Early Deaths in Childhood Cancer in Romania—A Single Institution Study

 ,
,
Abstract
:1. Introduction
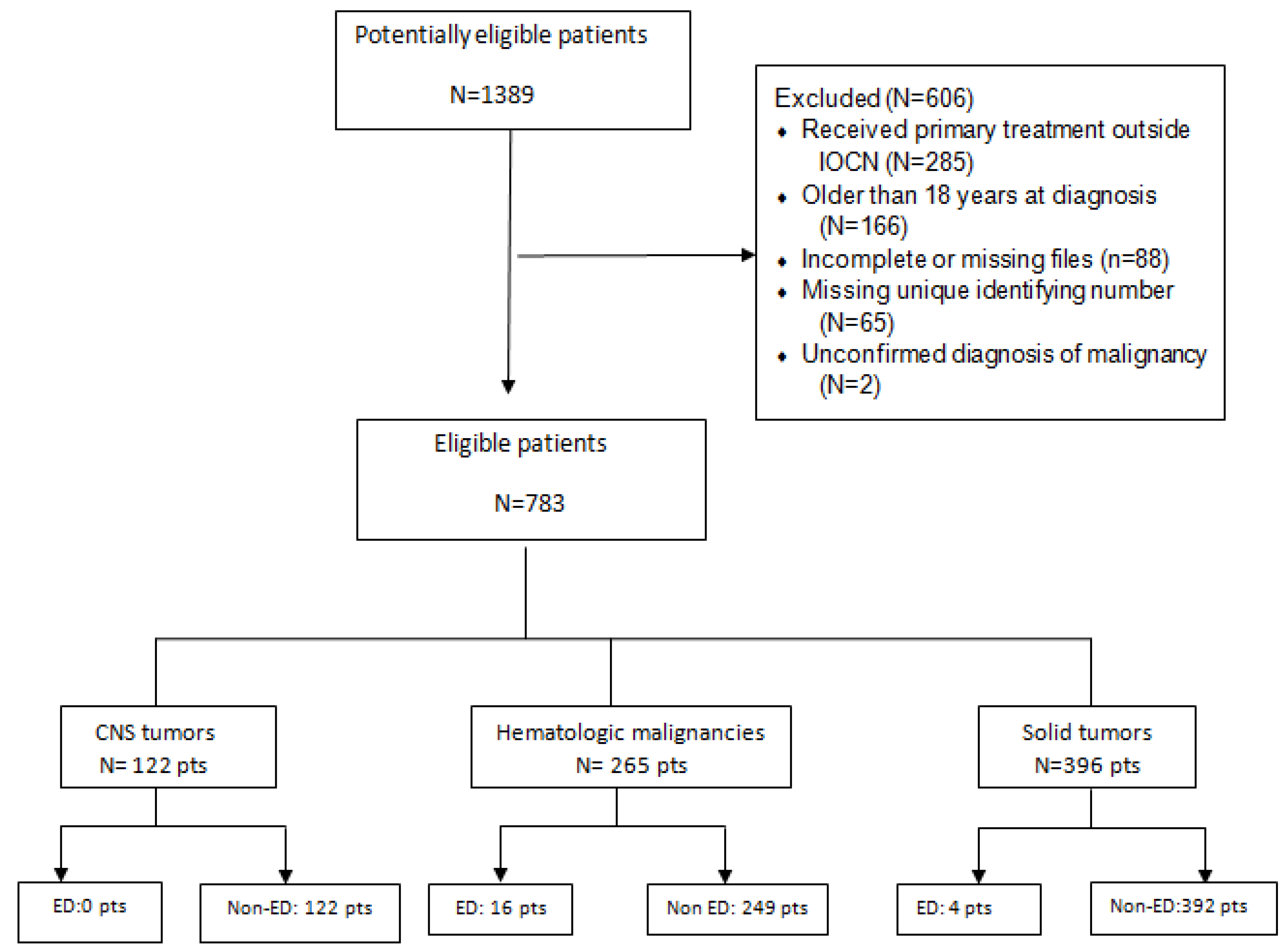
2. Materials and Methods
3. Results
Causes of Early Death
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jemal, A.; Siegel, R.; Xu, J.; Ward, E. Cancer statistics, 2010. CA Cancer J. Clin. 2010, 60, 277–300. [Google Scholar] [CrossRef] [PubMed]
- Howlader, N.; Noone, A.M.; Krapcho, M. (Eds.) SEER Cancer Statistics Review, 1975–2010; National Cancer Institute: Bethesda, MD, USA, 2013. Available online: http://seer.cancer.gov/csr/1975_2010/ (accessed on 23 July 2019).
