
Emerging Challenges and Opportunities in Pharmaceutical Manufacturing and Distribution




Centre for Process Systems Engineering, Department of Chemical Engineering, Imperial College London, South Kensington Campus, London SW7 2AZ, UK
*
Author to whom correspondence should be addressed.
Processes 2021, 9(3), 457; https://0-doi-org.brum.beds.ac.uk/10.3390/pr9030457
Submission received: 11 January 2021
/
Revised: 18 February 2021
/
Accepted: 25 February 2021
/
Published: 3 March 2021
(This article belongs to the Special Issue Expanding the Horizons of Manufacturing: Towards Wide Integration, Smart Systems and Tools)
Abstract
:The rise of personalised and highly complex drug product profiles necessitates significant advancements in pharmaceutical manufacturing and distribution. Efforts to develop more agile, responsive, and reproducible manufacturing processes are being combined with the application of digital tools for seamless communication between process units, plants, and distribution nodes. In this paper, we discuss how novel therapeutics of high-specificity and sensitive nature are reshaping well-established paradigms in the pharmaceutical industry. We present an overview of recent research directions in pharmaceutical manufacturing and supply chain design and operations. We discuss topical challenges and opportunities related to small molecules and biologics, dividing the latter into patient- and non-specific. Lastly, we present the role of process systems engineering in generating decision-making tools to assist manufacturing and distribution strategies in the pharmaceutical sector and ultimately embrace the benefits of digitalised operations.
1. Introduction
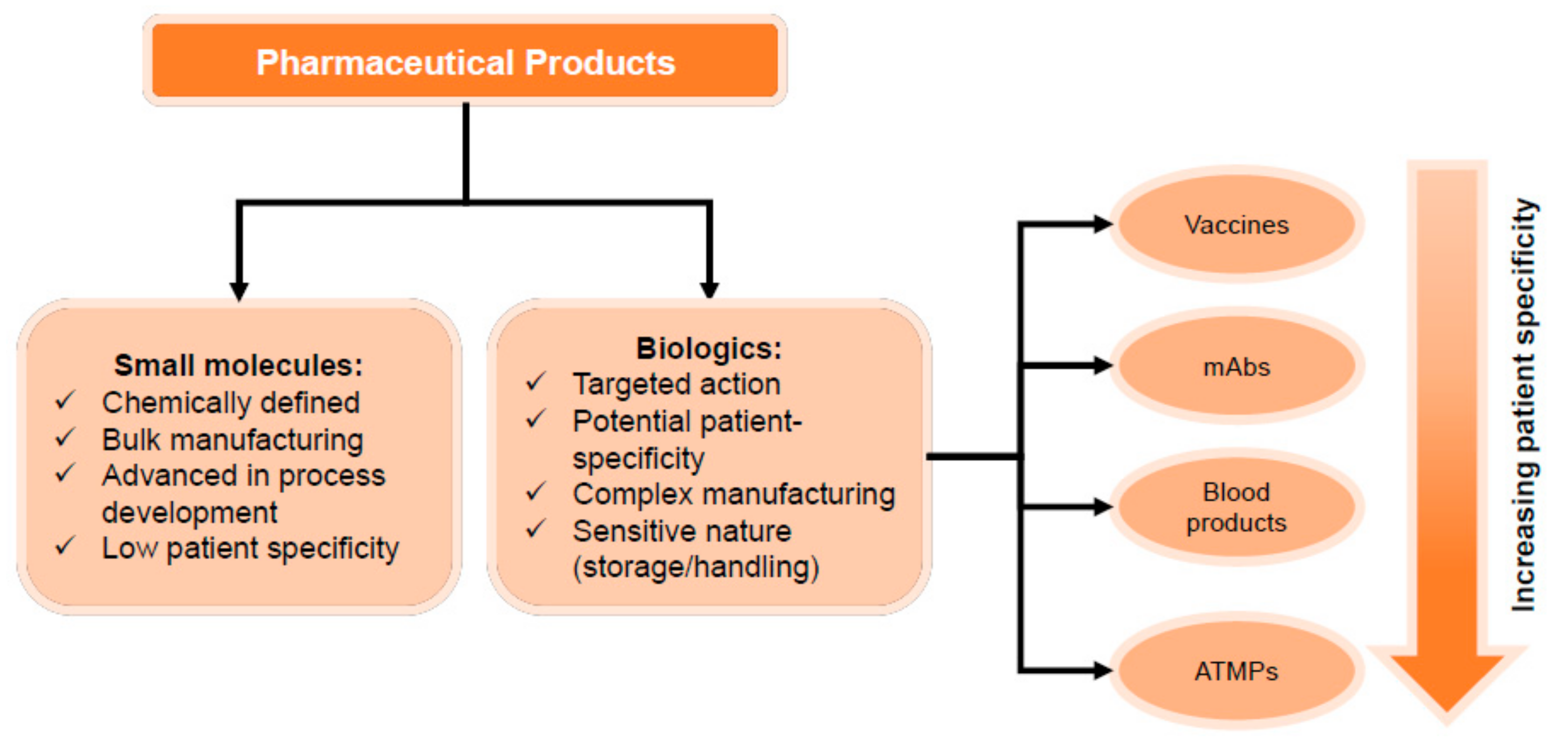
Complexity in pharmaceutical manufacturing and distribution is highly dependent on the product nature. Therapeutic drugs can be classified into two broad categories: (a) small molecules, (b) biologics. The former refers to chemically synthesised drugs, while the latter refers to products that involve components extracted from or produced by a living organism [1]. Biologics include monoclonal antibodies (mAbs), vaccines, blood products, and advanced therapy medicinal products (ATMPs). Figure 1 illustrates the drug categories considered here. Each of these products is characterised by key specifications and/or formulation that dominate decisions related to its manufacturing and supply chain. Small molecules are pharmaceuticals based on chemical components and characterised by large scale manufacturing. On the other hand, manufacturing of biologics involves cell-based production systems and complex downstream separation trains, largely performed in batch/semi-batch mode [2,3]. This often presents challenges in the optimisation and scale up of unit operations.
Enhanced clinical disease understanding has led the pharmaceutical industry to move from one-size-fits-all approaches and develop targeted therapeutics such as ATMPs. Their production process differs significantly from small molecules or mAbs as it involves a series of product- and often patient-specific steps [4]. Their patient-specific nature may challenge scale up and distribution and has led to a shift in the manufacturing and supply chain status quo, highlighting the need for smaller, more agile, and often regional manufacturing units that translate into distributed networks closer to the patient. In addition, such products are coupled with stringent distribution timelines and tight storage constraints that need to be satisfied. As a result, questions related to optimal number and location of facilities arise, as well as how can one design a robust investment planning model. Furthermore, network and task coordination become of primary importance as the supply chain becomes more complex. Once the network has been designed, manufacturers need to ensure that distribution and storage conditions are met and maintained throughout the product journey, in order to reduce losses due to product degradation that can lead to drug shortages or reduced quality.
In this paper, we discuss how the nature of therapeutics may impact the design of suitable manufacturing processes and supply chain networks. We have performed a literature review and we summarise some of the latest initiatives taken to assist the decision-making process in the pharmaceutical industry. We also discuss how process systems engineering has been aiding innovation in this space. In the last part of this paper, we present a perspective on current and future developments in this space.
2. Engineering Challenges and Opportunities in Pharmaceutical Manufacturing and Supply Chain
Recently, the term Pharma 4.0 has been introduced, referring to the adaptation of digital strategies and tools of Industry 4.0 principles, and their application to pharmaceutical manufacturing and supply chain practices [5,6]. In this context, digital tools and orchestration platforms are being developed under Industry 4.0/5.0 principles [7]. The term refers to manufacturing digitalisation and automation of processes, introducing autonomous, computerised systems. It utilises different types of mathematical models (e.g., statistical, kinetic) and Internet of Things to facilitate and maintain internal communication within and across the factories. Application of Industry 4.0/5.0 principles aims to facilitate: (a) data collection, analysis, and interpretation, (b) man-machine co-operation, (c) online monitoring and control, and (d) intra- and inter-facility data sharing. In the last few years, we have seen the emergence of cloud-based applications coming to assist decision-making in the pharmaceutical industry. Several industrial players have embraced Pharma 4.0 either through the development of digital platforms to be used by manufacturers (e.g., Siemens) or by integrating digitalisation into their manufacturing processes (e.g., ChemeCon GmbH) [8].
2.1. Manufacturing
Pharmaceutical manufacturing is divided in two main parts: firstly, the pharmaceutical ingredient or drug (active pharmaceutical ingredient (API)/drug substance) is being produced, while the second step is focused on making this product suitable for administration to the patients (drug product). Common process steps usually involve drug formulation-specific and therefore differ across drug types. Often, small molecule primary manufacturing involves chemical synthesis and purification steps, while secondary manufacturing starts with the mixing of the API with excipients, followed by granulation, compression, coating, and packaging. On the other hand, biologics involve the production of either the API or parts of the drug product by a living organism. For example, mAbs are produced in mammalian cell culture systems using bioreactors, a process referred to also as upstream (USP) [2]. Following USP, the product undergoes a series of separation/purification steps, including filtration and chromatography to ensure that impurities are removed from the final formulation. Different to all other categories, ATMPs, such as chimeric antigen receptor T (CAR-T) cells, often involve one or more patient-specific steps [9]. Autologous CAR-T cells are a representative example as their manufacturing is based on T cells that have been extracted from the patient’s blood stream [10,11].
