
Using Technology to Assess Bidirectionality between Daily Pain and Physical Activity: The Role of Marginalization during Emerging Adulthood

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Measures
2.3.1. Pain
2.3.2. Physical Activity
2.3.3. Marginalized Status
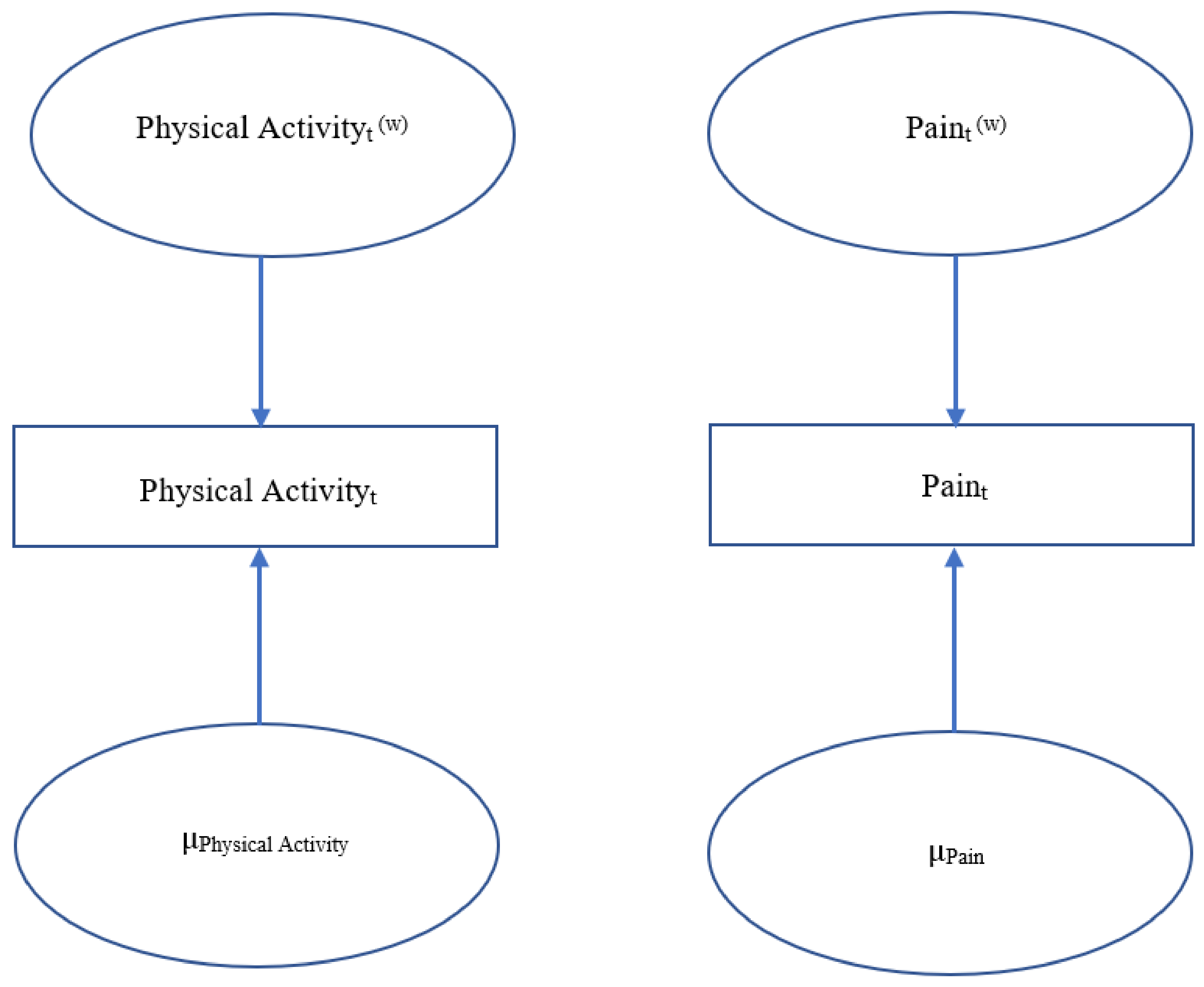
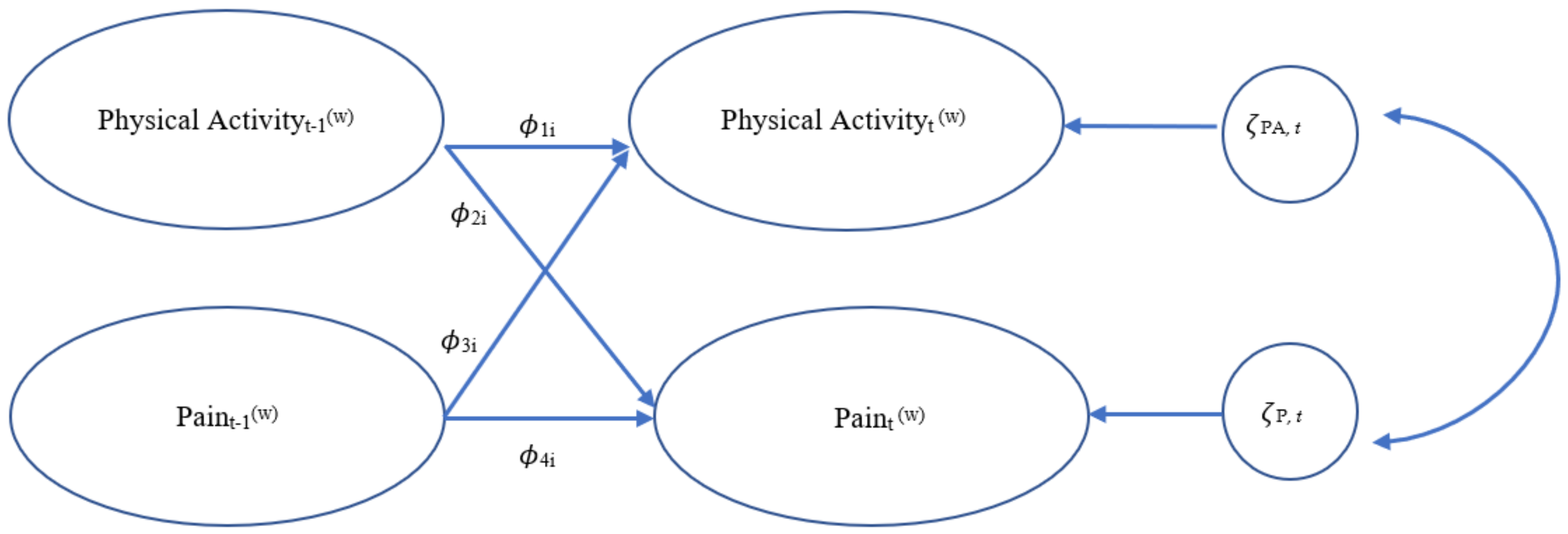
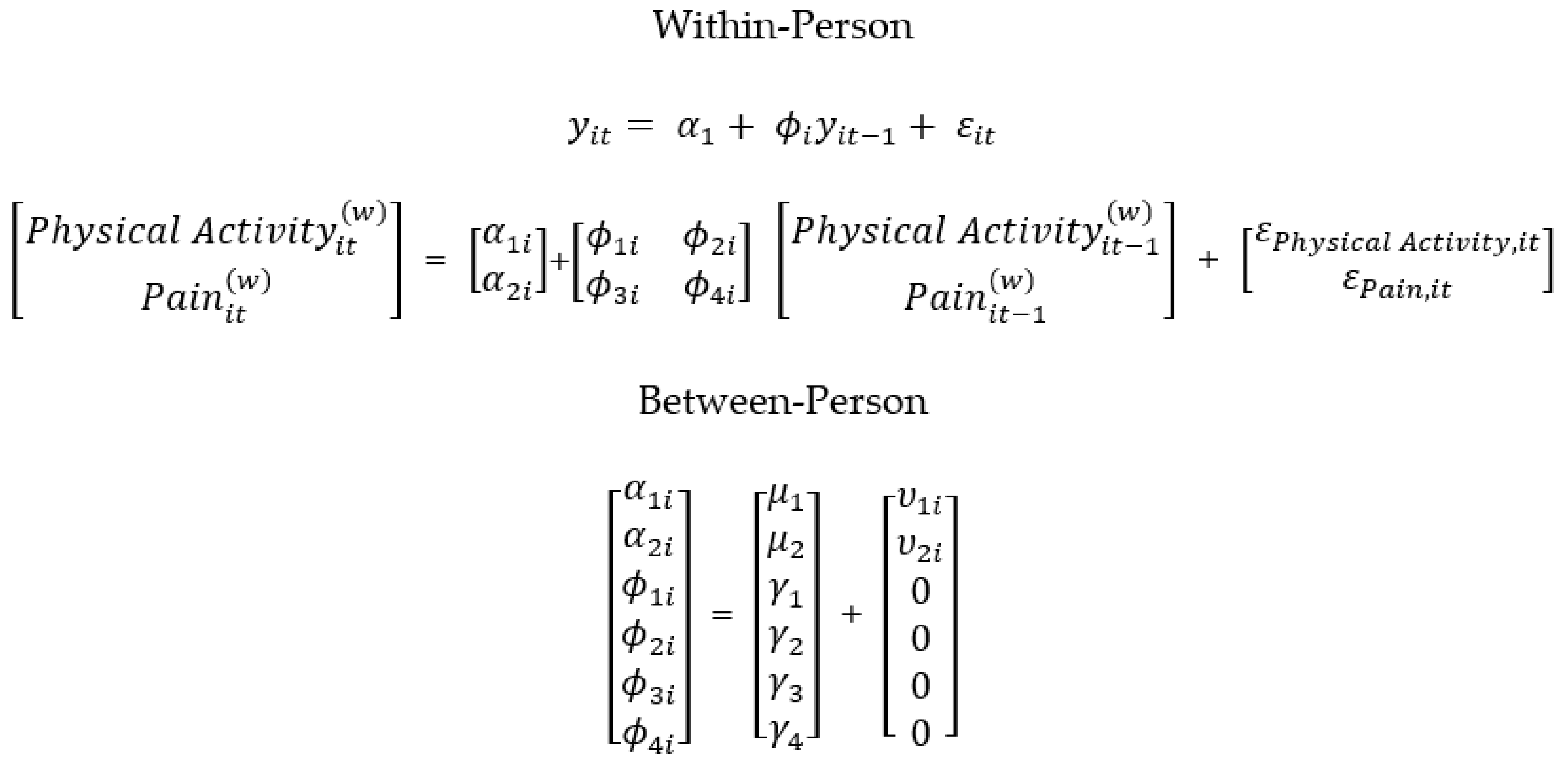
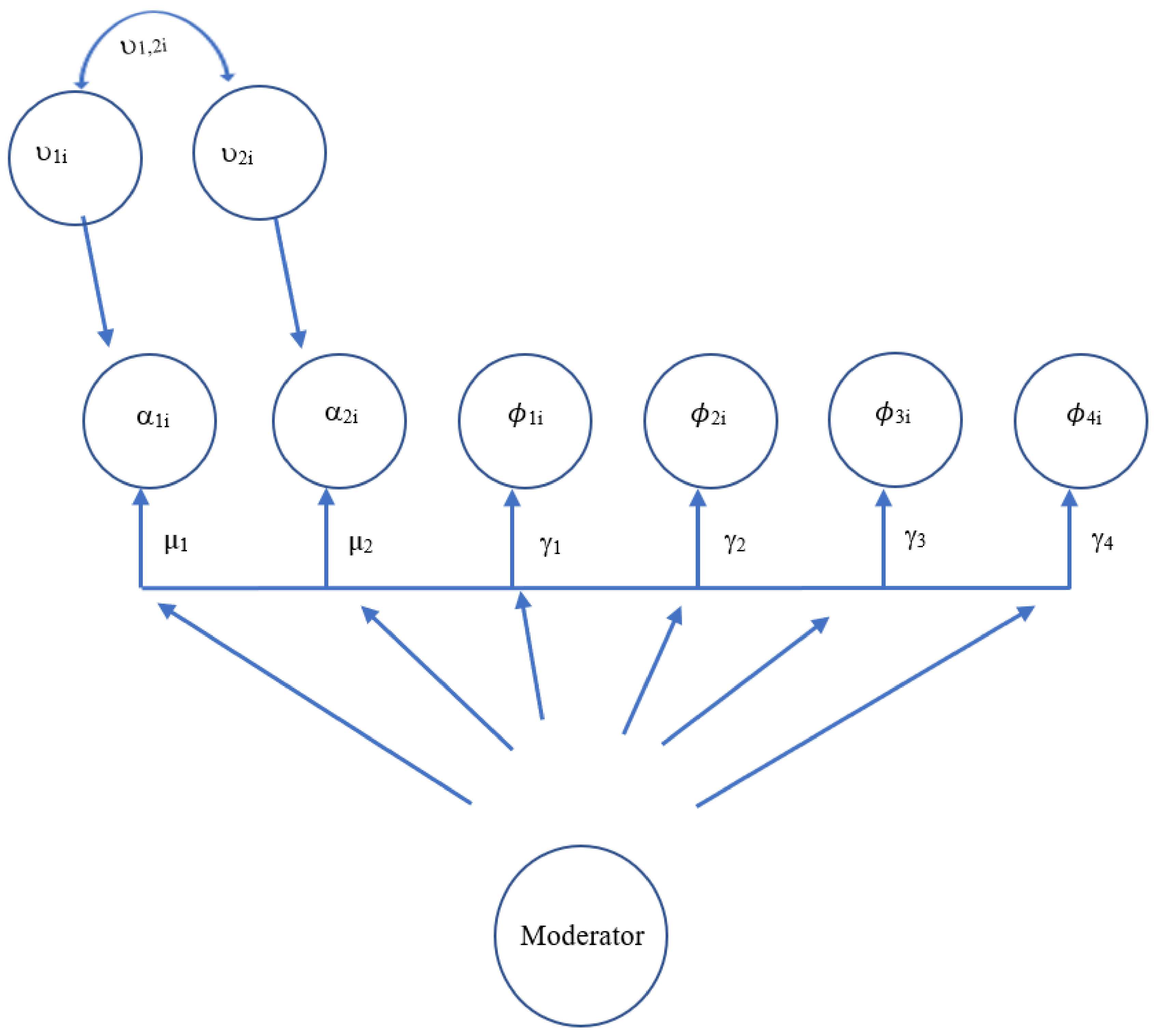
2.4. Statistical Analyses
Missing Data
3. Results
3.1. Descriptive Data
3.1.1. Pain
3.1.2. Physical Activity
3.2. Model Estimates
4. Discussion
4.1. Limitations and Future Directions
4.2. Strengths and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arnett, J.J. Emerging adulthood: A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef]
- Nelson, M.C.; Story, M.; Larson, N.I.; Neumark-Sztainer, D.; Lytle, L.A. Emerging Adulthood and College-aged Youth: An Overlooked Age for Weight-related Behavior Change. Obesity 2008, 16, 2205–2211. [Google Scholar] [CrossRef]
- Irwin, C.E. Young Adults Are Worse Off Than Adolescents. J. Adolesc. Health 2010, 46, 405–406. [Google Scholar] [CrossRef]
- Lester, N.; Lefebvre, J.C.; Keefe, F.J. Pain in young adults: I. Relationship to gender and family pain history. Clin. J. Pain. 1994, 10, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Heuscher, Z.; Gilkey, D.P.; Peel, J.L.; Kennedy, C.A. The Association of Self-Reported Backpack Use and Backpack Weight with Low Back Pain Among College Students. J. Manip. Physiol. Ther. 2010, 33, 432–437. [Google Scholar] [CrossRef] [PubMed]
- Gilkey, D.P.; Keefe, T.J.; Peel, J.L.; Kassab, O.M.; Kennedy, C.A. Risk Factors Associated With Back Pain: A Cross-Sectional Study of 963 College Students. J. Manip. Physiol. Ther. 2010, 33, 88–95. [Google Scholar] [CrossRef]