- Pastore, G.; Viscomi, S.; Mosso, M.L.; Maule, M.M.; Terracini, B.; Magnani, C.; Merletti, F. Early deaths from childhood cancer: A report from the childhood Cancer Registry of Piedmont, Italy, 1967–1998. Eur. J Pediatr. 2004, 163, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Green, A.L.; Furutani, E.; Ribeiro, K.B.; Galindo, C.R. Death Within 1 Month of Diagnosis in Childhood Cancer: An Analysis of Risk Factors and Scope of the Problem. J. Clin. Oncol. 2017, 35, 1320–1327. [Google Scholar] [CrossRef] [PubMed]
- Becker, C.; Graf, N.; Grabow, D.; Creutzig, U.; Reinhardt, D.; Weyer-Elberich, V.; Spix, C.; Kaatsch, P. Early deaths from childhood cancer in Germany 1980–2016. Cancer Epidemiol. 2020, 65, 101669. [Google Scholar] [CrossRef] [PubMed]
- Gatta, G.; Capocaccia, R.; Stiller, C.; Kaatsch, P.; Berrino, F.; Terenziani, M. The Eurocare Working Group Childhood Cancer Survival Trends in Europe: A EUROCARE Working Group Study. J. Clin. Oncol. 2005, 23, 3742–3751. [Google Scholar] [CrossRef] [PubMed]
- Gatta, G.; Corazziari, I.; Magnani, C.; Peris-Bonet, R.; Roazzi, P.; Stiller, C. Childhood cancer survival in Europe. Ann. Oncol. 2003, 14, v119–v127. [Google Scholar] [CrossRef] [PubMed]
- Gatta, G.; Botta, L.; Rossi, S.; Aareleid, T.; Bielska-Lasota, M.; Clavel, J.; Dimitrova, N.; Jakab, Z.; Kaatsch, P.; Lacour, B. Childhood cancer survival in Europe 1999–2007: Results of Eurocare-5—A population based study. Lancet Oncol. 2014, 15, 35–47. [Google Scholar] [CrossRef]
- Pheby, D.; Martinez, C.; Roumagnac, M. European Network of Cancer Registries (ENCR): Recommendations for Coding Incidence Date. 1995. Available online: https://www.encr.eu/sites/default/files/pdf/incideng.pdf (accessed on 19 November 2020).
- Bray, F.; Parkin, D.M. Evaluation of data quality in the cancer registry: Principles and methods. Part I: Comparability, validity and timeliness. Eur. J. Cancer 2009, 45, 747–755. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, J.; Ries, I.; Hankey, B. The SEER Program Code Manual 1988 (Revised Edition 1992); National Institutes of Health, National Cancer Institute: Bethesda, MD, USA, 1992. [Google Scholar]
- Moreno, F.; Loria, D.; Abriata, G.; Terracini, B. Childhood cancer: Incidence and early deaths in Argentina, 2000–2008. Eur. J. Cancer 2013, 49, 465–473. [Google Scholar] [CrossRef] [PubMed]
- Hamre, M.R.; Williams, J.; Chuba, P.; Bhambhani, K.; Ravindranath, Y.; Severson, R.K. Early deaths in childhood cancer. Med. Pediatr. Oncol. 2000, 34, 343–347. [Google Scholar] [CrossRef]
- Molgaard-Hansen, L.; Möttönen, M.; Glosli, H.; Jónmundsson, G.K.; Abrahamsson, J.; Hasle, H. Nordic Society of Paediatric Haematology and Oncology (NOPHO) Early and treatment-related deaths in childhood acute myeloid leukaemia in the Nordic countries: 1984–2003. Br. J. Haematol. 2010, 151, 447–459. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristic | Children Dead within One Month | Children Surviving beyond One Month | All Children N = 783 | |
|---|---|---|---|---|
| Sex | ||||
| Male | 12 (3%) | 391 (97%) | 403 (51.46%) | |
| Female | 8 (2.2%) | 372 (97.8%) | 380 (48.54%) | |
| Age at diagnosis (years) | ||||
| <1 | - | 26 (100%) | 26 (3.32%) | |
| 1–4 | 9 (4.5%) | 191 (95.5%) | 200 (25.54%) | |
