
The Safety and Effectiveness of Laparoscopic Pyloromyotomy Using 3-mm Electrocautery Hook versus Open Surgery for Treatment of Hypertrophic Pyloric Stenosis in Infants




Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Outcomes of the Study
2.3. Study Design
2.4. Surgical Technique
2.4.1. Open Pyloromyotomy
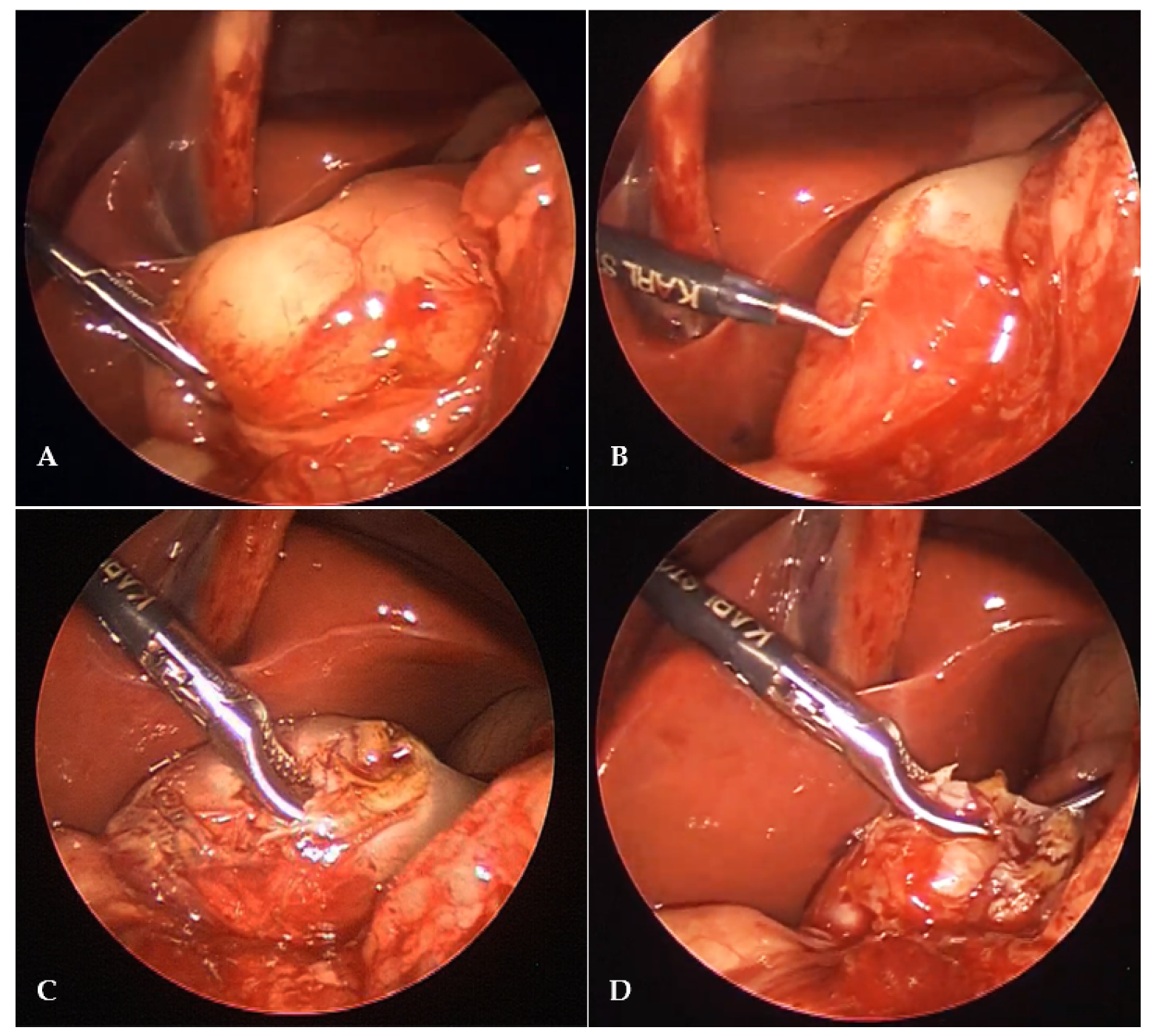
2.4.2. Laparoscopic Pyloromyotomy
2.5. Postoperative Protocol and Follow-Up
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Galea, R.; Said, E. Infantile hypertrophic pyloric stenosis: An epidemiological review. Neonatal. Netw. 2018, 37, 197–204. [Google Scholar]
- Abdellatif, M.; Ghozy, S.; Kamel, M.G.; Elawady, S.S.; Ghorab, M.M.E.; Attia, A.W.; Le Huyen, T.T.; Duy, D.T.V.; Hirayama, K.; Huy, N.T. Association between exposure to macrolides and the development of infantile hypertrophic pyloric stenosis: A systematic review and meta-analysis. Eur. J. Pediatr. 2019, 178, 301–314. [Google Scholar]
- Zhu, J.; Zhu, T.; Lin, Z.; Qu, Y.; Mu, D. Perinatal risk factors for infantile hypertrophic pyloric stenosis: A meta-analysis. J. Pediatr. Surg. 2017, 52, 1389–1397. [Google Scholar] [CrossRef]
- van den Bunder, F.A.I.M.; Allema, J.H.; Benninga, M.A.; de Blaauw, I.; van de Brug, T.; den Dulk, M.; Hulscher, J.B.F.; Keyzer-Dekker, C.M.G.; Witvliet, M.J.; van Heurn, E.L.W.; et al. The Dutch incidence of infantile hypertrophic pyloric stenosis and the influence of seasons. Eur. J. Pediatr. Surg. 2020. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Čagalj, I.Č.; Žitko, V.; Nevešćanin, A.; Krželj, V. Late-onset hypertrophic pyloric stenosis in a 14-weeks-old full term male infant. Acta Med. 2019, 62, 82–84. [Google Scholar] [CrossRef] [Green Version]
- Zampieri, N.; Corato, V.; Scirè, G.; Camoglio, F.S. Hypertrophic pyloric stenosis: 10 years’ experience with standard open and laparoscopic approach. Pediatr. Gastroenterol. Hepatol. Nutr. 2021, 24, 265–272. [Google Scholar] [CrossRef]
- Dalton, B.G.; Gonzalez, K.W.; Boda, S.R.; Thomas, P.G.; Sherman, A.K.; Peter, S.D.S. Optimizing fluid resuscitation in hypertrophic pyloric stenosis. J. Pediatr. Surg. 2016, 51, 1279–1282. [Google Scholar] [CrossRef]
- Tutay, G.J.; Capraro, G.; Spirko, B.; Garb, J.; Smithline, H. Electrolyte profile of pediatric patients with hypertrophic pyloric stenosis. Pediatr. Emerg. Care 2013, 29, 465–468. [Google Scholar] [CrossRef] [Green Version]
- Hussain, M. Sonographic diagnosis of infantile hypertrophic pyloric stenosis- use of simultaneous grey-scale & coour doppler examination. Int. J. Health Sci. 2008, 2, 134–140. [Google Scholar]
