Understanding the EMR-Related Experiences of Pregnant Japanese Women to Redesign Antenatal Care EMR Systems

 , , , , ,
, , , , , 
Abstract
:1. Introduction
- RQ1: What are the current EMR-related experiences of pregnant Japanese women?
- RQ2: What are the ideal EMR-related experiences for pregnant Japanese women?
- RQ3: How important are the different EMR-related experiences for pregnant Japanese women?
1.1. Background—Antenatal Care
1.2. Background—Antenatal Care in Japan
1.3. Background—General Overview of EMR Systems in Examination Rooms
1.4. Background—Patient Attitudes towards EMR Systems
1.5. Background—EMR Systems in Japanese Antenatal Care Settings
2. Materials and Methods
2.1. Field-Based Observational Study
2.1.1. Data Collection
2.1.2. Data Analysis
- Familiarization with the data: the researchers went through the data multiple times to gain a deeper understanding and familiarize themselves with it.
- Coding the data: after becoming familiar with the data, the researchers generated an initial set of codes. The codes were then associated with different parts of the notes. The coding process was repeated over three iterations during which the codes were extended and refined.
- Searching for the themes: at this stage, the researchers refocused the analysis on a broader level and extracted several themes by combining several codes together.
- Reviewing the themes: once the initial set of themes was identified, the researchers merged some themes together and discarded the themes that had little data associated with them.
- Defining and naming the themes: the themes were finally named and clearly defined in terms of EMR-related experiences.
- Producing the report: the resulting EMR-related experiences are presented in the results section.
2.2. Web Survey
- Currently, how much are pregnant Japanese women experiencing it?
- Ideally, how much or how would pregnant Japanese women want to experience it?
