
Comparison of Lower and Upper Quarter Y Balance Test Performance in Adolescent Students with Borderline Intellectual Functioning Compared to Age- and Sex-Matched Controls


Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Measurements
2.3. Anthropometry
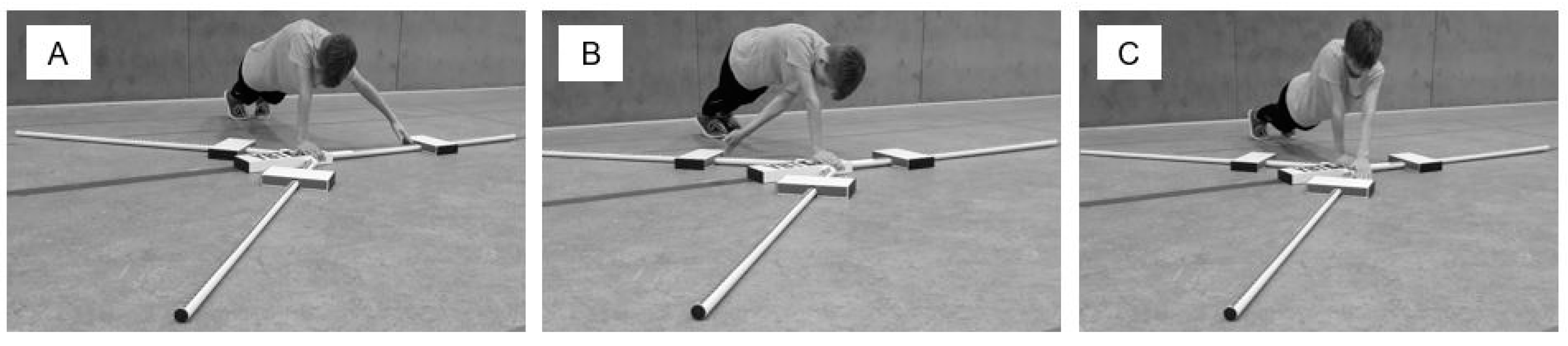
2.4. Y Balance Tests–General Execution Details
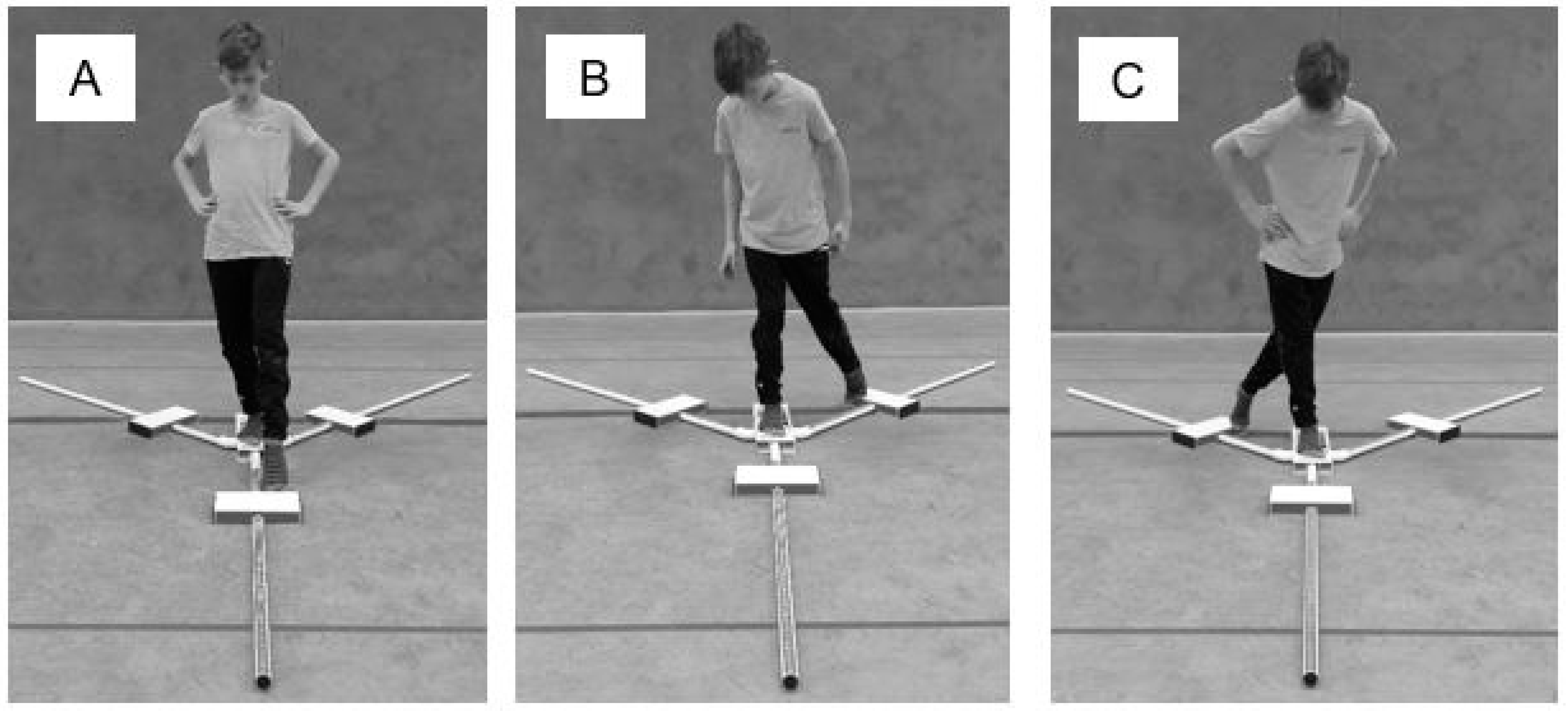
2.5. Lower Quarter Y Balance Test
2.6. Data and Statistical Analyses
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Wieland, J.; Zitman, F.G. It is time to bring borderline intellectual functioning back into the main fold of classification systems. BJPsych. Bull. 2016, 40, 204–206. [Google Scholar] [CrossRef] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, DSM-IV-TR; APA: Washington, DC, USA, 2000. [Google Scholar]
- Baglio, F.; Cabinio, M.; Ricci, C.; Baglio, G.; Lipari, S.; Griffanti, L.; Preti, M.G.; Nemni, R.; Clerici, M.; Zanette, M.; et al. Abnormal development of sensory-motor, visual temporal and parahippocampal cortex in children with learning disabilities and borderline intellectual functioning. Front. Hum. Neurosci. 2014, 8, 806. [Google Scholar] [CrossRef] [Green Version]
- Peltopuro, M.; Ahonen, T.; Kaartinen, J.; Seppala, H.; Narhi, V. Borderline intellectual functioning: A systematic literature review. Intellect. Dev. Disabil. 2014, 52, 419–443. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karande, S.; Kanchan, S.; Kulkarni, M. Clinical and psychoeducational profile of children with borderline intellectual functioning. Indian J. Pediatri. 2008, 75, 795–800. [Google Scholar] [CrossRef]
