
Independent Risk Factors for RBC Transfusion in Children Undergoing Surgery. Analysis of 14,248 Cases at a German University Hospital
 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Aim
2.2. Data Acquisition
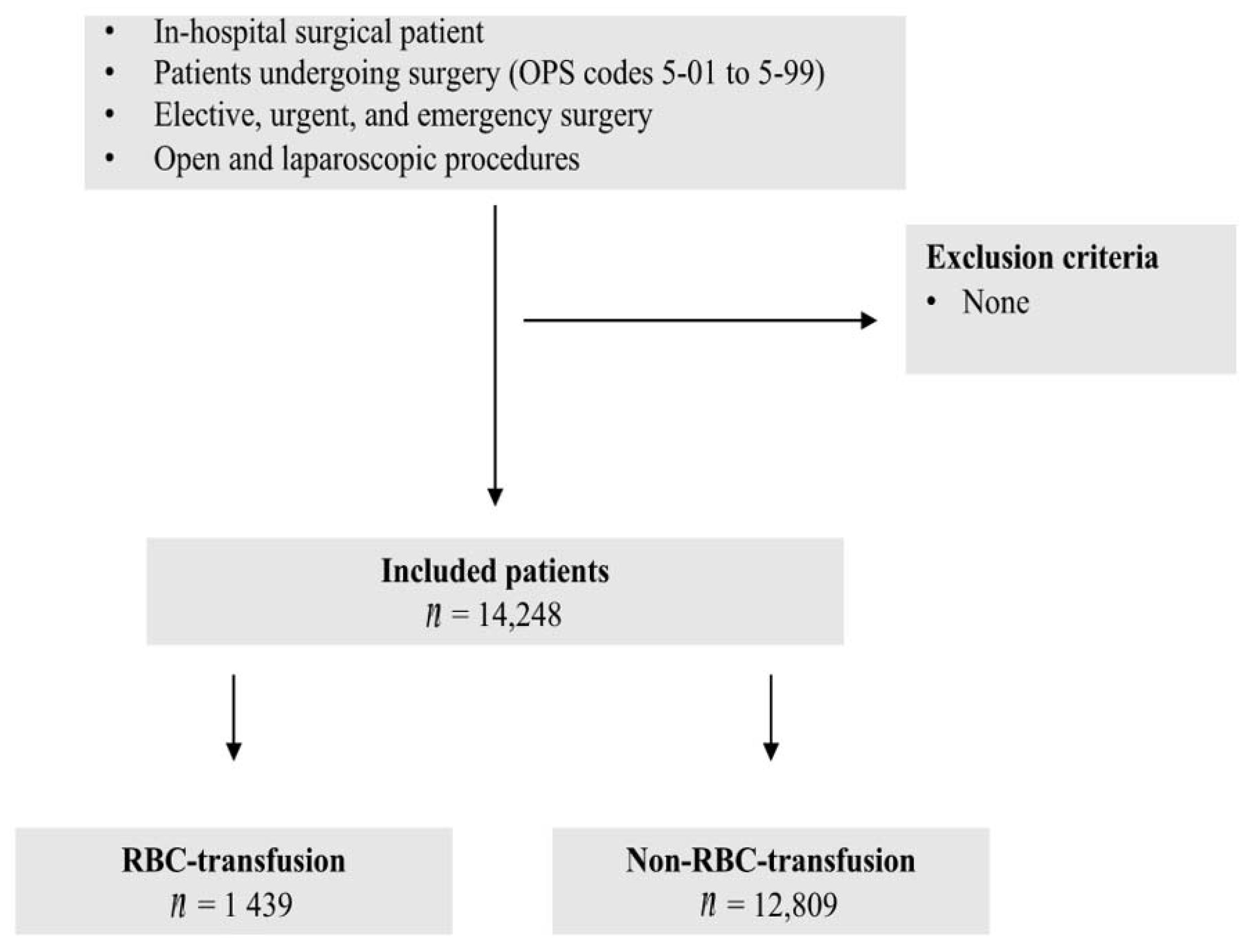
2.3. Patient Inclusion and Exclusion Criteria
2.4. Statistics
3. Results
3.1. Patients’ Characteristics
3.2. RBC Transfusion
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goobie, S.M.; Gallagher, T.; Gross, I.; Shander, A. Society for the advancement of blood management administrative and clinical standards for patient blood management programs. 4th edition (pediatric version). Paediatr. Anaesth. 2019, 29, 231–236. [Google Scholar] [CrossRef]
- Parker, R.I. Transfusion in critically ill children: Indications, risks, and challenges. Crit. Care Med. 2014, 42, 675–690. [Google Scholar] [CrossRef] [PubMed]
- Lavoie, J. Blood transfusion risks and alternative strategies in pediatric patients. Paediatr. Anaesth. 2011, 21, 14–24. [Google Scholar] [CrossRef]
- Howard-Quijano, K.; Schwarzenberger, J.C.; Scovotti, J.C.; Alejos, A.; Ngo, J.; Gornbein, J.; Mahajan, A. Increased red blood cell transfusions are associated with worsening outcomes in pediatric heart transplant patients. Anesth. Analg. 2013, 116, 1295–1308. [Google Scholar] [CrossRef]
- Stainsby, D.; Jones, H.; Wells, A.W.; Gibson, B.; Cohen, H.; Group, S.S. Adverse outcomes of blood transfusion in children: Analysis of UK reports to the serious hazards of transfusion scheme 1996–2005. Br. J. Haematol. 2008, 141, 73–79. [Google Scholar] [CrossRef]
- Vossoughi, S.; Perez, G.; Whitaker, B.I.; Fung, M.K.; Stotler, B. Analysis of pediatric adverse reactions to transfusions. Transfusion 2018, 58, 60–69. [Google Scholar] [CrossRef]