- How important is this EMR-related experience to pregnant Japanese women?
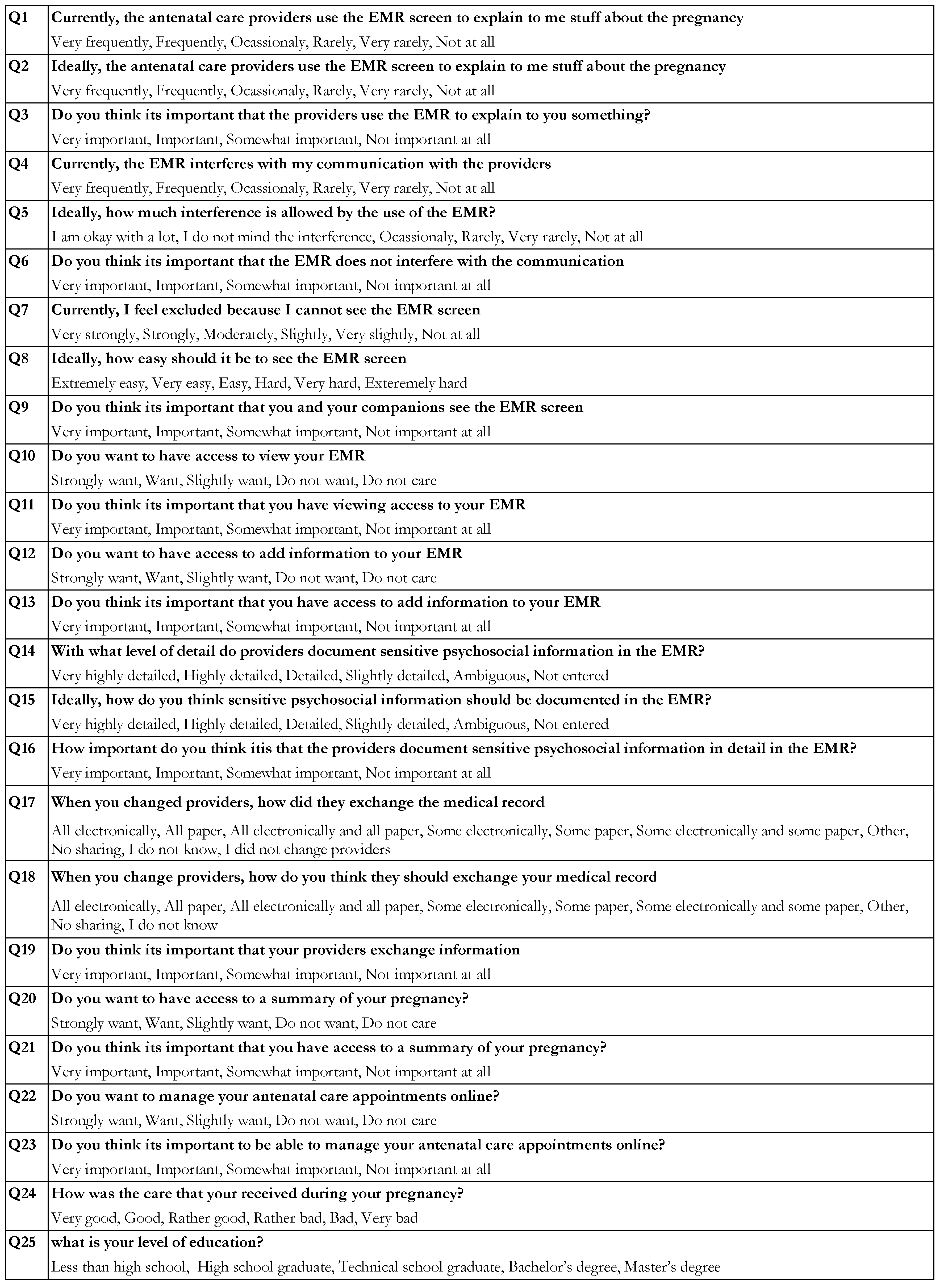
2.2.1. Web Survey Design
- The current frequency of the experience.
- The ideal frequency of the experience.Answers to these types of questions were reported on a 6-point Likert-type frequency scale, with 1 being the high end and 6 being the low end.
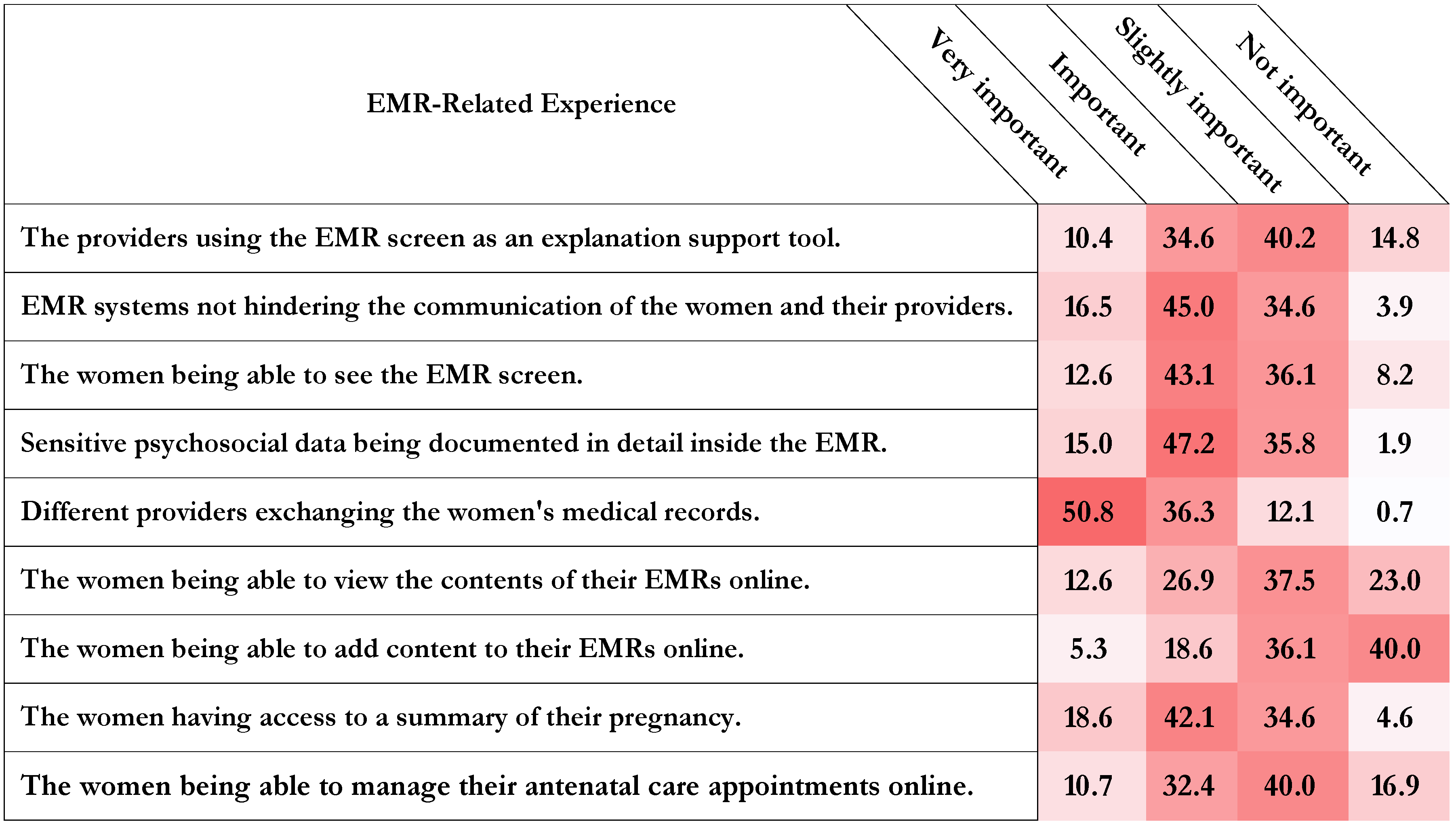
- The importance of the experience to them.Answers to this type of question were reported on the following scale (“1 = Very important”, “2 = Important”, “3 = Slightly important”, “4 = Not important”).
- Wanting the experience.Answers to this type of question were reported on the following scale (“1 = Strongly want”, “2 = Want”, “3 = Slightly want”, “4 = Do not want”, “5 = Do not care”).
- The importance of having the experience.Answers to this type of question were reported on the following scale (“1 = Very important”, “2 = Important”, “3 = Slightly important”, “4 = Not important”).
2.2.2. Web Survey Method
3. Results
3.1. EMR-Related Experiences
3.1.1. Explanation
3.1.2. Interruption
3.1.3. Exclusion
3.1.4. Distrust
3.1.5. Exchange
3.1.6. Online Viewing
3.1.7. Online Editing
3.1.8. Summarization
3.1.9. Assistance
3.2. Web Survey Participants
- Current experiences of Exclusion and Distrust.
- Aspired experiences of Explanation and Interruption.
- Priorities regarding the experience of Explanation.
3.3. Pregnant Japanese Women’s Attitudes toward the EMR-Related Experiences
3.3.1. Attitudes towards the Experience of Explanation
3.3.2. Attitudes towards the Experience of Interruption
3.3.3. Attitudes towards the Experience of Exclusion
3.3.4. Attitudes towards the Experience of Distrust
3.3.5. Attitudes towards the Experience of Exchange
3.3.6. Attitudes towards the Experience of Online Viewing
3.3.7. Attitudes towards the Experience of Online Editing
3.3.8. Attitudes towards the Experience of Summarization
3.3.9. Attitudes towards the Experience of Assistance
