
Extending the UTAUT2 Model with a Privacy Calculus Model to Enhance the Adoption of a Health Information Application in Malaysia


Abstract
:1. Introduction
2. Literature Review
2.1. Technology Adoption Models
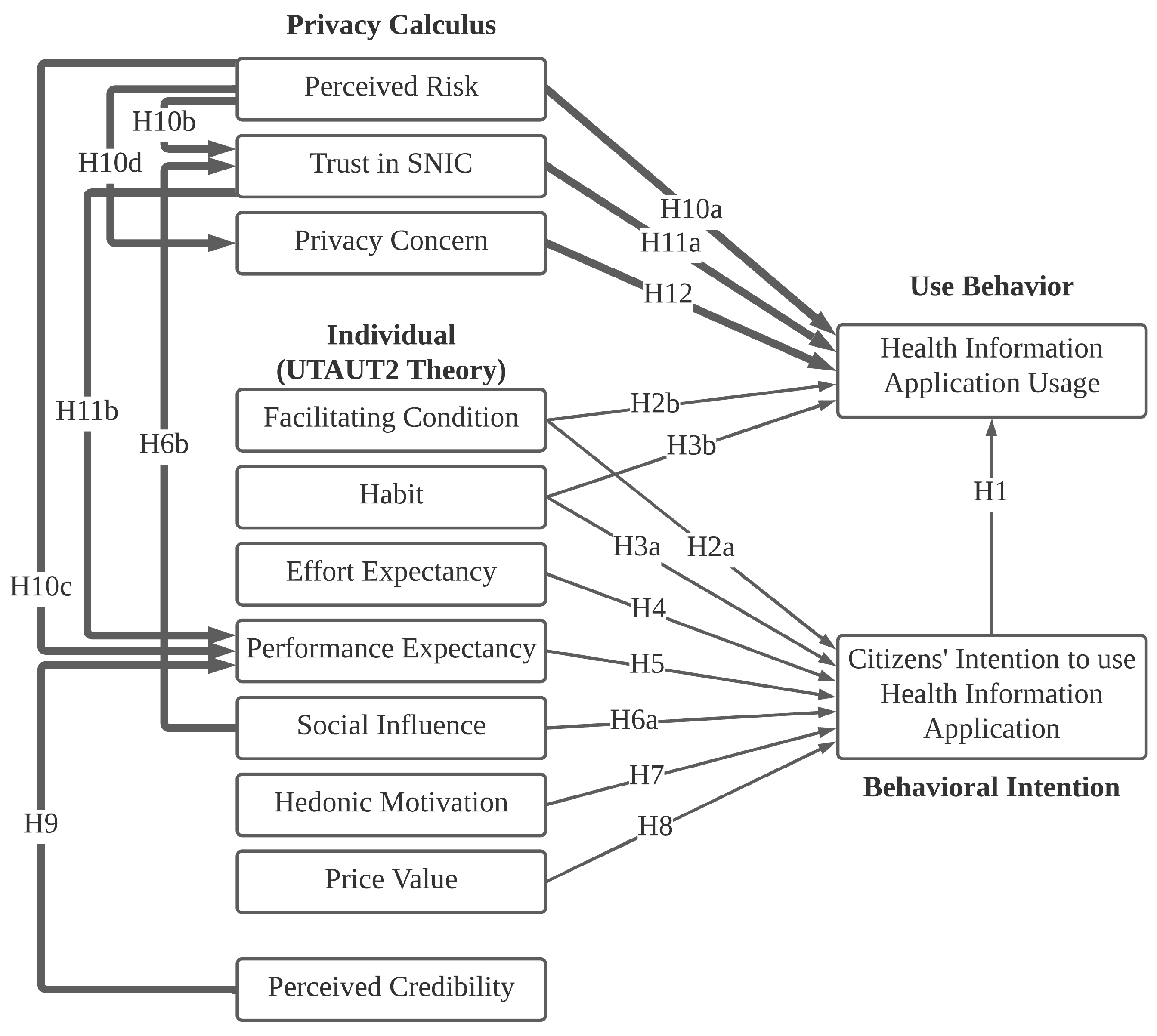
2.2. Model Development
2.3. UTAUT2 and the New Integrated Constructs and Relationships
3. Method
Data Collection and Analysis Process
4. Results
4.1. Respondent Characteristics
4.2. Evaluation of the Measurement Model
4.3. Discriminant Validity
4.4. Evaluation of the Structural Model
5. Discussion
6. Contributions and Implications
7. Limitations
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hassan, I.B.; Murad, M.A.A. Privacy and security problems in using health information application in Smart National Identity Card (SNIC). World Appl. Sci. J. 2014, 32, 688–692. [Google Scholar] [CrossRef]
- Shukri, M.; Hafiz, M. The Privacy and Security of an Identification Card: Malaysian Perspective; Scientific Report; Universiti Malaysia Sarawak: Sarawak, Malaysia, 2015; Volume 65855. [Google Scholar]
- Neo, H.F.; Yeow, P.H.; Eze, U.C.; Loo, H.S. Organizations adoption of MyKad initiative. Commun. IBIMA 2012, 2012, 542549. [Google Scholar] [CrossRef] [Green Version]
- Loo, W.; Yeow, P.H.; Chong, S. Acceptability of multipurpose smart national identity card: An empirical study. J. Glob. Inf. Technol. Manag. 2011, 14, 35–58. [Google Scholar] [CrossRef]
- Yeow, P.H.; Hong Loo, W.; Choy Chong, S. Accepting Multipurpose “Smart” Identity Cards in a Developing Country. J. Urban Technol. 2007, 14, 23–50. [Google Scholar] [CrossRef]
- Yeow, P.H.; Loo, W.H. Acceptability of ATM and Transit Applications Embedded in Multipurpose Smart Identity Card: An Exploratory Study in Malaysia. Int. J. Electron. Gov. Res. 2009, 5, 37–56. [Google Scholar] [CrossRef] [Green Version]
- Perera, G.; Holbrook, A.; Thabane, L.; Foster, G.; Willison, D. Views on health information sharing and privacy from primary care practices using electronic medical records. Int. J. Med. Inform. 2011, 80, 94–101. [Google Scholar] [CrossRef]
- McGinn, C.A.; Grenier, S.; Duplantie, J.; Shaw, N.; Sicotte, C.; Mathieu, L.; Leduc, Y.; Légaré, F.; Gagnon, M.P. Comparison of user groups’ perspectives of barriers and facilitators to implementing electronic health records: A systematic review. BMC Med. 2011, 9, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Duartea, P.; Pinho, J.C. A mixed methods UTAUT2-based approach to assess mobile health adoption. J. Bus. Res. 2019, 102, 140–150. [Google Scholar] [CrossRef]
- Hird, N.; Ghosh, S.; Kitano, H. Digital health revolution: Perfect storm or perfect opportunity for pharmaceutical R&D. Drug Discov. Today 2016, 21, 900–911. [Google Scholar]
- Gurupur, V.P.; Wan, T.T. Challenges in implementing mHealth interventions: A technical perspective. mHealth 2017, 3, 32. [Google Scholar] [CrossRef] [Green Version]
- Leming, Z.; Jie, B.; Valerie, W.; Bambang, P. Barriers to and Facilitators of the Use of Mobile Health Apps From a Security Perspective: Mixed-Methods Study. JMIR Mhealth Uhealth 2019, 7, e11223. [Google Scholar]
- Proudfoot, J.G.; Parker, G.B.; Pavlovic, D.H.; Manicavasagar, V.; Adler, E.; Whitton, A.E. Community attitudes to the appropriation of mobile phones for monitoring and managing depression, anxiety, and stress. J. Med. Internet Res. 2010, 12, e1475. [Google Scholar] [CrossRef] [PubMed]
- Kenny, R.; Dooley, B.; Fitzgerald, A. Developing mental health mobile apps: Exploring adolescents’ perspectives. Health Inform. J. 2016, 22, 265–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Matteo, D.; Fine, A.; Fotinos, K.; Rose, J.; Katzman, M. Patient willingness to consent to mobile phone data collection for mental health apps: Structured questionnaire. JMIR Ment. Health 2018, 5, e9539. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Venkatesh, V.; Morris, M.G.; Davis, G.B.; Davis, F.D. User Acceptance of Information Technology: Toward a Unified View. MIS Q. 2003, 27, 425–478. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Thong, J.Y.; Xu, X. Consumer acceptance and use of information technology: Extending the unified theory of acceptance and use of technology. MIS Q. 2012, 36, 157–178. [Google Scholar] [CrossRef] [Green Version]