| 5–9 | 4 (2.3%) | 171 (97.7%) | 175 (22.34%) | |
| 10–14 | 7 (3.5%) | 200 (96.5%) | 207 (26.44%) | |
| 15–18 | - | 175 (100%) | 175 (22.34%) | |
| Period of diagnosis | ||||
| 1996–1999 | 5 (2.5%) | 198 (97.5%) | 203 (25.92%) | |
| 2000–2004 | 4 (1.5%) | 263 (98.5%) | 267 (34.1%) | |
| 2005–2008 | 11(3.5%) | 302 (96.5%) | 313 (40%) | |
| Diagnostic group | ||||
| CNS tumours | - | 122 (100%) | 122 (15.58%) | |
| Leukaemias | 11 (8%) | 125 (92%) | 136 (17.3%) | |
| Lymphomas | 5 (4%) | 124 (96%) | 129 (16.5%) | |
| Soft tissue and other extraosseous sarcomas | Rhabdomyosarcoma | 1 (2.9%) | 34 (97.1%) | 35 (4.4%) |
| Other STS | - | 29 (100%) | 29 (3.7) | |
| Extracranial GCT | 1 (2.5%) | 39 (97.5%) | 40 (5.1%) | |
| Renal tumours | Wilms’tumour | 2 (3.6%) | 54 (96.4%) | 56 (7.2%) |
| Other renal tumours | - | 4 (100%) | 4 (0.5%) | |
| Neuroblastoma | - | 44 (100%) | 44 (5.6%) | |
| Malignant bone tumours | Osteosarcoma | - | 37 (100%) | 37 (4.7%) |
| Ewing sarcoma | - | 32 (100%) | 32 (4.1%) | |
| Chondrosarcoma | - | 5 (100%) | 5 (0.6%) | |
| Malignant epithelial neoplasms and malignant melanomas | Nasopharyngeal carcinoma | - | 22 (100%) | 22 (2.8%) |
| Thyroid carcinoma | - | 40 (100%) | 40 (5.1%) | |
| Malignant melanoma | 7 (100%) | 7 (0.9%) | ||
| Other carcinoma | - | 28 (100%) | 28 (3.5%) | |
| Retinoblastoma | - | 15 (100%) | 15 (1.9%) | |
| Hepatic tumours | - | 2 (100%) | 2 (0.25%) | |
| Performance status at admission | ||||
| 0–2 | 2 (0.4%) | 518 (99.6%) | 520 (66.4%) | |
| 3–4 | 18 (12.6%) | 124 (88.4%) | 142 (18.1%) | |
| Unknown | - | 121 | 121 (15.5%) | |
| Diagnostic Group | Diagnosis | Children Dead within One Month | Children Surviving beyond One Month | All Children N = 783 |
|---|---|---|---|---|
| CNS tumours | Medulloblastoma | - | 45 | 45 (5.7%) |
| Ependymoma | - | 13 | 13 (1.7%) | |
| Astrocytoma | - | 44 | 44 (5.6%) | |
| Other CNS | - | 20 | 20 (2.5%) | |
| Leukaemias | ALL | 6 (5.6%) | 101 | 107 (13.7%) |
| AML | 5 (17.2%) | 24 | 29 (3.7%) | |
| Lymphomas | NHL—Non Burkitt’s | 3 (8.3%) | 36 | 39 (4.6%) |
| Burkitt’s lymphoma | 2 (9.1%) | 23 | 25 (2.8%) | |
| Hodgkin lymphoma | - | 65 | 65 (7.9%) | |
| Soft tissue and other extraosseous sarcomas | Rhabdomyosarcoma | 1 (2.9%) | 34 | 35 (4.5%) |
| Fibrosarcomas, peripheral nerve sheath tumours | - | 3 | 3 (0.38%) | |
| Other STS | - | 26 | 26 (3.3%) | |
| Germ cell tumours, trophoblastic tumours and neoplasms of gonads | Extracranial GCT | 1 (2.5%) | 39 | 40 (5.1%) |
| Gonadal carcinoma | 4 | 4 (0.5%) | ||
| Renal tumour | Wilms’tumour | 2 (3.6%) | 54 | 56 (7.2%) |
| Rhabdoid renal tumour | - | 1 | 1 (0.12%) | |
| Kidney sarcoma | - | 1 | 1 (0.12%) | |
| Renal carcinoma | - | 2 | 2 (0.25%) | |
| Neuroblastoma | Neuroblastoma | - | 44 | 44 (5.6%) |
| Malignant bone tumours | Osteosarcoma | - | 37 | 37 (4.7%) |
| Ewing sarcoma | - | 32 | 32 (4.1%) | |
| Chondrosarcoma | - | 5 | 5 (0.6%) | |
| Other malignant epithelial neoplasm and malignant melanomas | Nasopharyngeal carcinoma | - | 22 | 22 (2.8%) |
| Thyroid carcinoma | - | 40 | 40 (5.1%) | |
| Malignant Melanoma | - | 7 | 7 (0.9%) | |
| Adrenocortical carcinomas | - | 1 | 1 (0.12%) | |
| Skin carcinoma | - | 1 | 1 (0.12%) | |