- Reis, J.; Flegel, M.; Kennedy, C. An Assessment of Lower Back Pain in Young Adults: Implications for College Health Education. J. Am. Coll. Health 1996, 44, 289–293. [Google Scholar] [CrossRef]
- Linet, M.S.; Stewart, W.F.; Celentano, D.D.; Ziegler, D.; Sprecher, M. An epidemiologic study of headache among adolescents and young adults. JAMA 1989, 261, 2211–2216. [Google Scholar] [CrossRef]
- Bigal, M.E.; Bigal, J.M.; Betti, M.; Bordini, C.A.; Speciali, J.G. Evaluation of the Impact of Migraine and Episodic Tension-type Headache on the Quality of Life and Performance of a University Student Population. Headache 2001, 41, 710–719. [Google Scholar] [CrossRef] [PubMed]
- Freburger, J.K.; Holmes, G.M.; Agans, R.P.; Jackman, A.M.; Darter, J.D.; Wallace, A.S.; Castel, L.D.; Kalsbeek, W.D.; Carey, T.S. The Rising Prevalence of Chronic Low Back Pain. Arch. Intern. Med. 2009, 169, 251–258. [Google Scholar] [CrossRef] [Green Version]
- Turk, D.C.; Fillingim, R.; Ohrbach, R.; Patel, K.V. Assessment of Psychosocial and Functional Impact of Chronic Pain. J. Pain 2016, 17, T21–T49. [Google Scholar] [CrossRef] [PubMed]
- Harris, G.R.; Susman, J.L. Managing musculoskeletal complaints with rehabilitation therapy: Summary of the Philadelphia Panel evidence-based clinical practice guidelines on musculoskeletal rehabilitation interventions. J. Fam. Pr. 2002, 51, 1042–1046. [Google Scholar]
- Koes, B.W.; van Tulder, M.; Lin, C.-W.C.; Macedo, L.; McAuley, J.; Maher, C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur. Spine J. 2010, 19, 2075–2094. [Google Scholar] [CrossRef] [Green Version]
- Hanney, W.J.; Kolber, M.J.; Beekhuizen, K.S. Implications for Physical Activity in the Population with Low Back Pain. Am. J. Lifestyle Med. 2008, 3, 63–70. [Google Scholar] [CrossRef]
