
The Most Common Location of Schools with Viral Upper Respiratory Tract Infection Clusters in Taiwan, 2011–2019

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Policy
2.2. Definition of Confirmed Cases
2.3. Data Source
2.4. Data Analysis
3. Results
4. Discussion
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Nayak, J.; Hoy, G.; Gordon, A. Influenza in Children. Cold Spring Harb Perspect Med. 2021, 11, a038430. [Google Scholar] [CrossRef] [PubMed]
- Flu & Young Children, CDC, USA. 2022. Available online: https://www.cdc.gov/flu/highrisk/children.htm (accessed on 1 March 2022).
- Mandell, G.L.; Bennett, J.E.; Dolin, R. Principles and Practice of Infectious Diseases, 8th ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2015; pp. 2000–2024.e6. [Google Scholar]
- Paules, C.; Subbarao, K. Influenza. Lancet 2017, 390, 697–708. [Google Scholar] [CrossRef]
- U.S. Centers for Disease Control and Prevention, National Center for Prevention Services. Epidemiology and Prevention of Vaccine-Preventable Diseases: Influenza, 13th ed.; U.S. Department of Health and Human Services: Washington, DC, USA, 2015; Volume 12, pp. 187–208.
- Lee, C.W.; Tai, Y.L.; Huang, L.M.; Chi, H.; Huang, F.Y.; Chiu, N.C.; Huang, C.Y.; Tu, Y.H.; Wang, J.Y.; Huang, D.T. Efficacy of clarithromycin-naproxen-oseltamivir combination therapy versus oseltamivir alone in hospitalized pediatric influenza patients. J. Microbiol. Immunol. Infect. 2021, 54, 876–884. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, K.G.; Wood, J.M.; Zambon, M. Influenza. Lancet 2003, 362, 1733–1745. [Google Scholar] [CrossRef]
- U.S. Centers for Disease Control and Prevention. Prevention and Control of Influenza. Recommendations of the Advisory Committee on Immunization Practices (ACIP). Morb. Mortal. Wkly. Rep. Recomm. Rep. 2006, 55, 1–42. [Google Scholar]
- Asha, K.; Kumar, B. Emerging Influenza D Virus Threat: What We Know So Far! J. Clin. Med. 2019, 8, 192. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. Influenza Type A Viruses and Subtypes. 2013. Available online: http://www.cdc.gov/flu/avianflu/influenza-a-virus-subtypes.htm (accessed on 1 March 2022).
- Centers for Disease Control and Prevention: Types of Influenza Viruses. Available online: http://www.cdc.gov/flu/about/viruses/types.htm (accessed on 1 March 2022).
- Ziegler, T.; Mamahit, A.; Cox, N.J. 65 years of influenza surveillance by a World Health Organization-coordinated global network. Influenza Other Respir Viruses 2018, 12, 558–565. [Google Scholar] [CrossRef] [PubMed]
- Statistics of Communicable Diseases and Surveillance Report, Taiwan: Taiwan Centers for Disease Control. Available online: https://www.cdc.gov.tw/InfectionReport/List/DRiONFTwYxu8T162Hm6yFw (accessed on 1 March 2022).
- Lin, F.H.; Chou, Y.C.; Chen, B.C.; Lu, J.C.; Liu, C.J.; Hsieh, C.J.; Yu, C.P. An Increased Risk of School-Aged Children with Viral Infection among Diarrhea Clusters in Taiwan during 2011–2019. Children 2021, 8, 807. [Google Scholar] [CrossRef] [PubMed]
- Lin, F.H.; Chen, B.C.; Chou, Y.C.; Hsieh, C.J.; Yu, C.P. Incidence and Risk Factors for Notifiable Typhoid and Paratyphoid in Taiwan during the Period 2011–2020. Healthcare 2021, 9, 1316. [Google Scholar] [CrossRef] [PubMed]
- University Cambridge, School of the Biological Sciences. Some Studies that Do Not Require Ethical Approval Include Those Involving Information Freely Available in the Public Domain. 2020. Available online: https://www.bio.cam.ac.uk/psyres/approval (accessed on 1 March 2022).