- Calle-Toro, J.S.; Kaplan, S.L.; Andronikou, S. Are we performing ultrasound measurements of the wall thickness in hypertrophic pyloric stenosis studies the same way? Pediatr. Surg. Int. 2020, 36, 399–405. [Google Scholar] [CrossRef]
- El-Gohary, Y.; Abdelhafeez, A.; Paton, E.; Gosain, A.; Murphy, A.J. Pyloric stenosis: An enigma more than a century after the first successful treatment. Pediatr. Surg. Int. 2018, 34, 21–27. [Google Scholar] [CrossRef]
- Ono, S.; Takenouchi, A.; Terui, K.; Yoshida, H.; Terui, E. Risk factors for unsuccessful atropine therapy in hypertrophic pyloric stenosis. Pediatr. Int. 2019, 61, 1151–1154. [Google Scholar] [CrossRef]
- Kawahara, H.; Takama, Y.; Yoshida, H.; Nakai, H.; Okuyama, H.; Kubota, A.; Yoshimura, N.; Ida, S.; Okada, A. Medical treatment of infantile hypertrophic pyloric stenosis: Should we always slice the “olive”? J. Pediatr. Surg. 2005, 40, 1848–1851. [Google Scholar] [CrossRef]
- Takeuchi, M.; Yasunaga, H.; Horiguchi, H.; Hashimoto, H.; Matsuda, S. Pyloromyotomy versus i.v. atropine therapy for the treatment of infantile pyloric stenosis: Nationwide hospital discharge database analysis. Pediatr. Int. 2013, 55, 488–491. [Google Scholar] [CrossRef]
- Huang, W.H.; Zhang, Q.L.; Chen, L.; Cui, X.; Wang, Y.J.; Zhou, C.M. The safety and effectiveness of laparoscopic versus open surgery for congenital hypertrophic pyloric stenosis in infants. Med. Sci. Monit. 2020, 26. [Google Scholar] [CrossRef]
- Sathya, C.; Wayne, C.; Gotsch, A.; Vincent, J.; Sullivan, K.J.; Nasr, A. Laparoscopic versus open pyloromyotomy in infants: A systematic review and meta-analysis. Pediatr. Surg. Int. 2017, 33, 325–333. [Google Scholar] [CrossRef]
- Costanzo, C.M.; Vinocur, C.; Berman, L. Postoperative outcomes of open versus laparoscopic pyloromyotomy for hypertrophic pyloric stenosis. J. Surg. Res. 2018, 224, 240–244. [Google Scholar] [CrossRef]
- Oomen, M.W.; Hoekstra, L.T.; Bakx, R.; Ubbink, D.T.; Heij, H.A. Open versus laparoscopic pyloromyotomy for hypertrophic pyloric stenosis: A systematic review and meta-analysis focusing on major complications. Surg. Endosc. 2012, 26, 2104–2110. [Google Scholar] [CrossRef] [Green Version]
- Shah, A.A.; Shah, A.V. Laparoscopic pyloromyotomy using an indigenous endoknife. J. Indian Assoc. Pediatr. Surg. 2004, 9, 46–47. [Google Scholar]
- Ramji, J.; Joshi, R.S. Laparoscopic pyloromyotomy for congenital hypertrophic pyloric stenosis: Our experience with twenty cases. Afr. J. Paediatr. Surg. 2021, 18, 14–17. [Google Scholar] [CrossRef]
