
Longitudinal Motor-Developmental Outcomes in Infants with a Critical Congenital Heart Defect

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
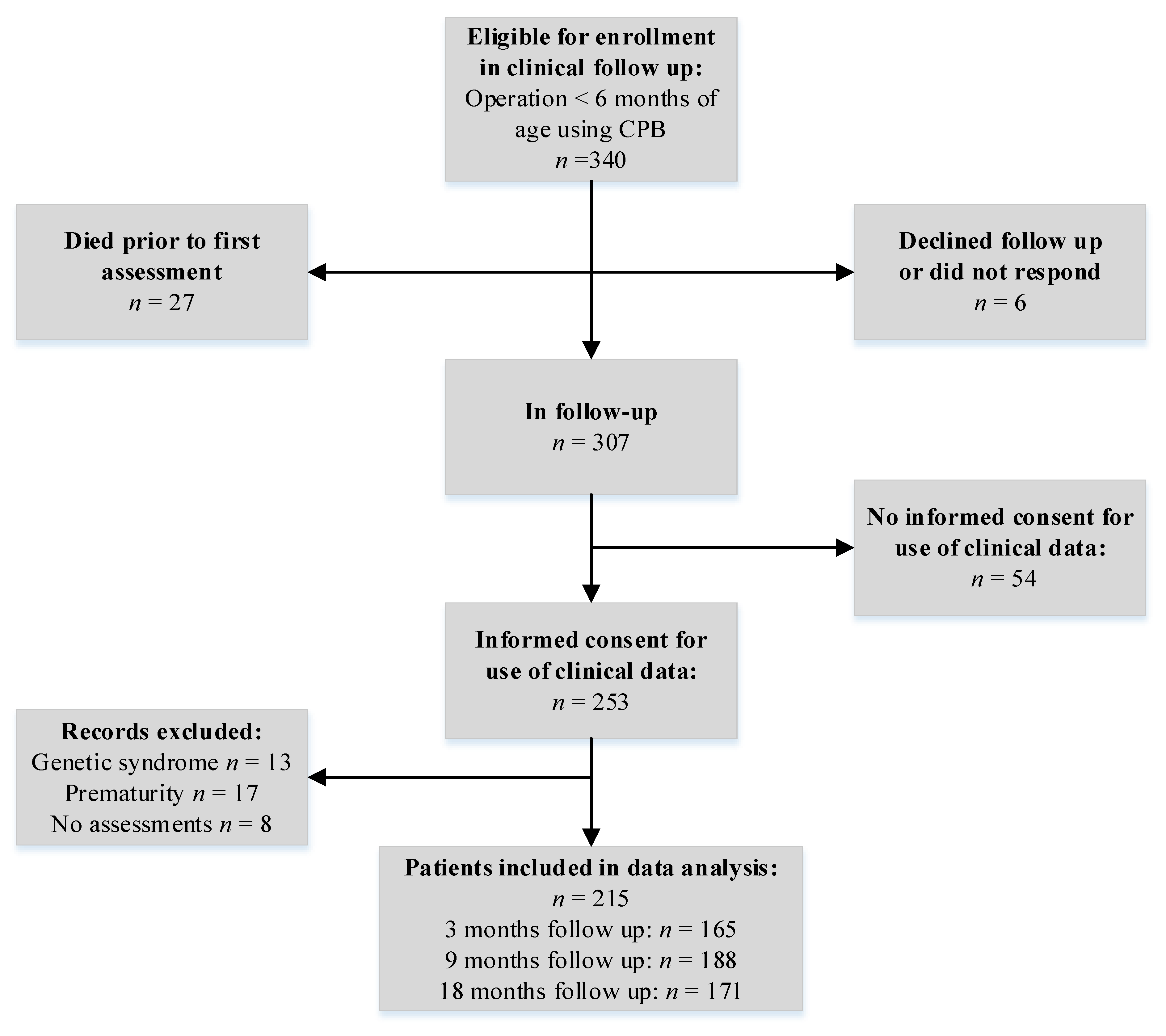
2.2. Participants
2.3. Outcome Assessment
2.4. Statistical Analysis
3. Results
3.1. Developmental Outcomes
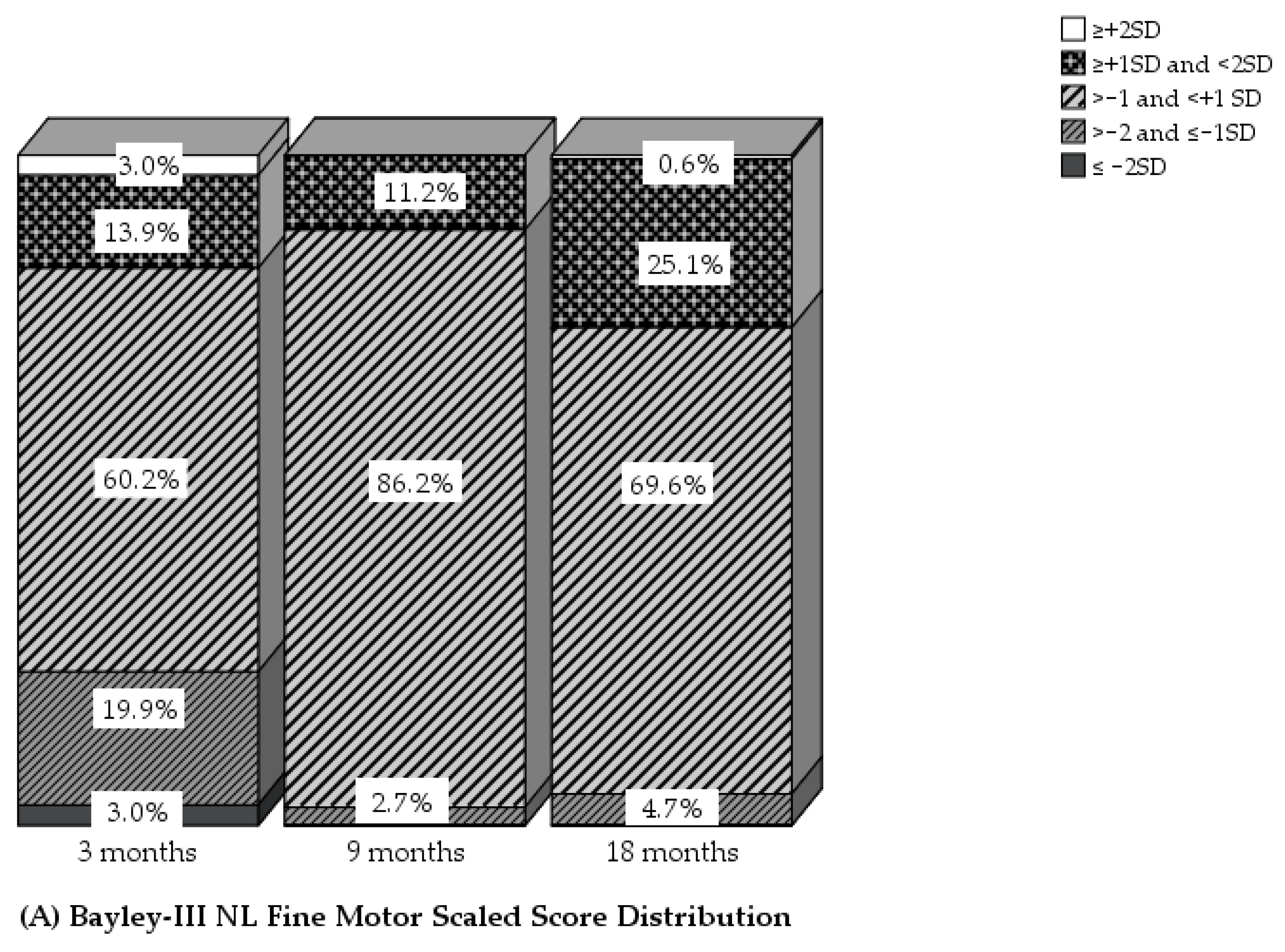
3.1.1. Fine Motor Development
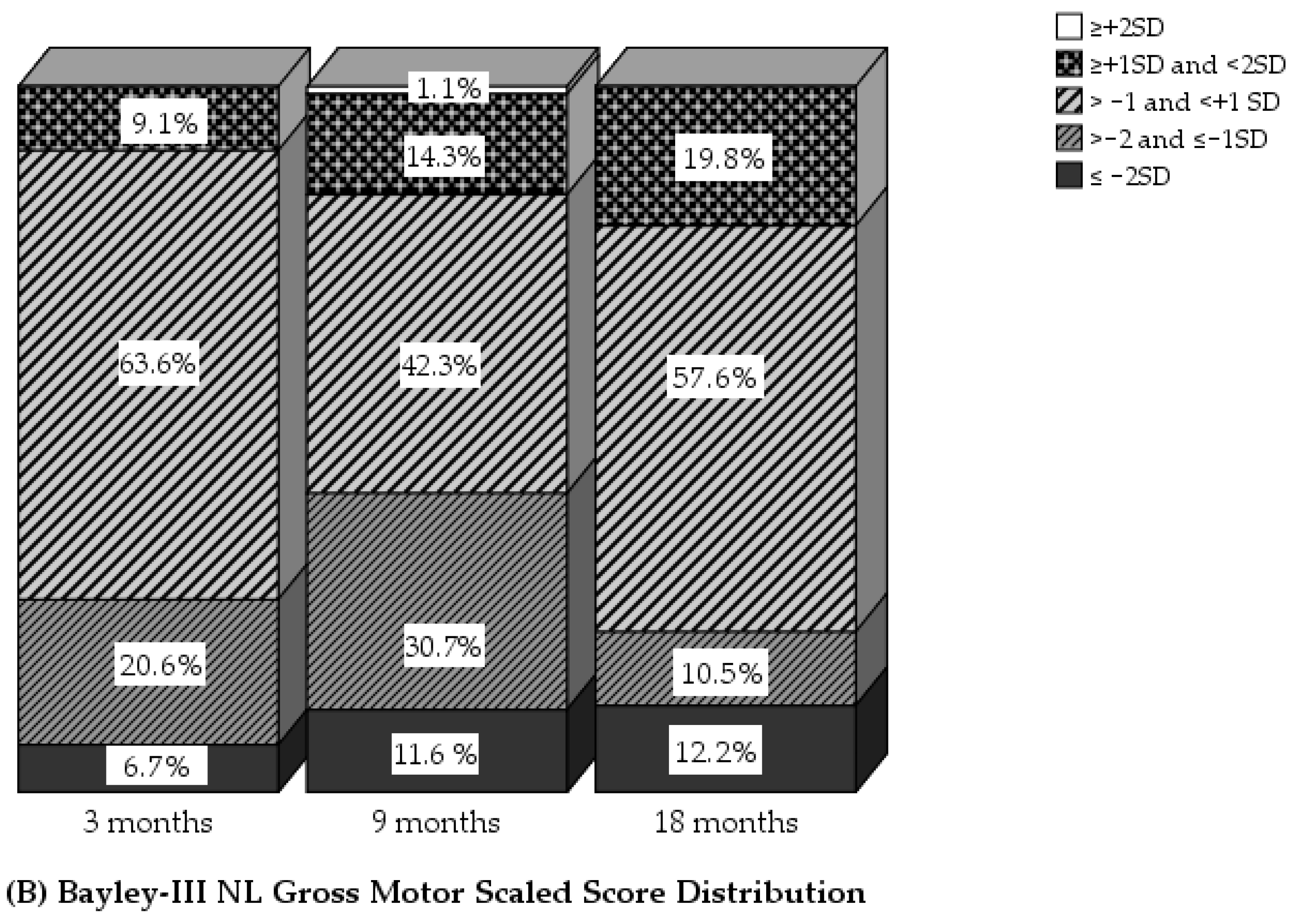
3.1.2. Gross Motor Development
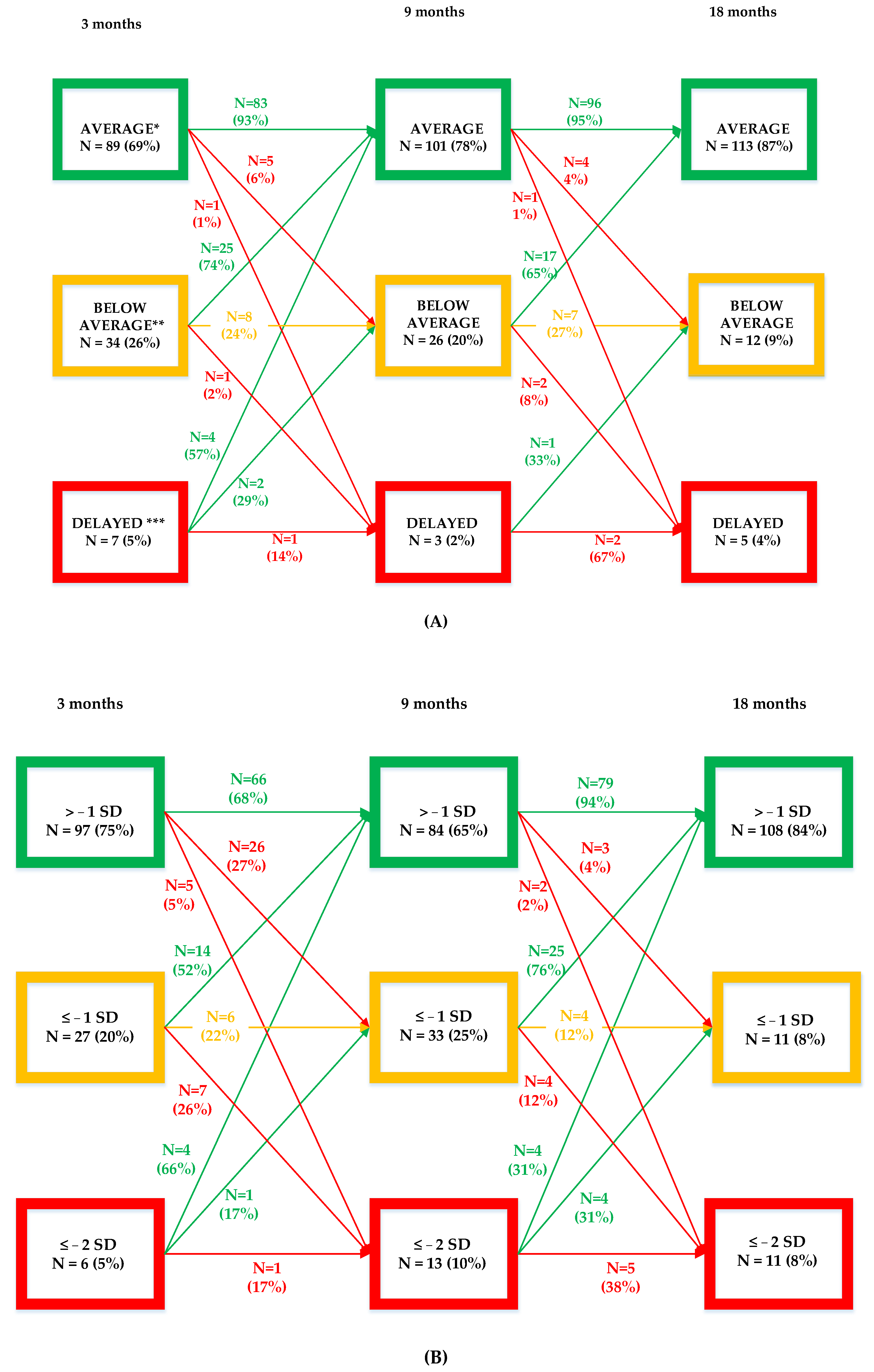
3.2. Longitudinal Motor Development 0–18 Months
3.2.1. Total Motor Trajectories
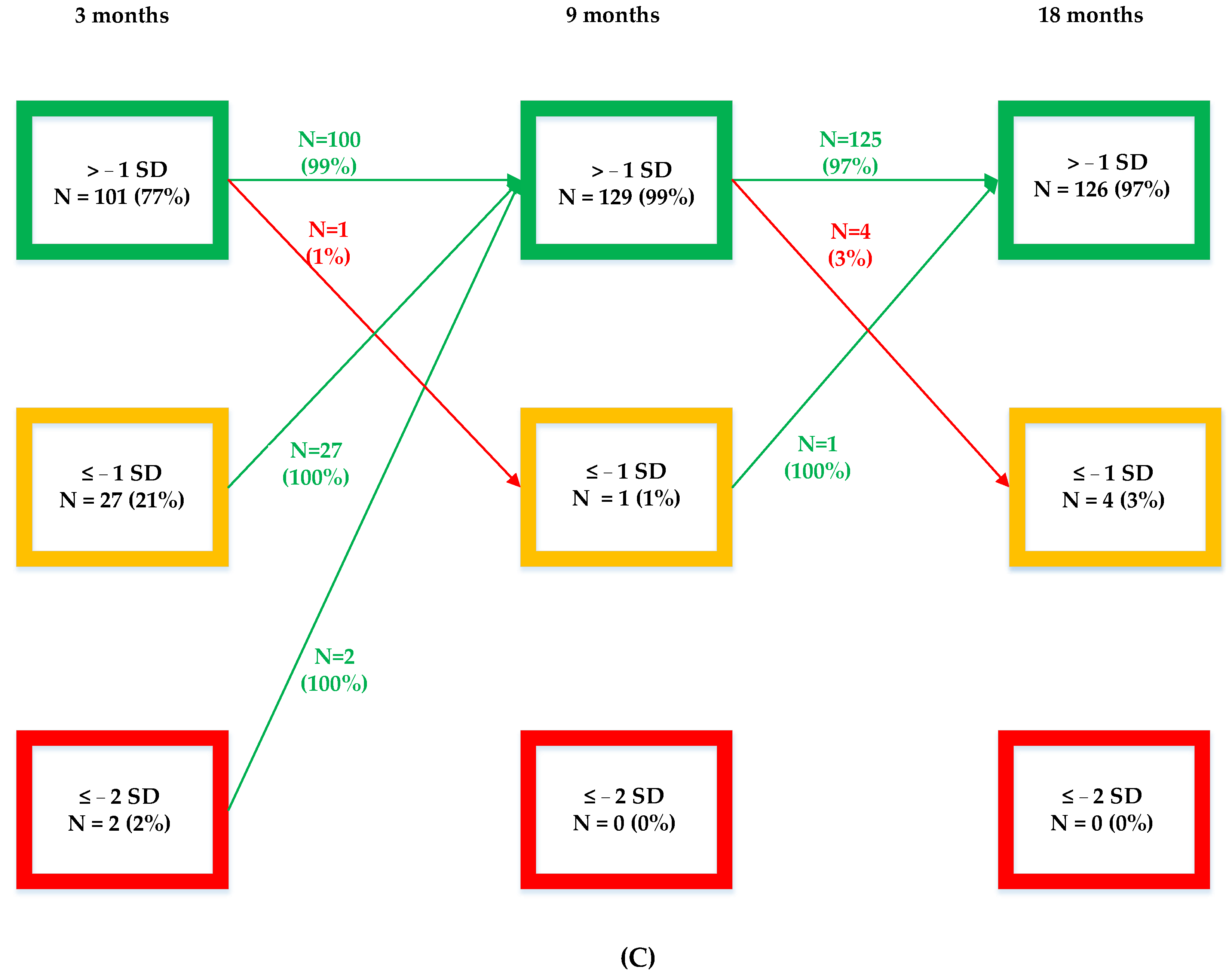
3.2.2. Gross Motor Trajectories
3.2.3. Fine Motor Trajectories
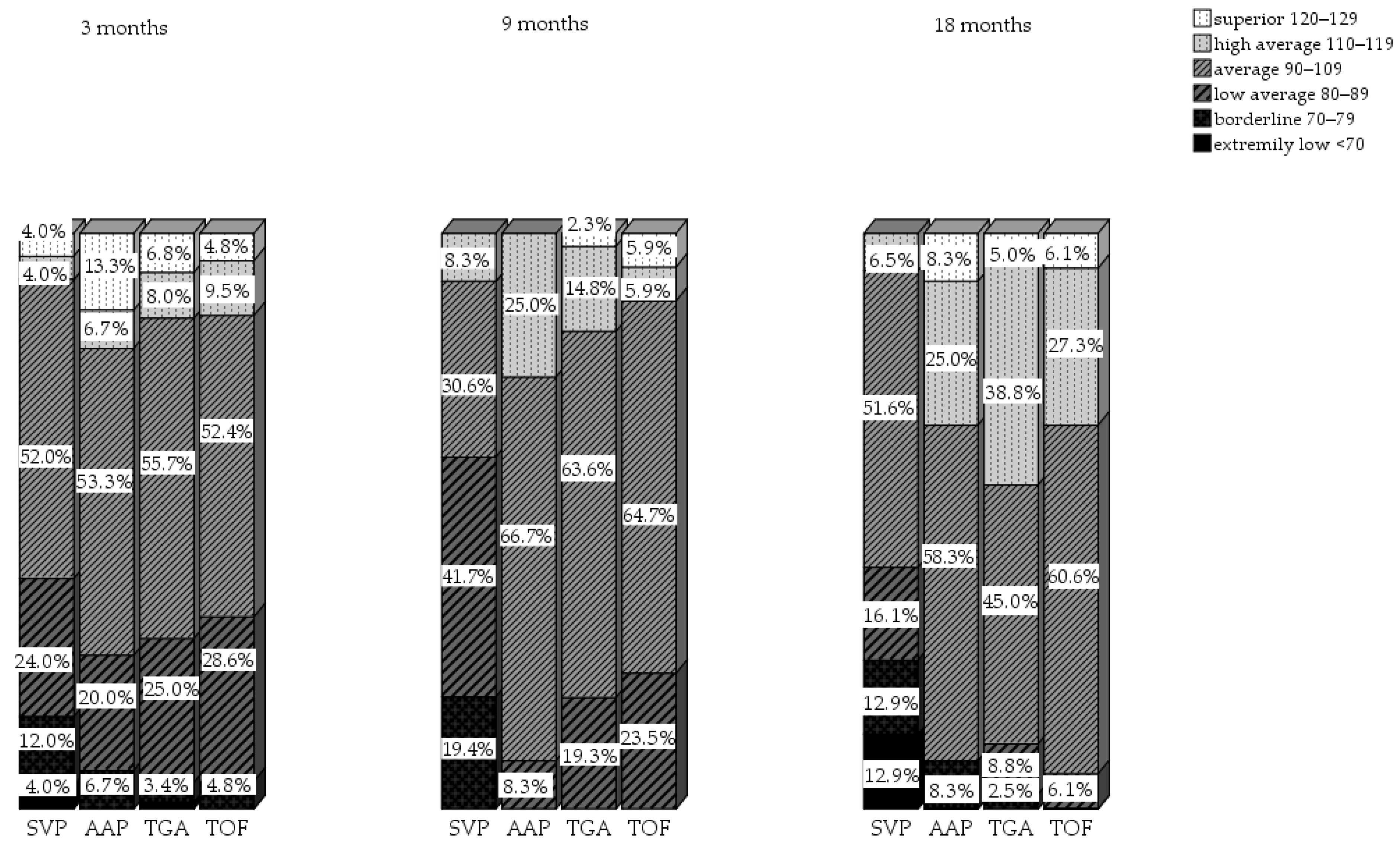
3.3. Motor Development per Diagnosis Group
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Liu, Y.; Chen, S.; Zu, L.; Black, G.C.; Choy, M.; Li, N.; Keavney, B.D. Global Birth Prevalence of Congenital Heart Defects 1970–2017: Updated Systematic Review and Meta-Analysis of 260 Studies. Int. J. Epidemiol. 2019, 48, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Heron, M. Deaths: Leading Causes for 2019. Natl. Vital Stat. Rep. 2021, 70, 1–114. [Google Scholar] [PubMed]
- Oster, M.E.; Lee, K.A.; Honein, M.A.; Riehle-Colarusso, T.; Shin, M.; Correa, A. Temporal Trends in Survival among Infants with Critical Congenital Heart Defects. Pediatrics 2013, 131, e1502–e1508. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khairy, P.; Ionescu-Ittu, R.; MacKie, A.S.; Abrahamowicz, M.; Pilote, L.; Marelli, A.J. Changing Mortality in Congenital Heart Disease. J. Am. Coll. Cardiol. 2010, 56, 1149–1157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandalenakis, Z.; Giang, K.W.; Eriksson, P.; Liden, H.; Synnergren, M.; Wåhlander, H.; Fedchenko, M.; Rosengren, A.; Dellborg, M. Survival in Children with Congenital Heart Disease: Have We Reached a Peak at 97%? J. Am. Heart Assoc. 2020, 9, e017704. [Google Scholar] [CrossRef]
- Brosig, C.L.; Bear, L.; Allen, S.; Simpson, P.; Zhang, L.; Frommelt, M.; Mussatto, K.A. Neurodevelopmental Outcomes at 2 and 4 Years in Children with Congenital Heart Disease. Congenit. Heart Dis. 2018, 13, 700–705. [Google Scholar] [CrossRef]
- Latal, B. Neurodevelopmental Outcomes of the Child with Congenital Heart Disease. Clin. Perinatol. 2016, 43, 173–185. [Google Scholar] [CrossRef]