- Vuijk, P.J.; Hartman, E.; Scherder, E.; Visscher, C. Motor performance of children with mild intellectual disability and borderline intellectual functioning. J. Intellect. Disabil. Res. 2010, 54, 955–965. [Google Scholar] [CrossRef] [PubMed]
- Hassiotis, A.; Ukoumunne, O.; Tyrer, P.; Piachaud, J.; Gilvarry, C.; Harvey, K.; Fraser, J. Prevalence and characteristics of patients with severe mental illness and borderline intellectual functioning. Report from the UK700 randomised controlled trial of case management. Br. J. Psychiatry 1999, 175, 135–140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Piaget, J.; Inhelder, B. La Psychologie de L’enfant; Presses Universitaires de France: Paris, France, 1966. [Google Scholar]
- Diamond, A. Close interrelation of motor development and cognitive development and of the cerebellum and prefrontal cortex. Child Dev. 2000, 71, 44–56. [Google Scholar] [CrossRef]
- Kaupuzs, A.; Larins, V. Balance performance in children with borderline intellectual functioning and specific language impairment. Soc. Welf. Interdiscip. Approach 2017, 1, 132–141. [Google Scholar] [CrossRef] [Green Version]
- Alesi, M.; Battaglia, G.; Pepi, A.; Bianco, A.; Palma, A. Gross motor proficiency and intellectual functioning: A comparison among children with Down syndrome, children with borderline intellectual functioning, and typically developing children. Medicine 2018, 97, e12737. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Plisky, P.J. Y Balance Test Home Study Course. Available online: https://www.functionalmovement.com/articles/662/ybt_online-course/ (accessed on 20 July 2021).