Pharmaceutical manufacturers are focused on delivering efficacious and safe products at quantities that meet the global demand. In addition, process and product standardisation are primary goals to ensure batch-to-batch variability is minimised. In parallel, production processes need to be economically viable, adding to the complexity of identifying the best candidate design(s). These are often conflicting objectives (Table 1) that require systematic procedures for the identification of the most suitable operating units and modes that will meet product specifications, while yielding a profitable process. In an effort towards process improvement and modernisation, the pharmaceutical industry has pioneered by creating new and/or adapting existing innovations. Here, we present some of them and discuss the challenges that remain open in each space.
2.1.1. Quality by Design
The emergence of biologically derived drugs has underlined the necessity for thorough system understanding that includes detailed mapping of how process conditions may affect product quality. Quality by design (QbD) was firstly discussed by Juran [12] in 1992 and refers to the integration of quality into the process and product. In other words, all design and operation decisions are taken aiming to meet a predefined product quality. In the pharmaceutical industry, QbD has been increasingly endorsed by regulators and adapted by manufacturers [13,14,15,16], while in recent years it has become an integral part of approval submission dossiers. QbD suggests that firstly the quality target product profile (QTTP) needs to be decided, followed by the identification of the critical quality attributes (CQAs) [16,17]. CQAs are defined as product properties and/or characteristics that need to be within certain limits. The process is then designed, aiming to meet the pre-defined QTTP, while maintaining CQAs within the allowed threshold. This is achieved by manipulating those process parameters that directly affect CQA performance, known as critical process parameters (CPPs). QbD offers a systematic procedure for the development of processes based on thorough system understanding and prior knowledge integrated to the design and operation. Efforts have been made to integrate mathematical models with QbD principles to explore CPP-CQA interplay. Such understanding enables the determination of a set of feasible points within the space of the operating conditions that assure that the CQAs are within specifications, known also as “design space” (DS). This has allowed manufactures to move away from uniquely optimal operating profiles and adopt a more flexible strategy, whereby the manufacturing process is approved to operate within the DS and allowing greater flexibility for post-approval improvements within the DS.
Despite the wide application of QbD in mAbs and lately in vaccines, when it comes to ATMPs, QbD-driven processes remain an open challenge [18]. The often patient-/donor-specific nature of the starting material renders systematic CQA identification impossible to perform. In addition, the manufacturing performance of cell-based therapies is highly dependent on the quality of the extracted cells, leading therefore to a highly variable CPP-CQA interplay. As ATMP manufacturing matures and more understanding on the optimal portfolio of conditions is gained, QbD principles can be adapted to incorporate patient profile and incoming materials as key CPPs and map their impact on the process and product performance.
2.1.2. Continuous Manufacturing
Process performance has been the driver for many of the latest advances in the pharmaceutical industry, such as the one of continuous manufacturing (CM). CM offers the possibility for robust processes that involve smaller equipment size. In addition, by running longer and producing higher product yields, CM processes can lead to decreased batch-to-batch variability and therefore minimise the risk of drug shortages due to unmet quality specifications [19,20]. On the other hand, operating in continuous mode is translated into a must-have requirement of rapid, online measurements and a high level of process understanding to allow the operator to ensure that the product will meet specifications. This is of utmost importance in CM as its plug-and-play profile means that an intermediate intervention is not possible which translates into a significant financial and shortage risk if the process deviates from the optimal significantly. CM is one of the most discussed trends and innovations of the latest years in the pharmaceutical industry, endorsed by regulators [21]. Promising eco-efficient processes of higher productivity, CM has been successfully applied in many existing production processes leading to significant improvements [19]. Small molecules have seen applications of CM early on with the initiatives from Novartis-MIT on continuous crystallisation [22] and the GSK-Pfizer partnership for the development of continuous processing technology for oral solid dosage (OSD) drugs [23]. Innovation has been demonstrated in the space of biologics as well with Genzyme and Bayer as leading adapters of perfusion and other continuous manufacturing processes [24], while Novasep, GE Healthcare, Knauer, and ChromaCon are some of the equipment manufacturers offering small- and pilot-scale continuous chromatography systems. Warikoo et al. [25] demonstrated one of the first fully continuous pilot-scale bioprocesses for the production of a mAb and a recombinant human enzyme. They designed and used a system composed by a 12 L perfusion bioreactor connected to 4-column periodic counter-current chromatography and they successfully demonstrated the production and purification of the desired products. Godawat et al. [26] showcased an end-to-end continuous bioprocess using a perfusion bioreactor connected to an ATF cell retention device. The upstream mixture was then processed by two 4-column PCC systems. Additionally, Karst et al. [27] presented a lab-scale continuous mAb production process using a perfusion cell culture, a surge tank, and a continuous capture process.
Despite the success of CM in small molecules, challenges still exist that prevent biologics from reaching a fully continuous process at scale. A significant percentage of this slower adaptation can be attributed to system complexity. Relying on living organisms as production systems, biologics are coupled with complex process dynamics that challenge the identification and maintenance of the optimal operating profile. Although, CM promises more stable processes and decreased batch-to-batch variability, it requires increased certainty that the optimal operating conditions will be maintained throughout the process. This is to ensure that the desired product will meet specifications and reduce financial and supply risks associated to out-of-spec batches. To enable the design of robust processes that are continuously monitored requires suitable analytics to be in place. Despite advances in the field of continuous online measurements [28,29,30,31,32], process analytical technologies (PATs) are yet to be further developed in order for uninterrupted CM to be realised. Focusing on biologics and specifically mAbs, another limiting step that hinders end-to-end continuous processing is upstream/downstream (USP/DSP) integration. Process intensification via process integration in mAbs is a challenge, firstly as DSP units are not at the scale to handle the volumes produces by the USP counterpart. A way to mitigate this would be scaling up DSP equipment, risking increasing the already high DSP cost (80% of the end-to-end process).
Aiming to tackle this, initiatives have been made towards the development of smaller scale separation units, operating in continuous mode, increasing therefore their volume processing capabilities [26,33,34]. Another alternative could be to scale out the DSP step, offering also higher operating flexibility. Some of the remaining challenges are currently being tackled through the development of computer-modelling platforms as discussed later in the manuscript. Manufacturing challenges increase as products become more specialised. For example, CAR-T cells (ATMPs) are manufactured using closed-box production platforms that do not allow for task parallelisation or scale up [35,36]. This translates into integrated lines of unit operations being occupied for the entire manufacturing (>10 days) duration of a single therapy before they can become available to receive the next one. As ATMPs gain momentum, manufacturers will be required to increase their capacity. Given that volumetric scale up is not possible, other possibilities can be explored, such as scale-out, referring to multiple suites running in parallel or a completely granular manufacturing procedure where every step is performed in a separate unit, allowing therefore for sequential manufacturing with decreased waiting times. The latter model could greatly benefit from process intensification initiatives as it resembles the well-known model of biologics.
2.2. Supply Chains
Supply chain design decisions, strategies, and operations are highly dependent on the product that is delivered to the patient. With increasingly complex portfolios and stringent regulations to deliver an effective and safe therapy to end-users, pharmaceutical supply chains costs are on the rise. The nature of the product type, from the chemically-derived small molecules to highly targeted biologics, such as mAbs and ATMPs, entails different distribution and storage challenges [37]. Table 1 summarises the main challenges faced in pharmaceutical supply chains and related innovations.