- Abu-Kishk, I.; Stolero, S.; Klin, B.; Lotan, G. Myringotomy knife for pyloromyotomy. Surg. Laparosc. Endosc. Percutan. Tech. 2010, 20, e47–e49. [Google Scholar] [CrossRef]
- Jain, V.; Choudhury, S.R.; Chadha, R.; Puri, A.; Naga, A.S. Laparoscopic pyloromyotomy: Is a knife really necessary? World J. Pediatr. 2012, 8, 57–60. [Google Scholar] [CrossRef]
- Lauriti, G.; Cascini, V.; Chiesa, P.L.; Pierro, A.; Zani, A. Atropine treatment for hypertrophic pyloric stenosis: A systematic review and meta-analysis. Eur. J. Pediatr. Surg. 2018, 28, 393–399. [Google Scholar] [CrossRef]
- Ramstedt, C. Zur operation der angeborenen pylorus stenose. Med. Klin. 1912, 8, 1702–1705. [Google Scholar]
- Pogorelić, Z.; Huskić, D.; Čohadžić, T.; Jukić, M.; Šušnjar, T. Learning curve for laparoscopic repair of pediatric inguinal hernia using percutaneous internal ring suturing. Children 2021, 8, 294. [Google Scholar] [CrossRef]
- Jukic, M.; Todoric, M.; Todoric, J.; Susnjar, T.; Pogorelic, Z. Laparoscopic versus open high ligation for adolescent varicocele: A 6-year single center study. Indian Pediatr. 2019, 56, 653–658. [Google Scholar]
- Mihanović, J.; Šikić, N.L.; Mrklić, I.; Katušić, Z.; Karlo, R.; Jukić, M.; Jerončić, A.; Pogorelić, Z. Comparison of new versus reused Harmonic scalpel performance in laparoscopic appendectomy in patients with acute appendicitis-a randomized clinical trial. Langenbecks Arch. Surg. 2021, 406, 153–162. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Aralica, M.; Jukić, M.; Žitko, V.; Despot, R.; Jurić, I. Gallbladder disease in children: A 20-year single-center experience. Indian Pediatr. 2019, 56, 384–386. [Google Scholar]
- Ismail, I.; Elsherbini, R.; Elsaied, A.; Aly, K.; Sheir, H. Laparoscopic vs. open pyloromyotomy in treatment of infantile hypertrophic pyloric stenosis. Front. Pediatr. 2020, 8, 426. [Google Scholar] [CrossRef]
- Peter, S.D.S.; Holcomb, G.W., 3rd; Calkins, C.M.; Murphy, J.P.; Andrews, W.S.; Sharp, R.J.; Snyder, C.L.; Ostlie, D.J. Open versus laparoscopic pyloromyotomy for pyloric stenosis: A prospective, randomized trial. Ann. Surg. 2006, 244, 363–370. [Google Scholar] [CrossRef]
- Kim, S.S.; Lau, S.T.; Lee, S.L.; Schaller, R., Jr.; Healey, P.J.; Ledbetter, D.J.; Sawin, R.S.; Waldhausen, J.H. Pyloromyotomy: A comparison of laparoscopic, circumumbilical, and right upper quadrant operative techniques. J. Am. Coll. Surg. 2005, 201, 66–70. [Google Scholar]