- Im, I.; Kim, Y.; Han, H.J. The Effects of Perceived Risk and Technology Type on Users’ Acceptance of Technologies. Inf. Manag. 2008, 45, 1–9. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, S.W.; Song, C.H. The Effects of Trust and Perceived Risk on Users’ Acceptance of ICT Services; KAIST: Daejeon, Korea, 2010. [Google Scholar]
- Rana, N.P. Evaluating Suitability of Alternative Theoretical Paradigm for Examining Citizen Adoption of E-Government; Brunel University: London, UK, 2012. [Google Scholar]
- Taiwo, A.A.; Mahmood, A.K.; Downe, A.G. User acceptance of eGovernment: Integrating risk and trust dimensions with UTAUT model. In Proceedings of the 2012 International Conference on Computer & Information Science (ICCIS), Kuala Lumpur, Malaysia, 12–14 June 2012; Volume 1, pp. 109–113. [Google Scholar]
- Culnan, M.; Armstrong, P. Information privacy concerns, procedural fairness, and impersonal trust: An empirical investigation. Organ. Sci. 1999, 10, 104–115. [Google Scholar] [CrossRef]
- Tavares, J.; Oliveira, T. Electronic health record patient portal adoption by health care consumers: An acceptance model and survey. J. Med. Internet Res. 2016, 18, e5069. [Google Scholar] [CrossRef] [Green Version]
- Tavares, J.; Oliveira, T. Electronic Health Record Portal Adoption: A cross country analysis. BMC Med. Inform. Decis. Mak. 2017, 17, 17. [Google Scholar] [CrossRef] [Green Version]
- Wills, M.J.; El-Gayar, O.F.; Bennett, D. Examining healthcare professionals’ acceptance of electronic medical records using UTAUT. Issues Inf. Syst. 2008, 9, 396–401. [Google Scholar]
- Kim, S.; Lee, K.H.; Hwang, H.; Yoo, S. Analysis of the factors influencing healthcare professionals’ adoption of mobile electronic medical record (EMR) using the unified theory of acceptance and use of technology (UTAUT) in a tertiary hospital. BMC Med. Inform. Decis. Mak. 2015, 16, 1–12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ami-Narh, J.T.; Williams, P.A. A revised UTAUT model to investigate E-health acceptance of health professionals in Africa. J. Emerg. Trends Comput. Inf. Sci. 2012, 3, 1383–1391. [Google Scholar]
- Hennington, A.; Janz, B.D. Information systems and healthcare XVI: Physician adoption of electronic medical records: Applying the UTAUT model in a healthcare context. Commun. Assoc. Inf. Syst. 2007, 19, 5. [Google Scholar] [CrossRef] [Green Version]
- Venkatesh, V.; Sykes, T.A.; Zhang, X. ‘Just what the doctor ordered’: A revised UTAUT for EMR system adoption and use by doctors. In Proceedings of the 2011 44th Hawaii International Conference on System Sciences, Kauai, HI, USA, 4–7 January 2011. [Google Scholar]
- Yuan, S.; Ma, W.; Kanthawala, S.; Peng, W. Keep Using My Health Apps: Discover Users’ Perception of Health and Fitness Apps with the UTAUT2 Model. Telemed. e-Health 2015, 21, 735–741. [Google Scholar] [CrossRef]
- Gao, Y.; Li, H.; Luo, Y. An empirical study of wearable technology acceptance in healthcare. Ind. Manag. Data Syst. 2015, 115, 1704–1723. [Google Scholar] [CrossRef]
- Nysveen, H.; Pedersen, P.E. Consumer adoption of RFID-enabled services. Applying an extended UTAUT model. Inf. Syst. Front. 2016, 18, 293–314. [Google Scholar] [CrossRef]
- Zhou, T. Examining Location-Based Services Usage from the Perspectives of unified theory of acceptance and use of technology and Privacy Risk. J. Electron. Commer. Res. 2012, 13, 135. [Google Scholar]
- Weinhard, A.; Hauser, M.; Thiesse, F. Explaining Adoption of Pervasive Retail Systems with a Model based on UTAUT2 and the Extended Privacy Calculus. In Proceedings of the 21st Pacific Asia Conference on Information, Langkawi, Malaysia, 16–20 July 2017. [Google Scholar]
- Fernandes, T.; Oliveira, E. Understanding consumers’ acceptance of automated technologies in service encounters: Drivers of digital voice assistants adoption. J. Bus. Res. 2021, 122, 180–191. [Google Scholar] [CrossRef]
- Pitardi, V.; Marriott, H.R. Alexa, she’s not human but… Unveiling the drivers of consumers’ trust in voice-based artificial intelligence. Psychol. Mark. 2021, 38, 626–642. [Google Scholar] [CrossRef]
- Kowatsch, T.; Maass, W. IoT-I Deliverable—D2.4: Social Acceptance and Impact Evaluation. Work Report. 2012. Available online: https://www.alexandria.unisg.ch/publications/211859 (accessed on 1 March 2022).