2.2.1. Demand Scales
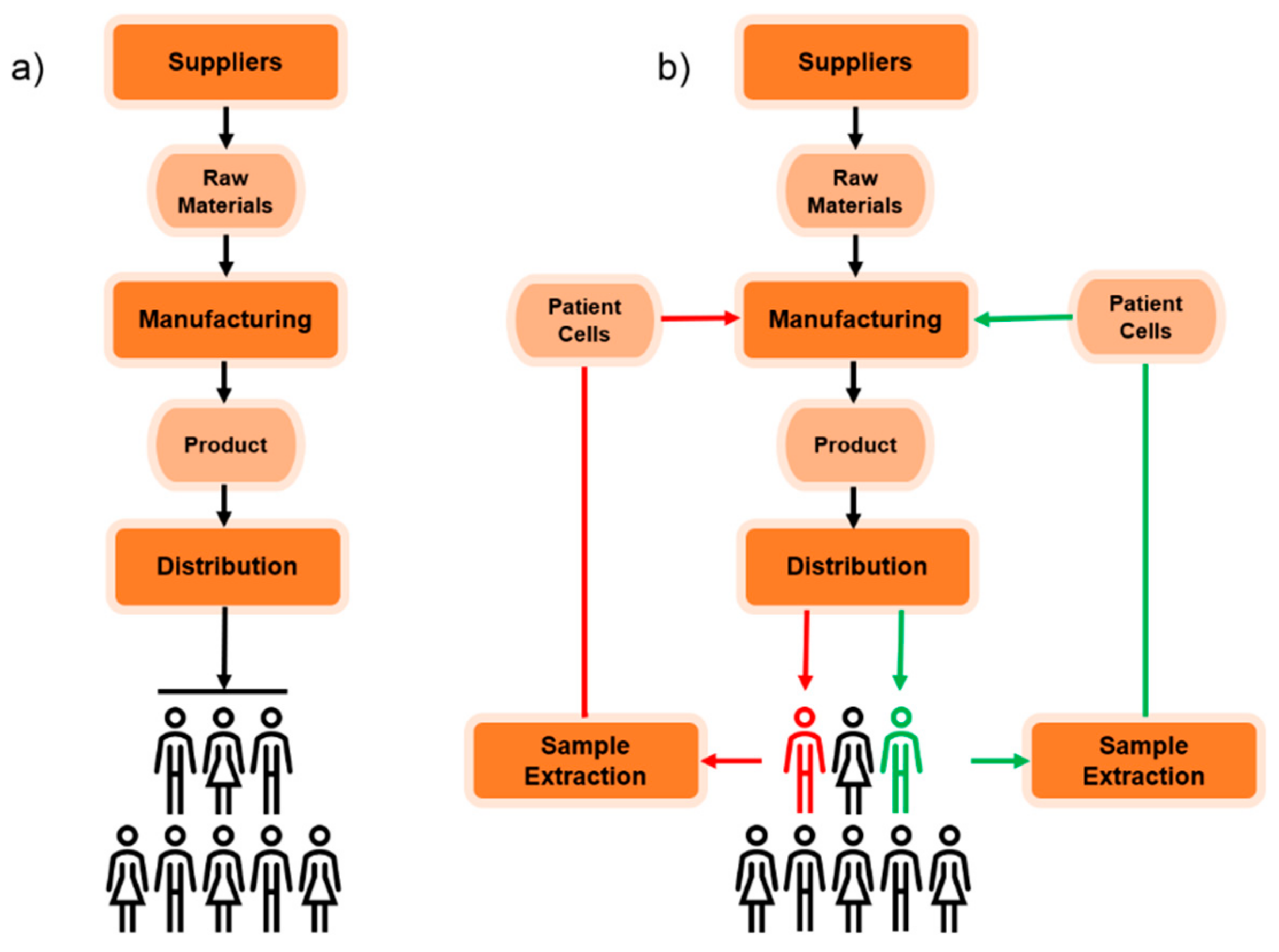
The pharmaceutical industry is inherently global, and its supply chains comprise a network of manufacturers (primary and secondary), which include in-house or external contractors, packaging facilities, regional distribution centres (wholesalers), and final healthcare providers, such as hospital and pharmacies. Off-the shelf products, prescription drugs and vaccines can be produced on a large scale, with single manufactured batches delivering numerous patient non-specific doses, following a one-size-fits-all distribution approach. This strategy is preserved in the case of emerging specialty drug products as well. Demands for these products, which are often biologics, including mAbs, can be predicted to be smaller in scale as they provide treatment of rare and complex chronic diseases, which only certain patient subgroups present. However, as the complexity of the treatment increases, it becomes increasingly difficult to synthesise a product that is compatible with the entire patient cohort. In the case of ATMPs, distribution has been envisioned through two channels: allogeneic and autologous. Allogeneic therapies are manufactured in larger batches from unrelated donor tissues [38]. Off-the-shelf production offered by the allogenic route is presenting several donor-patient matching challenges which have slowed down the success of these therapies in clinical trials. By contrast, autologous ATMPs have thus far been more successful clinically [9] and have the potential to reconfigure standard supply chain structures, as they represent a turning point in the feasibility of personalised medicines. Figure 2 illustrates the general supply chain structure for batch-produced drugs and patient-specific therapeutics. In the instance of CAR-T cell therapies, a sample of cells is extracted from the patient, shipped, modified, and administered to the patient, with a minimised cycle time (17–19 days return time for leading commercial products) [39,40,41,42]. The supply chain for these therapies is closer to the customer and the need for a 1:1 business model emerges, where the product released by a single batch is patient-specific. Opportunities of scale up are limited and decentralisation of manufacturing is a promising approach [43]. Companies, expanding their primary and specialty drugs portfolios to personalised therapeutics, are expected to deal with a spectrum of decoupled demands simultaneously, which require extensive coordination of the stakeholders in the supply chain [44].
2.2.2. New Players
The pharmaceutical ecosystem comprises large R&D multinationals, local companies, generic manufactures, contract development, and manufacturing organizations (contract manufacturing organisations, CMOs, and contract and development manufacturing organisations, CDMOs) and biotechnology companies [45]. Large R&D multinationals are the key players in the marketplace, with presence in branded products and manufacturing sites across many locations. In recent years, their research focus has shifted to unmet needs of smaller patient populations, such as prevention and cure of rare diseases [46]. The increasing complexity of novel targeted therapeutics and lack of in-house manufacturing expertise of large multinationals in these contexts have determined an increased in mergers and acquisition (M&A) and outsourcing strategies through CMOs or CDMOs [46]. For instance, CellforCure was acquired by Novartis, expanding the company’s manufacturing capabilities in CAR-T cell therapies, Hitachi acquired Aptech to increase manufacturing capabilities in Europe, Thermo Fisher acquire CMO Brammer Bio for $1.7 bn and GE Healthcare was acquired by Danaher ($21.4 bn) [43]. CMOs and CDMOs are equivalently attractive for biotechnology companies, which are often the main innovators in genetically engineered therapeutics, but lack of manufacturing resources and liquidity for in-house manufacturing. As the number of stakeholders involved in clinical and commercial supply chains increases, end-to-end monitoring of CQAs becomes increasingly difficult [47]. Outsourcing distribution and handling to specialised contract logistic providers is an appealing option to assure safe and secure delivery of complex biological drug products; however, management and coordination between the multiple agents becomes the key challenge.
2.2.3. Logistics Considerations
Manufacturers indicate on the product label the stability conditions for the product, which must be maintained throughout the whole supply chain. Small molecule drug products can typically be stored at 25 °C [43]. By contrast, the stability of bioproducts is highly compromised by temperature excursions and shocks. For instance, blood products, conventional vaccines (e.g., live-attenuated viruses) and monoclonal antibodies must be transported and stored under refrigeration conditions of 2–9 °C [48]. If cold chain logistics introduce additional costs in the supply chain, these are further exacerbated when handling ATMPs. CAR-Ts can be stored and transported either fresh (−80 °C) or cryopreserved (−180 °C), depending on the manufacturing practice, noting that they are also highly sensitive to shear stress and vibrations, because of their cell-based nature [9]. This ensures stability, maintains viability, and prevents genetic changes. Other genetically engineered products, such as mRNA vaccines, must be stored and handled under similar conditions (−70 °C) [49]. Monitoring the CQAs in relation to storage and transport environment conditions and ensuring timely delivery of therapies becomes increasingly crucial as the product structure and scope increases in complexity. Whether distribution is tackled in-house or outsourced, transparency of manufacturing and logistics operations facilitates quality assurance and effectiveness of the entire supply chain [47].
2.2.4. End-to-End Monitoring
CAR-Ts and personalised therapies offer a new perspective on the importance of track and trace capabilities for supply chain management and real-time monitoring. In these supply chains, chain of identity (COI) and tracking is crucial in order to ensure return of the therapy to the right patient by the end of the product cycle [9]. In addition, chain of custody (COC) principles must be applied with the aim of recording data related to handling, collection, and performed actions on the sample, thus monitoring the patient-specific product profile closely. It is worth noting that potential success of off-the-shelf ATMPs will equally require donor information to be tracked throughout the supply chain to ensure compatibility and aid effective donor-patient matching. Patients will also need to be monitored for several years after receipt of therapy; this information should be used to improve therapy design wherever possible. Initiatives to improve end-to-end visibility of supply chains are emerging in the fields of conventional non-specific products as well, such as Merck KGaA’s commitment to utilise data analytics to predict and prevent drug shortages [50]. Companies are in fact becoming more aware of the improved supply-and-demand forecasting that traceability offers, including its potential to prevent API stock-outs and counterfeit drugs from entering the supply chain. As discussed above, drugs, including targeted biologics and small molecules, can also greatly benefit from real-time monitoring of CQAs, as the risk of failing to comply with labelled requirements can be reduced.
As highlighted by Papathanasiou [51], cloud-based platforms can facilitate communication and seamless connection between stakeholders. Maintaining and upgrading data security will though become a constant requirement for reducing vulnerabilities to the increasing sophistication of cyber-attacks. Particularly, secure safeguarded systems to protect data will become central to foster patient trust for data sharing and conduct the research needed to drive personalised medicine [52]. Alongside cloud-based solutions, blockchain-based alternatives are being developed in recent years. In a nutshell, blockchain is part of the broader category of distributed ledger technologies (DLTs) and it is based in the participation of a network of devices, called nodes, that keep a copy of the database [53]. A distinct advantage of the blockchain is that it does not require a central trusted party to verify the validity of the data but it relies on a consensus protocol which is publicly available and agreed upon by all the participants [54]. The information stored in the blockchain is public, immutable, and tamper-proof, while the security of the sensible data is assured by the utilization of strong state-of-the-art cryptographic algorithms. By adopting the blockchain a unified distributed health records database that can be accessed by every stakeholder along the supply chain, from the raw material providers to the final patient, with different levels of access to the information. For instance, information about the QC and storage conditions of a therapy along the supply chain could be accessed by everyone at any time by scanning a QR code attached to the therapy, while patient-specific data would be cryptographically sealed for most of the stakeholders except the patient himself and the hospital. An extensive review of blockchain solutions in the healthcare sector is out of the scope of this work and can be found elsewhere [55]. Despite the great potential, scalability of blockchain application remains an issue and is yet to be demonstrated. An interesting use-case is the recent partnership between NHS England and Hedera Hashgraph, a company providing blockchain-based solutions, in an attempt to use blockchain for enabling cold chain monitoring of COVID-19 vaccines for a selected group of facilities [56]. Other examples of blockchain-based tools for real-time monitoring of storage conditions of sensitive goods and traceability solutions are being developed by Modum.io [57] and is under investigation in a leading Italian company of the ophthalmic sector [53].