- Number of Respiratory Viruses Isolates, Taiwan: Taiwan Centers for Disease Control. Available online: https://nidss.cdc.gov.tw/Home/Index?op=2 (accessed on 15 December 2019).
- Communicable Disease Control Act. Taiwan Centers for Disease Control. 2022. Available online: https://law.moj.gov.tw/ENG/LawClass/LawAll.aspx?pcode=L0050001 (accessed on 1 March 2022).
- Statistics of Communicable Diseases and Surveillance Report. Taiwan Centers for Disease Control. 2022. Available online: https://www.cdc.gov.tw/InfectionReport/Info/DRiONFTwYxu8T162Hm6yFw?infoId=pbOn-dfpv6agFdaCxkzGDQ (accessed on 1 March 2022).
- Boktor, S.W.; Hafner, J.W. Influenza. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Chen, H.L.; Hsu, S.T.; Chen, C.M. Taiwan Centers for Disease Control. 2022. Available online: https://www.cdc.gov.tw/Uploads/archives/b32df17c-133d-488d-9a1d-91a9f8859a29.pdf (accessed on 1 March 2022).
- Kleynhans, J.; Treurnicht, F.K.; Cohen, C.; Vedan, T.; Seleka, M.; Maki, L.; von Gottberg, A.; McCarthy, K.; Ramkrishna, W.; McMorrow, M.; et al. Outbreak of influenza a in a boarding school in South Africa, 2016. Pan Afr. Med. J. 2019, 33, 42. [Google Scholar] [CrossRef] [PubMed]
- Tramuto, F.; Restivo, V.; Costantino, C.; Colomba, G.M.E.; Maida, C.M.; Casuccio, A.; Vitale, F. Surveillance Data for Eight Consecutive Influenza Seasons in Sicily, Italy. Am. J. Trop. Med. Hyg. 2019, 101, 1232–1239. [Google Scholar] [CrossRef] [PubMed]
- Doi, I.; Nagata, N.; Tsukagoshi, H.; Komori, H.; Motoya, T.; Watanabe, M.; Keta, T.; Kawakami, M.; Tsukano, T.; Honda, M.; et al. An outbreak of acute respiratory infections due to human respiratory syncytial virus in a nursing home for the elderly in Ibaraki, Japan, 2014. Jpn. J. Infect. Dis. 2014, 67, 326–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, L.; van der Hoek., W.; Krafft, T.; Pilot, E.; Asten, L.V.; Lin, G.; Wu, S.; Duan, W.; Yang, P.; Wang, Q. Influenza vaccine effectiveness estimates against influenza A(H3N2) and A(H1N1) pdm09 among children during school-based outbreaks in the 2016–2017 season in Beijing, China. Hum. Vaccines Immunother. 2019, 16, 816–822. [Google Scholar] [CrossRef] [PubMed]
- Kodama, F.; Nace, D.A.; Jump, R.L.P. Respiratory Syncytial Virus and Other Noninfluenza Respiratory Viruses in Older Adults. Infect. Dis. Clin. North Am. 2017, 31, 767–790. [Google Scholar] [CrossRef] [PubMed]
- Prasad, R.; Mohanakumari, V.V.; Sasi, R.V.; Nair, R.; Jones, S.; Pillai, M.R. Complete Genome Analysis of Influenza A(H1N1) Viruses Isolated in Kerala, India. Microbiol. Resour Announc. 2020, 9, e00062-20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Owuor, D.C.; Ngoi, J.M.; Otieno, J.R.; Otieno, G.P.; Nyasimi, F.M.; Nyiro, J.U.; Agoti, C.N.; Chaves, S.S.; Nokes, D.J. Genetic characterization of influenza A(H3N2) viruses circulating in coastal Kenya, 2009–2017. Influenza Other Respir Viruses 2020, 14, 320–330. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.; Cui, H.; Wang, Z.; Dong, S.; Zhang, C.; Li, J.; Meng, K.; Sun, Y.; Liu, J.; Guo, Z.; et al. Pathogenicity and transmissibility assessment of two strains of human influenza virus isolated in China in 2018. J. Int. Med. Res. 2021, 49, 300060520982832. [Google Scholar] [CrossRef] [PubMed]
- An Influenza-Like Cluster Event Occurred in a Military School in Kaohsiung City. Available online: https://khd.kcg.gov.tw/tw/department/news-show.php?num=1751&page=1&zone=2&author=98 (accessed on 1 March 2022).