- Mahida, J.B.; Asti, L.; Deans, K.J.; Minneci, P.C.; Groner, J.I. Laparoscopic pyloromyotomy decreases postoperative length of stay in children with hypertrophic pyloric stenosis. J. Pediatr. Surg. 2016, 51, 1436–1439. [Google Scholar] [CrossRef]
- Staerkle, R.F.; Lunger, F.; Fink, L.; Sasse, T.; Lacher, M.; von Elm, E.; Marwan, A.I.; Holland-Cunz, S.; Vuille-Dit-Bille, R.N. Open versus laparoscopic pyloromyotomy for pyloric stenosis. Cochrane Database Syst. Rev. 2021, 3, CD012827. [Google Scholar] [CrossRef]
- Saha, N.; Saha, D.K.; Rahman, M.A.; Aziz, M.A.; Islam, M.K. Laparoscopic versus open pyloromyotomy for infantile hypertropic pyloric stenosis: An early experience. Mymensingh. Med. J. 2012, 21, 430–434. [Google Scholar]
- Kethman, W.C.; Harris, A.H.S.; Hawn, M.T.; Wall, J.K. Trends and surgical outcomes of laparoscopic versus open pyloromyotomy. Surg. Endosc. 2018, 32, 3380–3385. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Perko, Z.; Druzijanić, N.; Tomić, S.; Mrklić, I. How to prevent lateral thermal damage to tissue using the harmonic scalpel: Experimental study on pig small intestine and abdominal wall. Eur. Surg. Res. 2009, 43, 235–240. [Google Scholar] [CrossRef]
- Družijanić, N.; Pogorelić, Z.; Perko, Z.; Mrklić, I.; Tomić, S. Comparison of lateral thermal damage of the human peritoneum using monopolar diathermy, Harmonic scalpel and LigaSure. Can. J. Surg. 2012, 55, 317–321. [Google Scholar] [CrossRef] [Green Version]
- Perko, Z.; Pogorelić, Z.; Bilan, K.; Tomić, S.; Vilović, K.; Krnić, D.; Druzijanić, N.; Kraljević, D.; Juricić, J. Lateral thermal damage to rat abdominal wall after harmonic scalpel application. Surg. Endosc. 2006, 20, 322–324. [Google Scholar] [CrossRef]
- Pogorelić, Z.; Katić, J.; Mrklić, I.; Jerončić, A.; Šušnjar, T.; Jukić, M.; Vilović, K.; Perko, Z. Lateral thermal damage of mesoappendix and appendiceal base during laparoscopic appendectomy in children: Comparison of the harmonic scalpel (Ultracision), bipolar coagulation (LigaSure), and thermal fusion technology (MiSeal). J. Surg. Res. 2017, 212, 101–107. [Google Scholar] [CrossRef]
- Bulat, C.; Pešutić-Pisac, V.; Capkun, V.; Marović, Z.; Pogorelić, Z.; Družijanić, N. Comparison of thermal damage of the internal thoracic artery using ultra high radiofrequency and monopolar diathermy. Surgeon 2014, 12, 249–255. [Google Scholar] [CrossRef]


{kind=link}
| Group I Open Pyloromyotomy (n = 61) | Group II Laparoscopic Pyloromyotomy (n = 64) | p | |
|---|---|---|---|
| Demographic characteristics of patients | |||
| Age (days) | 34 | 31 | 0.453 * |