- Marino, B.S.; Lipkin, P.H.; Newburger, J.W.; Peacock, G.; Gerdes, M.; Gaynor, J.W.; Mussatto, K.A.; Uzark, K.; Goldberg, C.S.; Johnson, W.H.; et al. Neurodevelopmental Outcomes in Children with Congenital Heart Disease: Evaluation and Management a Scientific Statement from the American Heart Association. Circulation 2012, 126, 1143–1172. [Google Scholar] [CrossRef] [Green Version]
- Ware, J.; Butcher, J.L.; Latal, B.; Sadhwani, A.; Rollins, C.K.; Brosig Soto, C.L.; Butler, S.C.; Eiler-Sims, P.B.; Ullman Shade, C.V.; Wernovsky, G. Neurodevelopmental Evaluation Strategies for Children with Congenital Heart Disease Aged Birth through 5 Years: Recommendations from the Cardiac Neurodevelopmental Outcome Collaborative. Cardiol. Young 2020, 30, 1609–1622. [Google Scholar] [CrossRef]
- Song, K.J.; Kim, M.G.; Ko, E.J.; Sung, I.Y. Neurodevelopmental Outcomes after Congenital Heart Disease Surgery in Infancy: A 2-Year Serial Follow-Up. Children 2021, 8, 911. [Google Scholar] [CrossRef]
- Huisenga, D.; La Bastide-Van Gemert, S.; Van Bergen, A.; Sweeney, J.; Hadders-Algra, M. Developmental Outcomes after Early Surgery for Complex Congenital Heart Disease: A Systematic Review and Meta-Analysis. Dev. Med. Child Neurol. 2020, 63, 29–46. [Google Scholar] [CrossRef] [PubMed]
- Sprong, M.C.A.; Broeders, W.; van der Net, J.; Breur, J.M.P.J.; de Vries, L.S.; Slieker, M.G.; van Brussel, M. Motor Developmental Delay After Cardiac Surgery in Children with a Critical Congenital Heart Defect: A Systematic Literature Review and Meta-Analysis. Pediatric Phys. Ther. 2021, 33, 186–197. [Google Scholar] [CrossRef] [PubMed]
- Marino, B.S. New Concepts in Predicting, Evaluating, and Managing Neurodevelopmental Outcomes in Children with Congenital Heart Disease. Curr. Opin. Pediatrics 2013, 25, 574–584. [Google Scholar] [CrossRef] [PubMed]
- Kamphuis, M.; Vogels, T.; Ottenkamp, J.; Van der Wall, E.E.; Verloove-Vanhorick, S.P.; Vliegen, H.W. Employment in Adults with Congenital Heart Disease. Arch. Pediatrics Adolesc. Med. 2002, 156, 1143–1148. [Google Scholar] [CrossRef] [Green Version]
- Kovacs, A.H.; Sears, S.F.; Saidi, A.S. Biopsychosocial Experiences of Adults with Congenital Heart Disease: Review of the Literature. Am. Heart J. 2005, 150, 193–201. [Google Scholar] [CrossRef]
- Haseba, S.; Sakakima, H.; Nakao, S.; Ohira, M.; Yanagi, S.; Imoto, Y.; Yoshida, A.; Shimodozono, M. Early Postoperative Physical Therapy for Improving Short-Term Gross Motor Outcome in Infants with Cyanotic and Acyanotic Congenital Heart Disease. Disabil. Rehabil. 2018, 40, 1694–1701. [Google Scholar] [CrossRef]