| Other carcinomas | - | 22 | 22 (2.8%) | |
| Retinoblastoma | Retinoblastoma | - | 15 | 15 (1.9%) |
| Hepatic tumours | Hepatoblastoma | - | 1 | 1 (0.12%) |
| Hepatic carcinoma | - | 1 | 1 (0.12%) |
| Cause of Death | Major Diagnostic Group | ||
|---|---|---|---|
| Leukaemia | Lymphomas | Solid Tumour | |
| Bleeding | 7 pts | - | - |
| Infection | 1 pts | - | - |
| Leukostasis | 3 pts | - | - |
| Treatment related | - | - | 1 pts |
| Organ failure due to organ compression/involvement by tumour | - | 5 pts | 3 pts |
| Characteristic. | Children Dead within One Month | Children Surviving beyond One Month | All Children | p | |
|---|---|---|---|---|---|
| Sex | F | 7 (6,4%) | 103 (93.6%) | 110 | 0.85 |
| M | 9 (5.8%) | 416 (94.2%) | 155 | ||
| PS at start of treatment | 0–2 | 2 (1%) | 205 (99%) | 207 | <0.01 |
| 3–4 | 14 (24.1%) | 44 (75.9%) | 58 | ||
| Year of diagnosis | 1996–1999 | 5 (6%) | 79 (94%) | 84 | 0.70 |
| 2000–2003 | 4 (4.5%) | 84 (95.5%) | 88 | ||
| 2004–2008 | 7 (7.5%) | 86 (92.5%) | 93 | ||
| Leukaemia | Yes | 11 (8%) | 127 (92%) | 138 | 0.17 |
| No | 5 (3.9%) | 122 (96.1%) | 127 | ||
| Age at diagnosis (years) | <1 year | - | 3 (100%) | 3 | |
| 1–4 years | 6 (8%) | 69 (92%) | 75 | ||
| 5–9 years | 3 (4.1%) | 71 (95.9%) | 74 | ||
| 10–14 years | 6 (8.8%) | 62 (91.2%) | 68 | ||
| 15–18 years | 1 (2.2%) | 44 (97.8%) | 45 | ||
| Time interval between symptoms onset and diagnosis | <49 days | 4 (4.1%) | 94 (95.9%) | 98 | 0.99 |
| ≥49 days | 5 (5.1%) | 94 (94.9%) | 99 | ||
| Unknown | 7 (10.3%) | 61 (89.7%) | 68 | ||
| Case No | Age at Diagnosis | Sex | Time Interval Between Symptoms Onset and Diagnosis (Days) | Diagnosis | Stage | PS | Disease Complications at Diagnosis | Treatment | Treatment Toxicity | Pathophysiology of Death | Cause of Death | Time Interval between Diagnosis and Death (Days) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 4 | M | 26 | Burkitt’s lymphoma | IIIB | 2 | Bowel obstruction | Cytoreductive chemotherapy | Grade 3 neutropenia, grade 3 anaemia | Bowel obstruction due to organ compression by tumour | Disease progression | 24 |
| 2 | 13 | M | Unknown | AML | NA | 4 | Grade 4 thrombocytopenia | Cytoreductive chemotherapy | - | Brain haemorrhage | Disease progression | 23 |
| 3 | 13 | F | 15 | LNH | IVB | 3 | Bowel obstruction | Corticotherapy | Bowel obstruction due to organ compression by tumour | Disease progression | 12 | |
| 4 | 10 | F | 29 | AML | NA | 3 | Grade 4 anaemia, grade 4 thrombocytopenia, bleeding | Cytoreductivechemotherapy | - | Brain haemorrhage | Disease progression | 13 |
| 5 | 6 | M | Unknown | ALL | NA | 4 | Grade 4 thrombocytopenia, bleeding | Corticotherapy | - | Brain haemorrhage | Disease progression | 29 |
| 6 | 9 | M | Unknown | ALL | NA | 3 | Grade 4 anaemia, hyperleukocytosis, tumourlysis syndrome, bleeding | Cytoreductive chemotherapy | - | Leukostasis | Disease progression | 26 |
| 7 | 13 | F | Unknown | AML | NA | 3 | Grade 4 thrombocytopenia, bleeding, febrile neutropenia | Cytoreductive chemotherapy | - | Brain haemorrhage | Disease progression | 13 |
| 8 | 1 | F | 4 | ALL | NA | 3 | Tumour lysis syndrome, bleeding | Treatment of tumour lysis syndrome, supportive treatment | - | Leukostasis | Disease progression | 6 |
