
Patient-Reported Outcome Measures and Clinical Outcomes in Children with Foregut Anomalies

 , , ,
, , ,
Abstract
:
1. Introduction
2. Materials and Methods
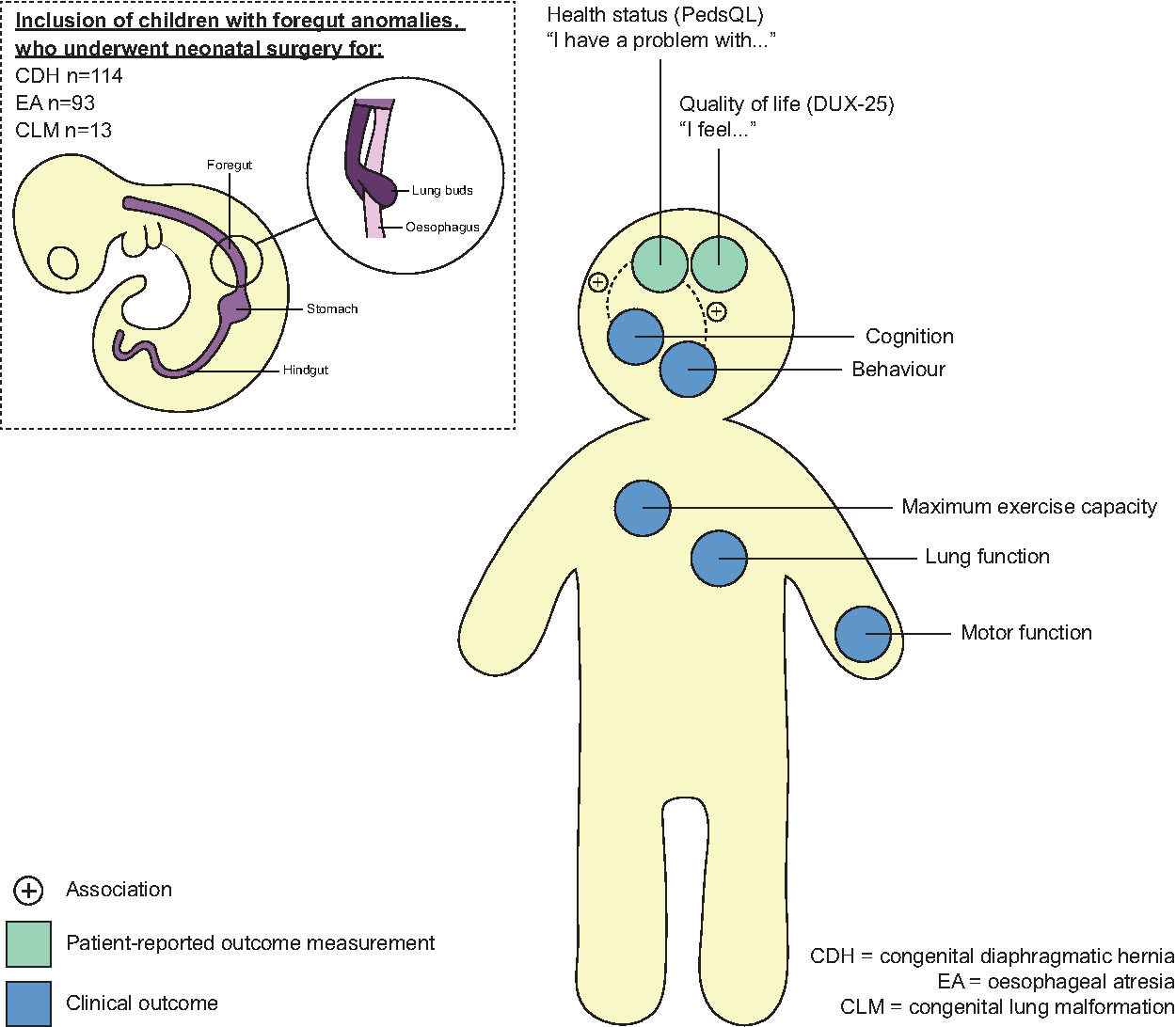
2.1. Study Population
2.2. Data Collection
2.3. Data Analysis
3. Results
3.1. Patient Characteristics
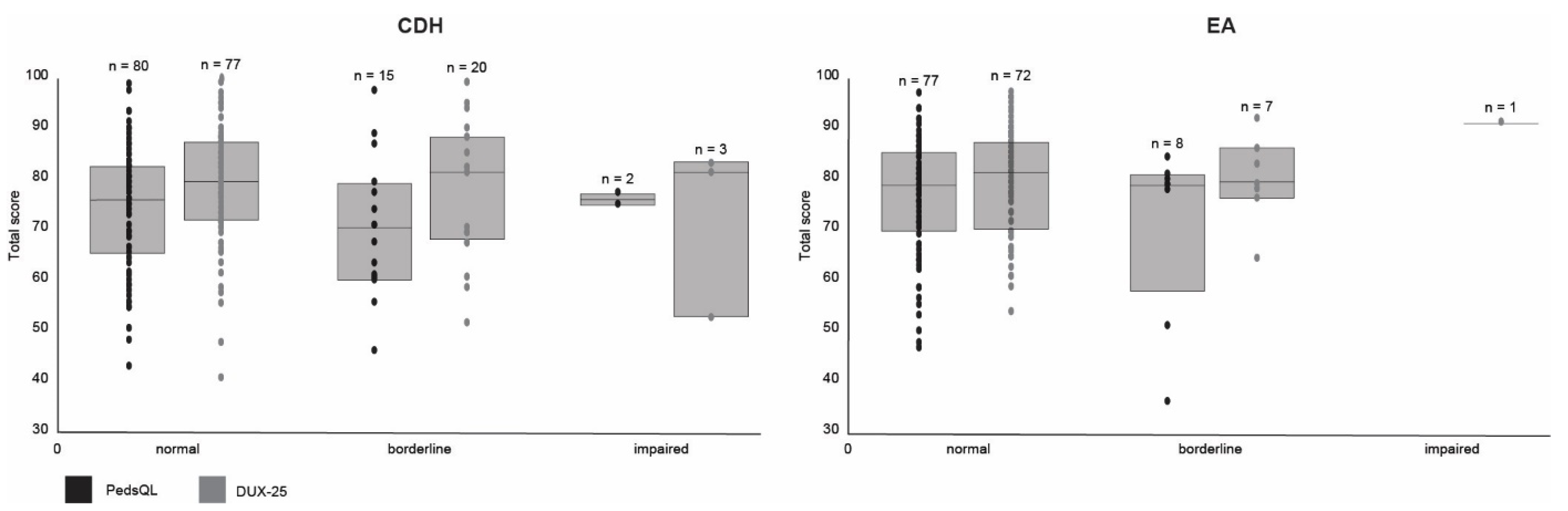
3.2. CDH
3.3. EA
3.4. CLM
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wijlaars, L.P.M.M.; Gilbert, R.; Hardelid, P. Chronic conditions in children and young people: Learning from administrative data. Arch. Dis. Child. 2016, 101, 881–885. [Google Scholar] [CrossRef] [Green Version]
- Ijsselstijn, H.; Gischler, S.J.; Wijnen, R.M.; Tibboel, D. Assessment and significance of long-term outcomes in pediatric surgery. Semin. Pediatr. Surg. 2017, 26, 281–285. [Google Scholar] [CrossRef] [Green Version]
- The Lancet Child Adolescent Health. Surviving and thriving through childhood. Lancet Child Adolesc. Health 2018, 2, 305. [Google Scholar] [CrossRef]
- Porter, M.E. What Is Value in Health Care? N. Engl. J. Med. 2010, 363, 2477–2481. [Google Scholar] [CrossRef] [PubMed]
- Fayed, N.; de Camargo, O.K.; Kerr, E.; Rosenbaum, P.; Dubey, A.; Bostan, C.; Faulhaber, M.; Raina, P.; Cieza, A. Generic patient-reported outcomes in child health research: A review of conceptual content using World Health Organization definitions. Dev. Med. Child Neurol. 2012, 54, 1085–1095. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.E.; Lee, T.H. From Volume to Value in Health Care: The Work Begins. JAMA 2016, 316, 1047–1048. [Google Scholar] [CrossRef] [PubMed]