- Gallagher, A.; Dagenais, L.; Doussau, A.; Décarie, J.C.; Materassi, M.; Gagnon, K.; Prud’homme, J.; Vobecky, S.; Poirier, N.; Carmant, L. Significant Motor Improvement in an Infant with Congenital Heart Disease and a Rolandic Stroke: The Impact of Early Intervention. Dev. Neurorehabil. 2017, 20, 165–168. [Google Scholar] [CrossRef]
- Snookes, S.H.; Gunn, J.K.; Eldridge, B.J.; Donath, S.M.; Hunt, R.W.; Galea, M.P.; Shekerdemian, L. A Systematic Review of Motor and Cognitive Outcomes After Early Surgery for Congenital Heart Disease. Pediatrics 2010, 125, e818–e827. [Google Scholar] [CrossRef]
- Darrah, J.; Redfern, L.; Maguire, T.O.; Beaulne, A.P.; Watt, J. Intra-Individual Stability of Rate of Gross Motor Development in Full-Term Infants. Early Hum. Dev. 1998, 52, 169–179. [Google Scholar] [CrossRef]
- Rollins, C.K.; Newburger, J.W.; Roberts, A.E. Genetic Contribution to Neurodevelopmental Outcomes in Congenital Heart Disease: Are Some Patients Predetermined to Have Developmental Delay? Curr. Opin. Pediatrics 2017, 29, 529. [Google Scholar] [CrossRef]
- Pierpont, M.E.; Brueckner, M.; Chung, W.K.; Garg, V.; Lacro, R.V.; McGuire, A.L.; Mital, S.; Priest, J.R.; Pu, W.T.; Roberts, A.; et al. Genetic Basis for Congenital Heart Disease: Revisited: A Scientific Statement from the American Heart Association. Circulation 2018, 138, e653–e711. [Google Scholar] [CrossRef] [PubMed]
- Gaynor, J.W.; Stopp, C.; Wypij, D.; Andropoulos, D.B.; Atallah, J.; Atz, A.M.; Beca, J.; Donofrio, M.T.; Duncan, K.; Ghanayem, N.S.; et al. Neurodevelopmental Outcomes After Cardiac Surgery in Infancy. Pediatrics 2015, 135, 816–825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hövels-Gürich, H.H. Factors Influencing Neurodevelopment after Cardiac Surgery during Infancy. Front. Pediatrics 2016, 4, 137. [Google Scholar] [CrossRef] [Green Version]
- Craig, A.A.; Adam, J.G. Bayley Scales of Infant and Toddler Development—Third Edition. San Antonio, TX: Harcourt Assessment. J. Psychoeduc. Assess. 2007, 25, 180–198. [Google Scholar] [CrossRef]
- Piper, M.C.; Pinnell, L.E.; Darrah, J.; Maguire, T.; Byrne, P.J. Construction and Validation of the Alberta Infant Motor Scale (AIMS). Proc. Can. J. Public Health 1992, 83, S46–S50. [Google Scholar]
- Harris, S.R.; Daniels, L.E. Reliability and Validity of the Harris Infant Neuromotor Test. J. Pediatrics 2001, 139, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Naef, N.; Wehrle, F.; Rousson, V.; Latal, B. Cohort and Individual Neurodevelopmental Stability between 1 and 6 Years of Age in Children with Congenital Heart Disease. J. Pediatrics 2019, 215, 83–89. [Google Scholar] [CrossRef]