2.2.5. Production Planning and Scheduling
Despite the exciting opportunities brought by digitalisation and advanced monitoring, well-established technologies still present a large margin of improvement in terms of adaptability of production levels to demand. One of the main bottlenecks of current manufacturing and distribution networks, for both small molecules and conventional biologics is the planning and scheduling of production in response to short-term demand fluctuations [45]. Primary manufacturing sites usually comprise multipurpose batch equipment setups to distribute the capital cost over a spectrum of products. In the instance of biopharmaceutical manufacturing, such as manufacturing of mAbs, perfusion and fed-batch modes are preferred modes of operation due to improved fermentation titres [58]. Significant losses in revenues can result from downtime due to changeovers and required extensive cleaning tasks to prevent contamination. This pushes manufacturers to operate the site in long product campaigns, which ensure profitable utilisation of the plant throughout the time horizon [45,59]. Small molecule drug substances exiting the primary sites are stored up to 1 year and can be further processed in secondary manufacturing sites upon demand. Simpler tasks of fill and finish and packaging taking place in this secondary stage allow more flexible scheduling of operations and supply products to distribution centres.
The intermediate storage installations between drug substance and drug product manufacturing can act as a buffer to tackle variations in market dynamics: the customer-facing end (hospitals and pharmacies) place orders on wholesalers, carry out an assessment on inventory levels and if necessary, place orders upstream. In the event of an API shortage, the lack of responsiveness of primary manufacturing long campaigns emerges, which can then lead to drug product shortages and impact patients in need of the therapy. Stockpiling has been a profitable option for well-established chemically synthesised drug products; however, it is not always the best-suited solution for more complex and expensive biologics with short shelf lives. The high value of these products constrains the size of product inventory held as this might constitute tying up working capital [60]. Off-the-shelf production has followed the above planning paradigm for years, but patient-specific therapies come to reshape this approach. Scheduling production becomes patient scheduling, where each batch contains solely a dose of therapy that is specific to the patient [9]. The business model changes radically and adaptation to demand dynamics becomes increasingly important as operations are now constrained by return times between collection of the sample at the start of the supply chain, manufacturing, product release, and re-infusion.
2.2.6. Capacity and Investment Planning
Investment planning into expansions, establishment, and shutdown of facilities would have to be carried out under high uncertainty of demand of pipeline products and drugs under development. In order to avoid financial losses related to poor forecasting and suboptimal utilisation of facilities, R&D companies are externalising development and manufacturing of novel entries in their portfolio to contractors. The problem of capacity management is outsourced to the CMO, which is able to better balance utilisation by making products for multiple innovators [43]. Stainless-steel plants are well-established production facilities for conventional vaccines, mAbs, small molecule products and are suitable for large scale production. The capital investment for these facilities can extend from $500 M to $1 bn [61], highlighting the financial losses that can derive from underutilisation of the facility. The process of setting up entirely new facilities can extend up to 5–10 years, which once more hinders flexibility and responsiveness to varying therapeutic needs of the population. It is often the case that capacity within the facility is expanded by either setting up suites in parallel or scaling up existing ones with larger equipment [62].
Nevertheless, the operational burden of cleaning tasks, contamination concerns, and the ever-present need of more flexible production as biopharmaceutical products become more advanced and complex, is pushing many companies to utilise single-use production technologies. This trend in manufacturing offers multiple advantages in terms of savings in instalment, which fall in the range of $20–$100 M (2–20% of the capital investment), and operational costs. Set up times for new facilities are shorter (1.5 years) and the advantage of parallelising production with suites is preserved, in order to cope with short-term demand changes. Interestingly, COVID-19 vaccine producers choose to rely on flexible single-use systems as opposed to traditional commercial-large scale bioreactors and fermenters, valuing the potential to install manufacturing capacity at a higher speed, which is crucial during a global health crisis [63]. The advantage of single-use equipment is seen also in the space of personalised medicines, where cross-contamination risk between products can cause loss of patient specificity and have detrimental effects on the patient’s health. Changeover time within each suite is decreased from 1 month to 0.5 days [61] as equipment components no longer require, cleaning, but are rather disposed, substituted, with an adaptable capacity to the incoming patient schedule. The environmental drawbacks of utilising high purity water and heat to clean and sterilise stainless steel equipment are removed. Disposal routes of single-use technologies is, however, still an issue to be considered. Used components are typically bio-hazardous, which entails that waste treatment tasks have to be carried out on-site prior to landfill disposal. Another option is to send used components to geographically separate waste-to-energy facilities for incineration and recovery of electricity. Latterly, initiatives, such as the Biopharma Recycling Program, are investigating recycling strategies to further reduce the environmental footprint of plastic single-use equipment and exploit the full benefits of flexible manufacturing [64].
3. Assisting Digitalisation in Pharmaceutical Industry via Process Systems Engineering (PSE)
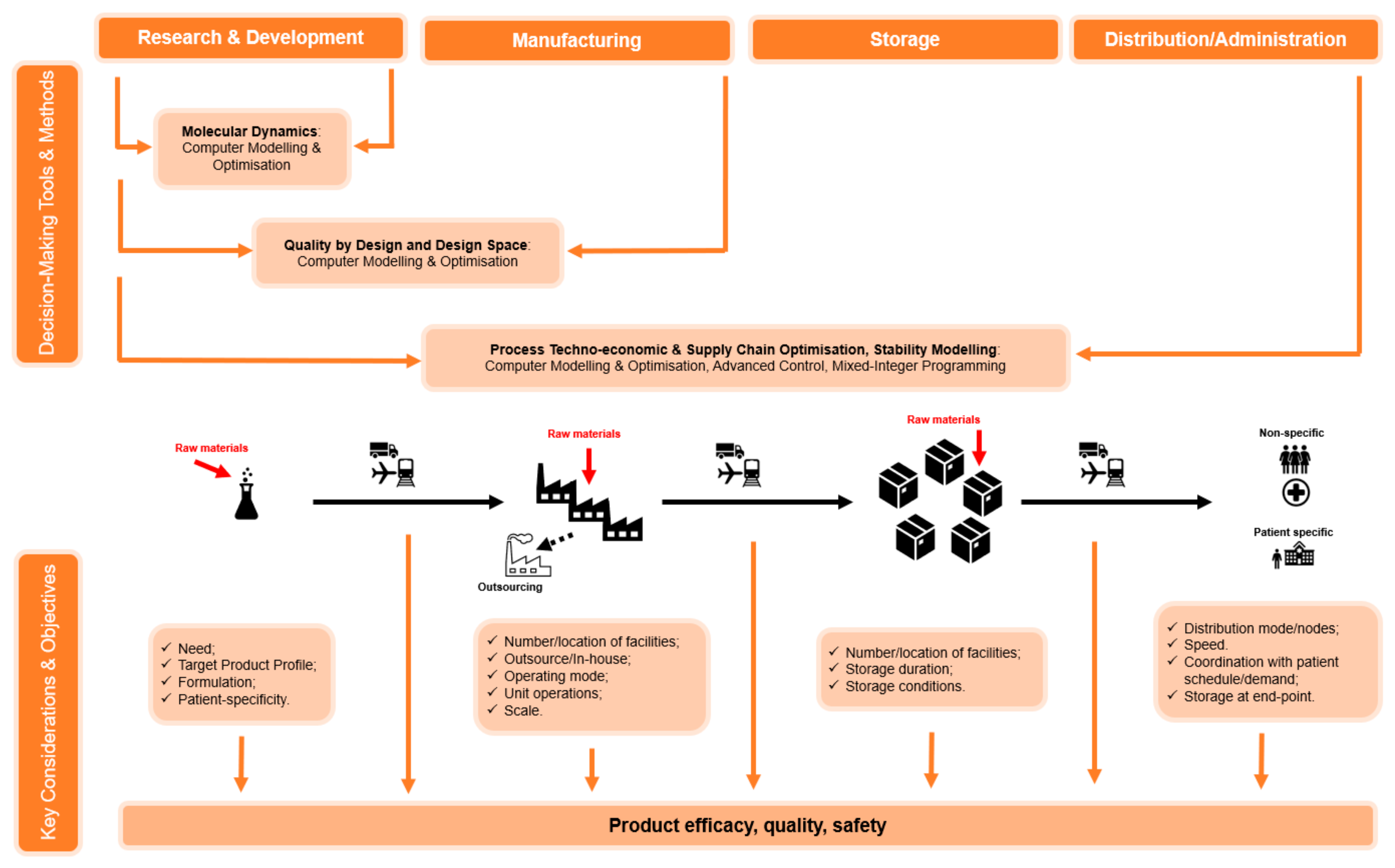
Process systems engineering (PSE) has been traditionally assisting decision making in the pharmaceutical industry [46,65,66,67,68]. The adoption of digitalisation in pharmaceutical manufacturing and the supply chain will be key for seamless data exchange across manufacturing facilities and supply chain networks, as it will allow connectivity of processes, products, and people. As highlighted previously in this manuscript, there is a wide range of opportunities to improve the strategies and operations of the entire pharmaceutical supply chain in order to meet the evolving therapeutic needs of the population. In this space, the concept of enterprise-wide optimisation [69,70] is at the core of a coordination between R&D, supply of materials, manufacturing, and distribution of pharmaceutical products. The main objectives of an enterprise-wide approach are to maximise profits, responsiveness to customer needs, resource utilisation and minimisation of costs, stock levels, and environmental footprints. This is achieved while accounting for the complex interactions between the many stakeholders of the supply chain. Instant flow of information and data sharing can also be achieved via the adoption of transactional IT tools, such as track and trace tools, cloud-based and blockchain platforms. Such tools can improve communication and operations across the supply chain, specifically in the evolving pharmaceutical ecosystem that comprises multiple players. Nevertheless, these digital tools do not provide comprehensive frameworks to support the decision-making process. Therefore, it is of paramount importance to develop analytical IT tools to explore, analyse alternatives, and predict actions for the design, planning, and operation of each of the components of the supply chain. The PSE community has largely focused on the development of sophisticated optimisation and decision-support tools so as to yield optimum performance and ensure customer satisfaction. Figure 3 presents a summary of key considerations and challenges currently faced by the pharmaceutical industry, as well as some of the most remarkable computational and other innovations that can assist the decision making.