- Withers, K.; Palmer, R.; Lewis, S.; Carolan-Rees, G. First steps in PROMs and PREMs collection in Wales as part of the prudent and value-based healthcare agenda. Qual. Life Res. 2020, 1–14. [Google Scholar] [CrossRef]
- Gischler, S.J.; Mazer, P.; Duivenvoorden, H.J.; van Dijk, M.; Bax, N.M.; Hazebroek, F.W.; Tibboel, D. Interdisciplinary structural follow-up of surgical newborns: A prospective evaluation. J. Pediatr. Surg. 2009, 44, 1382–1389. [Google Scholar] [CrossRef]
- Toussaint, L.C.; Zijp, M.H.V.D.C.-V.; Janssen, A.J.; Tibboel, D.; van Heijst, A.; Ijsselstijn, H. Perceived Motor Competence Differs from Actual Performance in 8-Year-Old Neonatal ECMO Survivors. Pediatrics 2016, 137, e20152724. [Google Scholar] [CrossRef] [Green Version]
- Madderom, M.J.; Gischler, S.J.; Duivenvoorden, H.; Tibboel, D.; Ijsselstijn, H. Neonatal extracorporeal membrane oxygenation: Impaired health at 5 years of age. Pediatr. Crit. Care Med. 2013, 14, 183–193. [Google Scholar] [CrossRef]
- Leeuwen, L.; Schiller, R.M.; Rietman, A.B.; van Rosmalen, J.; Wildschut, E.D.; Houmes, R.J.M.; Tibboel, D.; IJsselstijn, H. Risk Factors of Impaired Neuropsychologic Outcome in School-Aged Survivors of Neonatal Critical Illness. Crit. Care Med. 2018, 46, 401–410. [Google Scholar] [CrossRef]
- Harmsen, W.J.; Aarsen, F.J.; Zijp, M.H.M.V.D.C.-V.; Van Rosmalen, J.M.; Wijnen, R.M.H.; Tibboel, D.; Ijsselstijn, H. Developmental problems in patients with oesophageal atresia: A longitudinal follow-up study. Arch. Dis. Child. Fetal Neonatal Ed. 2017, 102, F214–F219. [Google Scholar] [CrossRef] [PubMed]