- Kijsanayotin, B.; Pannarunothai, S.; Speedie, S.M. Factors influencing health information technology adoption in Thailand’s community health centers: Applying the UTAUT model. Int. J. Med. Inform. 2009, 78, 404–416. [Google Scholar] [CrossRef] [PubMed]
- Dinev, T.; Hart, P. Privacy Concerns and Internet Use—A Model of Trade-Off Factors; Academy of Management: Briarcliff Manor, NY, USA, 2003. [Google Scholar]
- Dinev, T. Privacy calculus model in e-commerce. Eur. J. Inf. Syst. 2006, 15, 389–402. [Google Scholar] [CrossRef]
- Dinev, T.; Hart, P. An extended privacy calculus model for e-commerce transactions. Inf. Syst. Res. 2006, 17, 61–80. [Google Scholar] [CrossRef]
- Al-Sobhi, F.; Weerakkody, V.; El-Haddadeh, R. The Relative Importance of Intermediaries in eGovernment Adoption: A study of Saudi Arabia. In International Conference on Electronic Government; EGOV 2011, LNCS 6846; Janssen, M., Scholl, H.J., Wimmer, M.A., Tan, Y.-H., Eds.; Springer: Berlin/Heidelberg, Germany, 2011; pp. 62–74. [Google Scholar]
- Carter, L.; Schaupp, L.C. Relating acceptance and optimism to e-file adoption. Int. J. Electron. Gov. Res. (IJEGR) 2009, 5, 62–74. [Google Scholar] [CrossRef] [Green Version]
- Hussein, R.; Mohamed, N.; Ahlan, A.R.; Mahmud, M.; Aditiawarman, U. G2C adoption of e-government in Malaysia: Trust, perceived risk and political self-efficacy. Int. J. Electron. Gov. Res. (IJEGR) 2010, 6, 57–72. [Google Scholar] [CrossRef]
- Carter, L.; Shaupp, L.C.; Hobbs, J.; Campbell, R. The role of security and trust in the adoption of online tax filing. Transform. Gov. People Process. Policy 2011, 5, 303–318. [Google Scholar] [CrossRef] [Green Version]
- Chiang, L. Trust and security in the e-voting system. Electron. Gov. Int. J. 2009, 6, 343–360. [Google Scholar] [CrossRef]
- McLeod, A.; Pippin, S.; Catania, V. Using technology acceptance theory to model individual differences in tax software use. In Proceedings of the 15th Americas Conference on Information Systems, San Francisco, CA, USA, 6–9 August 2009; pp. 1–11. [Google Scholar]
- Smith, J. Determining Key Factors in E-Government Information System Security. Inf. Syst. Manag. 2006, 23, 23–32. [Google Scholar] [CrossRef]
- Belanger, F.; Carter, L. Trust and risk in e-government adoption. Strateg. Inf. Syst. 2008, 17, 165–176. [Google Scholar] [CrossRef] [Green Version]
- Ciborra, C.; Navarra, D.D. Good governance, development theory, and aid policy: Risks and challenges of e-government in Jordan. Inf. Technol. Dev. 2005, 11, 141–159. [Google Scholar] [CrossRef]
- Lee, S.M.; Tan, X.; Trimi, S. M-government, from rhetoric to reality: Learning from leading countries. Electron. Gov. Int. J. 2006, 3, 113–126. [Google Scholar] [CrossRef]
- Loukis, E.; Charalabidis, Y. Why do eGovernment projects fail? Risk factors of large information systems projects in the Greek public sector: An international comparison. Int. J. Electron. Gov. Res. (IJEGR) 2011, 7, 59–77. [Google Scholar] [CrossRef] [Green Version]
- Colesca, S. Increasing E-Trust: A Solution to Minimize Risk in E-Government Adoption. J. Appl. Quant. Methods 2009, 4, 31–44. [Google Scholar]
- Yeow, P.H.; Yuen, Y.; Loo, W. Ergonomics issues in national identity card for homeland security. Appl. Ergon. 2013, 44, 719–729. [Google Scholar] [CrossRef] [PubMed]
- Shachak, A.; Kuziemsky, C.; Petersen, C. Beyond TAM and UTAUT: Future directions for HIT implementation research. J. Biomed. Inform. 2019, 100, 103315. [Google Scholar] [CrossRef]
- Wilson, D.; Valacich, J.S. Unpacking the Privacy Paradox: Irrational Decision-Making within the Privacy Calculus. In Proceedings of the International Conference on Information Systems (ICIS 2012), Orlando, FL, USA, 16–19 December 2012. [Google Scholar]