- Fanucchi, G.L.; Stewart, A.; Jordaan, R.; Becker, P. Exercise reduces the intensity and prevalence of low back pain in 12–13 year old children: A randomised trial. Aust. J. Physiother. 2009, 55, 97–104. [Google Scholar] [CrossRef] [Green Version]
- Stephens, S.; Feldman, B.M.; Bradley, N.; Schneiderman, J.; Wright, F.V.; Singh-Grewal, D.; Lefebvre, A.; Benseler, S.M.; Cameron, B.; Laxer, R.; et al. Feasibility and effectiveness of an aerobic exercise program in children with fibromyalgia: Results of a randomized controlled pilot trial. Arthritis Rheum. 2008, 59, 1399–1406. [Google Scholar] [CrossRef] [PubMed]
- Landmark, T.; Romundstad, P.; Borchgrevink, P.C.; Kaasa, S.; Dale, O. Associations between recreational exercise and chronic pain in the general population: Evidence from the HUNT 3 study. Pain 2011, 152, 2241–2247. [Google Scholar] [CrossRef]
- American College Health Association. Canadian Reference Group Executive Summary, Spring 2013. Available online: http://www.cacuss.ca/health_data.htm (accessed on 2 March 2020).
- Yahia, N.; Wang, D.; Rapley, M.; Dey, R. Assessment of weight status, dietary habits and beliefs, physical activity, and nutritional knowledge among university students. Perspect. Public Health 2015, 136, 231–244. [Google Scholar] [CrossRef]
- Racette, S.B.; Deusinger, S.S.; Strube, M.J.; Highstein, G.R.; Deusinger, R.H. Changes in Weight and Health Behaviors from Freshman through Senior Year of College. J. Nutr. Educ. Behav. 2008, 40, 39–42. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Physical activity trends—United States, 1990–1998. J. Am. Med. Assoc. 2001, 50, 166–169. Available online: http://www.scotland.gov.uk/Topics/Statistics/Browse/Health/TrendPhysicalActivity (accessed on 2 March 2020).
- Bryant, L.L.; Grigsby, J.; Swenson, C.; Scarbro, S.; Baxter, J. Chronic Pain Increases the Risk of Decreasing Physical Performance in Older Adults: The San Luis Valley Health and Aging Study. 2007. Available online: https://0-academic-oup-com.brum.beds.ac.uk/biomedgerontology/article-abstract/62/9/989/525960 (accessed on 2 March 2021).