- Toussaint-Duyster, L.C.C.; van der Cammen-van Zijp, M.H.M.; Takken, T.; Harmsen, W.J.; Tibboel, D.; van Heijst, A.F.J.; de Blaauw, I.; Wijnen, R.M.H.; van Rosmalen, J.; IJsselstijn, H. Improvement of exercise capacity following neonatal respiratory failure: A randomized controlled trial. Scand. J. Med. Sci. Sports. 2020, 30, 662–671. [Google Scholar] [CrossRef] [PubMed]
- Toussaint-Duyster, L.C.C.; Zijp, M.H.M.V.D.C.; Spoel, M.; Tiddens, H.A.W.M.; Tibboel, D.; Wijnen, R.M.H.; Van Rosmalen, J.; Ijsselstijn, H. Lung function in school-aged congenital diaphragmatic hernia patients; a longitudinal evaluation. Pediatr. Pulmonol. 2019, 54, 1257–1266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNally, H.; Bennett, C.C.; Elbourne, D.; Field, D.J. United Kingdom collaborative randomized trial of neonatal extracorporeal membrane oxygenation: Follow-up to age 7 years. Pediatrics 2006, 117, e845–e854. [Google Scholar] [CrossRef] [PubMed]
- Gross, R.E. The Surgery of Infancy and Childhood: Its Principles and Techniques; W.B. Saunders Co.: Philadelphia, PA, USA, 1953. [Google Scholar]
- Delestrain, C.; Khen-Dunlop, N.; Hadchouel, A.; Cros, P.; Ducoin, H.; Fayon, M.; Gibertini, I.; Labbé, A.; Labouret, G.; Lebras, M.-N.; et al. Respiratory Morbidity in Infants Born with a Congenital Lung Malformation. Pediatrics 2017, 139, e20162988. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perined (Hoftiezer) Geboortegewichtcurven. Available online: https://www.perined.nl/producten/geboortegewichtcurven (accessed on 31 May 2020).