- Roberts, H.; Needelman, H.; Duncan, K.; Hoskoppal, A.; Kugler, J. Neurodevelopmental Outcomes in Infants after Surgery for Congenital Heart Disease: A Comparison of Single-Ventricle vs. Two-Ventricle Physiology. Congenit. Heart Dis. 2010, 5, 90–95. [Google Scholar] [CrossRef]
- Mussatto, K.A.; Hoffmann, R.G.; Hoffman, G.M.; Tweddell, J.S.; Bear, L.; Cao, Y.; Brosig, C. Risk and Prevalence of Developmental Delay in Young Children with Congenital Heart Disease. Pediatrics 2014, 133, e570–e577. [Google Scholar] [CrossRef] [Green Version]
- Stegeman, R.; Sprong, M.C.A.; Breur, J.M.P.J.; Groenendaal, F.; Vries, L.S.; Haas, F.; Net, J.; Jansen, N.J.G.; Benders, M.J.N.L.; Claessens, N.H.P.; et al. Early Motor Outcomes in Infants with Critical Congenital Heart Disease Are Related to Neonatal Brain Development and Brain Injury. Dev. Med. Child Neurol. 2021, 64, 192–199. [Google Scholar] [CrossRef]
- Acton, B.V.; Biggs, W.S.G.; Creighton, D.E.; Penner, K.A.H.; Switzer, H.N.; Thomas, J.H.P.; Joffe, A.R.; Robertson, C.M.T. Overestimating Neurodevelopment Using the Bayley-III after Early Complex Cardiac Surgery. Pediatrics 2011, 128, e794–e800. [Google Scholar] [CrossRef] [PubMed]
- Andropoulos, D.B.; Ahmad, H.B.; Haq, T.; Brady, K.; Stayer, S.A.; Meador, M.R.; Hunter, J.V.; Rivera, C.; Voigt, R.G.; Turcich, M.; et al. The Association between Brain Injury, Perioperative Anesthetic Exposure, and 12-Month Neurodevelopmental Outcomes after Neonatal Cardiac Surgery: A Retrospective Cohort Study. Paediatr. Anaesth. 2014, 24, 266–274. [Google Scholar] [CrossRef] [PubMed]
- Meuwly, E.; Feldmann, M.; Knirsch, W.; von Rhein, M.; Payette, K.; Dave, H.; Tuura, R.O.G.; Kottke, R.; Hagmann, C.; Latal, B.; et al. Postoperative Brain Volumes Are Associated with One-Year Neurodevelopmental Outcome in Children with Severe Congenital Heart Disease. Sci. Rep. 2019, 9, 10885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheatham, S.L.; Carey, H.; Chisolm, J.L.; Heathcock, J.C.; Steward, D. Early Results of Neurodevelopment Following Hybrid Stage I for Hypoplastic Left Heart Syndrome. Pediatric Cardiol. 2015, 36, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Khalid, O.M.; Harrison, T.M. Early Neurodevelopmental Outcomes in Children with Hypoplastic Left Heart Syndrome and Related Anomalies After Hybrid Procedure. Pediatric Cardiol. 2019, 40, 1591–1598. [Google Scholar] [CrossRef] [PubMed]