- Althoff, F.C.; Neb, H.; Herrmann, E.; Trentino, K.M.; Vernich, L.; Fullenbach, C.; Freedman, J.; Waters, J.H.; Farmer, S.; Leahy, M.F.; et al. Multimodal Patient Blood Management Program Based on a Three-pillar Strategy: A Systematic Review and Meta-analysis. Ann. Surg. 2019, 269, 794–804. [Google Scholar] [CrossRef] [PubMed]
- Meybohm, P.; Herrmann, E.; Steinbicker, A.U.; Wittmann, M.; Gruenewald, M.; Fischer, D.; Baumgarten, G.; Renner, J.; Van Aken, H.K.; Weber, C.F.; et al. Patient Blood Management is Associated with a Substantial Reduction of Red Blood Cell Utilization and Safe for Patient’s Outcome: A Prospective, Multicenter Cohort Study with a Noninferiority Design. Ann. Surg. 2016, 264, 203–211. [Google Scholar] [CrossRef]
- Piekarski, F.; Steinbicker, A.; Zacharowski, K.; Meybohm, P. Changes in Transfusion Practice in Children and Adolescents over Time. Transfus. Med. Hemotherapy 2020, 47, 379–384. [Google Scholar] [CrossRef] [PubMed]
- Piekarski, F.; Kaufmann, J.; Engelhardt, T.; Raimann, F.J.; Lustenberger, T.; Marzi, I.; Lefering, R.; Zacharowski, K.; Meybohm, P.; TraumaRegister, D.G.U. Changes in transfusion and fluid therapy practices in severely injured children: An analysis of 5118 children from the TraumaRegister DGU(R). Eur. J. Trauma Emerg. Surg. 2020. [Google Scholar] [CrossRef]
- de Gast-Bakker, D.H.; de Wilde, R.B.; Hazekamp, M.G.; Sojak, V.; Zwaginga, J.J.; Wolterbeek, R.; de Jonge, E.; Gesink-van der Veer, B.J. Safety and effects of two red blood cell transfusion strategies in pediatric cardiac surgery patients: A randomized controlled trial. Intensive Care Med. 2013, 39, 2011–2019. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Haemoglobin Concentrations for the Diagnosis of Anaemia and Assessment of Severity; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- R Core Team. R: A Language and Environment for Statistical Computing. R Foundation for Statistical Computing, Vienna, Austria. 2017. Available online: https://www.R-project.org/ (accessed on 23 July 2021).