{kind=link}
{kind=link}
{kind=link}
| Pathogens | Year | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2011 n = 76 | 2012 n = 72 | 2013 n = 118 | 2014 n = 154 | 2015 n = 178 | 2016 n = 166 | 2017 n = 358 | 2018 n = 255 | 2019 n = 487 | 2011–2019 n = 1864 | |
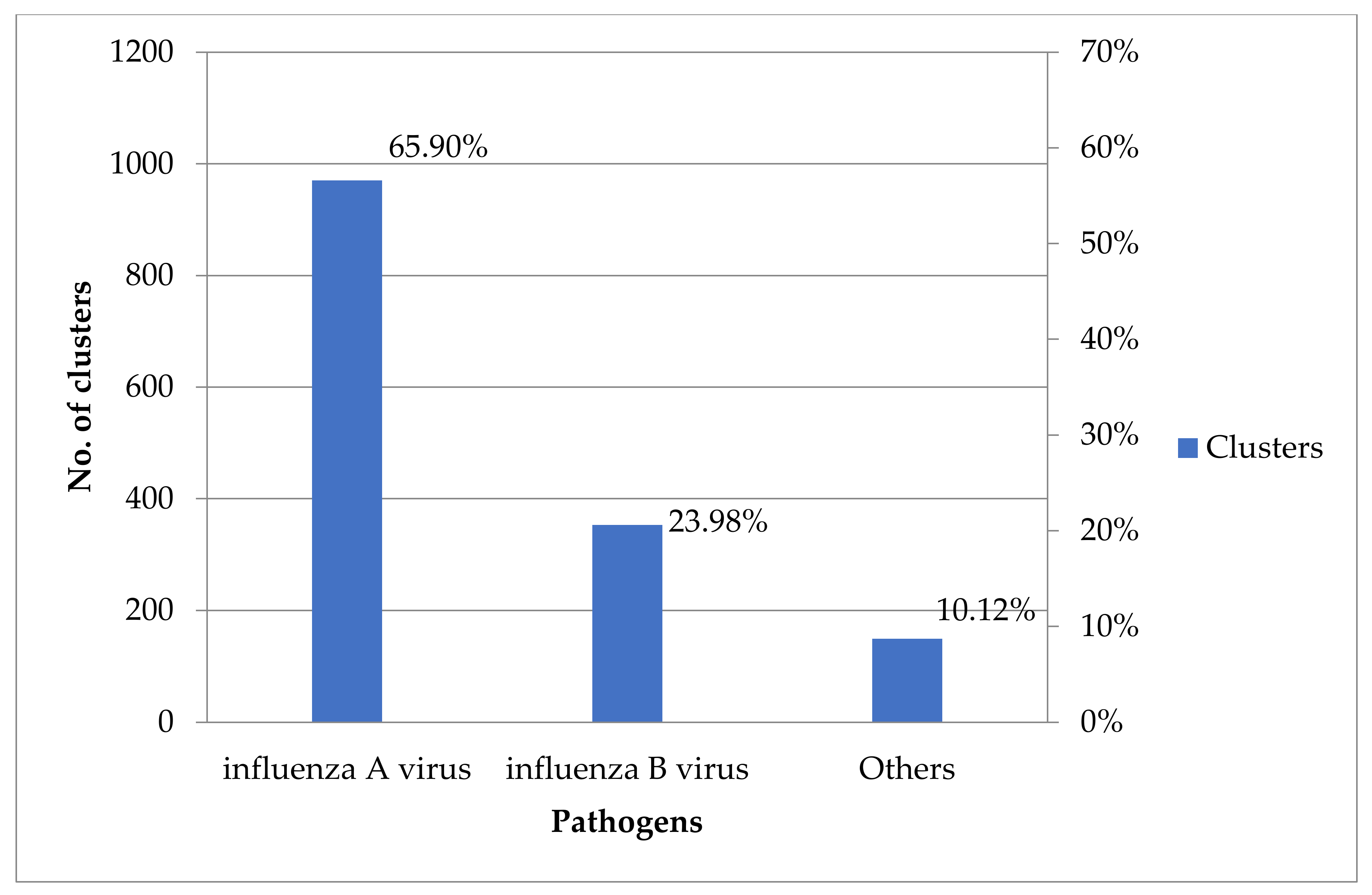
| Single influenza A virus | ||||||||||
| Influenza A (H1N1) virus | 14 | 5 | 30 | 17 | 16 | 43 | 5 | 16 | 75 | 221 |
| Influenza A (H3N2) virus | 1 | 31 | 34 | 21 | 95 | 30 | 200 | 76 | 58 | 546 |
| Influenza A virus—RIDTs analysis | 0 | 0 | 0 | 0 | 4 | 2 | 34 | 23 | 107 | 170 |
| Single influenza B virus | ||||||||||
| Influenza B virus | 26 | 9 | 1 | 48 | 26 | 13 | 32 | 41 | 72 | 268 |
| Influenza B virus—RIDTs analysis | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 10 | 45 | 57 |
| Mixed Influenza virus | ||||||||||
| Influenza A (H1N1) virus + Influenza A (H3N2) virus | 0 | 1 | 0 | 1 | 0 | 1 | 0 | 1 | 1 | 5 |
| Influenza A (H1N1) virus + Influenza B virus | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 3 |
| Influenza A (H3N2) virus + Influenza B virus | 1 | 0 | 0 | 2 | 1 | 0 | 6 | 1 | 1 | 12 |