- Dansie, E.J.; Turk, D.C.; Martin, K.R.; Van Domelen, D.; Patel, K.V. Association of Chronic Widespread Pain with Objectively Measured Physical Activity in Adults: Findings from the National Health and Nutrition Examination Survey. J. Pain 2014, 15, 507–515. [Google Scholar] [CrossRef]
- Braveman, P.; Egerter, S.; Williams, D.R. The Social Determinants of Health: Coming of Age. Annu. Rev. Public Health 2011, 32, 381–398. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arcaya, M.C.; Arcaya, A.L.; Subramanian, S.V. Inequalities in health: Definitions, concepts, and theories. Rev. Panam. Salud Publica 2015, 38, 261–271. [Google Scholar] [CrossRef] [PubMed]
- Gagnon, C.M.; Matsuura, J.T.; Smith, C.C.; Stanos, S.P. Ethnicity and Interdisciplinary Pain Treatment. Pain Pr. 2013, 14, 532–540. [Google Scholar] [CrossRef]
- Green, C.R.; Anderson, K.O.; Baker, T.A.; Campbell, L.C.; Decker, S.; Fillingim, R.; Kaloukalani, D.A.; Lasch, K.E.; Myers, C.; Tait, R.C.; et al. The Unequal Burden of Pain: Confronting Racial and Ethnic Disparities in Pain. Pain Med. 2003, 4, 277–294. [Google Scholar] [CrossRef]
- Fillingim, R.B.; King, C.D.; Ribeiro-Dasilva, M.C.; Rahim-Williams, B.; Riley, J.L. Sex, Gender, and Pain: A Review of Recent Clinical and Experimental Findings. J. Pain 2009, 10, 447–485. [Google Scholar] [CrossRef] [Green Version]
- Lipton, R.B.; Munjal, S.; Alam, A.; Buse, D.C.; Fanning, K.M.; Reed, M.L.; Schwedt, T.J.; Dodick, D.W. Migraine in America Symptoms and Treatment (MAST) Study: Baseline Study Methods, Treatment Patterns, and Gender Differences. Headache 2018, 58, 1408–1426. [Google Scholar] [CrossRef] [PubMed]
- Unruh, A.M. Gender variations in clinical pain experience. Pain 1996, 65, 123–167. [Google Scholar] [CrossRef]