- Faraoni, D.; DiNardo, J.A.; Goobie, S.M. Relationship between Preoperative Anemia and In-Hospital Mortality in Children Undergoing Noncardiac Surgery. Anesth. Analg. 2016, 123, 1582–1587. [Google Scholar] [CrossRef] [PubMed]
- Goobie, S.M.; Faraoni, D.; Zurakowski, D.; DiNardo, J.A. Association of Preoperative Anemia with Postoperative Mortality in Neonates. JAMA Pediatrics 2016, 170, 855–862. [Google Scholar] [CrossRef] [PubMed]
- Dunne, J.R.; Malone, D.; Tracy, J.K.; Gannon, C.; Napolitano, L.M. Perioperative anemia: An independent risk factor for infection, mortality, and resource utilization in surgery. J. Surg. Res. 2002, 102, 237–244. [Google Scholar] [CrossRef]
- Goobie, S.M.; DiNardo, J.A.; Faraoni, D. Relationship between transfusion volume and outcomes in children undergoing noncardiac surgery. Transfusion 2016, 56, 2487–2494. [Google Scholar] [CrossRef]
- Stey, A.M.; Vinocur, C.D.; Moss, R.L.; Hall, B.L.; Cohen, M.E.; Kraemer, K.; Ko, C.Y.; Kenney, B.D. Variation in intraoperative and postoperative red blood cell transfusion in pediatric surgery. Transfusion 2016, 56, 666–672. [Google Scholar] [CrossRef] [PubMed]
- Istaphanous, G.K.; Wheeler, D.S.; Lisco, S.J.; Shander, A. Red blood cell transfusion in critically ill children: A narrative review. Pediatric Crit. Care Med. 2011, 12, 174–183. [Google Scholar] [CrossRef]
- Lacroix, J.; Hebert, P.C.; Hutchison, J.S.; Hume, H.A.; Tucci, M.; Ducruet, T.; Gauvin, F.; Collet, J.P.; Toledano, B.J.; Robillard, P.; et al. Transfusion strategies for patients in pediatric intensive care units. N. Engl. J. Med. 2007, 356, 1609–1619. [Google Scholar] [CrossRef] [Green Version]
- Perez-Ferrer, A.; Gredilla-Diaz, E.; de Vicente-Sanchez, J.; Sanchez Perez-Grueso, F.; Gilsanz-Rodriguez, F. Implementation of a patient blood management program in pediatric scoliosis surgery. Rev. Esp. Anestesiol. Reanim. 2016, 63, 69–77. [Google Scholar] [CrossRef] [PubMed]
- Faraoni, D.; Meier, J.; New, H.V.; Van der Linden, P.J.; Hunt, B.J. Patient Blood Management for Neonates and Children Undergoing Cardiac Surgery: 2019 NATA Guidelines. J. Cardiothorac. Vasc. Anesth. 2019, 33, 3249–3263. [Google Scholar] [CrossRef]