- Plisky, P.J.; Gorman, P.P.; Butler, R.J.; Kiesel, K.B.; Underwood, F.B.; Elkins, B. The reliability of an instrumented device for measuring components of the star excursion balance test. N. Am. J. Sports Phys. Ther. 2009, 4, 92–99. [Google Scholar]
- Gorman, P.P.; Butler, R.J.; Plisky, P.J.; Kiesel, K.B. Upper Quarter Y Balance Test: Reliability and performance comparison between genders in active adults. J. Strength Cond. Res. 2012, 26, 3043–3048. [Google Scholar] [CrossRef]
- Schwiertz, G.; Beurskens, R.; Muehlbauer, T. Discriminative validity of the lower and upper quarter Y balance test performance: A comparison between healthy trained and untrained youth. BMC Sports Sci. Med. Rehabil. 2020, 12, 73. [Google Scholar] [CrossRef]
- Hartman, E.; Houwen, S.; Scherder, E.; Visscher, C. On the relationship between motor performance and executive functioning in children with intellectual disabilities. J. Intellect. Disabil. Res. 2010, 54, 468–477. [Google Scholar] [CrossRef]
- Westendorp, M.; Houwen, S.; Hartman, E.; Visscher, C. Are gross motor skills and sports participation related in children with intellectual disabilities? Res. Dev. Disabil. 2011, 32, 1147–1153. [Google Scholar] [CrossRef]
- Jeoung, B. Motor proficiency differences among students with intellectual disabilities, autism, and developmental disability. J. Exerc. Rehabil. 2018, 14, 275–281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilczyński, J.; Bieniek, K. Canonical correlations between somatic features and postural stability in children aged 10–12 years. Med. Stud. 2019, 35, 93–99. [Google Scholar] [CrossRef]
- Pena, G.M.; Pavão, S.L.; Oliveira, M.F.P.; Godoi, D.; de Campos, A.C.; Rocha, N.A.C.F. Dual-task effects on postural sway during sit-to-stand movement in children with Down syndrome. J. Intellect. Disabil. Res. 2019, 63, 576–586. [Google Scholar] [CrossRef]