In the pharmaceutical sector, changes introduced to approved processes and/or products need to be registered re-approved by regulators. This poses an additional challenge to the adaptation of new methods and technologies. Initiatives such as quality by design and design space identification that allow thorough process and product understanding can lead to more flexible processes and therefore faster approval procedures. In that respect, computer-based modelling initiatives and tools demonstrate significant potential as they offer lower-cost experimentation platforms and the ability to identify the optimal process operating profiles offline. Such models and platforms, also known as digital twins, find applications across a variety of activities in pharmaceutical manufacturing. Computer-based modelling in product development and manufacturing has demonstrated significant potential, offering low-cost experimentation platforms to assess CQA-CPP interplay under a vast spectrum of conditions [71,72,73]. In a similar fashion, PSE researchers are also looking to quantify parameter uncertainty and its impact on product and process performance [74,75]. From an operational standpoint, many groups are developing using digital twins for the design of optimal operating setups, optimisation profiles [76,77,78,79], and smart controllers [80,81,82] that can operate bypassing measurement unavailability.
In the field of supply chain management, optimisation-based approaches have improved strategies and operations of pharmaceutical and bio-pharmaceutical processes and distribution in multiple ways. Computational tools have been developed to seek optimal long-term strategic plans, considering the problem supply chain design and capacity planning, as well mid- and short-term decisions, addressing the problem of production planning and scheduling [69]. Supply chain design, capacity, and investment optimisation models focus on the long-term decisions regarding the strategic locations of the plants, storage, and sourcing of raw materials, contracts with CMOs and CDMOs and logistics providers as well as future investments in new capacity over the years [58,62,83,84,85,86,87]. Tools to optimise production planning and scheduling offer great potential in assisting operational, day-to-day decision-making. Systematic approaches in production planning yield estimates of production targets, inventory levels, and material flows across the supply chain over a horizon of several months [59,60,88]. Scheduling tools, instead, provide detailed sequencing of tasks and operations, fulfilling orders and meeting the production targets, relying on a more granular description of the manufacturing and distribution processes and accounting for resource constraints [89,90].
Integrating the different levels of decision-making across many time scales is an issue of great interest in research [91,92], alongside coordination between multiple geographically distributed manufacturing and storage facilities comprising the supply chain. The size of the optimisation problem becomes challenging to solve by commercially available solvers and numerous approaches, including rolling horizon, spatial [88], and temporal decomposition [88,89] schemes have been proposed in literature. Solving the above problems under uncertainty remains an open challenge [93]. Uncertainty introduced by demand fluctuations, on-going global competition and pending clinical trial results, challenges the long-term strategic decision-making. Most of the frameworks proposed in literature use stochastic programming and scenario-based approaches [85,86,94], often coupled with decomposition strategies [95] to tackle computationally intractable formulations. Case studies have mainly focused on manufacturing and distribution of chemically derived drugs and conventional biologics. Therefore, the novelty of patient-specific products and ATMPs is a fertile ground for PSE tools to support investment planning exercises and establish supply chains that can cope with the predicted demand and success of these products. Similarly, planning and scheduling tools can aid the decision-making and tackle the operational challenges brought by patient specificity and time constraints of the therapy cycle [96,97].
4. Conclusions and Outlook
In the latest years, pharmaceutical products have evolved towards disease- and patient-specific therapeutics, involving meticulous manufacturing steps. In addition, cell-based therapeutics and vaccines present high sensitivity to environmental and transport conditions, complicating supply chain logistics. Increased drug specificity and demand uncertainty are adding a further level of complexity when it comes to the design and operation of robust manufacturing processes and distribution networks. As discussed in this paper, the pharmaceutical industry has taken significant steps towards the improvement of existing and/or the development of novel processes that promise agile, responsive, and reproducible manufacturing. Similarly, distribution networks in the pharmaceutical sector are undergoing a paradigm shift, exploring the capabilities of decentralised models.
Such developments are accompanied by digital innovation in the pharmaceutical industry that comes to enable seamless communication between process units, production plants, and distribution nodes. As discussed earlier, process systems engineering has been at the forefront of enabling digitalisation through the development of computer modelling tools. The latter can assist with real-time monitoring of storage conditions that are critical for sensitive pharmaceutical products with short shelf-life, thus increasing drug safety. One of the main challenges hindering fast exploitation of Industry 4.0 principles in pharmaceutical manufacturing is the change of mindset. Practitioners should embrace the benefits arising from the realisation of Pharma 4.0 towards replacing paper-based systems with cloud-based servers. This will allow significantly improved agility and productivity in the operations of the pharmaceutical sector.
Author Contributions
Conceptualization, M.S., A.B., N.S. and M.M.P.; methodology, M.S., A.B. and M.M.P.; investigation, M.S., A.B. and M.M.P.; images/tables, M.S.; writing—original draft preparation, M.S., A.B. and M.M.P.; writing—review and editing, M.S., A.B., N.S. and M.M.P.; All authors have read and agreed to the published version of the manuscript.
Funding
Funding from the UK Engineering & Physical Sciences Research Council (EPSRC) for the Future Targeted Healthcare Manufacturing Hub hosted at University College London with UK university partners is gratefully acknowledged (Grant Reference: EP/P006485/1).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Acknowledgments
The authors would like to acknowledge expert opinion received through multiple conversations with the User Steering Committee of the Future Targeted Healthcare Manufacturing Hub. Financial and in-kind support from the consortium of industrial users and sector organisations is also acknowledged.
Conflicts of Interest
The authors declare no conflict of interest.
References
- European Medicines Agency (EMA). Biological Medicine European Medicines Agency. Available online: https://www.ema.europa.eu/en/glossary/biological-medicine (accessed on 28 December 2020).
- Papathanasiou, M.M.; Kontoravdi, C. Engineering challenges in therapeutic protein product and process design. Curr. Opin. Chem. Eng. 2020, 27, 81–88. [Google Scholar] [CrossRef]
- Shukla, A.A.; Wolfe, L.S.; Mostafa, S.S.; Norman, C. Evolving trends in mAb production processes. Bioeng. Transl. Med. 2017, 2, 58–69. [Google Scholar] [CrossRef]
- Iancu, E.M.; Kandalaft, L.E. Challenges and advantages of cell therapy manufacturing under Good Manufacturing Practices within the hospital setting. Curr. Opin. Biotechnol. 2020, 65, 233–241. [Google Scholar] [CrossRef]
- ISPE. Pharma 4.0. Available online: https://ispe.org/initiatives/pharma-4.0 (accessed on 15 February 2021).
- ISPE. Pharma 4.0: Hype or Reality. Available online: https://ispe.org/pharmaceutical-engineering/july-august-2018/pharma-40tm-hype-or-reality (accessed on 15 February 2021).
- Nahavandi, S. Industry 5.0—A Human-Centric Solution. Sustainability 2019, 11, 4371. [Google Scholar] [CrossRef] [Green Version]
- SIEMENS. Embracing the Digital Transformation. Available online: https://assets.new.siemens.com/siemens/assets/api/uuid:f06590be-f311-4966-94df-f490abcc7d40/siemens-pharma-digi-consulting-en.pdf (accessed on 15 February 2021).
- Papathanasiou, M.M.; Stamatis, C.; Lakelin, M.; Farid, S.; Titchener-Hooker, N.; Shah, N. Autologous CAR T-cell therapies supply chain: Challenges and opportunities? Cancer Gene. 2020, 27, 1–11. [Google Scholar] [CrossRef]
- Levine, B.L.; Miskin, J.; Wonnacott, K.; Keir, C. Global Manufacturing of CAR T Cell Therapy. Mol. Methods Clin. Dev. 2017, 4, 92–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, B.L. Performance-enhancing drugs: Design and production of redirected chimeric antigen receptor (CAR) T cells. Cancer Gene. 2015, 22, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Juran, J.M. Juran on Quality by Design: The New Steps for Planning Quality into Goods and Services; The Free Press: New York, NY, USA, 1992; ISBN 9780029166833. [Google Scholar]
- Warren, G. Quality by Design (QbD) Overview. 2015. Available online: https://www.pda.org/docs/default-source/website-document-library/chapters/presentations/australia/quality-by-design-(qbd)-overview.pdf?sfvrsn=f022b28e_6 (accessed on 1 February 2021).