- Solomon, B.D.; Baker, L.A.; Bear, K.A.; Cunningham, B.K.; Giampietro, P.F.; Hadigan, C.; Hadley, D.W.; Harrison, S.; Levitt, M.A.; Niforatos, N.; et al. An Approach to the Identification of Anomalies and Etiologies in Neonates with Identified or Suspected VACTERL (Vertebral Defects, Anal Atresia, Tracheo-Esophageal Fistula with Esophageal Atresia, Cardiac Anomalies, Renal Anomalies, and Limb Anomalies) Association. J. Pediatr. 2014, 164, 451–457.e1. [Google Scholar]
- Centraal Bureau voor de Statistiek. Leerlingen in het Basisonderwijs. 2020. Available online: https://opendata.cbs.nl/statline/#/CBS/nl/dataset/83295NED/table?ts=1529498582881 (accessed on 18 January 2021).
- UNESCO Institute of Statistics. International Standard Classification of Education (ISCED). 2011. Available online: http://uis.unesco.org/en/topic/international-standard-classification-education-isced (accessed on 20 June 2021).
- Morsberger, J.L.; Short, H.L.; Baxter, K.J.; Travers, C.; Clifton, M.S.; Durham, M.M.; Raval, M.V. Parent reported long-term quality of life outcomes in children after congenital diaphragmatic hernia repair. J. Pediatr. Surg. 2019, 54, 645–650. [Google Scholar] [CrossRef]
- Mikkelsen, A.; Boye, B.; Diseth, T.; Malt, U.; Mørkrid, L.; Ijsselstijn, H.; Emblem, R. Traumatic stress, mental health and quality of life in adolescents with esophageal atresia. J. Pediatr. Surg. 2020. [Google Scholar] [CrossRef]
- Pullens, B.; Dulfer, K.; Buysse, C.; Hoeve, L.; Timmerman, M.; Joosten, K. Long-term quality of life in children after open airway surgery for laryngotracheal stenosis. Int. J. Pediatr. Otorhinolaryngol. 2016, 84, 88–93. [Google Scholar] [CrossRef]
- Ta, N.H.; Gao, J.; Philpott, C. A systematic review to examine the relationship between objective and patient-reported outcome measures in sinonasal disorders: Recommendations for use in research and clinical practice. Int. Forum Allergy Rhinol. 2021, 11, 910–923. [Google Scholar] [CrossRef]
- Hoorens, V. Self-enhancement and Superiority Biases in Social Comparison. Eur. Rev. Soc. Psychol. 1993, 4, 113–139. [Google Scholar] [CrossRef]
- Conijn, J.M.; Smits, N.; Hartman, E.E. Determining at What Age Children Provide Sound Self-Reports: An Illustration of the Validity-Index Approach. Assessment 2020, 27, 1604–1618. [Google Scholar] [CrossRef] [PubMed]
- Toussaint-Duyster, L.C.C.; van der Cammen-van Zijp, M.H.M.; de Jongste, J.C.; Tibboel, D.; Wijnen, R.M.H.; Gischler, S.J.; Van Rosmalen, J.; Ijsselstijn, H.; Toussaint-Duyster, L.C. Congenital diaphragmatic hernia and exercise capacity, a longitudinal evaluation. Pediatr. Pulmonol. 2019, 54, 628–636. [Google Scholar] [CrossRef] [Green Version]
- Jové Blanco, A.; Gutiérrez Vélez, A.; Solís-García, G.; Salcedo Posadas, A.; Bellón Alonso, S.; Rodríguez Cimadevilla, J.L. Comorbidities and course of lung function in patients with congenital esophageal atresia. Arch. Argent Pediatr. 2020, 118, 25–30. [Google Scholar]
