
Prevalence of Iodine Deficiency among School Children from New Settlement in Kyrgyzstan

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
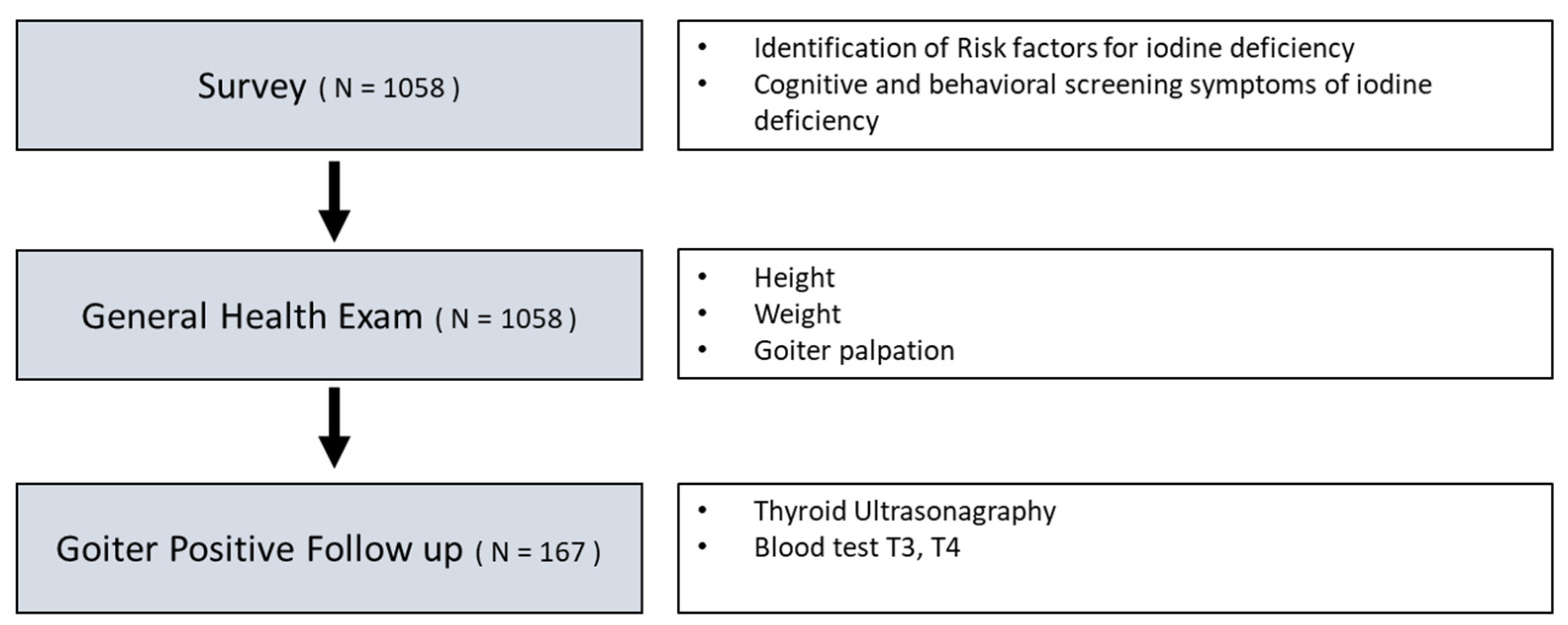
2.1. Study Design
2.2. Participants
2.3. Ethical Considerations
2.4. Measurement
2.5. Statistical Methods
3. Results
General Characteristics of Participants
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Guideline: Fortification of Food-Grade Salt with Iodine for the Prevention and Control of Iodine Deficiency Disorders; World Health Organization: Geneva, Switzerland, 2014. Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/25473709 (accessed on 30 June 2021).