| Influenza A virus—RIDTs analysis + Influenza B virus—RIDTs analysis | 0 | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 11 | 13 |
| Other pathogens | 14 | 5 | 15 | 13 | 8 | 20 | 28 | 31 | 15 | 149 |
| Routine test—pathogens not detected | 15 | 14 | 27 | 49 | 25 | 56 | 38 | 52 | 65 | 341 |
| Sample not collected | 4 | 7 | 11 | 3 | 3 | 0 | 10 | 4 | 37 | 79 |
| Pathogens | Year | p | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2011 n = 57 | 2012 n = 51 | 2013 n = 80 | 2014 n = 102 | 2015 n = 150 | 2016 n = 110 | 2017 n = 310 | 2018 n = 199 | 2019 n = 385 | ||
| Single influenza A virus | 15 | 36 | 64 | 38 | 115 | 75 | 239 | 115 | 240 | <0.001 |
| Single influenza B virus | 26 | 9 | 1 | 48 | 26 | 13 | 34 | 51 | 117 | |
| Mixed influenza virus | 2 | 1 | 0 | 3 | 1 | 2 | 9 | 2 | 13 | |
| a Other pathogens | 14 | 5 | 15 | 13 | 8 | 20 | 28 | 31 | 15 | |
| Pathogens | Year | p | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2011 n = 14 | 2012 n = 5 | 2013 n = 15 | 2014 n = 13 | 2015 n = 8 | 2016 n = 20 | 2017 n = 28 | 2018 * n = 22 | 2019 n = 15 | ||
