
Advanced Cutaneous Leiomyosarcoma of the Forearm

 ,
,  , ,
, , 
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
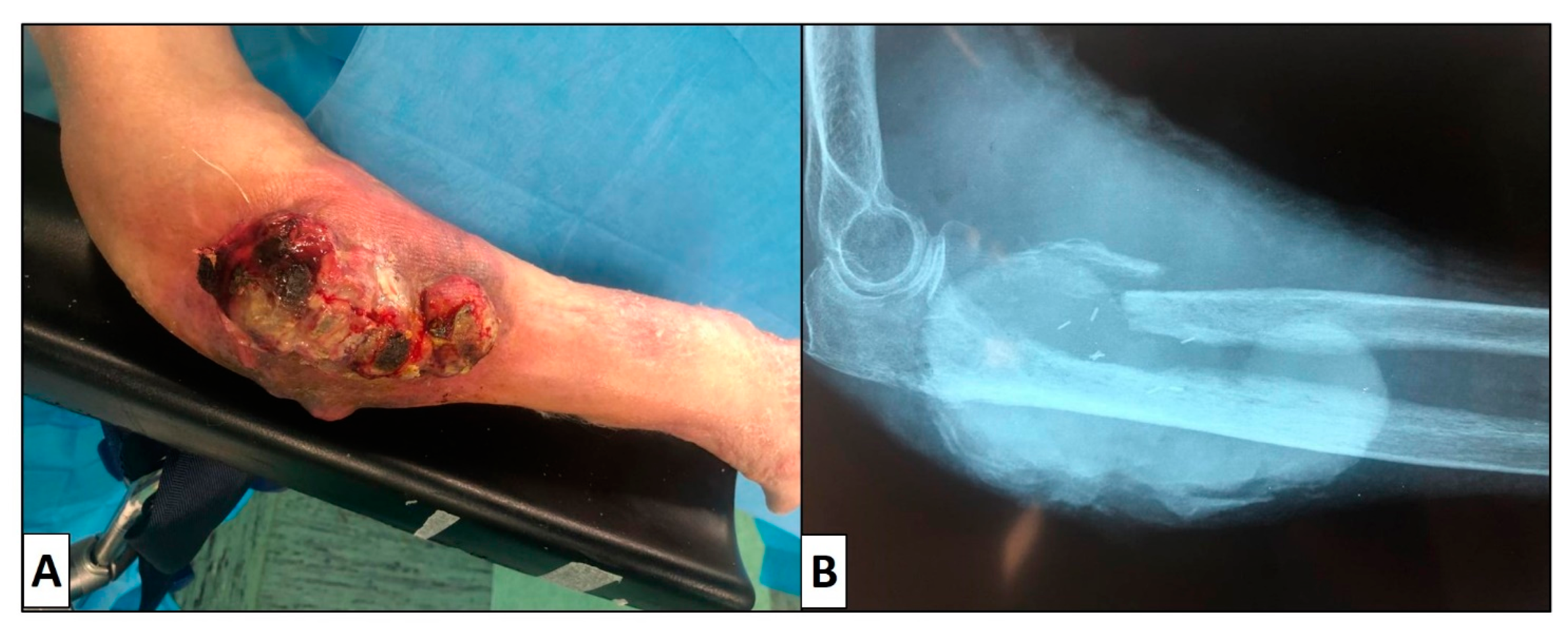
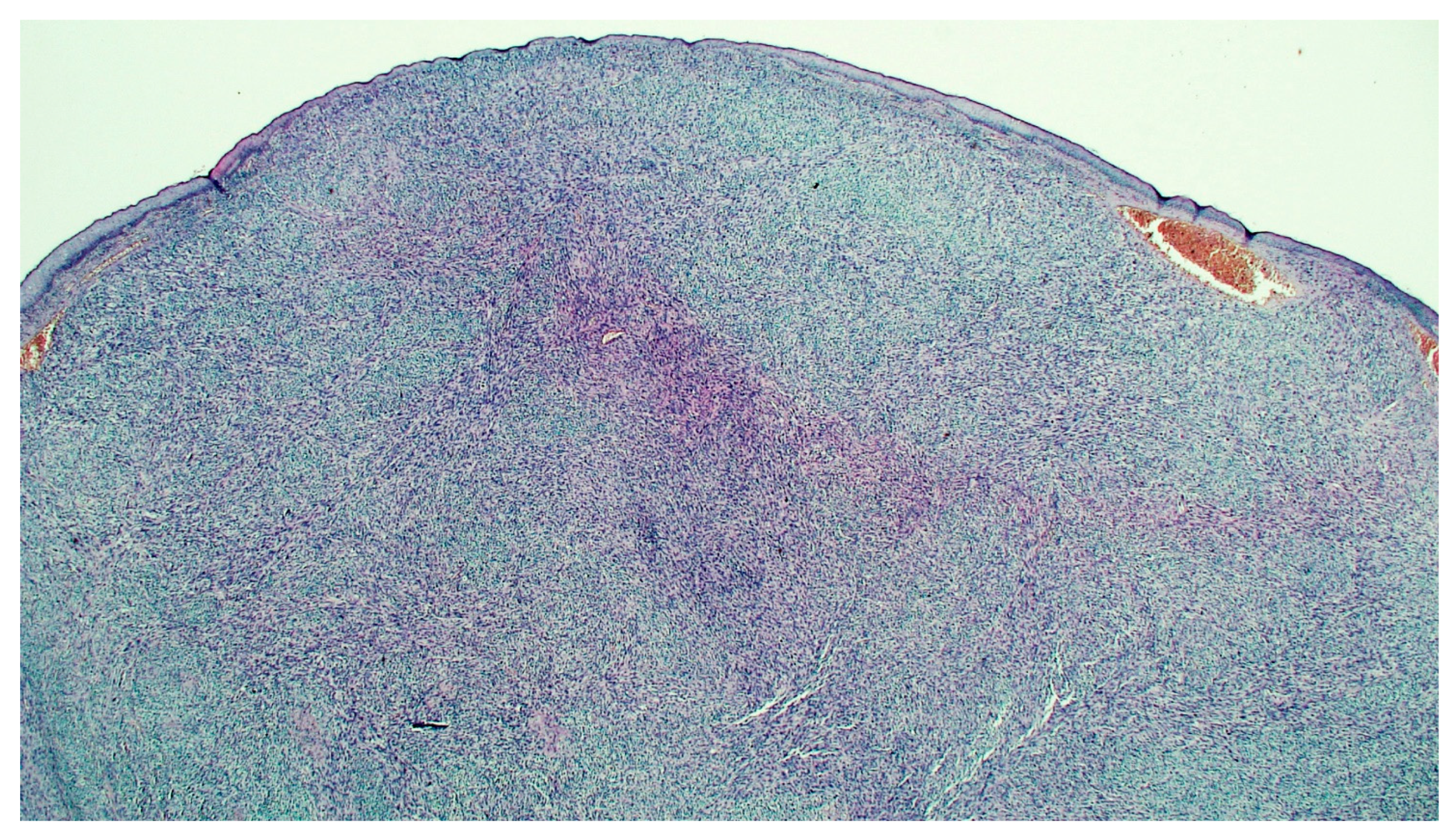
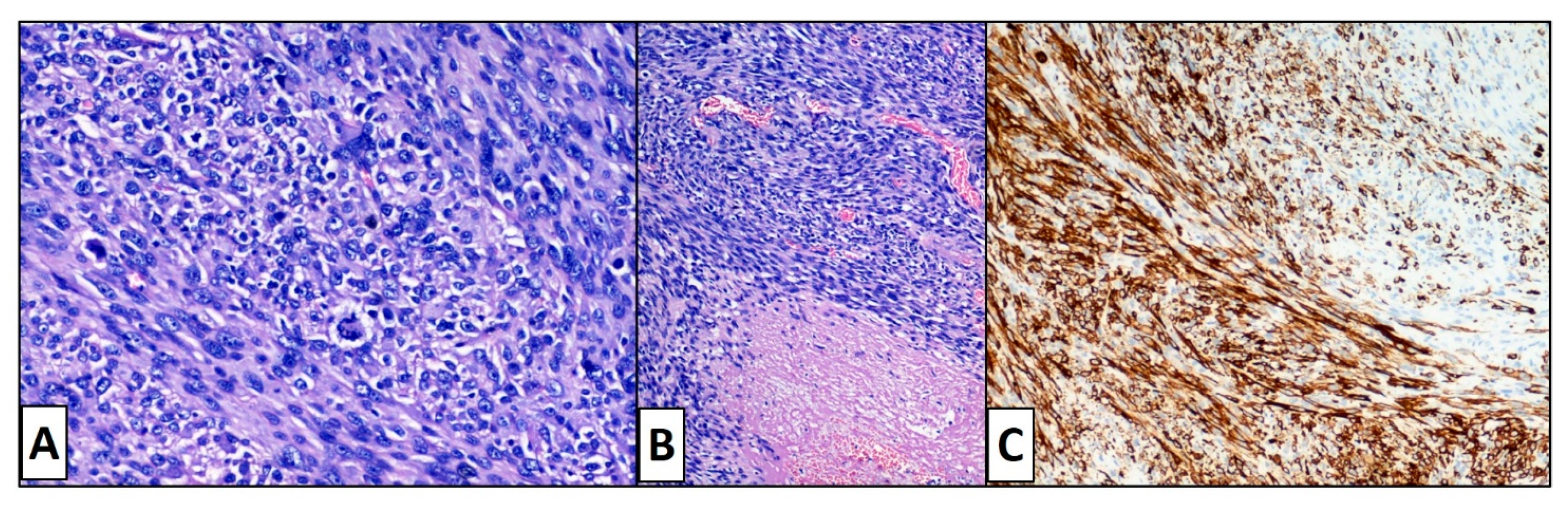
2. Case Report
3. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Hmida, L.; Letaief, F.; Doghri, R.; Meddeb, K.; Mahjoubi, K.; Mokrani, A.; Yahiaoui, Y.; Gabsi, A.; Cheraiet, N.; Rais, H.; et al. Cutaneous leiomyosarcoma on the trunk: An unusual presentation with an aggressive course—Case report and review of literature. PAN Afr. Med. J. 2018, 31, 190. [Google Scholar] [CrossRef] [PubMed]
- Winchester, D.S.; Hocker, T.L.; Brewer, J.D.; Baum, C.L.; Hochwalt, P.C.; Arpey, C.J.; Otley, C.C.; Roenigk, R.K. Leiomyosarcoma of the skin: Clinical, histopathologic, and prognostic factors that influence outcomes. J. Am. Acad. Dermatol. 2014, 71, 919–925. [Google Scholar] [CrossRef] [PubMed]
- Zacher, M.; Heppt, M.V.; Brinker, T.J.; Hayani, K.M.; Flaig, M.J.; Berking, C. Primary leiomyosarcoma of the skin: A comprehensive review on diagnosis and treatment. Med. Oncol. 2018, 35, 135. [Google Scholar] [CrossRef] [PubMed]
- Vestita, M.; Filoni, A.; Ingravallo, G.; Sportelli, P.; Bonamonte, D. Recurrent cutaneous leiomyosarcoma of the inner thigh. Indian J. Dermatol. Venereol. Leprol. 2015, 81, 309–311. [Google Scholar] [CrossRef] [PubMed]