- Aggarwal, V.R.; Macfarlane, T.V.; Macfarlane, G.J. Why is pain more common amongst people living in areas of low socio-economic status? A population-based cross-sectional study. Br. Dent. J. 2003, 194, 383–387. [Google Scholar] [CrossRef]
- Andersson, H.I.; Ejlertsson, G.; Leden, I.; Rosenberg, C. Chronic pain in a geographically defined general population: Studies of differences in age, gender, social class, and pain localization. Clin. J. Pain 1993, 9, 174–182. [Google Scholar] [CrossRef]
- Fuentes, M.; Hart-Johnson, T.; Green, C.R. The association among neighborhood socioeconomic status, race and chronic pain in black and white older adults. J. Natl. Med. Assoc. 2007, 99, 1160–1169. [Google Scholar] [PubMed]
- Tran, S.T.; Koven, M.L.; Castro, A.S.; Arce, A.B.G.; Carter, J.S. Sociodemographic and Environmental Factors are Associated with Adolescents’ Pain and Longitudinal Health Outcomes. J. Pain 2020, 21, 170–181. [Google Scholar] [CrossRef]
- Mathieu, R.A.; Powell-Wiley, T.M.; Ayers, C.R.; McGuire, D.K.; Khera, A.; Das, S.R.; Lakoski, S.G. Physical activity participation, health perceptions, and cardiovascular disease mortality in a multiethnic population: The Dallas Heart Study. Am. Hear. J. 2012, 163, 1037–1040. [Google Scholar] [CrossRef] [Green Version]
- Huang, T.T.K.; Harris, K.J.; Lee, R.E.; Nazir, N.; Born, W.; Kaur, H. Assessing overweight, obesity, diet, and physical activity in college students. J. Am. Coll. Health 2003, 52, 83–86. [Google Scholar] [CrossRef] [PubMed]
- Nguyen-Michel, S.T.; Unger, J.B.; Hamilton, J.; Spruijt-Metz, D.; Spruijt-Metz, N. Associations between physical activity and perceived stress/hassles in college students. Stress Health 2006, 22, 179–188. [Google Scholar] [CrossRef]