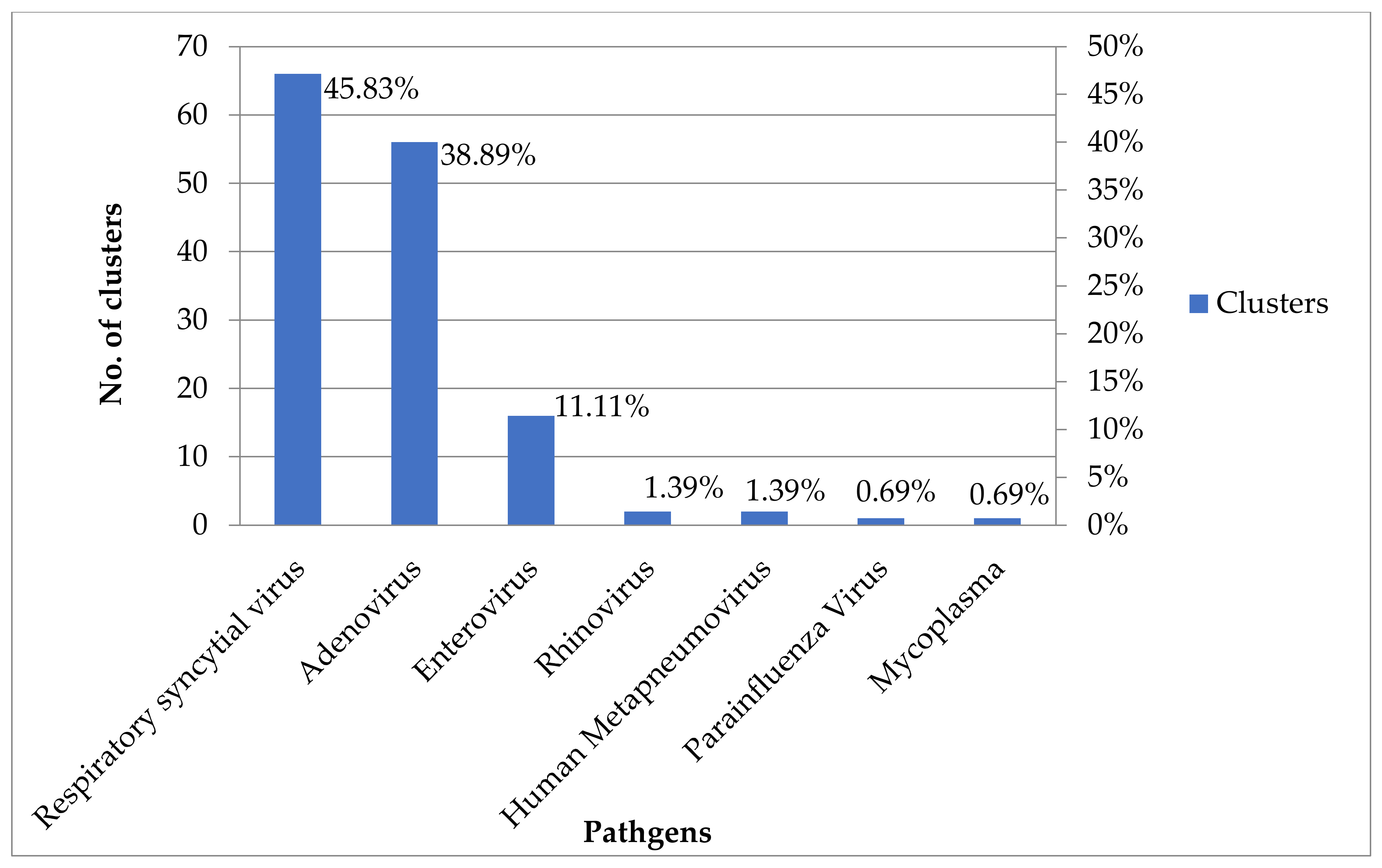
| Respiratory Syncytial Virus | 4 | 2 | 10 | 6 | 5 | 11 | 10 | 8 | 8 | 0.01 |
| Adenovirus | 6 | 2 | 3 | 5 | 1 | 5 | 15 | 11 | 6 | |
| Enterovirus | 2 | 0 | 2 | 0 | 2 | 2 | 3 | 3 | 1 | |
| Rhinovirus | 0 | 0 | 0 | 2 | 0 | 0 | 0 | - | 0 | |
| Adenovirus + Respiratory Syncytial Virus | 1 | 0 | 0 | 0 | 0 | 0 | 0 | - | 0 | |
| Enterovirus + Respiratory Syncytial Virus | 0 | 1 | 0 | 0 | 0 | 0 | 0 | - | 0 | |
| Human Metapneumovirus | 0 | 0 | 0 | 0 | 0 | 1 | 0 | - | 0 | |
| Adenovirus + Human Metapneumovirus | 0 | 0 | 0 | 0 | 0 | 1 | 0 | - | 0 | |
| Parainfluenza Virus + Mycoplasma | 1 | 0 | 0 | 0 | 0 | 0 | 0 | - | 0 | |
| InstitutionCategories | Year | p | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| 2011 n = 76 | 2012 n = 72 | 2013 n = 118 | 2014 n = 154 | 2015 n = 178 | 2016 n = 166 | 2017 n = 358 | 2018 n = 255 | 2019 n = 487 | ||
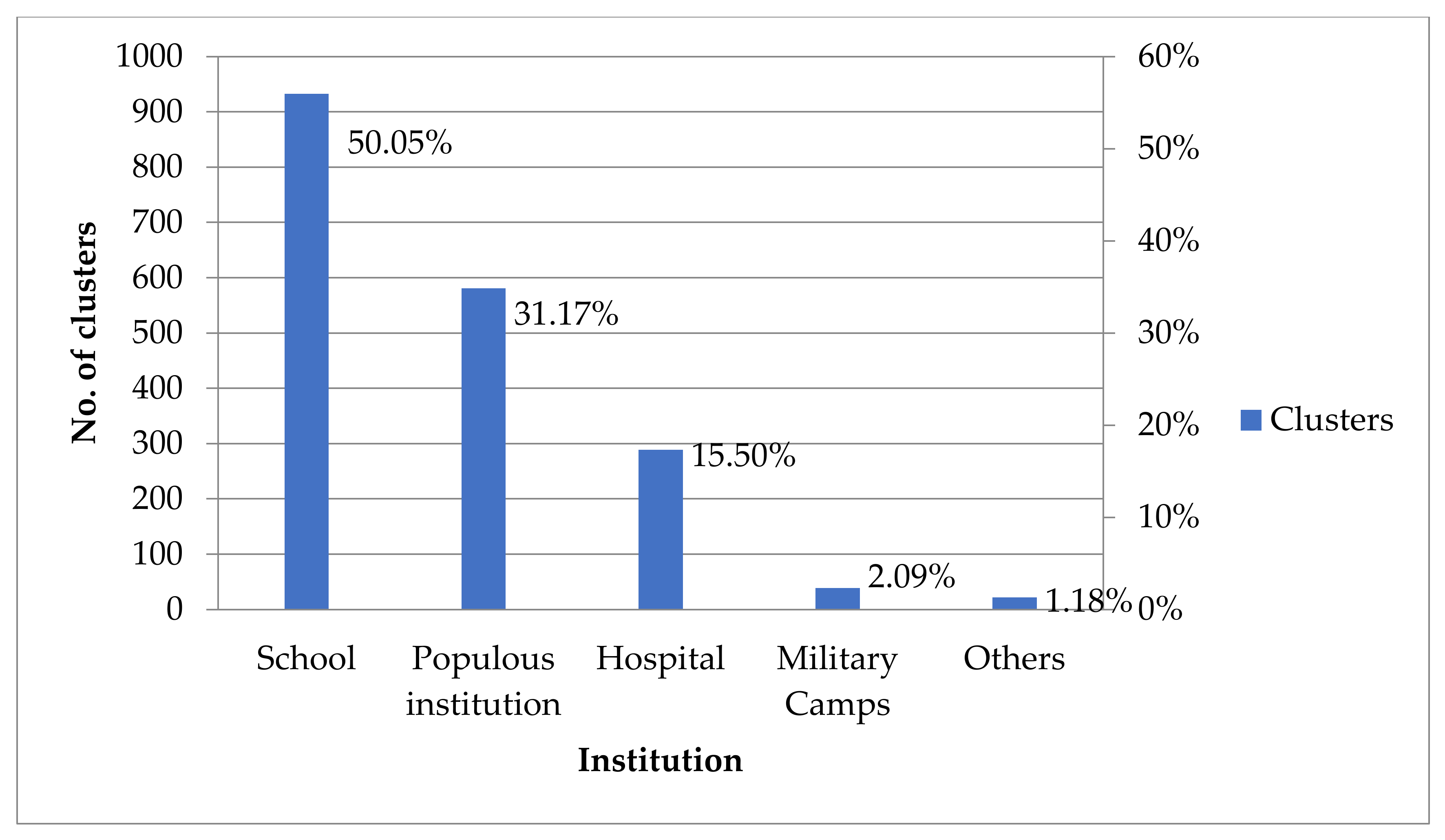
| Schools | 38 | 11 | 64 | 89 | 62 | 38 | 165 | 127 | 339 | <0.001 |
| Populous institutions | 24 | 37 | 37 | 37 | 70 | 64 | 135 | 86 | 91 | |