- Kozek-Langenecker, S.A.; Ahmed, A.B.; Afshari, A.; Albaladejo, P.; Aldecoa, C.; Barauskas, G.; De Robertis, E.; Faraoni, D.; Filipescu, D.C.; Fries, D.; et al. Management of severe perioperative bleeding: Guidelines from the European Society of Anaesthesiology: First update 2016. Eur. J. Anaesthesiol. 2017, 34, 332–395. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| RBC-Transfusion n (%) 1439 (10.1%) | Non-RBC-Transfusion n (%) 12,809 (89.9%) | p-Value | |
|---|---|---|---|
| Patient characteristics | |||
| Gender male | 55.9% (53.3–58.5%); n = 805 | 61.3% (60.4–62.1%); n = 7846 | <0.001 |
| Age (years) | 4.9 (±0.1), 2.0 (0.0; 9.0) | 6.4 (±0.0), 5.0 (1.0; 11.0) | <0.001 |
| Proportion of Age groups | <0.001 | ||
| 0 | 38.6%; n = 555 | 17.5%; n = 2240 | |
| 1–4 | 21.3%; n = 307 | 29.9%; n = 3829 | |
| 5–9 | 15.3%; n = 220 | 21.8%; n = 2796 | |
| 10–14 | 15.0%; n = 216 | 17.5%; n = 2242 | |
| 15–17 | 9.8%; n = 141 | 13.3%; n = 1702 | |
| Type of surgery | |||
| Proportion of surgery groups | <0.001 | ||
| Dermatology, Ophthalmology | 3.4%; n = 49 | 12.2%; n = 1567 | |
| Neurosurgery | 10.0%; n = 144 | 3.1%; n = 401 | |
| Otorhinolaryngology | 1.3%; n = 19 | 32.0%; n = 4096 | |
| Thoracic surgery | 0.7%; n = 10 | 0.4%; n = 55 | |
| Cardiac surgery | 2.0%; n = 29 | 0.3%; n = 44 | |
| Vascular surgery | 16.5%; n = 238 | 5.4%; n = 697 | |
| Visceral and endocrine surgery | 18.7%; n = 269 | 12.7%; n = 1621 | |
| Urology | 1.0%; n = 15 | 6.2%; n = 796 | |
| Gynaecology | 0.3%; n = 5 | 0.7%; n = 84 | |
| Obstetric | 0.1%; n = 1 | 0.4%; n = 52 | |
| Oral-maxillofacial surgery | 0.0%; n = 0 | 1.4%; n = 178 | |
| Trauma and orthopaedic surgery | 1.3%; n = 18 | 11.0%; n = 1403 | |
| Haematopoietic and lymphatic system | 18.8%; n = 271 | 1.5%; n = 194 | |
| Mixed group | 25.8%; n = 371 | 12.7%; n = 1621 |
| Risk Factor | Univariate Analysis | Multivariate Analysis |
|---|---|---|
| p-Value | p-Value; OR (with 95% CI) | |
| Gender | <0.001 | p = 0.036; OR = 1.19 (1.01–1.39) (female compared to male) |
| Age (years) 0 1–4 5–9 10–14 15–17 | <0.001 | (all compared to age 0) p < 0.001; OR = 0.28 (0.20–0.38) p < 0.001; OR = 0.21 (0.15–0.30) p < 0.001; OR = 0.18 (0.13–0.26) p < 0.001; OR = 0.14 (0.10–0.21) |
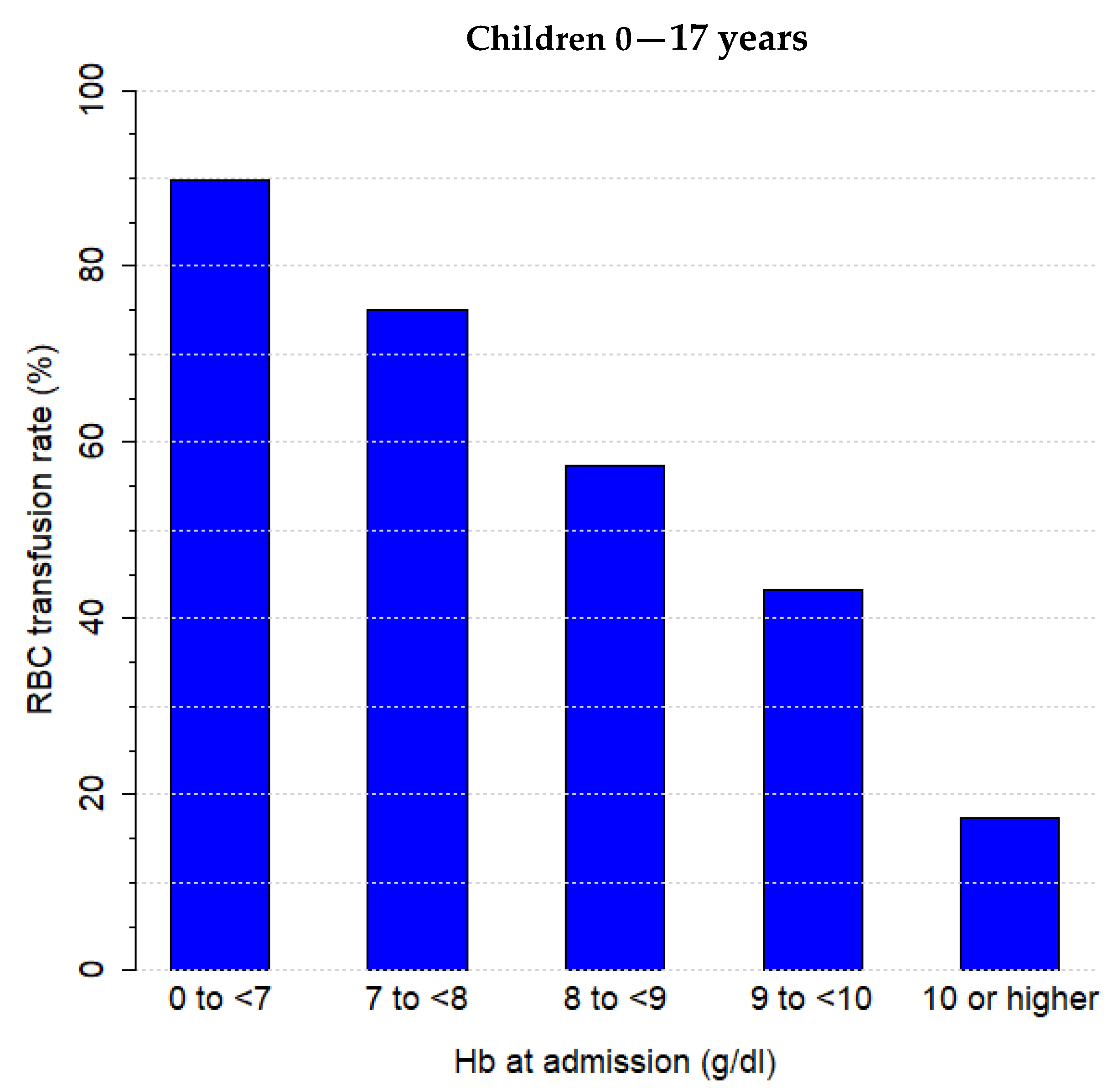
| Anaemia at admission Anaemia No anaemia Unknown 1 | <0.001 | p < 0.001; OR = 15.10 (11.58–19.90) p < 0.001; OR = 2.40 (1.76–3.30) (all compared to unknown) |