- Biban, B.G.; Lichiardopol, C. Iodine deficiency, still a global problem? Curr. Health Sci. J. 2017, 43, 103–111. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Nutrition Landscape Information System (NLiS) Country Profile Indicators: Interpretation Guide, 2nd ed.; World Health Organization: Geneva, Switzerland, 2019; Available online: https://apps.who.int/iris/bitstream/handle/10665/332223/9789241516952-eng.pdf?isAllowed=y&sequence=1 (accessed on 30 June 2021).
- Zimmermann, M.B. Iodine and iodine deficiency disorders. In Present Knowledge in Nutrition, 10th ed.; Erdman, J.W., Macdonald, I.A., Zeisel, S.H., Eds.; Wiley Online Books: Hoboken, NJ, USA, 2012; Chapter 36; pp. 554–567. [Google Scholar] [CrossRef]
- World Health Organization. Iodine and Health: Eliminating Iodine Deficiency Disorders Safely through Salt Iodization; WHO: Geneva, Switzerland, 1994; Available online: https://apps.who.int/iris/bitstream/handle/10665/58693/WHO_NUT_94.4.pdf;jsessionid=4F5621B8679DFA7DABF7A94ED70E84EA?sequence=1 (accessed on 30 June 2021).
- World Health Organization. Assessment of the Iodine Deficiency Disorders and Monitoring Their Elimination, 3rd ed.; WHO: Geneva, Switzerland, 2007; Available online: https://apps.who.int/iris/bitstream/handle/10665/43781/9789241595827_eng.pdf?sequence=1&isAllowed=y (accessed on 30 June 2021).
- Sultanalieva, R.B.; Beishekeyeva, G.I.; Gerasimov, G.A. Assessment of the provision of iodine supply to pregnant and lactating women in Kyrgyzstan. Clin. Exp. Thyroidol. 2016, 12, 34–37. [Google Scholar] [CrossRef] [Green Version]
- Sultanalieva, R.B.; Mamutova, S.; van der Haar, F. The current salt iodization strategy in Kyrgyzstan ensures sufficient iodine nutrition among school-age children but not pregnant women. Public Health Nutr. 2010, 13, 623–630. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, H.; Lee, S.J.; Lee, Y.N.; Shon, S. Community health needs assessment for a child health promotion program in Kyrgyzstan. Eval. Program. Plann. 2019, 74, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Matthys, B.; Davlatmamadova, M.; Karimova, G.; Jean-Richard, V.; Zimmermann, M.B.; Wyss, K. Iodine nutritional status and risk factors for goitre among schoolchildren in South Tajikistan. BMC Endocr. Disord. 2013, 13, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorokman, T.; Bachu, M.; Sokolhyk, I. Frequency of iodine deficiency disorders among children living in the iodine deficiency region. Rom J. Pediatr. 2021, 70, 44–52. [Google Scholar] [CrossRef]
- Neelopant, S.; Hatnoor, S.; Shashidhar, B.; Kirte, R.; Roy, S.; Vastrad, P.; Prasad, U. Iodine Deficiency Disorder Survey among 6 to 12 Years Children in Rural Areas of Raichur District. Int. J. Sci. Study 2021, 8, 119–125. [Google Scholar]
- Zimmermann, M.B.; Boelaert, K. Iodine deficiency and thyroid disorders. Lancet Diabetes Endocrinol. 2015, 3, 286–295. [Google Scholar] [CrossRef]