- Bjarnason-Wehrens, B.; Schmitz, S.; Dordel, S. Motor Development in Children with Congenital Cardiac Diseases. Eur. Cardiol. Rev. 2008, 4, 92. [Google Scholar] [CrossRef]
- McCrindle, B.W.; Williams, R.V.; Mital, S.; Clark, B.J.; Russell, J.L.; Klein, G.; Eisenmann, J.C. Physical Activity Levels in Children and Adolescents Are Reduced after the Fontan Procedure, Independent of Exercise Capacity, and Are Associated with Lower Perceived General Health. Arch. Dis. Child. 2007, 92, 509–514. [Google Scholar] [CrossRef] [Green Version]
- Long, S.H.; Galea, M.P.; Eldridge, B.J.; Harris, S.R. Performance of 2-Year-Old Children after Early Surgery for Congenital Heart Disease on the Bayley Scales of Infant and Toddler Development, Third Edition. Early Hum. Dev. 2012, 88, 603–607. [Google Scholar] [CrossRef]
- Steenis, L.J.P.; Verhoeven, M.; Hessen, D.J.; Van Baar, A.L. Performance of Dutch Children on the Bayley III: A Comparison Study of US and Dutch Norms. PLoS ONE 2015, 10, e0132871. [Google Scholar] [CrossRef]
- Mendonça, B.; Sargent, B.; Fetters, L. Cross-Cultural Validity of Standardized Motor Development Screening and Assessment Tools: A Systematic Review. Dev. Med. Child Neurol. 2016, 58, 1213–1222. [Google Scholar] [CrossRef]
- Li, X.; Robertson, C.M.T.; Yu, X.; Cheypesh, A.; Dinu, I.A.; Li, J. Early Postoperative Systemic Inflammatory Response Is an Important Determinant for Adverse 2-Year Neurodevelopment-Associated Outcomes after the Norwood Procedure. J. Thorac. Cardiovasc. Surg. 2014, 148, 202–206. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aly, S.A.; Zurakowski, D.; Glass, P.; Skurow-Todd, K.; Jonas, R.A.; Donofrio, M.T. Cerebral Tissue Oxygenation Index and Lactate at 24 Hours Postoperative Predict Survival and Neurodevelopmental Outcome after Neonatal Cardiac Surgery. Congenit. Heart Dis. 2017, 12, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Dagenais, L.; Materassi, M.; Desnous, B.; Vinay, M.C.; Doussau, A.; Sabeh, P.; Prud’homme, J.; Gagnon, K.; Lenoir, M.; Charron, M.A.; et al. Superior Performance in Prone in Infants with Congenital Heart Disease Predicts an Earlier Onset of Walking. J. Child Neurol. 2018, 33, 894–900. [Google Scholar] [CrossRef] [PubMed]
- Limperopoulos, C.; Majnemer, A.; Shevell, M.I.; Rohlicek, C.; Rosenblatt, B.; Tchervenkov, C.; Darwish, H.Z. Predictors of Developmental Disabilities after Open Heart Surgery in Young Children with Congenital Heart Defects. J. Pediatrics 2002, 141, 51–58. [Google Scholar] [CrossRef] [PubMed]