- Wiebe, S.; Guyatt, G.; Weaver, B.; Matijevic, S.; Sidwell, C. Comparative responsiveness of generic and specific quality-of-life instruments. J. Clin. Epidemiol. 2003, 56, 52–60. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| CDH | EA | CLM | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Participants (n = 114 *) | Non-Participants (n = 65) | p-Value | Participants (n = 93) | Non-Participants (n = 58) | p-Value | Participants (n = 13) | Non-Participants (n = 6) | p-Value | |
| Baseline characteristics | |||||||||
| Male | 70 (61.4) | 36 (55.4) | 0.53 | 57 (61.3) | 37 (63.8) | 0.45 | 10 (76.9) | 3 (50.0) | 0.32 |
| Gestational age in weeks | 38.7 (37.7–39.6) | 38.6 (38.0–39.9) | 0.87 | 37.9 (36.2–40.0) | 38.4 (36.1–40.0) | 0.81 | 38.7 (36.8–40.4) | 38.4 (37.5–39.9) | 0.58 |
| Birth weight in grams | 3000 (2800–3445) | 3000 (2503–3480) | 0.71 | 2850 (2160–3180) | 2735 (2108–3128) | 0.38 | 3265 (3070–3690) | 3088 (2846–3888) | 0.42 |
| Preterm birth | 14 (12.3) | 12 (18.5) | 0.18 | 32 (34.4) | 20 (34.5) | 0.50 | 3 (23.1) | 1 (16.7) | 1.00 |
| Small for gestational age A | 28 (24.6) | 10 (15.4) | 0.55 | 36 (38.7) | 21 (36.2) | 0.57 | 0 | 1 (16.7) | |
| Side of hernia | |||||||||
| Left | 98 (86.0) | 55 (84.6) | 0.83 | ||||||
| Right | 16 (14.0) | 10 (15.4) | 0.83 | ||||||
| Type repair | |||||||||
| Primary repair | 40 (35.1) | 24 (36.9) | 0.70 | ||||||
| Patch | 73 (64.0) | 41 (63.1) | 0.70 | ||||||
| Unknown | 1 (0.9) | 0 | |||||||
| Type of EA B | |||||||||
| Type A | 7 (7.5) | 6 (10.3) | 0.56 | ||||||
| Type B | 0 | 2 (3.4) | |||||||
| Type C | 82 (88.2) | 43 (74.1) | 0.06 | ||||||
| Type D | 0 | 1 (1.7) | |||||||
| Type E | 3 (3.2) | 4 (6.9) | 0.43 | ||||||
| Unknown | 1 (1.1) | 2 (3.4) | |||||||
| Staged repair | 10 (10.8) | 12 (20.7) | 0.10 | ||||||
| Type of CLM | |||||||||
| CPAM | 7 (53.8) | 5 (83.3) | 0.04 | ||||||
| BPS | 2 (15.4) | 1 (16.7) | 1.00 | ||||||
| CLE | 3 (23.1) | 0 | |||||||
| BC | 0 | 0 | |||||||
| Hybrid C | 1 (7.7) | 0 | |||||||
| Associated problems | |||||||||
| VACTERL D | 11 (11.8) | 12 (20.7) | 0.17 | ||||||
| Major anomalies | 26 (22.8) | 13 (20.0) | 0.71 | 35 (37.6) | 29 (50.0) | 0.18 | 1 (7.7) | 0 | |
| Minor anomalies | 5 (4.4) | 6 (9.2) | 0.21 | 28 (30.1) | 23 (39.7) | 0.29 | 0 | 1 (16.7) | |
| Type of primary surgery | |||||||||
| Thoracotomy | 1 (0.9) | 0 | 63 (67.7) | 43 (74.1) | 0.36 | 10 (76.9) | 3 (50.0) | 1.00 | |
| Thoracoscopy | 33 (28.9) | 22 (33.8) | 0.40 | 28 (30.1) | 14 (24.1) | 0.58 | 2 (15.4) | 1 (16.7) | 1.00 |
| Laparotomy | 67 (58.8) | 30 (46.2) | 0.21 | 0 | 0 | 0 | 0 | ||
| Laparoscopy | 1 (0.9) | 3 (4.6) | 0.13 | 0 | 0 | 0 | 0 | ||
| Converted | 10 (8.8) | 6 (9.2) | 1.00 | 2 (2.2) | 0 | 0 | 0 | ||