| Hospitals | 8 | 18 | 12 | 25 | 38 | 61 | 45 | 38 | 44 | |
| Military camps | 4 | 3 | 2 | 2 | 6 | 3 | 8 | 2 | 9 | |
| Others a | 2 | 3 | 3 | 1 | 2 | 0 | 5 | 2 | 4 | |
| Variables | Year | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | |
| Influenza A virus | |||||||||
| HIN1 | |||||||||
| A/California/07/2009 | √ | √ | √ | √ | √ | √ | √ | ||
| A/Michigan/45/2015 | √ | √ | √ | ||||||
| A/Brisbane/02/2018 | √ | ||||||||
| H3N2 | |||||||||
| A/Perth/16/2009 | √ | ||||||||
| A/Victoria/361/2011 | √ | √ | |||||||
| A/Texas/50/2012 | √ | √ | |||||||
| A/Switzerland/9715293/2013 | √ | √ | |||||||
| A/Hong Kong/4801/2014 | √ | √ | √ | √ | |||||
| A/Switzerland/9715293/2013 | √ | ||||||||
| A/Singapore/INFIMH-16–0019/2016 | √ | √ | √ | ||||||
| A/Switzerland/8060/2017 | √ | √ | |||||||
| Influenza B virus | |||||||||
| B/Brisbane/60/2008 (B/Vic) | √ | √ | √ | √ | √ | √ | √ | √ | |
| B/Florida/4/2006 (B/Yam) | √ | ||||||||
| B/Malaysia/2506/2004 (B/Vic) | √ | ||||||||
| B/Wisconsin/01/2010 (B/Yam) | √ | √ | √ | ||||||
| B/Massachusetts/02/2012 (B/Yam) | √ | √ | √ | √ | √ | √ | |||