- Carmel, I.E.; Bar-Yossef, T.; Ariav, C.; Paz, R.; Sabbag, H.; Levy, R. Sensorimotor impairments and strategies in adults with intellectual disabilities. Mot. Control 2008, 12, 348–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tyrer, F.; Dunkley, A.J.; Singh, J.; Kristunas, C.; Khunti, K.; Bhaumik, S.; Davies, M.J.; Yates, T.E.; Gray, L.J. Multimorbidity and lifestyle factors among adults with intellectual disabilities: A cross-sectional analysis of a UK cohort. J. Intellect. Disabil. Res. 2019, 63, 255–265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lahtinen, U.; Rintala, P.; Malin, A. Physical performance of individuals with intellectual disability: A 30-year follow-up. Adapt. Phys. Activ. Q. 2007, 24, 125–143. [Google Scholar] [CrossRef] [Green Version]
- Lipowicz, A.; Bugdol, M.N.; Szurmik, T.; Bibrowicz, K.; Kurzeja, P.; Mitas, A.W. Body balance analysis of children and youth with intellectual disabilities. J. Intellect. Disabil. Res. 2019, 63, 1312–1323. [Google Scholar] [CrossRef]
- Maïano, C.; Hue, O.; Morin, A.J.S.; Lepage, G.; Tracey, D.; Moullec, G. Exercise interventions to improve balance for young people with intellectual disabilities: A systematic review and meta-analysis. Dev. Med. Child Neurol. 2019, 61, 406–418. [Google Scholar] [CrossRef]
- Kapsal, N.J.; Dicke, T.; Morin, A.J.S.; Vasconcellos, D.; Maïano, C.; Lee, J.; Lonsdale, C. Effects of physical activity on the physical and psychosocial health of youth with Intellectual disabilities: A systematic review and meta-Analysis. J. Phys. Act. Health 2019, 16, 1187–1195. [Google Scholar] [CrossRef] [PubMed]