- Hassan, I.B.; Murad, M.A.A. Acceptance of Health Information Application in Smart National Identity Card (SNIC) Using a New I-P Framework. Int. J. Med. Health Sci. 2014, 8, 3782–3790. [Google Scholar]
- Hassan, I.B.; Murad, M.A.A.; Nor, R.N.H.B.; Abdullah, S.B. Towards Developing a New I-P Technology Adoption Framework: A Research Road Map. In Proceedings of the 2014 International Conference on Computer Assisted System in Health, Kuala Lumpur, Malaysia, 19–21 December 2014; pp. 77–83. [Google Scholar] [CrossRef]
- Davis, F.D. Perceived usefulness, perceived ease of use, and user acceptance of information technology. MIS Q. 1989, 13, 319–340. [Google Scholar] [CrossRef] [Green Version]
- Ajzen, I. The Theory of Planned Behavior. Organ. Behav. Hum. Decis. Process. 1991, 50, 179–211. [Google Scholar] [CrossRef]
- Al-Gahtani, S.; Hubona, G.; Wang, J. Information Technology (IT) in Saudi Arabia: Culture and the Acceptance and Use of IT. Inf. Manag. 2007, 44, 681–691. [Google Scholar] [CrossRef]
- Yuen, Y.; Yeow, P.; Lim, N.; Saylani, N. Internet Banking Adoption: Comparing Developed and Developing Countries. J. Comput. Inf. Syst. 2010, 51, 52–61. [Google Scholar]
- Dishaw, M.; Strong, D. Extending the technology acceptance model with task-technology fit constructs. Inf. Manag. 1999, 36, 9–21. [Google Scholar] [CrossRef]
- Cho, V. A study of the roles of trusts and risks in information-oriented online legal services using an integrated model. Inf. Manag. 2006, 43, 502–520. [Google Scholar] [CrossRef]
- Keselman, A.; Logan, R.; Smith, C.A.; Leroy, G.; Zeng-Treitler, Q. Developing informatics tools and strategies for consumer-centered health communication. J. Am. Med. Inform. Assoc. 2008, 15, 473–483. [Google Scholar] [CrossRef] [PubMed]
- Limayem, M.; Hirt, S.G.; Cheung, C.M.K. How Habit Limits the Predictive Power of Intentions: The Case of IS Con-tinuance. MIS Q. 2007, 31, 705–737. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.S.; Malhotra, N.K.; Narasimhan, S. Two Competing Perspectives on Automatic Use: A Theoretical and Empirical Comparison. Inf. Syst. Res. 2005, 16, 418–432. [Google Scholar] [CrossRef]
- Or, C.K.; Karsh, B.T.; Severtson, D.J.; Burke, L.J.; Brown, R.L.; Brennan, P.F. Factors affecting home care patients’ acceptance of a web-based interactive self-management technology. J. Am. Med. Inform. Assoc. 2011, 18, 51–59. [Google Scholar] [CrossRef] [Green Version]
- Po, R.W.; Lin, F.R.; Chuang, B.K.; Shaw, M.J. Exploring trust-based service value chain framework in tele-healthcare services. In Proceedings of the 2013 46th Hawaii International Conference on System Sciences, Wailea, HI, USA, 7–10 January 2013; pp. 1327–1336. [Google Scholar]
- Park, J.; Chung, T.L.; Hur, W.M. The Role of Consumer Innovativeness and Trust for Adopting Internet Phone Services. Int. J. E-Serv. Mob. Appl. (IJESMA) 2011, 3, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Gefen, D.; Karahanna, E.; Straub, D. Trust and TAM in online shopping: An integrated model. MIS Q. 2003, 27, 51–90. [Google Scholar] [CrossRef]
- Brown, S.A.; Venkatesh, V. Model of Adoption of Technology in the Household: A Baseline Model Test and Extension Incorporating Household Life Cycle. MIS Q. 2005, 29, 399–426. [Google Scholar] [CrossRef]
- Dodds, W.B.; Monroe, K.B.; Grewal, D. Effects of Price, Brand, and Store Information on Buyers. J. Mark. Res. 1991, 28, 307–319. [Google Scholar]
- Chan, K.Y.; Gong, M.; Xu, Y.; Thong, J.Y.L. Examining User Acceptance of SMS: An Empirical Study in China and Hong Kong. 2008. Available online: https://aisel.aisnet.org/pacis2008/294 (accessed on 1 March 2022).