| B/PHUKET/3073/2013 (B/Yam) | √ | √ | √ | √ | √ | √ | |||
| B/Colorado/06/2017 (B/Vic) | √ | ||||||||
| B/Colorado/06/2017 (B/Vic) | √ | ||||||||
| B/Washington/02/2019 (B/Vic) | √ | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lin, F.-H.; Chou, Y.-C.; Chien, W.-C.; Chung, C.-H.; Hsieh, C.-J.; Yu, C.-P. The Most Common Location of Schools with Viral Upper Respiratory Tract Infection Clusters in Taiwan, 2011–2019. Children 2022, 9, 720. https://0-doi-org.brum.beds.ac.uk/10.3390/children9050720
Lin F-H, Chou Y-C, Chien W-C, Chung C-H, Hsieh C-J, Yu C-P. The Most Common Location of Schools with Viral Upper Respiratory Tract Infection Clusters in Taiwan, 2011–2019. Children. 2022; 9(5):720. https://0-doi-org.brum.beds.ac.uk/10.3390/children9050720
Chicago/Turabian StyleLin, Fu-Huang, Yu-Ching Chou, Wu-Chien Chien, Chi-Hsiang Chung, Chi-Jeng Hsieh, and Chia-Peng Yu. 2022. "The Most Common Location of Schools with Viral Upper Respiratory Tract Infection Clusters in Taiwan, 2011–2019" Children 9, no. 5: 720. https://0-doi-org.brum.beds.ac.uk/10.3390/children9050720