTSD-Diagnosis Overlapping Items of both Item Selections | ||||
| Unhappy, sad. or depressed a | 0.60 | 47.5 | 0.762 | 0.766 |
| Nightmares a | 0.48 | 41.0 | 0.597 | 0.702 |
| Cannot concentrate, cannot pay attention for long a | 0.45 | 23.0 | 0.483 | 0.552 |
| Sudden changes in mood or feelings a | 0.45 | 19.7 | 0.537 | 0.554 |
| Trouble sleeping a | 0.42 | 36.1 | 0.522 | 0.588 |
| Too fearful, anxious a | 0.39 | 37.7 | 0.451 | 0.507 |
| Stubborn, sullen/irritable a | 0.38 | 34.4 | 0.451 | 0.468 |
| Fears certain places, animals, situations other than school a | 0.37 | 35.0 | 0.467 | 0.412 |
| Nervous, high-strung, or tense a | 0.33 | 25.0 | 0.455 | 0.480 |
| Clings to adults or too dependent a | 0.22 | 35.0 | 0.381 | 0.394 |
| Argues a lot a | 0.20 | 45.9 | 0.257 | 0.274 |
| Rare/Unassociated Behaviors Additional Items of CBCL-PTSD Subscale | ||||
| Withdrawn, does not get involved with others | 0.36 | 9.8 | 0.337 | – |
| Stomachaches and cramps | 0.25 | 13.1 | 0.203 | – |
| Feels others are out to get him/her | 0.25 | 13.1 | 0.305 | – |
| Cannot get his/her mind off certain thoughts, obsessions | 0.25 | 13.1 | 0.367 | – |
| Feels too guilty | 0.12 | 9.8 | 0.258 | – |
| Vomiting and throwing up | 0.07 | 3.3 | 0.061 | – |
| Secretive and keeps things to self | 0.03 | 27.9 | 0.249 | – |
| Headaches | 0.01 | 5.0 | 0.140 | – |
| Nausea and feels sick | −0.04 | 6.7 | 0.000 | – |
| Additional Psychometrically Suitable Items (Psychometrically Guided Item Selection) | ||||
| Disobedient at home | 0.41 | 32.8 | – | 0.561 |
| Impulsive or acts without thinking | 0.32 | 21.3 | – | 0.590 |
| Cries a lot | 0.30 | 39.3 | – | 0.649 |
| Too shy or timid | 0.28 | 36.1 | – | 0.371 |
| Does not get along with others | 0.28 | 23.3 | – | 0.383 |
| Worries | 0.27 | 29.7 | – | 0.653 |
| Can’t sit still, restless, or hyperactive | 0.22 | 26.2 | – | 0.373 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nehring, I.; Sattel, H.; Al-Hallak, M.; Sack, M.; Henningsen, P.; Mall, V.; Aberl, S. The Child Behavior Checklist as a Screening Instrument for PTSD in Refugee Children. Children 2021, 8, 521. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060521
Nehring I, Sattel H, Al-Hallak M, Sack M, Henningsen P, Mall V, Aberl S. The Child Behavior Checklist as a Screening Instrument for PTSD in Refugee Children. Children. 2021; 8(6):521. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060521
Chicago/Turabian StyleNehring, Ina, Heribert Sattel, Maesa Al-Hallak, Martin Sack, Peter Henningsen, Volker Mall, and Sigrid Aberl. 2021. "The Child Behavior Checklist as a Screening Instrument for PTSD in Refugee Children" Children 8, no. 6: 521. https://0-doi-org.brum.beds.ac.uk/10.3390/children8060521