- Yu, L.X.; Amidon, G.; Khan, M.A.; Hoag, S.W.; Polli, J.; Raju, G.K.; Woodcock, J. Understanding pharmaceutical quality by design. AAPS J. 2014, 16, 771–783. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, C.M.V. Quality by Design—FDA Lessons Learned and Challenges for International Harmonization. 2012. Available online: https://www.fda.gov/media/85369/download (accessed on 1 March 2021).
- PharmTech. EMA and FDA Release QbD Guidance. Available online: https://www.pharmtech.com/view/ema-and-fda-release-qbd-guidance (accessed on 28 December 2020).
- Eon-Duval, A.; Broly, H.; Gleixner, R. Quality attributes of recombinant therapeutic proteins: An assessment of impact on safety and efficacy as part of a quality by design development approach. Biotechnol. Prog. 2012, 28, 608–622. [Google Scholar] [CrossRef] [PubMed]
- Detela, G.; Lodge, A. Manufacturing process development of ATMPs within a regulatory framework for EU clinical trial & marketing authorisation applications. Cell Gene. Insights 2016, 2, 425–452. [Google Scholar] [CrossRef] [Green Version]
- Konstantinov, K.B.; Cooney, C.L. White paper on continuous bioprocessing 20–21 May 2014: Continuous Manufacturing Symposium. J. Pharm Sci. 2015, 104, 813–820. [Google Scholar] [CrossRef]
- Hummel, J.; Pagkaliwangan, M.; Gjoka, X.; Davidovits, T.; Stock, R.; Ransohoff, T.; Gantier, R.; Schofield, M. Modeling the Downstream Processing of Monoclonal Antibodies Reveals Cost Advantages for Continuous Methods for a Broad Range of Manufacturing Scales. Biotechnol. J. 2019, 14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chatterjee, S. FDA Perspective on Continuous Manufacturing. IFPAC Annu. Meet. 2012, 26, 34–42. [Google Scholar]
- Quon, J.L.; Zhang, H.; Alvarez, A.; Evans, J.; Myerson, A.S.; Trout, B.L. Continuous crystallization of Aliskiren hemifumarate. Cryst. Growth Des. 2012, 12, 3036–3044. [Google Scholar] [CrossRef]
- Taylor, P. Outsourcing PharmA GSK and Pfizer Team up on Continuous Manufacturing Project. Available online: https://www.outsourcing-pharma.com/Article/2015/11/03/GSK-and-Pfizer-team-up-on-continuous-manufacturing-project (accessed on 25 December 2020).
- Langer, E.S.; BioProcess International. Trends Perfusion Bioreactors the Next Revolution Bioprocessing? Available online: https://bioprocessintl.com/upstream-processing/bioreactors/trends-in-perfusion-bioreactors-323459/ (accessed on 23 December 2020).
- Warikoo, V.; Godawat, R.; Brower, K.; Jain, S.; Cummings, D.; Simons, E.; Johnson, T.; Walther, J.; Yu, M.; Wrigth, B.; et al. Integrated continuous production of recombinant therapeutic proteins. Biotechnol. Bioeng. 2012, 109, 3018–3029. [Google Scholar] [CrossRef] [PubMed]
- Godawat, R.; Konstantinov, K.; Rohani, M.; Warikoo, V. End-to-end integrated fully continuous production of recobinant monoclonal antibodies. J. Biotechnol. 2015, 213, 13–19. [Google Scholar] [CrossRef] [PubMed]
- Karst, D.J.; Steinebach, F.; Soos, M.; Morbidelli, M. Process performance and product quality in an integrated continuous antibody production process. Biotechnol. Bioeng. 2017, 114, 298–307. [Google Scholar] [CrossRef]
- André, S.; Cristau, L.S.; Gaillard, S.; Devos, O.; Calvosa, É.; Duponchel, L. In-line and real-time prediction of recombinant antibody titer by in situ Raman spectroscopy. Anal. Chim. Acta 2015, 892, 148–152. [Google Scholar] [CrossRef]
- Li, M.Y.; Ebel, B.; Paris, C.; Chauchard, F.; Guedon, E.; Marc, A. Real-time monitoring of antibody glycosylation site occupancy by in situ Raman spectroscopy during bioreactor CHO cell cultures. Biotechnol. Prog. 2018, 34, 486–493. [Google Scholar] [CrossRef]
- Shang, Y.; Zeng, Y.; Zeng, Y. Integrated Microfluidic Lectin Barcode Platform for High-Performance Focused Glycomic Profiling. Sci. Rep. 2016, 6, 20297. [Google Scholar] [CrossRef] [Green Version]
- Rüdt, M.; Brestrich, N.; Rolinger, L.; Hubbuch, J. Real-time monitoring and control of the load phase of a protein A capture step. Biotechnol. Bioeng. 2017, 114, 368–373. [Google Scholar] [CrossRef]
- Großhans, S.; Rüdt, M.; Sanden, A.; Brestrich, N.; Morgenstern, J.; Heissler, S.; Hubbuch, J. In-line Fourier-transform infrared spectroscopy as a versatile process analytical technology for preparative protein chromatography. J. Chromatogr. A 2018, 1547, 37–44. [Google Scholar] [CrossRef]
- Krättli, M.; Steinebach, F.; Morbidelli, M. Online control of the twin-column countercurrent solvent gradient process for biochromatography. J. Chromatogr A 2013, 1293, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Godawat, R.; Brower, K.; Jain, S.; Konstantinov, K.; Riske, F.; Warikoo, V. Periodic counter-current chromatography—design and operational considerations for integrated and continuous purification of proteins. Biotechnol. J. 2012, 7, 1496–1508. [Google Scholar] [CrossRef] [PubMed]
- Vormittag, P.; Gunn, R.; Ghorashian, S.; Veraitch, F.S. A guide to manufacturing CAR T cell therapies. Curr. Opin. Biotechnol. 2018, 53, 164–181. [Google Scholar] [CrossRef] [PubMed]
- Mock, U.; Nickolay, L.; Philip, B.; Cheung, G.W.K.; Zhan, H.; Johnston, I.C.D.; Kaiser, A.D.; Peggs, K.; Pule, M.; Thrasher, A.J.; et al. Automated manufacturing of chimeric antigen receptor T cells for adoptive immunotherapy using CliniMACS prodigy. Cytotherapy 2016, 18, 1002–1011. [Google Scholar] [CrossRef] [PubMed]
- Jaffer, G. Pharma’s Almanac. Keys to Successful Storage, Management and Transport of Biological Materials. Available online: https://www.pharmasalmanac.com/articles/keys-to-successful-storage-management-and-transport-of-biological-materials (accessed on 28 December 2020).
- Ruella, M.; Kenderian, S.S. Next-Generation Chimeric Antigen Receptor T-Cell Therapy: Going off the Shelf. BioDrugs 2017, 31, 473–481. [Google Scholar] [CrossRef] [PubMed]
- U.S. Food and Drug Administration. Summary Basis for Regulatory Action; U.S. Food and Drug Administration: Silver Spring, MD, USA, 2017; pp. 1–16. [Google Scholar]
- Novartis. Kymriah® (Tisagenlecleucel), First-in-Class CAR-T Therapy from Novartis, Receives Second FDA Approval to treat Appropriate r/r Patients with Large B-Cell Lymphoma. Available online: https://www.novartis.com/news/media-releases/kymriah-tisagenlecleucel-first-class-car-t-therapy-from-novartis-receives-second-fda-approval-treat-appropriate-rr-patients-large-b-cell-lymphoma#:~:text=Quantitative%20Sciences%20Hackathon-,Kymriah%C2%AE%20(tisagenlecleucel)%2C%20first%2Din%2Dclass%20CAR,with%20large%20B%2Dcell%20lymphoma (accessed on 5 January 2021).
- Novartis. Kymriah® (Tisagenlecleucel): Treatment Process, Dosing, Administration HCP. Available online: https://www.hcp.novartis.com/products/kymriah/acute-lymphoblastic-leukemia-children/treatment-process/ (accessed on 5 January 2021).
- Kite PharmA First CAR T Therapy for Certain Types of Relapsed or Refractory B-Cell Lymphoma. Available online: https://www.kitepharma.com/news/press-releases/2020/7/us-fda-approves-kites-tecartus-the-first-and-only-car-t-treatment-for-relapsed-or-refractory-mantle-cell-lymphoma (accessed on 20 November 2020).
- Lehmicke, M.; In Vivo. Manufacturing Cures: Infrastructure Challenges Facing Cell and Gene. Therapy Developers. Available online: https://invivo.pharmaintelligence.informa.com/IV124277/Manufacturing-Cures-Infrastructure-Challenges-Facing-Cell-And-Gene-Therapy-Developers (accessed on 15 December 2020).