3.4. Summary of the Findings
4. Discussion
4.1. Different Women, Different Attitudes
4.2. Opportunities and Challenges
4.3. EMR System Design Implications
4.4. Limitations and Future Work
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A. Survey Questions

References
- Chaudhry, B.; Wang, J.; Wu, S.; Maglione, M.; Mojica, W.; Roth, E.; Morton, S.C.; Shekelle, P.G. Systematic review: Impact of health information technology on quality, efficiency, and costs of medical care. Ann. Intern. Med. 2006, 144, 742–752. [Google Scholar] [CrossRef]
- Cornwall, A. Electronic health records: An international perspective. Health Issues 2002, 73, 19–23. [Google Scholar]
- Epstein, R.M.; Street, R.L. The values and value of patient-centered care. Ann. Fam. Med. 2011, 9, 100–103. [Google Scholar] [CrossRef] [PubMed]
- Demiris, G.; Afrin, L.B.; Speedie, S.; Courtney, K.L.; Sondhi, M.; Vimarlund, V.; Lovis, C.; Goossen, W.; Lynch, C. Patient-centered applications: Use of information technology to promote disease management and wellness. A white paper by the AMIA knowledge in motion working group. J. Am. Med. Inform. Assoc. 2008, 15, 8–13. [Google Scholar] [CrossRef]
- Saleem, J.J.; Flanagan, M.E.; Russ, A.L.; McMullen, C.K.; Elli, L.; Russell, S.A.; Bennett, K.J.; Matthias, M.S.; Rehman, S.U.; Schwartz, M.D.; et al. You and me and the computer makes three: Variations in exam room use of the electronic health record. J. Am. Med. Inform. Assoc. 2013, 21, e147–e151. [Google Scholar] [CrossRef] [PubMed]
- Searle, J. Fearing the Worst-Why Do Pregnant Women Feel ‘At Risk’? Aust. N. Z. J. Obstet. Gynaecol. 1996, 36, 279–286. [Google Scholar] [CrossRef] [PubMed]
- Oakley, A. The origins and development of antenatal care. In Effectiveness and Satisfaction in Antenatal Care; Spastics International Medical Publications: London, UK, 1982; pp. 1–23. [Google Scholar]