- Kazlouskaya, V.; Lai, Y.C.; Khachemoune, A. Leiomyosarcoma of the skin: Review of the literature with an emphasis on prognosis and management. Int. J. Dermatol. 2020, 59, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Massi, D.; Franchi, A.; Alos, L.; Cook, M.; Di Palma, S.; Enguita, A.B.; Ferrara, G.; Kazakov, D.V.; Mentzel, T.; Michal, M.; et al. Primary cutaneous leiomyosarcoma: Clinicopathological analysis of 36 cases. Histopathology 2010, 56, 251–262. [Google Scholar] [CrossRef] [PubMed]
- Touati, N.; Schöffski, P.; Litière, S.; Judson, I.; Sleijfer, S.; Van Der Graaf, W.; Italiano, A.; Isambert, N.; Gil, T.; Blay, J.; et al. European Organisation for Research and Treatment of Cancer Soft Tissue and Bone Sarcoma Group Experience with Advanced/Metastatic Epithelioid Sarcoma Patients Treated in Prospective Trials: Clinical Profile and Response to Systemic Therapy. Clin. Oncol. 2018, 30, 448–454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Garcia-Carbonero, R.; Supko, J.; Manola, J.; Seiden, M.; Harmon, D.; Ryan, D.; Quigley, M.; Merriam, P.; Canniff, J.; Goss, G.; et al. Phase II and Pharmacokinetic Study of Ecteinascidin 743 in Patients With Progressive Sarcomas of Soft Tissues Refractory to Chemotherapy. J. Clin. Oncol. 2004, 22, 1480–1490. [Google Scholar] [CrossRef] [PubMed]