| Unknown E | 1 (0.9) | 4 (6.2) | 0 | 1 (1.7) | 1 (7.7) | 2 (33.3) | |||
| Duration of anaesthetic exposure in the first 24 months of life in minutes | 270 (184–422) | 265 (170–505) | 0.90 | 393 (261–786) | 442 (299–798) | 0.25 | 203 (184–229) | 210 (58–264) | 0.80 |
| Characteristics at time of FU | |||||||||
| Age at FU | 8.2 (8.1–8.3) | 8.2 (8.1–8.3) | 8.2 (8.1–8.3) | ||||||
| Educational level | |||||||||
| Regular | 97 (85.1) | 26 (40.0) | 0.05 | 71 (76.3) | 30 (51.7) | 0.53 | 11 (84.6) | 1 (16.7) | 0.37 |
| Regular with help | 11 (9.6) | 4 (6.2) | 0.75 | 17 (18.3) | 3 (5.2) | 0.12 | 2 (15.4) | 1 (16.7) | 0.37 |
| Special education | 6 (5.3) | 7 (10.8) | 0.19 | 5 (5.4) | 7 (12.1) | 0.05 | 0 | 0 | |
| Other | 0 | 0 | 0 | 2 (3.4) | 0 | 0 | |||
| Unknown | 0 | 28 (43.1) | 0 | 16 (27.6) | 0 | 4 (66.7) | |||
| Maternal educational level | |||||||||
| Low (ISCED 0–2) | 8 (7.0) | 2 (3.1) | 1.00 | 15 (16.1) | 8 (13.8) | 1.00 | 2 (15.4) | 0 | |
| Middle (ISCED 3–4) | 43 (37.7) | 11 (16.9) | 0.53 | 37 (39.8) | 20 (34.5) | 0.86 | 2 (15.4) | 1 (16.7) | 1.00 |
| High (ISCED 5–8) | 47 (41.2) | 17 (26.2) | 0.53 | 39 (41.9) | 19 (32.8) | 0.86 | 7 (53.8) | 3 (50.0) | 1.00 |
| Unknown | 16 (14.0) | 35 (53.8) | 2 (2.2) | 11 (19.0) | 2 (15.4) | 2 (33.3) | |||
| CDH | EA | CLM | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Normal | Borderline | Impaired | Missing | Normal | Borderline | Impaired | Missing | Normal | Borderline | Impaired | Missing | ||
| Health and daily functioning | Cognition | 87 (76.3) | 21 (18.4) | 4 (3.5) | 2 (1.8) | 82 (88.2) | 9 (9.7) | 1 (1.1) | 1 (1.1) | 13 (100.0) | 0 | 0 | 0 |
| Proxy-reported behavior A | 68 (59.6) | 11 (9.6) | 15 (13.2) | 20 (17.5) | 51 (54.8) | 15 (16.1) | 5 (5.4) | 22 (23.7) | 8 (61.5) | 0 | 0 | 5 (38.5) | |
| Proxy-reported daily A executive functioning | 64 (56.1) | 5 (4.4) | 2 (1.8) | 43 (37.7) | 45 (48.4) | 2 (2.2) | 1 (1.1) | 45 (48.4) | 7 (53.8) | 0 | 0 | 6 (46.2) | |
| Motor function | 75 (65.8) | 37 (32.5) | 2 (1.8) | 65 (69.9) | 25 (26.9) | 3 (3.2) | 11 (84.6) | 2 (15.4) | 0 | ||||
| Maximum exercise capacity | 48 (42.1) | 52 (45.6) | 14 (12.3) | 43 (46.2) | 43 (46.2) | 7 (7.5) | 8 (61.5) | 4 (30.8) | 1 (7.7) | ||||
| Lung function | 69 (60.5) | 42 (36.8) | 3 (2.6) | 55 (59.1) | 37 (39.8) | 1 (1.1) | 7 (53.8) | 6 (46.2) | 0 | ||||
| No | Yes | Missing | No | Yes | Missing | No | Yes | Missing | |||||
| Gastroesophageal reflux A | 42 (36 8) | 4 (3.5) | 68 (59.6) | 40 (43.0) | 7 (7.5) | 46 (49.5) | 0 | 0 | 13 (100.0) | ||||
| Respiratory morbidity B | 105 (92.1) | 9 (7.9) | 0 | 60 (64.5) | 33 (33.5) | 0 | 12 (92.3) | 1 (7.7) | 0 | ||||
| Daily medication for physical condition | 87 (76.3) | 27 (23.7) | 0 | 70 (75.3) | 23 (24.7) | 0 | 11 (84.6) | 2 (15.4) | 0 | ||||