- Hildingsson, I.; Haines, H.; Cross, M.; Pallant, J.F.; Rubertsson, C. Women’s satisfaction with antenatal care: Comparing women in Sweden and Australia. Women Birth 2013, 26, e9–e14. [Google Scholar] [CrossRef]
- Statistics Bureau, Japan. Statistical Handbook of Japan 2017; Statistics Bureau, Japan: Tokyo, Japan, 2017.
- Minakami, H.; Hiramatsu, Y.; Koresawa, M.; Fujii, T.; Hamada, H.; Iitsuka, Y.; Ikeda, T.; Ishikawa, H.; Ishimoto, H.; Itoh, H.; et al. Guidelines for obstetrical practice in Japan: Japan Society of Obstetrics and Gynecology (JSOG) and Japan Association of Obstetricians and Gynecologists (JAOG) 2011 edition. J. Obstet. Gynaecol. Res. 2011, 37, 1174–1197. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nishida, H. Perinatal health care in Japan. J. Perinatol. Off. J. Calif. Perinat. Assoc. 1996, 17, 70–74. [Google Scholar]
- Miyaji, N.T.; Lock, M. Monitoring motherhood: Sociocultural and historical aspects of maternal and child health in Japan. Daedalus 1994, 123, 87–112. [Google Scholar]
- Nakamura, Y. Maternal and child health handbook in Japan. JMAJ 2010, 53, 259–265. [Google Scholar]
- Iida, M.; Horiuchi, S.; Nagamori, K. A comparison of midwife-led care versus obstetrician-led care for low-risk women in Japan. Women Birth 2014, 27, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Cresswell, K.M.; Worth, A.; Sheikh, A. Integration of a nationally procured electronic health record system into user work practices. BMC Med. Inform. Decis. Mak. 2012, 12, 15. [Google Scholar] [CrossRef] [PubMed]
- Aarts, J.; Ash, J.; Berg, M. Extending the understanding of computerized physician order entry: Implications for professional collaboration, workflow and quality of care. Int. J. Med. Inform. 2007, 76, S4–S13. [Google Scholar] [CrossRef]
- Carayon, P.; Karsh, B.T.; Cartmill, R.; Hoonakker, P.; Hundt, A.S.; Krueger, D.; Thuemling, T.; Wetterneck, T.; Brennan, P.F.; Walker, J.; et al. Incorporating Health IT into Workflow Redesign: Request for Information Summary Report; AHRQ Publication: Rockville, MD, USA, 2010.