- Van Der Graaf, W.T.A.; Blay, J.-Y.; Chawla, S.P.; Kim, D.-W.; Bui-Nguyen, B.; Casali, P.G.; Schöffski, P.; Aglietta, M.; Staddon, A.P.; Beppu, Y.; et al. Pazopanib for metastatic soft-tissue sarcoma (PALETTE): A randomised, double-blind, placebo-controlled phase 3 trial. Lancet 2012, 379, 1879–1886. [Google Scholar] [CrossRef]
- D’Angelo, S.P.; Mahoney, M.R.; Van Tine, B.A.; Atkins, J.; Milhem, M.M.; Jahagirdar, B.N.; Antonescu, C.R.; Horvath, E.; Tap, W.D.; Schwartz, G.K.; et al. Nivolumab with or without ipilimumab treatment for metastatic sarcoma (Alliance A091401): Two open-label, non-comparative, randomised, phase 2 trials. Lancet Oncol. 2018, 19, 416–426. [Google Scholar] [CrossRef]



Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cazzato, G.; Sergi, M.C.; Sablone, S.; Colagrande, A.; Lettini, T.; Fanelli, F.; Orsini, U.; Ingravallo, G. Advanced Cutaneous Leiomyosarcoma of the Forearm. Dermatopathology 2021, 8, 40-44. https://0-doi-org.brum.beds.ac.uk/10.3390/dermatopathology8010008
Cazzato G, Sergi MC, Sablone S, Colagrande A, Lettini T, Fanelli F, Orsini U, Ingravallo G. Advanced Cutaneous Leiomyosarcoma of the Forearm. Dermatopathology. 2021; 8(1):40-44. https://0-doi-org.brum.beds.ac.uk/10.3390/dermatopathology8010008
Chicago/Turabian StyleCazzato, Gerardo, Maria Chiara Sergi, Sara Sablone, Anna Colagrande, Teresa Lettini, Francesco Fanelli, Umberto Orsini, and Giuseppe Ingravallo. 2021. "Advanced Cutaneous Leiomyosarcoma of the Forearm" Dermatopathology 8, no. 1: 40-44. https://0-doi-org.brum.beds.ac.uk/10.3390/dermatopathology8010008