- Van Kim, N.A.; Nelson, T. Vigorous Physical Activity, Mental Health, Perceived Stress, and Socializing among College Students. Am. J. Health Promot. 2013, 28, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Meyer, I.H. Prejudice, Social Stress, and Mental Health in Lesbian, Gay, and Bisexual Populations: Conceptual Issues and Research Evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef]
- Perrin, A. Social Media Usage: 2005–2015; Pew Research Center’s Internet & American Life Project: Washington, DC, USA, 2015; pp. 2005–2015. Available online: www.pewinternet.org/2015/10/08/social-networking-usage-2005-2015/ (accessed on 12 July 2021).
- Swanson, J.A.; Walker, E. Academic Versus Non-academic Emerging Adult College Student Technology Use. Technol. Knowl. Learn. 2015, 20, 147–158. [Google Scholar] [CrossRef]
- Scott, J.; Rowlands, A.; Cliff, D.; Morgan, P.J.; Plotnikoff, R.; Lubans, D.R. Comparability and feasibility of wrist- and hip-worn accelerometers in free-living adolescents. J. Sci. Med. Sport 2017, 20, 1101–1106. [Google Scholar] [CrossRef] [Green Version]
- Rabbitts, J.A.; Holley, A.L.; Karlson, C.W.; Palermo, T.M. Bidirectional Associations Between Pain and Physical Activity in Adolescents. Clin. J. Pain 2014, 30, 251–258. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. The PHQ-15: Validity of a New Measure for Evaluating the Severity of Somatic Symptoms. Psychosom. Med. 2002, 64, 258–266. [Google Scholar] [CrossRef] [Green Version]
- Sherbourne, C.D.; Asch, S.M.; Shugarman, L.R.; Goebel, J.; Lanto, A.B.; Rubenstein, L.V.; Wen, L.; Zubkoff, L.; Lorenz, K.A. Early Identification of Co-Occurring Pain, Depression and Anxiety. J. Gen. Intern. Med. 2009, 24, 620–625. [Google Scholar] [CrossRef] [Green Version]
- Muthén, B.O. How to get the ICC in DSEM. 2019. Available online: https://www.statmodel.com/download/ICCinDSEM.pdf (accessed on 14 July 2021).