- Miller, R.H.; Sim, I. Physicians’ use of electronic medical records: Barriers and solutions. Health Aff. 2004, 23, 116–126. [Google Scholar] [CrossRef] [PubMed]
- Rose, A.F.; Schnipper, J.L.; Park, E.R.; Poon, E.G.; Li, Q.; Middleton, B. Using qualitative studies to improve the usability of an EMR. J. Biomed. Inform. 2005, 38, 51–60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ash, J.S.; Gorman, P.N.; Lavelle, M.; Payne, T.H.; Massaro, T.A.; Frantz, G.L.; Lyman, J.A. A cross-site qualitative study of physician order entry. J. Am. Med. Inform. Assoc. 2003, 10, 188–200. [Google Scholar] [CrossRef] [PubMed]
- Flanagan, M.E.; Saleem, J.J.; Millitello, L.G.; Russ, A.L.; Doebbeling, B.N. and computer-based workarounds to electronic health record use at three benchmark institutions. J. Am. Med. Inform. Assoc. 2013, 20, e59–e66. [Google Scholar] [CrossRef] [PubMed]
- Blijleven, V.; Koelemeijer, K.; Wetzels, M.; Jaspers, M. Workarounds Emerging From Electronic Health Record System Usage: Consequences for Patient Safety, Effectiveness of Care, and Efficiency of Care. JMIR Hum. Factors 2017, 4, e27. [Google Scholar] [CrossRef]
- Marcu, G.; Dey, A.K.; Kiesler, S. Designing for collaborative reflection. In Proceedings of the 8th International Conference on Pervasive Computing Technologies for Healthcare, Oldenburg, Germany, 20–23 May 2014; pp. 9–16. [Google Scholar]
- Walker, J.M.; Carayon, P. From tasks to processes: The case for changing health information technology to improve health care. Health Aff. 2009, 28, 467–477. [Google Scholar] [CrossRef] [PubMed]
- Scott, D.; Purves, I.N. Triadic relationship between doctor, computer and patient. Interact. Comput. 1996, 8, 347–363. [Google Scholar] [CrossRef]
- Pearce, C.; Arnold, M.; Phillips, C.; Trumble, S.; Dwan, K. The patient and the computer in the primary care consultation. J. Am. Med. Inform. Assoc. 2011, 18, 138–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pearce, C.; Dwan, K.; Arnold, M.; Phillips, C.; Trumble, S. Doctor, patient and computer—A framework for the new consultation. Int. J. Med. Inform. 2009, 78, 32–38. [Google Scholar] [CrossRef] [PubMed]
- Frankel, R.; Altschuler, A.; George, S.; Kinsman, J.; Jimison, H.; Robertson, N.R.; Hsu, J. Effects of exam-room computing on clinician–patient communication. J. Gen. Intern. Med. 2005, 20, 677–682. [Google Scholar] [CrossRef] [PubMed]
- Kazmi, Z. Effects of exam room EHR use on doctor-patient communication: A systematic literature review. J. Innov. Health Inform. 2014, 21, 30–39. [Google Scholar] [CrossRef]
- Booth, N.; Robinson, P.; Kohannejad, J. Identification of high-quality consultation practice in primary care: The effects of computer use on doctor–patient rapport. J. Innov. Health Inform. 2004, 12, 75–83. [Google Scholar] [CrossRef]
- Pearce, C.; Walker, H.; O’Shea, C. A visual study of computers on doctors’ desks. J. Innov. Health Inform. 2008, 16, 111–117. [Google Scholar] [CrossRef]
- Chan, W.S.; Stevenson, M.; McGlade, K. Do general practitioners change how they use the computer during consultations with a significant psychological component? Int. J. Med. Inform. 2008, 77, 534–538. [Google Scholar] [CrossRef]
- Als, A.B. The desk-top computer as a magic box: Patterns of behaviour connected with the desk-top computer; GPs’ and patients’ perceptions. Fam. Pract. 1997, 14, 17–23. [Google Scholar] [CrossRef]
- Greatbatch, D.; Heath, C.; Campion, P.; Luff, P. How do desk-top computers affect the doctor-patient interaction. Fam. Pract. 1995, 12, 32–36. [Google Scholar] [CrossRef]
- Montague, E.; Asan, O. Dynamic modeling of patient and physician eye gaze to understand the effects of electronic health records on doctor–patient communication and attention. Int. J. Med. Inform. 2014, 83, 225–234. [Google Scholar] [CrossRef] [PubMed]
- Noordman, J.; Verhaak, P.; van Beljouw, I.; van Dulmen, S. Consulting room computers and their effect on general practitioner–patient communication. Fam. Pract. 2010, 27, 644–651. [Google Scholar] [CrossRef] [PubMed]