| 9 | 14 | M | 82 | ALL | - | 2 | Febrile neutropenia | Cytoreductive chemotherapy | - | Septicaemia | Disease progression | 19 |
| 10 | 6 | F | 66 | Wilms’tumour | III | 3 | - | Neoadjuvant chemotherapy according to SIOP 93,unilateral nephrectomy | Postoperative complications | Postoperative complications | Treatment related | 30 |
| 11 | 1 | M | unknown | Wilms’tumour | III | 3 | Respiratory distress due to high tumour volume | Neoadjuvant chemotherapy according to SIOP 93 | - | Cardiac failure due to organ compression by tumour | Disease progression | 5 |
| 12 | 2 | M | Unknown | ALL | NA | 3 | Tumour lysis syndrome, hyperleukocytosis | Supportive treatment, treatment for tumour lysis syndrome | - | Leukostasis | Disease progression | 4 |
| 13 | 4 | M | Unknown | AML | NA | 3 | Grad 4 thrombocytopenia, bleeding | Supportive treatment | - | Gastrointestinal bleeding | Disease progression | 2 |
| 14 | 4 | M | Unknown | Burkitt’s lymphoma | IV | 4 | Increased liver enzymes, grade 4 thrombocytopenia | Cytoreductive chemotherapy according to NHL-BFM-95 | - | Acute liver failure due to organ involvement by tumour | Disease progression | 7 |
| 15 | 5 | F | 8 | Large B-cell Lymphoma | IV | 3 | Increased liver enzymes | Cytoreductive chemotherapy | - | Acute liver failure due to organ involvement by tumour | Disease progression | 24 |
| 16 | 2 | M | Unknown | Parapharyngeal embryonal rhabdomyosarcoma | III | 4 | Respiratory distress | Chemotherapy according to CESS 91 | - | Acute respiratory failure due to organ compression by tumour | Disease progression | 5 |
| 17 | 14 | M | Unknown | Non-Hodgkin lymphoma non-Burkitt | IVB | 4 | Respiratory distress | Cytoreductive chemotherapy according to NHL-BFM-95 | - | Acute respiratory failure due to organ compression by tumour | Disease progression | 4 |
| 18 | 1 | F | Unknown | ALL | NA | 4 | Grade 4 thrombocytopenia | Cytoreductive chemotherapy according to BFM 95 | - | Brain haemorrhage | Disease progression | 4 |
| 19 | 1 | M | 4 | Sacrococcygeal Yolk sac tumour | NA | 3 | Respiratory distress | Supportive treatment | - | Acute respiratory failure due to organ compression by tumour | Disease progression | 12 |
| 20 | 12 | F | Unknown | AML | NA | 3 | Febrile neutropenia, grade 4 thrombocytopenia | Cytoreductive and induction chemotherapy according to BFM-93 | - | Brain haemorrhage | Disease progression | 15 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pruteanu, D.P.; Olteanu, E.D.; Cosnarovici, R.; Mihut, E.; Ecea, R.; Todor, N.; Nagy, V. Early Deaths in Childhood Cancer in Romania—A Single Institution Study. Children 2021, 8, 814. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090814
Pruteanu DP, Olteanu ED, Cosnarovici R, Mihut E, Ecea R, Todor N, Nagy V. Early Deaths in Childhood Cancer in Romania—A Single Institution Study. Children. 2021; 8(9):814. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090814
Chicago/Turabian StylePruteanu, Doina Paula, Elena Diana Olteanu, Rodica Cosnarovici, Emilia Mihut, Radu Ecea, Nicolae Todor, and Viorica Nagy. 2021. "Early Deaths in Childhood Cancer in Romania—A Single Institution Study" Children 8, no. 9: 814. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090814