- Schwiertz, G.; Brueckner, D.; Schedler, S.; Kiss, R.; Muehlbauer, T. Performance and reliability of the Lower Quarter Y Balance Test in healthy adolescents from grade 6 to 11. Gait Posture 2018, 67, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Schwiertz, G.; Brueckner, D.; Schedler, S.; Kiss, R.; Muehlbauer, T. Reliability and minimal detectable change of the Upper Quarter Y Balance Test in healthy adolescents aged 12 to 17 years. Int. J. Sports Phys. Ther. 2019, 14, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Schwiertz, G.; Brueckner, D.; Beurskens, R.; Muehlbauer, T. Lower Quarter Y Balance Test performance: Reference values for healthy youth aged 10 to 17 years. Gait Posture 2020, 80, 148–154. [Google Scholar] [CrossRef]
- Azadeh, M.; Yahya, S.; Reza, S. The effect of 8 Weeks of Tai Chi exercises on girls’ static and dynamic balance with intellectual disability. Biol. Forum 2015, 7, 1256–1259. [Google Scholar]
- Kachouri, H.; Borji, R.; Baccouch, R.; Laatar, R.; Rebai, H.; Sahli, S. The effect of a combined strength and proprioceptive training on muscle strength and postural balance in boys with intellectual disability: An exploratory study. Res. Dev. Disabil. 2016, 53, 367–376. [Google Scholar] [CrossRef]
- Fotiadou, E.G.; Neofotistou, K.H.; Giagazoglou, P.F.; Tsimaras, V.K. The effect of a psychomotor education review 417 program on the static balance of children with intellectual disability. J. Strength Cond. Res. 2017, 31, 1702–1708. [Google Scholar] [CrossRef]
- Hsu, T.Y. Effects of Wii Fit balance game training on the balance ability of students with intellectual disabilities. J. Phys. Ther. Sci. 2016, 28, 1422–1426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ilbeigi, S.; Khirkhah, M.; Mahjur, M.; Soltani, H.; Khoshbakhti, J. Investigating the effects of 8 weeks of rope skipping on static and dynamic balance of educable mentally retarded boys. Int. J. Med. Res. Health Sci. 2016, 5, 349–353. [Google Scholar]