- Alkureishi, M.A.; Lee, W.W.; Lyons, M.; Press, V.G.; Imam, S.; Nkansah-Amankra, A.; Werner, D.; Arora, V.M. Impact of electronic medical record use on the patient–doctor relationship and communication: A systematic review. J. Gen. Intern. Med. 2016, 31, 548–560. [Google Scholar] [CrossRef] [PubMed]
- Safran, C.; Jones, P.C.; Rind, D.; Bush, B.; Cytryn, K.N.; Patel, V.L. Electronic communication and collaboration in a health care practice1. Artif. Intell. Med. 1998, 12, 137–151. [Google Scholar] [CrossRef]
- Strayer, S.M.; Semler, M.W.; Kington, M.L.; Tanabe, K.O. Patient attitudes toward physician use of tablet computers in the exam room. Fam. Med. 2010, 42, 643. [Google Scholar] [PubMed]
- Ross, S.E.; Todd, J.; Moore, L.A.; Beaty, B.L.; Wittevrongel, L.; Lin, C.T. Expectations of patients and physicians regarding patient-accessible medical records. J. Med. Int. Res. 2005, 7, e13. [Google Scholar] [CrossRef] [PubMed]
- Hassol, A.; Walker, J.M.; Kidder, D.; Rokita, K.; Young, D.; Pierdon, S.; Deitz, D.; Kuck, S.; Ortiz, E. Patient experiences and attitudes about access to a patient electronic health care record and linked web messaging. J. Am. Med. Inform. Assoc. 2004, 11, 505–513. [Google Scholar] [CrossRef]
- Walker, J.; Leveille, S.G.; Ngo, L.; Vodicka, E.; Darer, J.D.; Dhanireddy, S.; Elmore, J.G.; Feldman, H.J.; Lichtenfeld, M.J.; Oster, N.; et al. Inviting patients to read their doctors’ notes: Patients and doctors look ahead: Patient and physician surveys. Ann. Intern. Med. 2011, 155, 811–819. [Google Scholar] [CrossRef]
- Woods, S.S.; Schwartz, E.; Tuepker, A.; Press, N.A.; Nazi, K.M.; Turvey, C.L.; Nichol, W.P. Patient experiences with full electronic access to health records and clinical notes through the My HealtheVet Personal Health Record Pilot: Qualitative study. J. Med Internet Res. 2013, 15, e65. [Google Scholar] [CrossRef]
- Baldry, M.; Cheal, C.; Fisher, B.; Gillett, M.; Huet, V. Giving patients their own records in general practice: Experience of patients and staff. Br. Med. J. 1986, 292, 596–598. [Google Scholar] [CrossRef]
- Fisher, B.; Britten, N. Patient access to records: Expectations of hospital doctors and experiences of cancer patients. Br. J. Gen. Pract. 1993, 43, 52–56. [Google Scholar] [PubMed]
- Hawley, G.; Hepworth, J.; Wilkinson, S.A.; Jackson, C. From maternity paper hand-held records to electronic health records: What do women tell us about their use? Aust. J. Prim. Health 2016, 22, 339–348. [Google Scholar] [CrossRef] [PubMed]
- Halamka, J.D.; Mandl, K.D.; Tang, P.C. Early experiences with personal health records. J. Am. Med. Inform. Assoc. 2008, 15, 1–7. [Google Scholar] [CrossRef]
- Zulman, D.M.; Nazi, K.M.; Turvey, C.L.; Wagner, T.H.; Woods, S.S.; An, L.C. Patient interest in sharing personal health record information: A web-based survey. Ann. Intern. Med. 2011, 155, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Caine, K.; Hanania, R. Patients want granular privacy control over health information in electronic medical records. J. Am. Med. Inform. Assoc. 2012, 20, 7–15. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, P.H.; Caine, K.; Alpert, S.A.; Meslin, E.M.; Carroll, A.E.; Tierney, W.M. Patient preferences in controlling access to their electronic health records: A prospective cohort study in primary care. J. Gen. Intern. Med. 2015, 30, 25–30. [Google Scholar] [CrossRef] [PubMed]
- Morris, K.; Yamamoto, G.; Hiragi, S.; Ohtera, S.; Sakai, M.; Sugiyama, O.; Okamoto, K.; Nambu, M.; Kuroda, T. Designing an Authorization System Based on Patient Privacy Preferences in Japan. Stud. Health Technol. Inform. 2018, 247, 71–75. [Google Scholar]
- Yasunaga, H.; Imamura, T.; Yamaki, S.; Endo, H. Computerizing medical records in Japan. Int. J. Med. Inform. 2008, 77, 708–713. [Google Scholar] [CrossRef] [PubMed]
- Japan International Cooperation Agency. Project Study on Utilization of Information Technologies for Maternal and Child Health; Japan International Cooperation Agency: Tokyo, Japan, 2014.