- Freedson, P.S.; Melanson, E.; Sirard, J. Calibration of the Computer Science and Applications, Inc. accelerometer. Med. Sci. Sports Exerc. 1998, 30, 777–781. [Google Scholar] [CrossRef]
- Development of Planning and Development. Area Median Income (AMI) Chart. Available online: https://www.chicago.gov/city/en/depts/dcd/supp_info/area_median_incomeamichart.html (accessed on 12 July 2021).
- Hendricks, M.L.; Testa, R.J. A conceptual framework for clinical work with transgender and gender nonconforming clients: An adaptation of the Minority Stress Model. Prof. Psychol. Res. Pr. 2012, 43, 460–467. [Google Scholar] [CrossRef]
- Asparouhov, T.; Hamaker, E.L.; Muthén, B. Dynamic Structural Equation Models. Struct. Equ. Model. A Multidiscip. J. 2017, 25, 359–388. [Google Scholar] [CrossRef]
- Hamaker, E.L.; Asparouhov, T.; Brose, A.; Schmiedek, F.; Muthén, B. At the Frontiers of Modeling Intensive Longitudinal Data: Dynamic Structural Equation Models for the Affective Measurements from the COGITO Study. Multivar. Behav. Res. 2018, 53, 820–841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tran, S.T.; Grotkowski, K.; Miller, S.A.; Reed, B.W.; Koven, M.L.; Buscemi, J.; Greenley, R.N. Hassles predict physical health complaints in undergraduate students: A dynamic structural equation model analysis of daily diary data. Psychol. Health 2020, 828–846. [Google Scholar] [CrossRef]
- McNeish, D.; Hamaker, E.L. A primer on two-level dynamic structural equation models for intensive longitudinal data in Mplus. Psychol. Methods 2020, 25, 610–635. [Google Scholar] [CrossRef] [PubMed]
- U.S. Department of Health and Human Services. Physical Activity Guidelines for Americans, 2nd ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2018. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; MPlus: Los Angeles, CA, USA, 2017. [Google Scholar]
- Curry, K.; Green, R. Prevalence and management of headache in a university undergraduate population. J. Am. Acad. Nurse Pr. 2007, 19, 378–382. [Google Scholar] [CrossRef]
- Loprinzi, P.D.; Smith, B. Comparison Between Wrist-Worn and Waist-Worn Accelerometry. J. Phys. Act. Health 2017, 14, 539–545. [Google Scholar] [CrossRef]
- Hastie, B.A.; Riley, J.L.; Fillingim, R.B. Ethnic Differences and Responses to Pain in Healthy Young Adults. Pain Med. 2005, 6, 61–71. [Google Scholar] [CrossRef]
- Umeda, M.; Griffin, C.; Cross, A.; Heredia, C.; Okifuji, A. Conditioned pain modulation among young, healthy, and physically active African American and non-Hispanic White adults. J. Psychosom. Res. 2017, 98, 64–70. [Google Scholar] [CrossRef]
- Umeda, M.; Escobedo, T. Comparisons of Conditioned Pain Modulation and Physical Activity Between Hispanic and Non-Hispanic White Adults. J. Racial Ethn. Health Disparities 2018, 6, 472–480. [Google Scholar] [CrossRef]
- Bond, M.A. Leading the Way on Diversity: Community Psychology’s Evolution from Invisible to Individual to Contextual. Am. J. Community Psychol. 2016, 58, 259–268. [Google Scholar] [CrossRef]
- Wilson, A.C.; Palermo, T.M. Physical Activity and Function in Adolescents With Chronic Pain: A Controlled Study Using Actigraphy. J. Pain 2012, 13, 121–130. [Google Scholar] [CrossRef] [Green Version]
- Ellingson, L.D.; Shields, M.R.; Stegner, A.J.; Cook, D.B. Physical Activity, Sustained Sedentary Behavior, and Pain Modulation in Women with Fibromyalgia. J. Pain 2012, 13, 195–206. [Google Scholar] [CrossRef] [Green Version]