| median (IQR) | (23.5, 46) | (24, 38) | |
| Gender, n (%) | 0.570 † | ||
| Male | 50 (82) | 54 (85.7) | |
| Female | 11 (18) | 9 (14.3) | |
| Weight (g) | 3 700 | 3 800 | 0.226 * |
| median (IQR) | (3525, 4240) | (3030, 4025) | |
| Malnutrition, n (%) | 16 (26.2) | 11 (17.8) | 0.255 † |
| Associated anomalies, n (%) | 5 (8.9) | 6 (10.3) | 1.000 ‡ |
| Laboratory data of patients | |||
| Hypokalemia, n (%) | 13 (21.6) | 18 (29) | 0.350 † |
| Hypochloremia, n (%) | 24 (39.3) | 24 (37.5) | 0.316 † |
| Metabolic alkalosis, n (%) | 54 (88.5) | 55 (85.9) | 0.974 † |
| Ultrasound findings of patients | |||
| Ultrasound—wall thickness (mm) median (IQR) | 5.5 (5, 5.8) | 5.2 (4.8, 6) | 0.260 * |
| Ultrasound—length of pyloric canal (mm); median (IQR) | 19 (18, 21.5) | 19 (18, 21) | 0.857 * |
| Ultrasound—diameter of pylorus (mm); median (IQR) | 17 (15, 18) | 18 (16, 18.5) | 0.441 * |
| Group I Open Pyloromyotomy | Group II Laparoscopic Pyloromyotomy | p | |
|---|---|---|---|
| (n = 61) | (n = 64) | ||
| Surgical time (min) | 45 | 35 | 0.00008 * |
| median (IQR) | (40, 57.5) | (30, 45) | |
| Time to oral intake (min) | 22 | 6 | <0.00001 * |
| median (IQR) | (13.5, 24) | (4, 8) | |
| Postoperative vomiting, n (%) | 19 (31.1) | 10 (15.6) | 0.039 † |
| Length of hospital stay (days) | 6 | 3 | <0.00001 * |
| median (IQR) | (4.5, 8) | (2, 3) | |
| Complications, n (%) | 6 (9.8) | 2 (3.1) | 0.157 ‡ |
| Perforation of mucosa | 3 (4.9) | 2 (3.1) | |
| Wound infection | 3 (4.9) | 0 (0) | |
| Reoperations, n (%) | 3 (4.9) | 0 (0) | 0.113 ‡ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pogorelić, Z.; Zelić, A.; Jukić, M.; Llorente Muñoz, C.M. The Safety and Effectiveness of Laparoscopic Pyloromyotomy Using 3-mm Electrocautery Hook versus Open Surgery for Treatment of Hypertrophic Pyloric Stenosis in Infants. Children 2021, 8, 701. https://0-doi-org.brum.beds.ac.uk/10.3390/children8080701
Pogorelić Z, Zelić A, Jukić M, Llorente Muñoz CM. The Safety and Effectiveness of Laparoscopic Pyloromyotomy Using 3-mm Electrocautery Hook versus Open Surgery for Treatment of Hypertrophic Pyloric Stenosis in Infants. Children. 2021; 8(8):701. https://0-doi-org.brum.beds.ac.uk/10.3390/children8080701
Chicago/Turabian StylePogorelić, Zenon, Ana Zelić, Miro Jukić, and Carlos Martin Llorente Muñoz. 2021. "The Safety and Effectiveness of Laparoscopic Pyloromyotomy Using 3-mm Electrocautery Hook versus Open Surgery for Treatment of Hypertrophic Pyloric Stenosis in Infants" Children 8, no. 8: 701. https://0-doi-org.brum.beds.ac.uk/10.3390/children8080701