- Ebel, T.; George, K.; Larsen, E.; Shah, K.; Ungerman, D. Pharmaceuticals and Medical Products Operations; Mckinsey Co.: New York, NY, USA, 2013. [Google Scholar]
- Shah, N. Pharmaceutical supply chains: Key issues and strategies for optimisation. Comput. Chem. Eng. 2004, 29, 929–941. [Google Scholar] [CrossRef]
- Marques, C.M.; Moniz, S.; de Sousa, J.P.; Barbosa-Póvoa, A.P.; Reklaitis, G. Decision-support challenges in the chemical-pharmaceutical industry: Findings and future research directions. Comput. Chem. Eng. 2020, 134, 106672. [Google Scholar] [CrossRef]
- Srai, J.S.; Badman, C.; Krumme, M.; Futran, M.; Johnston, C. Future supply chains enabled by continuous processing-opportunities and challenges May 20-21, 2014 Continuous Manufacturing Symposium. J. Pharm. Sci. 2015, 104, 840–849. [Google Scholar] [CrossRef] [Green Version]
- Sykes, C. Time- and temperature-controlled transport: Supply chain challenges and solutions. Pharm. Ther. 2018, 43, 154–170. [Google Scholar]
- U.S. Food and Drug Administration. Vaccines and Related Biological Products Advisory Committee. December 10. 2020 Meeting Briefing Document. Available online: https://www.fda.gov/advisory-committees/vaccines-and-related-biological-products-advisory-committee/2020-meeting-materials-vaccines-and-related-biological-products-advisory-committee (accessed on 28 December 2020).
- Castellanos, S.; The Wall Street Journal. Drugmaker to Test Machine Learning to Prevent Drug Shortages. Available online: https://www.wsj.com/articles/drugmaker-to-test-machine-learning-to-prevent-drug-shortages-11571079794#:~:text=Merck%20KGaA%20plans%20to%20use,before%20they%20can%20be%20used (accessed on 28 December 2020).
- Papathanasiou, M. Advances in Enabling Smart Technologies across the Cell Therapy Supply Chain. Cell Gene. Insights 2018, 4, 495–500. [Google Scholar] [CrossRef]
- Raza, S.; Blackburn, L.; Moortie, S.; Cook, S.; Johnson, E.; Gaynor, L.; Kroese, M. The Personalised Medicine Technology Landscape; PHG Found: Cambridge, UK, 2018; ISBN 978-1-907198-31-1. [Google Scholar]
- Chiaccio, F.; D’Urso, D.; Compagno, L.; Chiarenza, M.; Velardita, L. Towards a Blockchain Based Traceability Process: A Case Study from Pharma Industry. IFIP Adv. Inf. Commun. Technol. 2019, 566, 451–457. [Google Scholar] [CrossRef]
- Nakamoto, S. Bitcoin: A Peer-to-Peer Electronic Cash System. Available online: https://bitcoin.org/bitcoin.pdf (accessed on 3 February 2021).
- Agbo, C.C.; Mahmoud, Q.H.; Eklund, J.M. Blockchain Technology in Healthcare: A Systematic Review. Healtcare 2019, 7, 56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- CISION, PR Newswire. Everyware and Hedera Hashgraph Enabling Cold ChaMonitoring of COVID-19 Vaccine for NHS Fcilities. Available online: https://www.prnewswire.com/news-releases/everyware-and-hedera-hashgraph-enabling-cold-chain-monitoring-of-covid-19-vaccine-for-nhs-facilities-301209642.html (accessed on 3 February 2021).
- Modum. Success Stories. Available online: https://www.modum.io/industries/success-stories (accessed on 3 February 2021).
- Siganporia, C.C.; Ghosh, S.; Daszkowski, T.; Papageorgiou, L.G.; Farid, S.S. Capacity planning for batch and perfusion bioprocesses across multiple biopharmaceutical facilities. Biotechnol. Prog. 2014, 30, 594–606. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vieira, M.; Pinto-Varela, T.; Moniz, S.; Barbosa-Póvoa, A.P.; Papageorgiou, L.G. Optimal planning and campaign scheduling of biopharmaceutical processes using a continuous-time formulation. Comput. Chem. Eng. 2016, 91, 422–444. [Google Scholar] [CrossRef] [Green Version]
- Lakhdar, K.; Zhou, Y.; Savery, J.; Titchener-Hooker, N.J.; Papageorgiou, L.G. Medium term planning of biopharmaceutical manufacture using mathematical programming. Biotechnol. Prog. 2005, 21, 1478–1489. [Google Scholar] [CrossRef]
- Millipore SigmA Bioprocess Online. Flexible Manufacturing of Vaccines. Available online: https://www.bioprocessonline.com/doc/flexible-manufacturing-of-vaccines-0001 (accessed on 20 December 2020).
- Papageorgiou, L.G.; Rotstein, G.E.; Shah, N. Strategic supply chain optimization for the pharmaceutical industries. Ind. Eng. Chem. Res. 2001, 40, 275–286. [Google Scholar] [CrossRef]
- MacDonald, G.J.; Genetic Engineering & Biotechnology News. Single-Use Tech Key for Capacity Hike Required for COVID-19. Available online: https://www.genengnews.com/topics/bioprocessing/single-use-tech-key-for-capacity-hike-required-for-covid-19/ (accessed on 29 December 2020).
- Markarian, J. Supply Chain Challenges for Single-Use Systems. Biopharm. Int. 2019, 32, 16–19. [Google Scholar]
- Gernaey, K.V.; Cervera-Padrell, A.E.; Woodley, J.M. A perspective on process systems engineering in pharmaceutical process development and innovation. Comput. Chem. Eng. 2012, 42, 15–29. [Google Scholar] [CrossRef]
- Papadakis, E.; Woodley, J.M.; Gani, R. Perspective on PSE in pharmaceutical process development and innovation. Comput. Aided Chem. Eng. 2018, 41, 597–656. [Google Scholar] [CrossRef]
- Barbosa-Póvoa, A.P.; Pinto, J.M. Process supply chains: Perspectives from academia and industry. Comput. Chem. Eng. 2020, 132, 106606. [Google Scholar] [CrossRef]
- Chen, Y.; Yang, O.; Sampat, C.; Bhalode, P.; Ramachandran, R.; Ierapetritou, M. Digital Twins in Pharmaceutical and Biopharmaceutical Manufacturing: A Literature Review. Processes 2020, 8, 1088. [Google Scholar] [CrossRef]
- Grossmann, I.E. Advances in mathematical programming models for enterprise-wide optimization. Comput. Chem. Eng. 2012, 47, 2–18. [Google Scholar] [CrossRef] [Green Version]
- Lainez, J.M.; Schaefer, E.; Reklaitis, G.V. Challenges and opportunities in enterprise-wide optimisation in the pharmaceutical industry. Comput. Chem. Eng. 2012, 47, 19–28. [Google Scholar] [CrossRef]
- Kotidis, P.; Demis, P.; Goey, C.H.; Correa, E.; McIntosh, C.; Trepekli, S.; Shah, N.; Klymenko, O.V.; Kontoravdi, C. Constrained global sensitivity analysis for bioprocess design space identification. Comput. Chem. Eng. 2019, 125, 558–568. [Google Scholar] [CrossRef]
- Böhl, O.J.; Schellenberg, J.; Bahnemann, J.; Hitzmann, B.; Scheper, T.; Solle, D. Implementation of QbD strategies in the inoculum expansion of a mAb production process. Eng. Life Sci. 2020. [Google Scholar] [CrossRef]
- Bano, G.; Wang, Z.; Facco, P.; Bezzo, F.; Barolo, M.; Ierapetritou, M. A novel and systematic approach to identify the design space of pharmaceutical processes. Comput. Chem. Eng. 2018, 115, 309–322. [Google Scholar] [CrossRef]
- Xie, X.; Schenkendorf, R. Robust Process Design in Pharmaceutical Manufacturing under Batch-to-Batch Variation. Processes 2019, 7, 509. [Google Scholar] [CrossRef] [Green Version]
- Mortier, S.T.F.C.; Van Bockstal, P.J.; Corver, J.; Nopens, I.; Gernaey, K.V.; De Beer, T. Uncertainty analysis as essential step in the establishment of the dynamic Design Space of primary drying during freeze-drying. Eur. J. Pharm. Biopharm. 2016, 103, 71–83. [Google Scholar] [CrossRef]
- Ganesh, S.; Su, Q.; Vo, L.B.D.; Pepka, N.; Rentz, B.; Vann, L.; Yazdanpanah, N.; O’Connor, T.; Nagy, Z.K.; Reklaitis, G.V. Design of condition-based maintenance framework for process operations management in pharmaceutical continuous manufacturing. Int. J. Pharm. 2020, 587, 119621. [Google Scholar] [CrossRef] [PubMed]
- Diab, S.; McQuade, D.T.; Gupton, B.F.; Gerogiorgis, D.I. Process Design and Optimization for the Continuous Manufacturing of Nevirapine, an Active Pharmaceutical Ingredient for HIV Treatment. Org. Process Res. Dev. 2019, 23, 320–333. [Google Scholar] [CrossRef]
- Giridhar, A.; Reklaitis, G.V. Real-Time Optimization: How to Change Setpoints in Pharmaceutical Manufacturing. In AAPS Advances the Pharmaceutical Sciences Series; Nagy, Z.K., El Hagrasy, A., Litster, J., Eds.; Springer: Cham, Switzerland, 2020; Volume 42, pp. 429–440. ISBN 978-3-030-41524-2_12. [Google Scholar]
- Kotidis, P.; Jedrzejewski, P.; Sou, S.N.; Sellick, C.; Polizzi, K.; del Val, I.J.; Kontoravdi, C. Model-based optimization of antibody galactosylation in CHO cell culture. Biotechnol. Bioeng. 2019, 116, 1612–1626. [Google Scholar] [CrossRef] [PubMed]
- Papathanasiou, M.M.; Burnak, B.; Katz, J.; Shah, N.; Pistikopoulos, E.N. Assisting continuous biomanufacturing through advanced control in downstream purification. Comput. Chem. Eng. 2019, 125, 232–248. [Google Scholar] [CrossRef]