- Bauer, R.A. Consumer behavior as risk-taking. In Dynamic Marketing for a Changing World; Hancock, R.S., Ed.; American Marketing Association: Chicago, IL, USA, 1960; pp. 389–398. [Google Scholar]
- Warkentin, M.; Gefen, D.; Pavlou, P.; Rose, G. Encouraging citizen adoption of e-government by building trust. Electron. Mark. 2002, 12, 157–162. [Google Scholar] [CrossRef]
- McKnight, D.H.; Choudhury, V.; Kacmar, C. Developing and validating trust measures for e-commerce: An integrative typology. Inf. Syst. Res. 2002, 13, 334–359. [Google Scholar] [CrossRef] [Green Version]
- Dowling, G.; Staelin, R. A Model of Perceived Risk and Risk Handling Activity. J. Consum. Res. 1994, 21, 119–134. [Google Scholar] [CrossRef]
- Berner, E. Ethical and Legal Issues in the Use of Health Information Technology to Improve Patient Safety. HEC Forum 2008, 20, 243–258. [Google Scholar] [CrossRef] [PubMed]
- Willison, D.J.; Schwartz, L.; Abelson, J.; Charles, C.; Swinton, M.; Northrup, D.; Thabane, L. Alternatives to Project-Specific Consent for Access to Personal Information for Health Research: What Is the Opinion of the Canadian Public? J. Am. Med. Inform. Assoc. 2007, 14, 706–712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rhonda, J.R. A Study of the Intent to Fully Utilize Electronic Personal Health Records in the Context of Privacy and Trust. Ph.D. Thesis, University of North Texas, Denton, TX, USA, 2012. [Google Scholar]
- David, D. Electronic Personal Health Records: A Matter of Trust. Ph.D. Thesis, McMaster University, Hamilton, ON, Canada, 2013. [Google Scholar]
- Anderson, C.L.; Agarwal, R. The Digitization of Healthcare: Boundary Risks, Emotion, and Consumer Willingness to Disclose Personal Health Information. Inf. Syst. Res. 2011, 22, 469–490. [Google Scholar] [CrossRef]
- Luo, X.; Li, H.; Zhang, J.; Shim, J. Examining multi-dimensional trust and multi-faceted risk in initial acceptance of emerging technologies: An empirical study of mobile banking services. Decis. Support Syst. 2010, 49, 222–234. [Google Scholar] [CrossRef]
- Featherman, M.; Pavlou, P. Predicting e-services adoption: A perceived risk facets perspective. Int. J. Hum.-Comput. Stud. 2003, 59, 451–474. [Google Scholar] [CrossRef] [Green Version]
- Dinev, T.; Xu, H.; Smith, J.H.; Hart, P. Information privacy and correlates: An empirical attempt to bridge and distinguish privacy-related concepts. Eur. J. Inf. Syst. 2014, 22, 295–316. [Google Scholar] [CrossRef]
- Xu, H.; Dinev, T.; Smith, J.; Hart, P. Information Privacy Concerns: Linking Individual Perceptions with Institutional Privacy Assurances. J. Assoc. Inf. Syst. 2011, 12, 798–824. [Google Scholar] [CrossRef]
- Liao, C.; Liu, C.C.; Chen, K. Examining the impact of privacy, trust and risk perceptions beyond monetary transactions: An integrated model. Electron. Commer. Res. Appl. 2011, 10, 702–715. [Google Scholar]
- Youn, S. Determinants of online privacy concern and its influence on privacy protection behaviors among young adolescents. J. Consum. Aff. 2009, 43, 389–418. [Google Scholar] [CrossRef]
- Xu, F.; Katina, M.; Xi, C. Factors Affecting Privacy Disclosure on Social Networksites: An Integrated Model; Springer Science+Business Media: New York, NY, USA, 2013; p. 18. [Google Scholar] [CrossRef]
- Bandyopadhyay, K.; Fraccastoro, K.A. The effect of culture on user acceptance on information technology. Commun. AIS 2007, 19, 522–543. [Google Scholar] [CrossRef]
- Li, X.; Hess, T.; Valacich, J. Why do we trust new technology? A study of initial trust formation with organizational information systems. J. Strateg. Inf. Syst. 2008, 17, 39–71. [Google Scholar] [CrossRef]
- Alkhalifah, A. Factors Affecting User Adoption of Identity Management Systems: An Empirical Study. Ph.D. Thesis, University of New South Wales, Sydney, Australia, 2013. [Google Scholar]
- Lee, M. Predicting and explaining the adoption of online trading: An empirical study in Taiwan. Decis. Support Syst. 2009, 47, 133–142. [Google Scholar] [CrossRef]
- Cohena, J.; Jonesa, M.; Bancilhona, J.M. Exploring South African Physicians’ Acceptance of e-Prescribing Technology. S. Afr. Comput. J. 2013, 50, 43–54. [Google Scholar]
- Tung, F.; Chang, S.; Chou, C. An extension of trust and TAM model with IDT in the adoption of the electronic logistics information system in HIS in the medical industry. Int. J. Med. Inform. 2008, 77, 324–335. [Google Scholar] [CrossRef]
- Malhotra, N.K.; Kim, S.S.; Agarwal, J. Internet users’ information privacy concerns (IUIPC): The construct, the scale, and a causal model. Inf. Syst. Res. 2004, 15, 336–355. [Google Scholar] [CrossRef] [Green Version]
- Junglas, I.A.; Johnson, N.A.; Spitzmüller, C. Personality traits and concern for privacy: An empirical study in the context of location-based services. Eur. J. Inf. Syst. 2008, 17, 387–402. [Google Scholar] [CrossRef]
- Bansal, G.; Zahedi, F.M.; Gefen, D. The impact of personal dispositions on information sensitivity, privacy concern and trust in disclosing health information online. Decis. Support Syst. 2010, 49, 138–150. [Google Scholar] [CrossRef]
- Angst, C.M.; Agarwal, R. Adoption of electronic health records in the presence of privacy concerns: The elaboration likelihood model and individual persuasion. MIS Q. 2009, 33, 339–370. [Google Scholar] [CrossRef] [Green Version]
- Naser, C.; Alpert, S.A. Protecting the Privacy of Medical Records: An Ethical Analysis; National Coalition for Patient Rights: Lexington, MA, USA, 1999. [Google Scholar]
- Alpert, S.A. Health Care Information: Confidentiality, Access, and Good Practice, in Ethics, Computing, and Medicine: Informatics and the Transformation of Health Care; Goodman, K.W., Ed.; Cambridge University Press: New York, NY, USA, 1998; pp. 75–101. [Google Scholar]
- Poll, D.; Mirick, O.; Lougee, L. Many Patients Withhold Health Data. Health Data Management. 1 June 2011. Available online: https://cdn.hcinnovationgroup.com/ebook/201106/resources/8.htm (accessed on 1 March 2022).
- Fung, M.; Paynter, J. The impact of information technology in health care privacy. In Privacy Protection for E-Services; IGI Global: Hershey, PA, USA, 2006; pp. 56–93. [Google Scholar]
- Mekawie, N.M. Factors affecting adoption of eHealth in Egypt. Ph.D. Thesis, Middlesex University, London, UK, 2013. [Google Scholar]
- Hong, Y.; Liu, Q.; LU, S.; Wang, L.; Dssouli, R. A Hierarchical Approach to the Specification of Privacy Preferences. In Proceedings of the 2007 Innovations in Information Technologies (IIT), Dubai, United Arab Emirates, 18–20 November 2007. [Google Scholar]
- Chellappa, R.K.; Sin, R.G. Personalization Versus Privacy: An Empirical Examination of the Online Consumer’s Dilemma. Inf. Technol. Manag. 2005, 6, 181–202. [Google Scholar] [CrossRef]
- Thong, J.Y.L. An integrated model of information systems adoption in small businesses. J. Manag. Inf. Syst. 1999, 15, 187–214. [Google Scholar] [CrossRef]
- Marine Stewardship Council. 2006. Available online: http://www.msc.com.my/msc/flagships.asp?link=mpc (accessed on 1 March 2022).