- Lee, K.; Lee, M.; Song, C. Balance training improves postural balance, gait, and functional strength in adolescents with intellectual disabilities: Single-blinded, randomized clinical trial. Disabil. Health J. 2016, 9, 416–422. [Google Scholar] [CrossRef] [PubMed]
- Hove, O. Weight survey on adults with mental retardation living in the community. Res. Dev. Disabil. 2004, 25, 9–17. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | 30 Students with BIF (YBT-LQ/UQ) | 30 Students without BIF (YBT-LQ) | 30 Students without BIF (YBT-UQ) | p-Value (YBT-LQ) | p-Value (YBT-UQ) |
|---|---|---|---|---|---|
| Age (years) | 13.7 ± 1.2 | 13.7 ± 1.3 | 13.7 ± 1.2 | 0.84 | 1.00 |
| Sex (m/f) | 22/8 | 22/8 | 22/8 | ||
| Body mass (kg) | 58.6 ± 11.5 | 56.1 ± 11.0 | 53.4 ± 11.6 | 0.39 | 0.09 |
| Body height (cm) | 163.0 ± 7.9 | 166.1 ± 10.6 | 167.0 ± 11.1 | 0.21 | 0.11 |
| Arm length, left (cm) | 81.5 ± 4.7 | – | 83.0 ± 6.6 | – | 0.34 |
| Arm length, right (cm) | 81.0 ± 4.8 | – | 83.5 ± 7.1 | – | 0.12 |
| Leg length, left (cm) | 90.0 ± 5.2 | 91.3 ± 6.9 | – | 0.41 | – |
| Leg length, right (cm) | 90.0 ± 5.3 | 91.2 ± 6.3 | – | 0.42 | – |
| Measure | Students with BIF (n = 30) | Students without BIF (n = 30) | p-Value | d-Value |
|---|---|---|---|---|
| Right leg reach | ||||
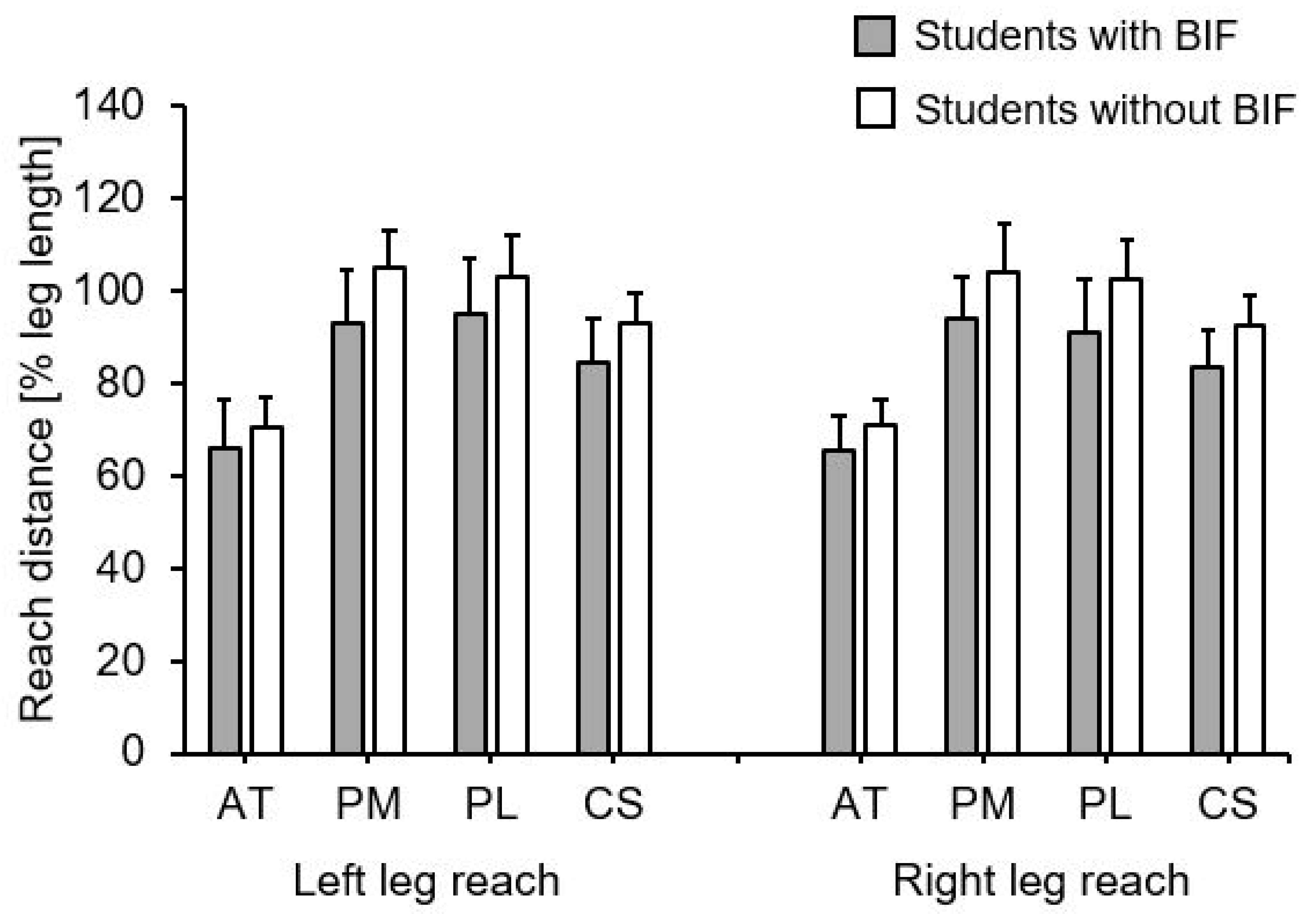
| AT (% LL) | 65.3 ± 7.6 | 70.8 ± 5.6 | 0.002 | 0.82 |
| PM (% LL) | 94.1 ± 9.1 | 104.3 ± 10.2 | <0.001 | 1.05 |
| PL (% LL) | 91.2 ± 11.2 | 102.8 ± 8.1 | <0.001 | 1.19 |
| CS (% LL) | 83.5 ± 7.9 | 92.6 ± 6.5 | <0.001 | 1.26 |
| Left leg reach | ||||
| AT (% LL) | 65.9 ± 10.4 | 70.7 ± 6.1 | 0.031 | 0.57 |
| PM (% LL) | 93.3 ± 11.3 | 105.1 ± 8.0 | <0.001 | 1.23 |