- De Lusignan, S.; Pearce, C.; Kumarapeli, P.; Stavropoulou, C.; Kushniruk, A.; Sheikh, A.; Shachak, A.; Mendis, K. Reporting Observational Studies of the Use of Information Technology in the Clinical Consultation. Yearb. Med. Inf. 2011, 39, 47. [Google Scholar]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.W.; Jones, P.S.; Mineyama, Y.; Zhang, X.E. Cultural differences in responses to a Likert scale. Res. Nurs. Health 2002, 25, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Kahneman, D.; Riis, J. Living, and thinking about it: Two perspectives on life. Sci. Well-Being 2005, 1, 285–304. [Google Scholar]
- Beale, T.; Heard, S.; Kalra, D.; Lloyd, D. OpenEHR Architecture Overview; The OpenEHR Foundation: London, UK, 2006. [Google Scholar]
- Bender, D.; Sartipi, K. HL7 FHIR: An Agile and RESTful approach to healthcare information exchange. In Proceedings of the 2013 IEEE 26th International Symposium on Computer-Based Medical Systems (CBMS), Porto, Portugal, 20–22 June 2013; pp. 326–331. [Google Scholar]
- Zhou, X.; Ackerman, M.S.; Zheng, K. Doctors and psychosocial information: Records and reuse in inpatient care. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Atlanta, GA, USA, 10–15 April 2010; pp. 1767–1776. [Google Scholar]
- Zhou, X.; Ackerman, M.S.; Zheng, K. I just don’t know why it’s gone: Maintaining informal information use in inpatient care. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Boston, MA, USA, 4–9 April 2009; pp. 2061–2070. [Google Scholar]
- Suzuki, S.; Eto, M. Domestic violence against women during pregnancy in Japan. J. Matern.-Fetal Neonatal Med. Off. J. Eur. Assoc. Perinat. Med. Fed. Asia Ocean. Perinat. Soc. Int. Soc. Perinat. Obstet. 2016, 30, 497–498. [Google Scholar] [CrossRef] [PubMed]
- Nagae, M.; Dancy, B.L. Japanese women’s perceptions of intimate partner violence (IPV). J. Interpers. Violence 2010, 25, 753–766. [Google Scholar] [CrossRef] [PubMed]
- Hawley, G.; Hepworth, J.; Jackson, C.; Wilkinson, S.A. Integrated care among healthcare providers in shared maternity care: What is the role of paper and electronic health records? Aust. J. Prim. Health 2017, 23, 397–406. [Google Scholar] [CrossRef] [PubMed]
- Mishra, V.K.; Hoyt, R.E.; Wolver, S.E.; Yoshihashi, A.; Banas, C. Qualitative and Quantitative Analysis of Patients’ Perceptions of the Patient Portal Experience with OpenNotes. Appl. Clin. Inform. 2019, 10, 010–018. [Google Scholar]
- Wang, Y.; Wang, L.; Rastegar-Mojarad, M.; Moon, S.; Shen, F.; Afzal, N.; Liu, S.; Zeng, Y.; Mehrabi, S.; Sohn, S.; et al. Clinical information extraction applications: A literature review. J. Biomed. Inform. 2018, 77, 34–49. [Google Scholar] [CrossRef]
- Helou, S.; Yamamoto, G.; Kondoh, E.; Tamura, H.; Hiragi, S.; Sugiyama, O.; Okamoto, K.; Nambu, M.; Kuroda, T. Understanding the Roles of EMR Systems in Japanese Antenatal Care Settings. Stud. Health Technol. Inform. 2018, 251, 257. [Google Scholar]
- Nakamura, M. Current status of electronic medical recording in Japan and issues involved. Jpn. Med Assoc. J. 2006, 49, 70. [Google Scholar]
- Wilcox, L.; Morris, D.; Tan, D.; Gatewood, J. Designing patient-centric information displays for hospitals. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Atlanta, GA, USA, 10–15 April 2010; pp. 2123–2132. [Google Scholar]