- Peterson, N.E.; Sirard, J.R.; Kulbok, P.A.; DeBoer, M.D.; Erickson, J.M. Sedentary behavior and physical activity of young adult university students. Res. Nurs. Health 2018, 41, 30–38. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n | % | ||
|---|---|---|---|
| Gender | |||
| Male | 76 | 28.68 | |
| Female | 183 | 69.06 | |
| Other/Gender Non-Conforming/Queer | 6 | 2.26 | |
| Race | |||
| White | 141 | 53.21 | |
| Black/African American | 17 | 6.42 | |
| American Indian/Alaskan Native | 1 | 0.38 | |
| Asian/Asian American | 60 | 22.64 | |
| Native Hawaiian/Pacific Islander | 1 | 0.38 | |
| Other | 45 | 16.98 | |
| Ethnicity | |||
| Hispanic | 62 | 23.40 | |
| Non Hispanic | 203 | 76.60 | |
| SES (Parent Income) | |||
| $0–$24,999 | 24 | 9.06 | |
| $25,000–$49,999 | 41 | 15.47 | |
| $50,000–$74,999 | 47 | 17.74 | |
| $75,000–$99,999 | 48 | 18.11 | |
| $100,000–$124,999 | 39 | 14.72 | |
| $125,000–$149,999 | 20 | 7.55 | |
| $150,000–$174,999 | 11 | 4.15 | |
| $175,000–$199,999 | 10 | 3.77 | |
| $200,000+ | 21 | 7.92 |
| Average Total Daily Pain | Average MVPA | ||
|---|---|---|---|
| M (SD) | M (SD) | ||
| Race | |||
| White | 1.33 (1.08) * | 217.69 (64.86) | |
| Person of Color | 0.95 (0.92) | 213.96 (56.77) | |
| Ethnicity | |||
| Hispanic | 1.17 (0.97) | 221.85 (52.02) | |
| Non Hispanic | 1.15 (1.04) | 214.16 (63.72) | |
| Gender | |||
| Male | 0.95 (0.90) * | 213.41 (63.64) | |
| Female | 1.25 (1.08) | 217.53 (60.05) | |
| SES (Parent Income) | |||
| $0–$49,999 | 1.19 (0.99) | 209.32 (59.43) | |
| $50,000+ | 1.14 (1.04) | 218.67 (62.02) |
| Level | Estimate | Standard Deviation | p Value (One-Tailed) | 95% Credibility Interval |
|---|---|---|---|---|
| Within | ||||
| Outcome: Pain | ||||
| Predictor: Paint−1 | 0.27 | 0.02 | <0.001 * | 0.23, 0.32 |
| Predictor: MVPAt−1 | 0.02 | 0.02 | 0.15 | −0.02, 0.06 |
| Outcome: MVPA | ||||
| Predictor: MVPAt−1 | 0.14 | 0.02 | <0.001 * | 0.10, 0.18 |
| Predictor: Paint−1 | −0.01 | 0.02 | 0.26 | −0.05, 0.03 |
| Covariance | −0.00 | 0.02 | 0.45 | −0.04, 0.04 |
| Residual Variances | ||||
| MVPA | 0.98 | 0.01 | <0.001 * | 0.97, 0.99 |
| Pain | 0.92 | 0.01 | <0.001 * | 0.90, 0.95 |
| Between | ||||
| Means | ||||
| MVPA | 3.86 | 0.22 | <0.001 * | 3.45, 4.31 |
| Pain | 1.26 | 0.10 | <0.001 * | 1.08, 1.47 |
| Variances | ||||
| MVPA | 1.00 | 0.00 | <0.001 | 1.00, 1.00 |
| Pain | 1.00 | 0.00 | <0.001 | 1.00, 1.00 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bedree, H.; Miller, S.A.; Buscemi, J.; Greenley, R.N.; Tran, S.T. Using Technology to Assess Bidirectionality between Daily Pain and Physical Activity: The Role of Marginalization during Emerging Adulthood. Children 2021, 8, 756. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090756
Bedree H, Miller SA, Buscemi J, Greenley RN, Tran ST. Using Technology to Assess Bidirectionality between Daily Pain and Physical Activity: The Role of Marginalization during Emerging Adulthood. Children. 2021; 8(9):756. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090756
Chicago/Turabian StyleBedree, Helen, Steven A. Miller, Joanna Buscemi, Rachel Neff Greenley, and Susan T. Tran. 2021. "Using Technology to Assess Bidirectionality between Daily Pain and Physical Activity: The Role of Marginalization during Emerging Adulthood" Children 8, no. 9: 756. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090756