- Abbag, F.; Abu-Eshy, S.; Mahfouz, A.; Alsaleem, M.; Alsaleem, S.; Patel, A.; Mirdad, T.; Shati, A.; Awadalla, N. Iodine Deficiency Disorders as a Predictor of Stunting among Primary School Children in the Aseer Region, Southwestern Saudi Arabia. Int. J. Environ. Res. Public Health 2021, 18, 7644. [Google Scholar] [CrossRef] [PubMed]
- Elias, E.; Tsegaye, W.; Stoecker, B.J.; Gebreegziabher, T. Excessive intake of iodine and low prevalence of goiter in school age children five years after implementation of national salt iodization in Shebedino woreda, southern Ethiopia. BMC Public Health 2021, 21, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Olivieri, A.; Angelis, S.; Moleti, M.; Vermiglio, F. Iodine Deficiency and Thyroid Function. In Thyroid, Obesity and Metabolism; Springer: Cham, Switzerland, 2021; pp. 3–20. [Google Scholar]
- Campanozzi, A.; Rutigliano, I.; Macchia, P.E.; De Filippo, G.; Barbato, A.; Iacone, R.; Russo, O.; D’Angelo, G.; Frigeri, M.; Pensabene, L.; et al. Iodine deficiency among Italian children and adolescents assessed through 24-hour urinary iodine excretion. Am. J. Clin. Nutr. 2019, 109, 1080–1087. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Ren, Z.; Li, S.; Tan, L.; Zhang, W. The relationship of different levels of high iodine and goiter in school children: A meta-analysis. Nutr. Metab. 2021, 18, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Sunamak, O.; Düren, M. Comparison of physical examination and simultaneous ultrasonography results in patient in whom thyroid gland nodule was diagnosed on scintigraphy previously and referred to general surgery clinics. Haydarpasa Numune Med. J. 2019, 59, 67–70. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Items | Category | n | % | Mean(SD) | Min–Max |
|---|---|---|---|---|---|
| Sex | Boy | 500 | 47.3 | ||
| Girl | 558 | 52.7 | |||
| Age | 7–9 | 407 | 38.5 | 10.7 (2.64) | 7–15 |
| 10–12 | 325 | 30.7 | |||
| 13–15 | 326 | 30.8 | |||
| Weight (kg) | Z score ≤ −2 | 76 | 7.2 | 32.8 (6.37) | 21–60 |
| Height (cm) | Z score ≤ −2 | 31 | 2.9 | 142.66 (12.24) | 120.6–167.2 |
| Age Group | Gender | n | BMI Percentile | SD | BMI z-Score | SD | Height (cm) | SD | Stunted: Z Score < −2 (n) | X2 | Weight (kg) | SD | Underweight: Z Score < −2 (n) | X2 | Signs of Iodine Deficiency (Mean, SD) | Signs of Iodine Deficiency (Median, SE) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 7–9 years | M | 199 | 29.7 | 30.12 | 0.32 | 0.60 | 129.9 | 4.72 | 0 | 27.6 | 2.09 | 0 | 1.9 (1.52) | 2 (0.10) | ||
| F | 208 | 23.8 | 28.51 | 0.21 | 0.52 | 129.5 | 4.94 | 0 | 27.2 | 1.88 | 0 | 2.2 (1.70) | 2 (0.11) | |||
| subtotal | 407 | 26.7 | 29.42 | 0.26 | 0.56 | 129.7 | 4.83 | 0 | 27.4 | 2.00 | 0 | 2.0 (1.62) | 2 (0.08) | |||
| 10–12 years | M | 142 | 1.9 | 4.03 | −1.04 | 0.79 | 146.1 | 5.48 | 2 | 33.3 | 2.36 | 0 | 2.6 (1.66) | 3 (0.13) | ||
| F | 183 | 2.7 | 5.59 | −1.02 | 0.80 | 145.9 | 5.43 | 5 | 33.1 | 2.27 | 2 | 2.6 (1.87) | 3 (0.13) | |||