| Type of surgery Dermatology, Ophthalmology Neurosurgery Otorhinolaryngology Thoracic surgery Cardiac surgery Vascular surgery Visceral and endocrine surgery Urology Gynaecology Obstetric Oral-maxillofacial surgery Trauma and orthopaedic surgery Haematopoietic and lymphatic system Mixed group | <0.001 | (all compared to Derm. and Oph.) p < 0.001; OR = 10.14 (6.48–16.19) p < 0.001; OR = 0.29 (0.15–0.53) p = 0.598; OR = 1.31 (0.46–3.36) p < 0.001; OR = 4.79 (2.05–11.04) p < 0.001; OR = 9.93 (6.48–15.59) p < 0.001; OR = 2.48 (1.64–3.83) p = 0.676; OR = 1.17 (0.55–2.35) p = 0.014; OR = 3.64 (1.16–9.51) p = 0.559; OR = 0.55 (0.03–2.71) p = 0.963; OR = 0.00 (0.00–0.00) p = 0.669; OR = 1.15 (0.60–2.13) p < 0.001; OR = 36.98 (23.51–59.41) p < 0.001; OR = 5.86 (3.91–8.99) |
| Sepsis/SIRS 2 | <0.001 | p < 0.001; OR = 10.16 (6.98–15.07) |
| Respiratory dysfunction | <0.001 | p < 0.001; OR = 7.56 (6.01–9.52) |
| Cardiovascular dysfunction | <0.001 | p < 0.001; OR = 4.68 (3.43–6.40) |
| Neurological dysfunction | <0.001 | p = 0.029, OR = 1.77 (1.06–2.97) |
| Renal dysfunction | <0.001 | p < 0.001; OR = 16.17 (8.33–33.55) |
| Hepatic dysfunction | <0.001 | p = 0.988; OR = 5.58 × 106 (0.00–∞) 3 |
| Hb Values and Transfusion Rates | RBC-Transfusion n (%) 1439 (10.1%) | Non-RBC-Transfusion n (%) 12,809 (89.9%) | p-Value |
|---|---|---|---|
| Hb value at admission (g/dL) | 10.9 (±0.1), 10.3 (8.4; 12.7) | 12.6 (±0.0), 12.5 (11.1; 13.7) | <0.001 |
| Anaemia rate at admission | 82.4% (79.6–85.0%); n = 661 | 29.6% (28.0–31.2%); n = 963 | <0.001 |
| Proportion of anaemia groups at admission | <0.001 | ||
| Anaemia at admission (%) | 45.9%; n = 661 | 7.5%; n = 963 | |
| No anaemia at admission (%) | 9.8%; n = 141 | 17.9%; n = 2291 | |
| Unknown anaemia status at admission 1 | 44.3%; n = 637 | 74.6%; n = 9555 | |
| Hb value at discharge (g/dL) | 10.1 (±0.1), 9.8 (8.7; 11.3) | 12.3 (±0.0), 12.3 (11.2; 13.3) | <0.001 |
| Anaemia rate at discharge | 87.9% (85.4–90.1%); n = 711 | 25.6% (24.4–26.8%); n = 1393 | <0.001 |
| Proportion of anaemia groups at discharge | <0.001 | ||
| Anaemia at discharge | 49.4%; n = 711 | 10.9%; n = 1393 | |
| No anaemia at discharge | 6.8%; n = 98 | 31.6%; n = 4052 | |