- Feidl, F.; Vogg, S.; Wolf, M.; Podobnik, M.; Ruggeri, C.; Ulmer, N.; Wachli, R.; Souquet, J.; Broly, H.; Butté, A.; et al. Process-wide control and automation of an integrated continuous manufacturing platform for antibodies. Biotechnol. Bioeng. 2020, 117, 1367–1380. [Google Scholar] [CrossRef]
- Su, Q.; Moreno, M.; Ganesh, S.; Reklaitis, G.V.; Nagy, Z.K. Resilience and risk analysis of fault-tolerant process control design in continuous pharmaceutical manufacturing. J. Loss. Prev. Process. Ind. 2018, 55, 411–422. [Google Scholar] [CrossRef]
- De Carvalho, M.I.; Ribeiro, D.; Barbosa-Póvoa, A.P. Design and Planning of Sustainable Vaccine Supply Chain. In Pharmaceutical Supply Chains Medicine Shortages; Barbosa-Póvoa, A.P., Jenzer, H., De Miranda, J.L., Eds.; Springer: Cham, Switzerland, 2019; pp. 23–55. ISBN 978-3-030-15398-4. [Google Scholar]
- Liu, S.; Papageorgiou, L.G. Multi-objective optimisation for production, distribution and capacity planning of global supply chains in the process industry. Omega 2014, 41, 369–382. [Google Scholar] [CrossRef]
- Gatica, G.; Papageorgiou, L.G.; Shah, N. Capacity Planning Under Uncertainty for the Pharmaceutical Industry. Trans. Icheme 2003, 81, 665–678. [Google Scholar] [CrossRef] [Green Version]
- Tsang, K.H.; Samsatli, N.J.; Shah, N. Capacity Investment Planning for Multiple Vaccines Under Uncertainty 1: Capacity Planning. Inst. Chem. Eng. 2007, 85, 120–128. [Google Scholar] [CrossRef]
- Liu, S.; Papageorgiou, L.G.; Shah, N. Optimal design of low-cost supply chain networks on the benefits of new product formulations. Comput. Ind. Eng. 2020, 139, 1061893. [Google Scholar] [CrossRef]
- Sousa, R.T.; Liu, S.; Papageorgiou, L.G.; Shah, N. Global supply chain planning for pharmaceuticals. Chem. Eng. Res. Des. 2011, 89, 2396–2409. [Google Scholar] [CrossRef]
- Stefansson, H.; Jensson, P.; Shah, N. Multiscale Planning and Scheduling in the Secondary Pharmaceutical Industry. Am. Inst. Chem. Eng. 2006, 52, 4133–4149. [Google Scholar] [CrossRef]
- Amaro, A.C.S.; Barbosa-Póvoa, A.P. Planning and scheduling of industrial supply chains with reverse flows: A real pharmaceutical case study. Comput. Chem. Eng. 2008, 32, 2606–2625. [Google Scholar] [CrossRef]
- Rossi, F.; Casas-Orozco, D.; Reklaitis, G.; Manenti, F.; Buzzi-Ferraris, G. A computational framework for integrating campaign scheduling, dynamic optimization and optimal control in multi-unit batch processes. Comput. Chem. Eng. 2017, 107, 184–220. [Google Scholar] [CrossRef]
- Dias, L.S.; Ierapetritou, M.G. From process control to supply chain management: An overview of integrated decision making strategies. Comput. Chem. Eng. 2017, 106, 826–835. [Google Scholar] [CrossRef]
- Jankauskas, K.; Papageorgiou, L.G.; Farid, S.S. Fast genetic algorithm approaches to solving discrete-time mixed integer linear programming problems of capacity planning and scheduling of biopharmaceutical manufacture. Comput. Chem. Eng. 2019, 121, 212–223. [Google Scholar] [CrossRef]
- Franco, C.; Alfonso-Lizarazo, E. Optimization under uncertainty of the pharmaceutical supply chain in hospitals. Comput. Chem. Eng. 2020, 135, 106689. [Google Scholar] [CrossRef]
- Levis, A.A.; Papageorgiou, L.G. A Hierarchial Solution Approach for Multi-Site Capacity Planning Under Uncertainty in the Pharmaceutical Industry. Comput. Chem. Eng. 2004, 28, 707–725. [Google Scholar] [CrossRef]
- Wang, X.; Kong, Q.; Papathanasiou, M.M.; Shah, N. Precision healthcare supply chain design through multi-objective stochastic programming. Comput. Aided Chem. Eng. 2018, 44, 2137–2142. [Google Scholar] [CrossRef]
- Moschou, D.; Papathanasiou, M.M.; Lakelin, M.; Shah, N. Investment Planning in Personalised Medicine. Comput. Aided Chem. Eng. 2020, 48, 49–54. [Google Scholar] [CrossRef]
Figure 1.
Schematic of simplified pharmaceutical product categories.

Figure 2.
Pharmaceutical supply chain for (a) batch-produced drugs and (b) patient-specific therapeutics.
Figure 2.
Pharmaceutical supply chain for (a) batch-produced drugs and (b) patient-specific therapeutics.

Figure 3.
Pharmaceutical manufacturing and supply chain ecosystem.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Summary of the key challenges and opportunities in pharmaceutical manufacturing and distribution. The tick sign highlights the relevance of the identified issues and solutions to each drug product category.
Table 1.
Summary of the key challenges and opportunities in pharmaceutical manufacturing and distribution. The tick sign highlights the relevance of the identified issues and solutions to each drug product category.
| Decisions | Challenges and Issues | Small Molecules | Conventional Biologics | Personalised Products | Solutions and Opportunities |
|---|---|---|---|---|---|
| Manufacturing | |||||
| Product Portfolio | Identification of product profile | ✔ | ✔ | Understand QTTP; Outsource manufacturing and development to contractors | |
| Process Design and Operations | Long approval times | ✔ | ✔ | ✔ | Standardisation; Single-use technology; Multiproduct facilities |
| Batch solutions are well-established | ✔ | ✔ | Incentivise investment in continuous manufacturing | ||
| Batch-to-batch variability and shortages | ✔ | Continuous manufacturing; QbD | |||
| Identification of optimal operating units and modes | ✔ | ✔ | ✔ | Process optimisation tools; QbD | |
| Measurements availability and lack of process understanding | ✔ | ✔ | Develop online PAT tools; Digital twins of process; QbD | ||
| Capacity Planning | Long lead times for scale up | ✔ | ✔ | Scale up existing suites; Scale out through new suites instalment; Single use equipment | |
| Patient-specific products and process | ✔ | Scale out and set up of parallel suites | |||
| Uncertainty of long-term demand | ✔ | ✔ | ✔ | Decision-making tools for long-term investment strategies; Multiproduct facilities; Outsource production to CMOs and CDMOs | |
| Production Planning and Scheduling | Adaptability to short-term demand fluctuations | ✔ | ✔ | ✔ | Real time demand forecasts; Continuous manufacturing for flexible campaigns; Single use equipment to reduce changeover times Planning and scheduling decision-making tools |
| Time constraint and patient specificity | ✔ | COI and COC; Monitor patient schedule; Planning and scheduling decision-making tools | |||
| Quality Control | Quality assurance tasks lead times | ✔ | ✔ | ✔ | Continuous manufacturing; QbD |
| Unavailability of measurements | ✔ | ✔ | ✔ | Digital twins for real-time monitoring | |
| Distribution | |||||
| Inventory Planning | Prevention of shortages | ✔ | ✔ | Real-time sharing of stock data, inventory levels and forecasted demand | |
| Monitor CQAs and CPPs | ✔ | ✔ | Track & Trace tools; Outsource distribution to contract logistics providers | ||
| Time constraint and patient specificity | ✔ | COI and COC; Track & Trace tools | |||
| Network Structure | Compliance and coordination of stakeholders. | ✔ | ✔ | ✔ | Track & Trace tools; Data sharing |
| Time constraint and patient specificity | ✔ | Decentralised supply chain closer to the patient | |||
| Transport Modes and Connections | Monitor CQAs and CPPs | ✔ | ✔ | Track & Trace tools; Outsource distribution to contract logistics providers | |
| Counterfeit drugs entering supply chain | ✔ | ✔ | Track & Trace tools | ||
| Time constraint and patient specificity | ✔ | ✔ | Track & Trace tools; Outsource distribution to contract logistics providers | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Sarkis, M.; Bernardi, A.; Shah, N.; Papathanasiou, M.M. Emerging Challenges and Opportunities in Pharmaceutical Manufacturing and Distribution. Processes 2021, 9, 457. https://0-doi-org.brum.beds.ac.uk/10.3390/pr9030457
AMA Style
Sarkis M, Bernardi A, Shah N, Papathanasiou MM. Emerging Challenges and Opportunities in Pharmaceutical Manufacturing and Distribution. Processes. 2021; 9(3):457. https://0-doi-org.brum.beds.ac.uk/10.3390/pr9030457
Chicago/Turabian StyleSarkis, Miriam, Andrea Bernardi, Nilay Shah, and Maria M. Papathanasiou. 2021. "Emerging Challenges and Opportunities in Pharmaceutical Manufacturing and Distribution" Processes 9, no. 3: 457. https://0-doi-org.brum.beds.ac.uk/10.3390/pr9030457
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.