- Piper, A.M.; Hollan, J.D. Supporting medical conversations between deaf and hearing individuals with tabletop displays. In Proceedings of the 2008 ACM conference on Computer supported cooperative work, San Diego, CA, USA, 8–12 November 2008; pp. 147–156. [Google Scholar]
- Bardram, J.E.; Hansen, T.R.; Soegaard, M. Large interactive displays in hospitals-Motivation, examples, and challenges. In Proceedings of the CHI 2006 Workshop, Information Visualization and Interaction Techniques for Collab Across Multiple Displays, Montreal, QC, Canada, 22–23 April 2006. [Google Scholar]
- Chen, Y.; Ngo, V.; Harrison, S.; Duong, V. Unpacking exam-room computing: Negotiating computer-use in patient-physician interactions. In Proceedings of the SIGCHI Conference on Human Factors in Computing Systems, Vancouver, BC, Canada, 7–12 May 2011; pp. 3343–3352. [Google Scholar]
- Kildea, J.; Battista, J.; Cabral, B.; Hendren, L.; Herrera, D.; Hijal, T.; Joseph, A. Design and Development of a Person-Centered Patient Portal Using Participatory Stakeholder Co-Design. J. Med. Int. Res. 2019, 21, e11371. [Google Scholar] [CrossRef]
- Steglich, S. I-Centric User Interaction. Ph.D. Thesis, Berlin Institute of Technology, Berlin, Germany, 2003. [Google Scholar]
- Pandita, R. Internet: A change agent an overview of internet penetration & growth across the world. Int. J. Inf. Dissem. Technol. 2017, 7, 83. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
| Experience | Definition | Type |
|---|---|---|
| Explanation | The providers using the EMR screen as an explanation support tool. | Current |
| Interruption | EMR systems hinder the communication of the women and their providers. | Current |
| Exclusion | The pregnant women feeling excluded by not being able to see the EMR screen. | Current |
| Distrust | Sensitive psychosocial data not being documented in detail inside the EMR. | Current |
| Exchange | Different providers exchanging the women’s medical records. | Current |
| Online Viewing | The pregnant women being able to view the contents of their EMRs online. | Future |
| Online Editing | The pregnant women being able to add content to their EMRs online. | Future |
| Summarization | The women having access to a summary of their pregnancy. | Future |
| Assistance | The women being able to manage their antenatal care appointments online. | Future |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Helou, S.; Abou-Khalil, V.; Yamamoto, G.; Kondoh, E.; Tamura, H.; Hiragi, S.; Sugiyama, O.; Okamoto, K.; Nambu, M.; Kuroda, T. Understanding the EMR-Related Experiences of Pregnant Japanese Women to Redesign Antenatal Care EMR Systems. Informatics 2019, 6, 15. https://0-doi-org.brum.beds.ac.uk/10.3390/informatics6020015
Helou S, Abou-Khalil V, Yamamoto G, Kondoh E, Tamura H, Hiragi S, Sugiyama O, Okamoto K, Nambu M, Kuroda T. Understanding the EMR-Related Experiences of Pregnant Japanese Women to Redesign Antenatal Care EMR Systems. Informatics. 2019; 6(2):15. https://0-doi-org.brum.beds.ac.uk/10.3390/informatics6020015
Chicago/Turabian StyleHelou, Samar, Victoria Abou-Khalil, Goshiro Yamamoto, Eiji Kondoh, Hiroshi Tamura, Shusuke Hiragi, Osamu Sugiyama, Kazuya Okamoto, Masayuki Nambu, and Tomohiro Kuroda. 2019. "Understanding the EMR-Related Experiences of Pregnant Japanese Women to Redesign Antenatal Care EMR Systems" Informatics 6, no. 2: 15. https://0-doi-org.brum.beds.ac.uk/10.3390/informatics6020015