| PL (% LL) | 95.1 ± 11.8 | 103.3 ± 8.8 | 0.003 | 0.77 |
| CS (% LL) | 84.7 ± 9.6 | 93.1 ± 6.4 | <0.001 | 1.02 |
| Variables | Students with BIF (n = 30) | Students without BIF (n = 30) | p-Value | d-Value |
|---|---|---|---|---|
| Right arm reach | ||||
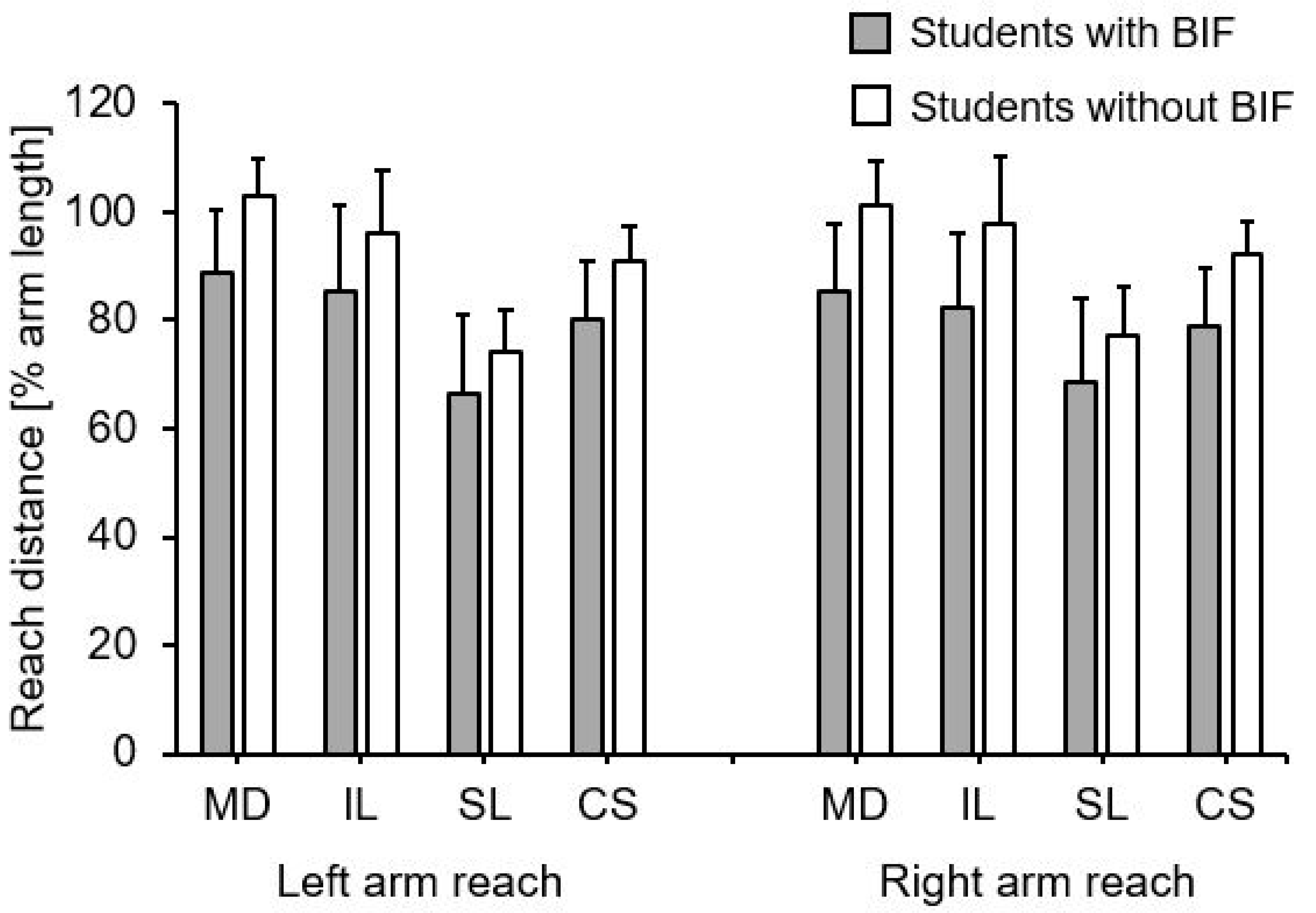
| MD (% AL) | 85.2 ± 12.6 | 101.3 ± 8.3 | <0.001 | 1.51 |
| IL (% AL) | 82.5 ± 13.6 | 97.9 ± 12.2 | <0.001 | 1.19 |
| SL (% AL) | 68.7 ± 15.4 | 77.3 ± 8.8 | 0.010 | 0.68 |
| CS (% AL) | 78.8 ± 10.7 | 92.2 ± 6.3 | <0.001 | 1.52 |
| Left arm reach | ||||
| MD (% AL) | 88.8 ± 11.7 | 102.8 ± 7.1 | <0.001 | 1.45 |
| IL (% AL) | 85.4 ± 16.0 | 95.9 ± 11.9 | 0.006 | 0.74 |
| SL (% AL) | 66.6 ± 14.5 | 74.2 ± 7.9 | 0.015 | 0.77 |
| CS (% AL) | 80.3 ± 10.8 | 91.0 ± 6.5 | <0.001 | 1.20 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bauer, J.; Kammermeier, H.; Schwiertz, G.; Muehlbauer, T. Comparison of Lower and Upper Quarter Y Balance Test Performance in Adolescent Students with Borderline Intellectual Functioning Compared to Age- and Sex-Matched Controls. Children 2021, 8, 805. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090805
Bauer J, Kammermeier H, Schwiertz G, Muehlbauer T. Comparison of Lower and Upper Quarter Y Balance Test Performance in Adolescent Students with Borderline Intellectual Functioning Compared to Age- and Sex-Matched Controls. Children. 2021; 8(9):805. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090805
Chicago/Turabian StyleBauer, Julian, Helena Kammermeier, Gerrit Schwiertz, and Thomas Muehlbauer. 2021. "Comparison of Lower and Upper Quarter Y Balance Test Performance in Adolescent Students with Borderline Intellectual Functioning Compared to Age- and Sex-Matched Controls" Children 8, no. 9: 805. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090805