| subtotal | 325 | 2.3 | 4.98 | −1.03 | 0.79 | 146.0 | 5.45 | 7 | 33.2 | 2.31 | 2 | 2.6 (1.78) | 3 (0.09) | |||
| 13–15 years | M | 159 | 0.6 | 2.10 | −1.61 | 1.35 | 154.2 | 6.93 | 20 | 38.7 | 6.42 | 44 | 3.0 (1.82) | 3 (0.14) | ||
| F | 167 | 0.2 | 0.62 | −1.64 | 1.35 | 156.8 | 5.87 | 4 | 39.8 | 6.72 | 30 | 3.1 (1.55) | 3 (0.12) | |||
| subtotal | 326 | 0.4 | 1.54 | −1.62 | 1.35 | 155.5 | 6.53 | 24 | 39.2 | 6.59 | 74 | 3.1 (1.6) | 3 (0.09) | |||
| Total | 1058 | 11.1 | 22.20 | −0.72 | 1.24 | 142.7 | 12.24 | 31 (2.9%) | <0.001 | 32.8 | 6.37 | 76 (7.2%) | <0.001 | 2 (0.05) |
| Age Groups | n | % | Height (cm) | Stunted: Z Score < −2 (n) | X2 | Weight (kg) | Underweight: Z Score < −2 (n) | X2 | TSH (mU/L) | FreeT4 (ng/dL) | Perceived Cognitive Signs of Iodine Deficiency | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fast Fatigue | Declined Memory and School Performance | Decreased Concentration and Attention | ||||||||||||
| 7–9 years | Boy | 16 | 9.6 | 130.6 (±5.72) | 0 | 27.4 (±2.21) | 0 | 3.2 (±0.55) | 1.2 (±0.16) | 13 | 13 | 13 | ||
| Girl | 43 | 59 | 131.9 (±4.42) | 0 | 27.8 (±1.43) | 0 | 2.8 (±0.68) | 1.7 (±1.53) | 37 | 37 | 37 | |||
| Subtotal | 59 | 131.5 (±4.79) | 0 | 27.7 (±1.66) | 0 | 2.9 (±0.65) | 1.6 (±1.29) | 50 | 50 | 50 | ||||
| 10–12 years | Boy | 36 | 21.6 | 145.9 (±5.21) | 1 | 33.2 (±1.77) | 0 | 2.9 (±0.54) | 1.4 (±0.26) | 32 | 32 | 32 | ||
| Girl | 38 | 22.8 | 144.2 (±4.98) | 2 | 31.9 (±1.84) | 1 | 3.1 (±0.49) | 1.3 (±0.23) | 30 | 30 | 30 | |||
| Subtotal | 74 | 145.0 (±5.12) | 3 | 32.5 (±1.92) | 1 | 3.0 (±0.52) | 1.4 (±0.25) | 62 | 62 | 62 | ||||
| 13–15 years | Boy | 15 | 9.0 | 152.1 (±4.25) | 0 | 35.4 (±3.38) | 8 | 3.0 (±0.30) | 1.4 (±0.27) | 11 | 11 | 11 | ||
| Girl | 19 | 11.4 | 146.2 (±9.84) | 4 | 35.1 (±2.51) | 7 | 3.0 (±0.41) | 1.5 (±0.20) | 18 | 18 | 18 | |||
| Subtotal | 34 | 148.8 (±8.31) | 4 | 35.3 (±2.88) | 15 | 3.0 (±0.34) | 1.5 (±0.24) | 29 | 29 | 29 | ||||
| Overall | 167 | 141.0 (±9.21) | 7(4.2%) | 0.024 | 31.4 (±3.55) | 16(9.6%) | <0.001 | 2.97 (±.54) | 1.47 (±0.82) | 141 | 141 | 141 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Urmatova, B.; Shin, H.; Shon, S.; Abdyldayeva, Z.; Ishaeva, E.; Knyazeva, V. Prevalence of Iodine Deficiency among School Children from New Settlement in Kyrgyzstan. Children 2021, 8, 817. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090817
Urmatova B, Shin H, Shon S, Abdyldayeva Z, Ishaeva E, Knyazeva V. Prevalence of Iodine Deficiency among School Children from New Settlement in Kyrgyzstan. Children. 2021; 8(9):817. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090817
Chicago/Turabian StyleUrmatova, Begaiym, Hyunsook Shin, Soonyoung Shon, Zeinep Abdyldayeva, Elmira Ishaeva, and Valeriya Knyazeva. 2021. "Prevalence of Iodine Deficiency among School Children from New Settlement in Kyrgyzstan" Children 8, no. 9: 817. https://0-doi-org.brum.beds.ac.uk/10.3390/children8090817