- Bellinger, D.C.; Jonas, R.A.; Rappaport, L.A. Developmental and Neurologic Status of Children after Heart Surgery with Hypothermic Circulatory Arrest or Low-Flow Cardiopulmonary Arrest. J. Neurosurg. Anesthesiol. 2007, 7, 196. [Google Scholar] [CrossRef]
- Sarajuuri, A.; Jokinen, E.; Puosi, R.; Mildh, L.; Mattila, I.; Lano, A.; Lönnqvist, T. Neurodevelopment in Children with Hypoplastic Left Heart Syndrome. J. Pediatrics 2010, 157, 414–420. [Google Scholar] [CrossRef]
- Ravishankar, C.; Zak, V.; Williams, I.A.; Bellinger, D.C.; Gaynor, J.W.; Ghanayem, N.S.; Krawczeski, C.D.; Licht, D.J.; Mahony, L.; Newburger, J.W.; et al. Association of Impaired Linear Growth and Worse Neurodevelopmental Outcome in Infants with Single Ventricle Physiology: A Report from the Pediatric Heart Network Infant Single Ventricle Trial. J. Pediatrics 2013, 162, 250–256. [Google Scholar] [CrossRef] [Green Version]
- Peyvandi, S.; Chau, V.; Guo, T.; Xu, D.; Glass, H.C.; Synnes, A.; Poskitt, K.; Barkovich, A.J.; Miller, S.P.; McQuillen, P.S. Neonatal Brain Injury and Timing of Neurodevelopmental Assessment in Patients with Congenital Heart Disease. J. Am. Coll. Cardiol. 2018, 71, 1986–1996. [Google Scholar] [CrossRef]
- Claessens, N.H.P.; Moeskops, P.; Buchmann, A.; Latal, B.; Knirsch, W.; Scheer, I.; Išgum, I.; de Vries, L.S.; Benders, M.J.N.L.; von Rhein, M. Delayed Cortical Gray Matter Development in Neonates with Severe Congenital Heart Disease. Pediatric Res. 2016, 80, 668–674. [Google Scholar] [CrossRef]
- Von Rhein, M.; Dimitropoulos, A.; Valsangiacomo Buechel, E.R.; Landolt, M.A.; Latal, B. Risk Factors for Neurodevelopmental Impairments in School-Age Children after Cardiac Surgery with Full-Flow Cardiopulmonary Bypass. J. Thorac. Cardiovasc. Surg. 2012, 144, 577–583. [Google Scholar] [CrossRef] [Green Version]
- Ridgway, C.L.; Ong, K.K.; Tammelin, T.H.; Sharp, S.; Ekelund, U.; Jarvelin, M.R. Infant Motor Development Predicts Sports Participation at Age 14 Years: Northern Finland Birth Cohort of 1966. PLoS ONE 2009, 4, e6837. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, R.; Hillman, C.; Arent, S.; Petitpas, A. Physical Activity: An Underestimated Investment in Human Capital? J. Phys. Act. Health 2013, 10, 289–308. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Udholm, S.; Aldweib, N.; Hjortdal, V.E.; Veldtman, G.R. Prognostic Power of Cardiopulmonary Exercise Testing in Fontan Patients: A Systematic Review. Open Heart 2018, 5, e000812. [Google Scholar] [CrossRef] [PubMed]