- Sekaran, U. Research methods for business: A skill building approach. Leadersh. Organ. Dev. J. 2013, 34, 700–701. [Google Scholar]
- Chin, W. How to Write Up and Report PLS Analyses, Handbook of Partial Least Squares; Springer: Berlin/Heidelberg, Germany, 2010; pp. 655–690. [Google Scholar]
- Hair, J.F.; Black, W.C.; Babin, B.J.; Anderson, R.E.; Tatham, R.L. Multivariate Data Analysis; Pearson Prentice: Upper Saddle River, NJ, USA, 2010; Volume 2, p. 70. [Google Scholar]
- Hair, J.; Anderson, R.; Tatham, R.; Black, W. Multivariate Data Analysis, 5th ed.; Prentice Hall: Upper Saddle River, NJ, USA, 1998. [Google Scholar]
- Henseler, J.; Ringle, C.M.; Sarstedt, M. A New Criterion for Assessing Discriminant Validity in Variance-based Structural Equation Modeling. J. Acad. Mark. Sci. 2015, 43, 115–135. [Google Scholar] [CrossRef] [Green Version]
- Ringle, C.M.; Wende, S.; Becker, J.M. Smartpls 3; SmartPLS: Hamburg, Germany, 2014. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciencies; Routledge: London, UK; Lawrence Erlbaum Associates, Inc.: Mahwah, NJ, USA, 1988; Volume 88. [Google Scholar]
- Chin, W.W. The partial least squares approach to structural equation modeling. Mod. Methods Bus. Res. 1998, 295, 295–336. [Google Scholar]
- Hair, J.F.; Hult, G.T.M.; Ringle, C.M.; Sarstedt, M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM); Sage: Thousand Oaks, CA, USA, 2014. [Google Scholar]
- Van der Heijden, V. Factors influencing the usage of websites: The case of a generic portal in The Netherlands. Inf. Manag. 2003, 40, 541–549. [Google Scholar] [CrossRef] [Green Version]
- Davis, F.D.; Venkatesh, V. Toward Preprototype User Acceptance Testing of New Information Systems: Implications for Software Project Management. IEEE Trans. Eng. Manag. 2004, 51, 31–46. [Google Scholar] [CrossRef]
- Phichitchaisopa, N.; Naenna, T. Factors affecting the adoption of healthcare information technology. EXCLI J. 2013, 12, 413–436. [Google Scholar]
- Yaghoubi, N.; Kord, B.; Shakeri, R. E-Government Services and User Acceptance: The Unified Models’ Perspective. Eur. J. Econ. Financ. Adm. Sci. 2010, 24, 36–49. [Google Scholar]
- Gefen, D.; Straub, D.W.; Boudreau, M.C. Structural equation modeling and regression: Guidelines for research practice. Commun. Assoc. Inf. Syst. 2000, 4, 7. [Google Scholar] [CrossRef] [Green Version]
- Wannasiri, B. User Acceptance of E-Government Services: An emperical investigation of the E-Tax Filing and Payment in Thailand. Ph.D. Thesis, Korea Advanced Institute of Science and Technology, Daedeok Campus (KAIST), Daejeon, Korea, 2011. [Google Scholar]
- Peng, H.; Xu, X.; Liu, W. Drivers and Barriers in the Acceptance of Mobile Payment in China. Commun. Inf. Sci. Manag. Eng. 2011, 1, 73–78. [Google Scholar]
- Ernst, C.P.H. Risk Hurts Fun: The Influence of Perceived Privacy Risk on Social Network Site Usage; Springer Gabler: Wiesbaden, Germany, 2014. [Google Scholar]
- Ling, K.C.; bin Daud, D.; Piew, T.H.; Keoy, K.H.; Hassan, P. Perceived Risk, Perceived Technology, Online Trust for the Online Purchase Intention in Malaysia. Int. J. Bus. Manag. 2011, 6, 16. [Google Scholar]
- Murkherjee, A.; Nath, P. Role of electronic trust in online retailing: A re-examination of the commitment-trust theory. Eur. J. Mark. 2007, 41, 1173–1202. [Google Scholar] [CrossRef]
- Chen, Y.; Barnes, S. Initial trust and online buyer behavior. Ind. Manag. Data Syst. 2007, 107, 21–36. [Google Scholar] [CrossRef]
- Gefen, D.; Pavlou, P.A. An inverted-U theory of trust: The moderating role of perceived regulatory effectiveness of online marketplaces. In Proceedings of the Twenty Seventh International Conference on Information System, Regensburg, Germany, 4–8 September 2006. [Google Scholar]
- Pavlou, P.A. Consumer acceptance of electronic commerce: Integrating trust and risk with the technology acceptance model. Int. J. Electron. Commer. 2003, 7, 101–134. [Google Scholar]
- Koufaris, M.; Hampton-Sosa, W. The development of initial trust in an online company by new customers. Inf. Manag. 2004, 41, 377–397. [Google Scholar] [CrossRef] [Green Version]
- Warrington, T.B.; Abgrab, N.J.; Caldwell, M. Building trust to develop competitive advantage in E-business relationships. Compet. Rev. 2000, 10, 160–168. [Google Scholar] [CrossRef]
- Thokozani, U. Building Consumer Mobile Money Adoption and Trust in Conditions Where Infrastructures Are Unreliable. Ph.D. Thesis, University of Pretoria, Pretoria, South Africa, 2012. [Google Scholar]
- Keith, M.J.; Babb, J.S.; Furner, C.P.; Abdullat, A. Privacy Assurance and Network Effects in the adoption of Location-Based Services: An iPhone Experiment. ICIS 2010 Proceedings: 237. 2010. Available online: https://aisel.aisnet.org/icis2010_submissions/237 (accessed on 1 March 2022).