| Unknown anaemia status at discharge | 43.8%; n = 630 | 57.5%; n = 7364 | |
| Platelet transfusion rate | 47.9% (45.3–50.6%); n = 690 | 0.7% (0.5–0.8%); n = 87 | <0.001 |
| FFP 2 transfusion rate | 30.6% (28.2–33.0%); n = 440 | 0.4% (0.3–0.5%); n = 45 | <0.001 |
| Fibrinogen transfusion rate | 3.3% (2.4–4.3%); n = 47 | 0.0% (0.0–0.1%); n = 5 | <0.001 |
| PCC 3 transfusion rate | 3.3% (2.4–4.3%); n = 47 | 0.1% (0.1–0.2%); n = 19 | <0.001 |
| Complications | RBC-Transfusion n (%) 1439 (10.1%) | Non-RBC-Transfusion n (%) 12,809 (89.9%) | p-Value |
|---|---|---|---|
| Sepsis/SIRS 1 | 23.6% (21.4–25.8%); n = 339 | 0.4% (0.3–0.5%); n = 45 | <0.001 |
| Respiratory dysfunction | 41.2% (38.7–43.8%); n = 593 | 2.7% (2.4–3.0%); n = 342 | <0.001 |
| Cardiovascular dysfunction | 24.5% (22.3–26.8%); n = 353 | 1.0% (0.9–1.2%); n = 132 | <0.001 |
| Neurological dysfunction | 4.8% (3.7–6.0%); n = 69 | 0.5% (0.3–0.6%); n = 58 | <0.001 |
| Renal dysfunction | 11.7% (10.1–13.4%); n = 168 | 0.1% (0.1–0.2%); n = 14 | <0.001 |
| Hepatic dysfunction | 0.6% (0.2–1.1%); n = 8 | 0.0% (0.0–0.0%); n = 0 | <0.001 |
| Mortality | 7.1% (5.8–8.5%); n = 102 | 0.1% (0.0–0.1%); n = 9 | <0.001 |
| Hospital LOS 2 (days) | 42.0 (± 1.1), 32.0 (13.0; 53.0) | 4.4 (± 0.1), 2.0 (1.0; 4.0) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Piekarski, F.; Neef, V.; Meybohm, P.; Rolle, U.; Schneider, W.; Zacharowski, K.; Schmitt, E. Independent Risk Factors for RBC Transfusion in Children Undergoing Surgery. Analysis of 14,248 Cases at a German University Hospital. Children 2021, 8, 634. https://0-doi-org.brum.beds.ac.uk/10.3390/children8080634
Piekarski F, Neef V, Meybohm P, Rolle U, Schneider W, Zacharowski K, Schmitt E. Independent Risk Factors for RBC Transfusion in Children Undergoing Surgery. Analysis of 14,248 Cases at a German University Hospital. Children. 2021; 8(8):634. https://0-doi-org.brum.beds.ac.uk/10.3390/children8080634
Chicago/Turabian StylePiekarski, Florian, Vanessa Neef, Patrick Meybohm, Udo Rolle, Wilfried Schneider, Kai Zacharowski, and Elke Schmitt. 2021. "Independent Risk Factors for RBC Transfusion in Children Undergoing Surgery. Analysis of 14,248 Cases at a German University Hospital" Children 8, no. 8: 634. https://0-doi-org.brum.beds.ac.uk/10.3390/children8080634