| Daily medication for psychological condition | 111 (97.4) | 3 (2.6) | 0 | 92 (98.9) | 1 (1.1) | 0 | 12 (92.3) | 1 (7.7) | 0 | ||||
| Scoliosis | 108 (94.5) | 6 (5.3) | 0 | 88 (94.6) | 5 (5.4) | 0 | 13 (100.0) | 0 | 0 | ||||
| Tube feeding | 112 (98.2) | 2 (1.8) | 0 | 89 (95.7) | 4 (4.3) | 0 | 13 (100.0) | 0 | 0 | ||||
| Home oxygen | 114 (100.0) | 0 | 0 | 92 (98.9) | 1 (1.1) | 0 | 13 (100.0) | 0 | 0 | ||||
| Independent Variables | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Cognition | Behavior | Motor Function | Maximum Exercise Capacity | Lung Function | |||||||||||
| Borderline (n = 21) | Impaired (n = 4) | Borderline (n = 11) | Impaired (n = 15) | Impaired (n = 37) | Impaired (n = 52) | Impaired (n = 42) | |||||||||
| Dependent variables | B | p-value | B | p-value | B | p-value | B | p-value | B | p-value | B | p-value | B | p-value | |
| CDH | PedsQL | ||||||||||||||
| Physical functioning | −16.57 | 0.042 * | −24.15 | 0.14 | −7.02 | 0.51 | −5.03 | 0.59 | 0.35 | 0.96 | −10.15 | 0.15 | −4.65 | 0.46 | |
| Emotional functioning | −17.36 | 0.031 * | −23.17 | 0.15 | −7.20 | 0.49 | −5.79 | 0.53 | 2.11 | 0.76 | −1.22 | 0.86 | −5.09 | 0.41 | |
| Social functioning | −19.91 | 0.017 * | −31.21 | 0.059 | −6.89 | 0.51 | −8.89 | 0.35 | −2.53 | 0.72 | −5.97 | 0.41 | −5.75 | 0.38 | |
| School functioning | −14.63 | 0.054 | −31.79 | 0.041 * | −13.71 | 0.18 | −8.39 | 0.33 | −2.33 | 0.72 | −0.14 | 0.98 | −4.16 | 0.48 | |
| Psychosocial health | −17.38 | 0.021 * | −28.60 | 0.056 | −8.17 | 0.40 | −7.84 | 0.36 | −0.41 | 0.95 | −3.72 | 0.57 | −4.82 | 0.41 | |
| Total score | −17.44 | 0.022 * | −26.76 | 0.079 | −8.87 | 0.36 | −6.63 | 0.44 | −0.26 | 0.97 | −5.06 | 0.43 | −4.86 | 0.41 | |
| DUX-25 | |||||||||||||||
| Physical functioning | 3.20 | 0.71 | −13.24 | 0.45 | 9.56 | 0.36 | −1.81 | 0.86 | 10.81 | 0.13 | −9.83 | 0.18 | −1.05 | 0.87 | |
| Home functioning | −1.30 | 0.88 | −20.49 | 0.28 | 17.58 | 0.096 | 1.14 | 0.91 | 12.41 | 0.086 | −9.87 | 0.18 | 0.89 | 0.90 | |
| Emotional functioning | −0.20 | 0.98 | −20.42 | 0.19 | 7.39 | 0.44 | −4.19 | 0.64 | 13.60 | 0.037 * | −7.04 | 0.29 | 1.24 | 0.84 | |
| Social functioning | −6.50 | 0.44 | −21.41 | 0.20 | 12.84 | 0.21 | −0.49 | 0.96 | 11.51 | 0.097 | −8.23 | 0.24 | −0.08 | 0.99 | |
| Close social functioning | −5.86 | 0.51 | −32.69 | 0.065 | 14.10 | 0.19 | −2.04 | 0.84 | 13.30 | 0.067 | −11.42 | 0.12 | 1.11 | 0.87 | |
| Far social functioning | −6.47 | 0.44 | −14.27 | 0.41 | 12.54 | 0.21 | 2.68 | 0.78 | 10.27 | 0.14 | −5.20 | 0.46 | −0.63 | 0.92 | |
| Total score | −0.82 | 0.92 | −18.72 | 0.26 | 10.58 | 0.30 | −2.01 | 0.83 | 12.00 | 0.071 | −8.95 | 0.19 | 0.41 | 0.95 | |
| Borderline (n = 9) | Impaired (n = 1) | Borderline (n = 15) | Impaired (n = 5) | Impaired (n = 25) | Impaired (n = 43) | Impaired (n = 37) | |||||||||