- Xu, H.; Teo, H. Alleviating Consumers’ Privacy Concerns in Location-Based Services: A Psychological Control Perspective. ICIS 2004 Proceedings. 2004, Volume 4. Available online: https://aisel.aisnet.org/cgi/viewcontent.cgi?article=1152&context=icis2004 (accessed on 1 March 2022).
- Xu, H.; Teo, H.H.; Tan, B.C.Y. Predicting the Adoption of Location-Based Services: The Roles of Trust and Privacy Risk. 2005. Available online: https://aisel.aisnet.org/icis2005/71/ (accessed on 1 March 2022).
- Sheng, H.; Nah, F.; Siau, K. An Experimental Study on Ubiquitous commerce Adoption: Impact of Personalization and Privacy Concerns. J. Assoc. Inf. Syst. 2008, 9, 344–376. [Google Scholar] [CrossRef]


{kind=link}
| Question | Categories | Number | Percentage |
|---|---|---|---|
| Gender | Male | 377 | 52.4% |
| Female | 343 | 47.6% | |
| Age group | 18–24 | 439 | 61.0% |
| 25–45 | 234 | 32.5% | |
| 46–63 | 46 | 6.4% | |
| 64 or older | 1 | 0.1% | |
| Experience | <3 Years | 23 | 3.2% |
| 3–10 years | 253 | 35.1% | |
| >10 Years | 444 | 61.7% | |
| Use frequency | Zero times | 224 | 31.1% |
| One time | 48 | 6.7% | |
| Two times | 56 | 7.8% | |
| Three times | 67 | 9.3% | |
| Four times | 69 | 9.6% | |
| Five times | 95 | 13.2% | |
| Six times | 43 | 6.0% | |
| Seven times | 47 | 6.5% | |
| Eight times | 36 | 5.0% | |
| Nine times | 14 | 1.9% | |
| Ten times | 21 | 2.9% |
| Construct | Item | Loading | CR | AVE |
|---|---|---|---|---|
| Effort expectancy | 0.884 | 0.657 | ||
| EE1 | Learning how to use MyKad’s HI application is easy for me. | 0.841 | ||
| EE2 | My MyKad’s HI application seldom incurs any errors when I use it. | 0.750 | ||
| EE3 | I find MyKad’s HI application easy to use. | 0.832 | ||
| EE4 | It is easy for me to complete my hospital visit within seconds by using MyKad’s HI application. | 0.816 | ||
| Facilitating condition | 0.817 | 0.529 | ||
| FC1 | MyKad holders with MyKad’s HI application do not have to bring health card anymore. | 0.747 | ||
| FC2 | Not many hospitals or medical centers recognize MyKad’s health information. | 0.769 | ||
| FC3 | Not many hospitals or medical centers have hardware and software devices which can read and write health information in MyKad. | 0.668 | ||
| FC4 | I could obtain assistance from hospitals if I have any inquiry about MyKad’s HI application. | 0.720 | ||
| Performance Expectancy | 0.920 | 0.697 | ||
| PE1 | Using MyKad’s HI application helps me accomplish a quick verification process at hospitals. | 0.833 | ||
| PE2 | Using MyKad’s HI application increases the reliability of my personal medical history. | 0.864 | ||
| PE3 | MyKad’s HI application allows doctors to know their patient’s health information immediately. | 0.856 | ||
| PE4 | MyKad’s HI allows paperless transaction (without filling in a medical form). | 0.797 | ||
| PE5 | It saves a lot of time in searching patient’s previous health record. | 0.824 | ||
| Social influence | 0.832 | 0.624 | ||
| SI1 | The fact that most Malaysian have MyKad effects my intention to use MyKad’s HI application. | 0.809 | ||
| SI2 | Malaysian government’s encouragement effects my intention to use MyKad’s HI health application. | 0.841 | ||
| SI3 | My peer group affects me to apply for MyKad’s HI application. | 0.714 | ||
| Habit | 0.898 | 0.747 | ||
| HB1 | The use of MyKad health information application has become a habit for me. | 0.899 | ||
| HB2 | I am ’habited’ to using MyKad’s HI application while visiting hospitals. | 0.908 | ||
| HB3 | I must use MyKad’s HI application. | 0.781 | ||
| Hedonic motivation | 0.878 | 0.644 | ||
| HM1 | Using MyKad’s HI application is enjoyable, e.g., simple thumbprint verification. | 0.813 | ||
| HM2 | Using MyKad’s HI application is nice for an accurate diagnosis of disease in emergencies. | 0.830 | ||
| HM3 | I feel more satisfied when I use health information application in MyKad. | 0.828 | ||
| HM4 | Using MyKad’s HI application offers me new experiences. | 0.735 | ||
| Price value | 0.830 | 0.620 | ||
| PV1 | The replacement cost of MyKad with an activated HI application due to damage is reasonable. | 0.700 | ||
| PV2 | I have applied for MyKad as HI application because it is free of charge. | 0.787 | ||
| PV3 | MyKad with an activated HI application is a good value for the application processing fee. | 0.867 | ||
| Trust in SNIC | 0.921 | 0.659 | ||
| IT1 | MyKad’s HI application has enough security to make me feel comfortable using it | 0.787 | ||
| IT2 | I feel assured that legal structures adequately protect me from problems on the use of MyKad’s HI application. | 0.790 | ||
| IT3 | I trust the technology that MyKad’s HI application is using. | 0.800 | ||
| IT4 | I trust in the ability of MyKad’s HI application to protect my health privacy. | 0.840 | ||
| IT5 | I trust in MyKad as a HI application. | 0.828 | ||
| IT6 | I have confidence in the reliability and integrity of the MyKad’s HI application transaction. | 0.826 | ||
| Privacy Concern | 0.887 | 0.612 | ||