- King-Dowling, S.; Proudfoot, N.A.; Cairney, J.; Timmons, B.W. Motor Competence, Physical Activity, and Fitness across Early Childhood. Med. Sci. Sport. Exerc. 2020, 52, 2342–2348. [Google Scholar] [CrossRef] [PubMed]
- Barnett, L.M.; van Beurden, E.; Morgan, P.J.; Brooks, L.O.; Beard, J.R. Childhood Motor Skill Proficiency as a Predictor of Adolescent Physical Activity. J. Adolesc. Health 2009, 44, 252–259. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Characteristics and Clinical Data | Total (n = 215) |
|---|---|
| Male | 136 (63) |
| Birth weight, gram | 3422 ± 564 |
| Gestational age, weeks | 39.4 ± 1.34 |
| Apgar score 5 min | 8.8 ± 1.2 |
| Prenatal diagnosis | 147 (69) |
| Balloon Atrioseptostomy (BAS) | 59 (27) |
| Age at surgery (days) | 9 (7–21) |
| Total intubation duration pre/per/post-surgery (hours) | 99 (47–195) |
| Aortic Cross Clamp (ACC) time (minutes) | 79 (62–97) |
| Cardio Pulmonary Bypass (CPB) time (minutes) | 136 (108–167) |
| Low-Cardiac-Output Syndrome (LCOS) pre-surgery | 25 (12) |
| Low-Cardiac-Output Syndrome (LCOS) post-surgery | 44 (21) |
| Length of hospital stay (days) | 19 (14–28) |
| Intensive-Care-Unit stay (days) | 9 (5–14) |
| Cardiac Diagnosis | |
| Transposition of Great Arteries (TGA) | 94 (44) |
| Congenital Corrected TGA (ccTGA) | 1 (1) |
| Tetralogy of Fallot (TOF) | 39 (18) |
| Single-Ventricle Physiology (SVP) | 40 (19) |
| Truncus Arteriosus | 3 (1) |
| Hypoplastic Left-Heart Complex | 9 (4) |
| Aortic arch pathology | 20 (9) |
| Total Anomalous Pulmonary Venous Connection (TAPVC) | 5 (2) |
| Others | 4 (2) |
| Age at follow up 3 (months) | 3.3 (3.0–3.6) |
| Age at follow up 9 (months) | 9.6 (9.0–10.4) |
| Age at follow up 18 (months) | 18.9 (18.1–19.6) |
| Total | SVP | TGA | TOF | AAP | p-Value | |
|---|---|---|---|---|---|---|
| 3 months | n = 165 | n = 25 | n = 88 | n = 21 | n = 15 | |
| Bayley-III | ||||||
| Motor composite score | 96.6 (13.3) | 93.8 (13.0) | 97.9 (12.4) | 96.8 (13.5) | 100.8 (14.9) | 0.055 |
| Fine motor scaled score | 9.4 (2.9) | 8.8 (2.7) | 9.5 (2.8) | 10.1 (3.3) | 10 (2.8) | 0.130 |
| Gross motor scaled score | 9.2 (2.7) | 8.7 (2.8) | 9.6 (2.6) | 8.7 (2.2) | 9.9 (3.1) | 0.063 |
| PDI ≤ −2 SD | 4 (2.4) | 1 (4) | 1 (1.1) | 0 (0) | 0 (0) | |
| FM SS ≤ −2 SD | 5 (3) | 1 (4) | 1 (1.1) | 1 (4.5) | 0 (0) | |