| B | p-value | B | p-value | B | p-value | B | p-value | B | p-value | B | p-value | B | p-value | ||
| EA | PedsQL | ||||||||||||||
| Physical functioning | −2.76 | 0.78 | −62.34 | 0.032 * | −3.56 | 0.64 | −23.65 | 0.092 | −10.24 | 0.095 | −3.10 | 0.63 | −7.60 | 0.19 | |
| Emotional functioning | −3.62 | 0.72 | −56.38 | 0.089 | 4.67 | 0.54 | −20.03 | 0.13 | −1.43 | 0.82 | 4.83 | 0.45 | −7.66 | 0.18 | |
| Social functioning | 1.82 | 0.87 | −63.43 | 0.043 * | −5.67 | 0.49 | −27.30 | 0.090 | −6.46 | 0.34 | −0.60 | 0.93 | −5.02 | 0.42 | |
| School functioning | −4.18 | 0.68 | −52.31 | 0.055 | −4.43 | 0.54 | −30.54 | 0.025 * | −7.03 | 0.22 | 1.07 | 0.87 | −7.62 | 0.16 | |
| Psychosocial health | −1.44 | 0.89 | −56.46 | 0.063 | −0.94 | 0.90 | −24.97 | 0.058 | −4.29 | 0.47 | 1.14 | 0.85 | −7.05 | 0.20 | |
| Total score | −2.82 | 0.77 | −58.90 | 0.044 * | −1.50 | 0.83 | −29.16 | 0.029 * | −6.32 | 0.28 | 1.20 | 0.84 | −6.50 | 0.23 | |
| DUX-25 | |||||||||||||||
| Physical functioning | −11.45 | 0.41 | 24.15 | 0.45 | −4.88 | 0.67 | −13.59 | 0.48 | 9.10 | 0.28 | 2.68 | 0.73 | 4.78 | 0.54 | |
| Home functioning | −16.20 | 0.23 | 14.38 | 0.67 | −7.52 | 0.52 | −2.60 | 0.89 | 12.84 | 0.13 | 3.42 | 0.66 | 6.68 | 0.39 | |
| Emotional functioning | −6.34 | 0.62 | 19.94 | 0.49 | −7.69 | 0.43 | −0.89 | 0.96 | 12.93 | 0.090 | 2.01 | 0.78 | 5.81 | 0.40 | |
| Social functioning | −7.07 | 0.58 | 8.42 | 0.79 | −4.57 | 0.67 | −6.74 | 0.69 | 12.60 | 0.11 | 4.97 | 0.50 | 5.87 | 0.42 | |
| Close social functioning | −6.19 | 0.66 | 7.97 | 0.80 | −9.15 | 0.41 | −5.19 | 0.79 | 12.85 | 0.12 | 3.40 | 0.60 | 10.03 | 0.19 | |
| Far social functioning | −5.60 | 0.67 | 6.86 | 0.83 | −1.77 | 0.87 | −15.27 | 0.39 | 11.74 | 0.13 | 7.17 | 0.33 | 4.10 | 0.56 | |
| Total score | −10.15 | 0.42 | 17.59 | 0.57 | −6.44 | 0.55 | −3.91 | 0.81 | 11.69 | 0.13 | 2.92 | 0.69 | 5.92 | 0.41 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sreeram, I.I.; ten Kate, C.A.; van Rosmalen, J.; Schnater, J.M.; Gischler, S.J.; Wijnen, R.M.H.; IJsselstijn, H.; Rietman, A.B. Patient-Reported Outcome Measures and Clinical Outcomes in Children with Foregut Anomalies. Children 2021, 8, 587. https://0-doi-org.brum.beds.ac.uk/10.3390/children8070587
Sreeram II, ten Kate CA, van Rosmalen J, Schnater JM, Gischler SJ, Wijnen RMH, IJsselstijn H, Rietman AB. Patient-Reported Outcome Measures and Clinical Outcomes in Children with Foregut Anomalies. Children. 2021; 8(7):587. https://0-doi-org.brum.beds.ac.uk/10.3390/children8070587
Chicago/Turabian StyleSreeram, Isabel I., Chantal A. ten Kate, Joost van Rosmalen, Johannes M. Schnater, Saskia J. Gischler, René M. H. Wijnen, Hanneke IJsselstijn, and André B. Rietman. 2021. "Patient-Reported Outcome Measures and Clinical Outcomes in Children with Foregut Anomalies" Children 8, no. 7: 587. https://0-doi-org.brum.beds.ac.uk/10.3390/children8070587