| PC1 | I am concerned about the privacy of my health information while using MyKad. | 0.718 | ||
| PC2 | I am concerned that the HI application in MyKad is collecting too much health data from me. | 0.778 | ||
| PC3 | I am concerned that the MyKad service providers will use my health data without my authorization. | 0.823 | ||
| PC4 | I am concerned that health information in MyKad may be used or edited without permission. | 0.807 | ||
| PC5 | I am concerned that my family may access my health records by pretending to be the patient. | 0.782 | ||
| Perceived Risk | 0.886 | 0.609 | ||
| PR1 | The decision of whether to use MyKad’s HI application is risky. | 0.753 | ||
| PR2 | I perceive that HI in MyKad can be accessed by unauthorized individuals without my knowledge. | 0.780 | ||
| PR3 | I feel vulnerable when using HI application in MyKad. | 0.764 | ||
| PR4 | I believe that there could be negative consequences from using HI application in MyKad. | 0.789 | ||
| PR5 | There would be a high potential for privacy loss associated with storing health information into MyKad. | 0.813 | ||
| Perceived credibility | 0.857 | 0.666 | ||
| PCR1 | I perceive that it is secure to load health information into my MyKad. | 0.825 | ||
| PCR2 | MyKad’s HI application is difficult to be forged. | 0.801 | ||
| PCR3 | The MyKad’s HI application is well established. | 0.821 | ||
| Behavioral intention | 0.932 | 0.821 | ||
| ITU1 | I intend (expect) to continue using MyKad’s HI application in the near future. | 0.877 | ||
| ITU2 | I will always try to use MyKad’s HI application in my daily life. | 0.919 | ||
| ITU3 | I plan to continue using MyKad’s HI application frequently. | 0.922 | ||
| Use behavior | 1.000 | 1.000 | ||
| AU1 | Per 10 times, how many times you use HI application in MyKad when required by the respective authorities. | 1.0 |
| UB 1 | EE 2 | FC 3 | HB 4 | HM 5 | TS 6 | BI 7 | PC 8 | PCR 9 | PE 10 | PR 11 | PV 12 | SI 13 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| UB | |||||||||||||
| EE | 0.288 | ||||||||||||
| FC | 0.065 | 0.598 | |||||||||||
| HB | 0.425 | 0.676 | 0.335 | ||||||||||
| HM | 0.244 | 0.783 | 0.568 | 0.614 | |||||||||
| TS | 0.286 | 0.724 | 0.433 | 0.606 | 0.712 | ||||||||
| BI | 0.359 | 0.550 | 0.360 | 0.489 | 0.565 | 0.593 | |||||||
| PC | 0.040 | 0.354 | 0.442 | 0.193 | 0.348 | 0.303 | 0.248 | ||||||
| PCR | 0.325 | 0.568 | 0.410 | 0.473 | 0.573 | 0.628 | 0.491 | 0.467 | |||||
| PE | 0.154 | 0.597 | 0.586 | 0.359 | 0.643 | 0.536 | 0.455 | 0.367 | 0.359 | ||||
| PR | 0.125 | 0.329 | 0.373 | 0.233 | 0.328 | 0.266 | 0.184 | 0.628 | 0.498 | 0.229 | |||
| PV | 0.379 | 0.748 | 0.510 | 0.739 | 0.784 | 0.739 | 0.609 | 0.348 | 0.568 | 0.533 | 0.428 | ||
| SI | 0.294 | 0.729 | 0.628 | 0.637 | 0.658 | 0.624 | 0.522 | 0.328 | 0.549 | 0.630 | 0.335 | 0.722 |
| DV: Behavioral Intention | UTAUT2 1 | UTAUT2 with Privacy Calculus Model | VIF |
|---|---|---|---|
| 0.339 | 0.338 | ||
| Adj. | 0.332 | 0.332 | |
| Performance Expectancy | 0.013 *** | 0.013 *** | 1.731 |
| Effort expectancy | 0.010 ** | 0.010 ** | 2.304 |
| Social influence | 0.004 * | 0.004 * | 1.797 |
| Facilitating condition | 0 | 0 | 1.559 |
| Hedonic motivation | 0.013 *** | 0.013 *** | 2.234 |
| Price value | 0.028 **** | 0.028 **** | 1.918 |
| Habit | 0.010 ** | 0.010 ** | 1.749 |
| DV: use behavior | |||
| 0.196 | 0.202 | ||
| Adj. | 0.193 | 0.196 | |
| Behavioral intention | 0.053 **** | 0.045 **** | 1.477 |
| Facilitating condition | 0.008 ** | 0.007 ** | 1.322 |
| Habit | 0.100 **** | 0.079 **** | 1.451 |
| Perceived risk | 0.006 ** | 1.441 | |
| Privacy concern | 0.045 ** | 1.503 | |
| Trust in SNIC | 0.001 | 1.742 | |
| New relationships incorporated into UTAUT2 | |||
| Social influence → trust in SNIC | 0.272 **** | 1.069 | |
| Perceived risk → trust in SNIC | 0.017 ** | 1.069 | |
| Perceived credibility → performance expectancy | 0.001 | 1.535 | |
| Perceived Risk → performance expectancy | 0.008 ** | 1.187 | |
| Trust in SNIC → performance expectancy | 0.189 **** | 1.37 | |
| Perceived risk → privacy concern | 0.397 **** | 1 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bile Hassan, I.; Murad, M.A.A.; El-Shekeil, I.; Liu, J. Extending the UTAUT2 Model with a Privacy Calculus Model to Enhance the Adoption of a Health Information Application in Malaysia. Informatics 2022, 9, 31. https://0-doi-org.brum.beds.ac.uk/10.3390/informatics9020031
Bile Hassan I, Murad MAA, El-Shekeil I, Liu J. Extending the UTAUT2 Model with a Privacy Calculus Model to Enhance the Adoption of a Health Information Application in Malaysia. Informatics. 2022; 9(2):31. https://0-doi-org.brum.beds.ac.uk/10.3390/informatics9020031
Chicago/Turabian StyleBile Hassan, Ismail, Masrah Azrifah Azmi Murad, Ibrahim El-Shekeil, and Jigang Liu. 2022. "Extending the UTAUT2 Model with a Privacy Calculus Model to Enhance the Adoption of a Health Information Application in Malaysia" Informatics 9, no. 2: 31. https://0-doi-org.brum.beds.ac.uk/10.3390/informatics9020031