| GM SS ≤ −2 SD | 11 (6.7) | 2 (8) | 5 (5.7) | 1 (4.8) | 1 (6.7) | |
| Discrepancy GM < FM | 28 (17) | 4 (16) | 14 (15.9) | 6 (28,6) | 3 (20) | |
| 9 months | n = 188 | n = 36 | n = 88 | n = 34 | n = 12 | |
| Bayley-III | ||||||
| Motor composite score * | 98.3 (11.6) | 91.2 (12.3) | 100.6 (10.4) | 99.5 (11.1) | 102.1 (9.7) | 0.001 * |
| Fine motor scaled score * | 10.47 (1.6) | 9.9 (1.6) | 10.5 (1.4) | 10.9 (1.7) | 11.6 (1.6) | 0.046 * |
| Gross motor scaled score * | 8.7 (3.2) | 6.8 (3.5) | 9.4 (3.0) | 8.6 (2.9) | 8.8 (2.8) | 0.001 * |
| PDI ≤ −2 SD | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| FM SS ≤ −2 SD | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| GM SS ≤ −2 SD | 22 (11.7) | 11 (30.6) | 5 (5.7) | 2 (5.9) | 1 (8.3) | |
| Discrepancy GM < FM | 57 (30.3) | 19 (52.8) | 19 (21.6) | 9 (26.5) | 6 (50) | |
| 18 months | n = 171 | n = 31 | n = 80 | n = 33 | n = 12 | |
| Bayley-III | ||||||
| Motor composite score * | 103.6 (12.7) | 93.2 (14.9) | 106.61 (11.1) | 105.9 (9.7) | 105.4 (11.3) | <0.000 * |
| Fine motor scaled score * | 11.20 (2.0) | 9.9 (2.5) | 11.44 (1.6) | 11.6 (1.7) | 11.9 (2.4) | 0.002 * |
| Gross motor scaled score * | 9.7 (3.3) | 7.45 (3.7) | 10.63 (3.1) | 10.2 (2.8) | 9.6 (2.6) | 0.001 * |
| PDI ≤ −2 SD | 4 (2.3) | 4 (12.9) | 0 (0) | 0 (0) | 0 (0) | |
| FM SS ≤ −2 SD | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| GM SS ≤ −2 SD | 21 (12.2) | 10 (32.3) | 5 (6.3) | 2 (6.1) | 1 (8.3) | |
| Discrepancy GM < FM | 43 (25.3) | 12 (38.7) | 15 (18.8) | 8 (25) | 3 (25) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sprong, M.C.A.; van Brussel, M.; de Vries, L.S.; van der Net, J.; Nijman, J.; Breur, J.M.P.J.; Slieker, M.G. Longitudinal Motor-Developmental Outcomes in Infants with a Critical Congenital Heart Defect. Children 2022, 9, 570. https://0-doi-org.brum.beds.ac.uk/10.3390/children9040570
Sprong MCA, van Brussel M, de Vries LS, van der Net J, Nijman J, Breur JMPJ, Slieker MG. Longitudinal Motor-Developmental Outcomes in Infants with a Critical Congenital Heart Defect. Children. 2022; 9(4):570. https://0-doi-org.brum.beds.ac.uk/10.3390/children9040570
Chicago/Turabian StyleSprong, Maaike C. A., Marco van Brussel, Linda S. de Vries, Janjaap van der Net, Joppe Nijman, Johannes M. P. J. Breur, and Martijn G. Slieker. 2022. "Longitudinal Motor-Developmental Outcomes in Infants with a Critical Congenital Heart Defect" Children 9, no. 4: 570. https://0-doi-org.brum.beds.ac.uk/10.3390/children9040570