
Immunohistopathological Analysis of Immunoglobulin E-Positive Epidermal Dendritic Cells with House Dust Mite Antigens in Naturally Occurring Skin Lesions of Adult and Elderly Patients with Atopic Dermatitis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Subjects and Skin Samples
2.2. Histological, Immunohistochemical, and Double-Immunofluorescence Staining
2.3. Evaluation of Immunohistopathological Findings
3. Results
3.1. Clinical and Laboratory Data of the Patients with AD and the Control Subjects
3.2. Double-Immunofluorescence and Immunohistochemical Studies
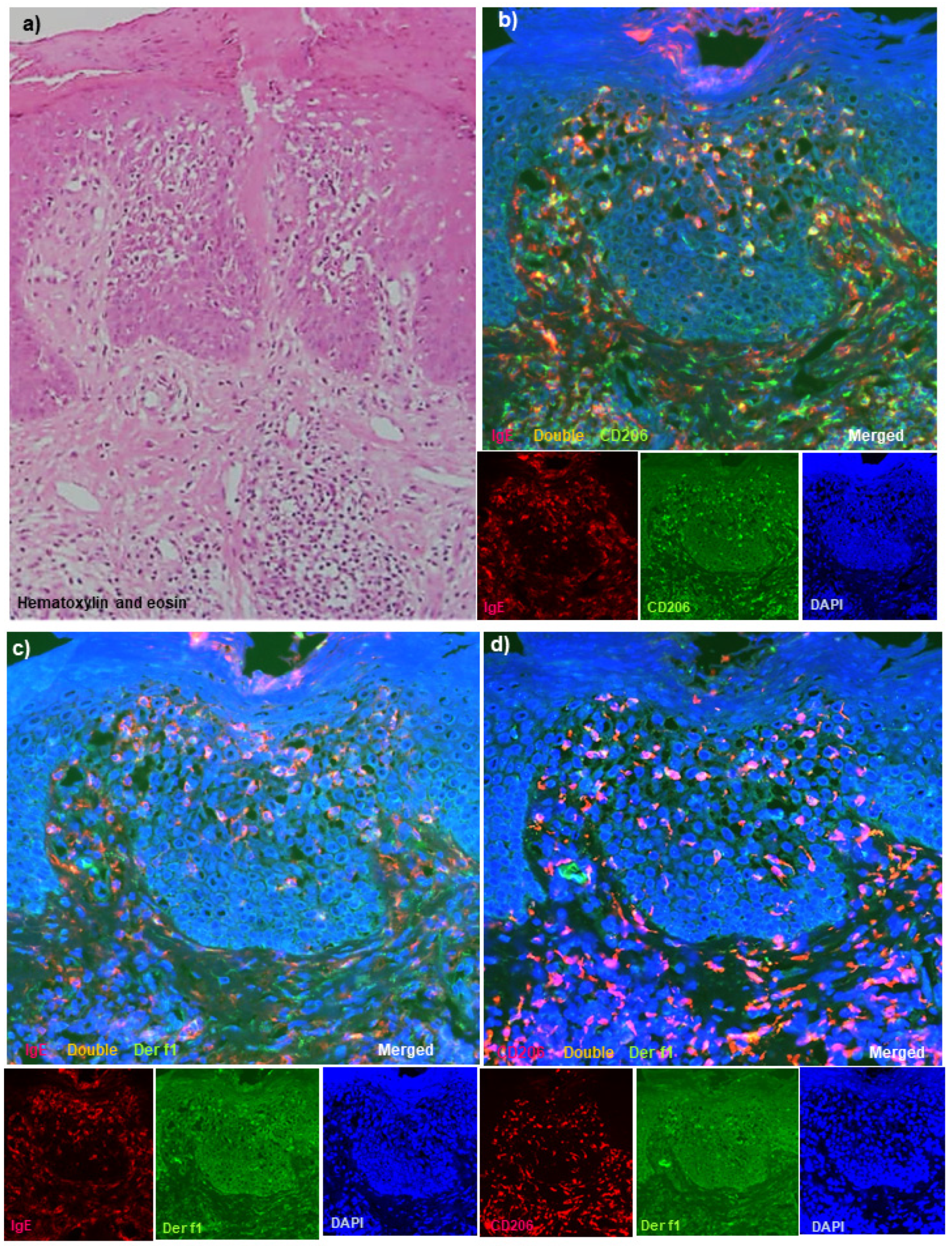
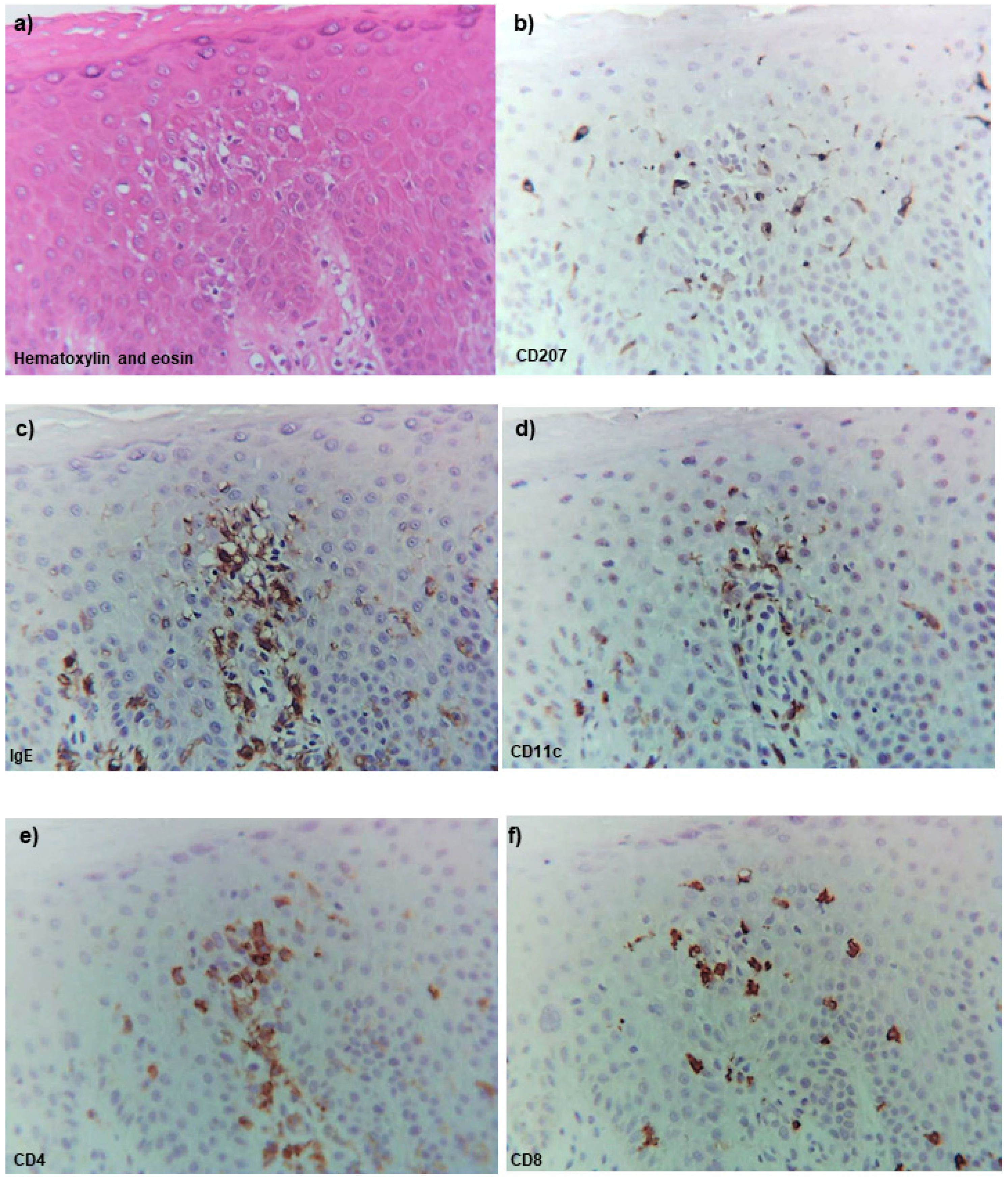
3.3. Hematoxylin-Eosin Staining
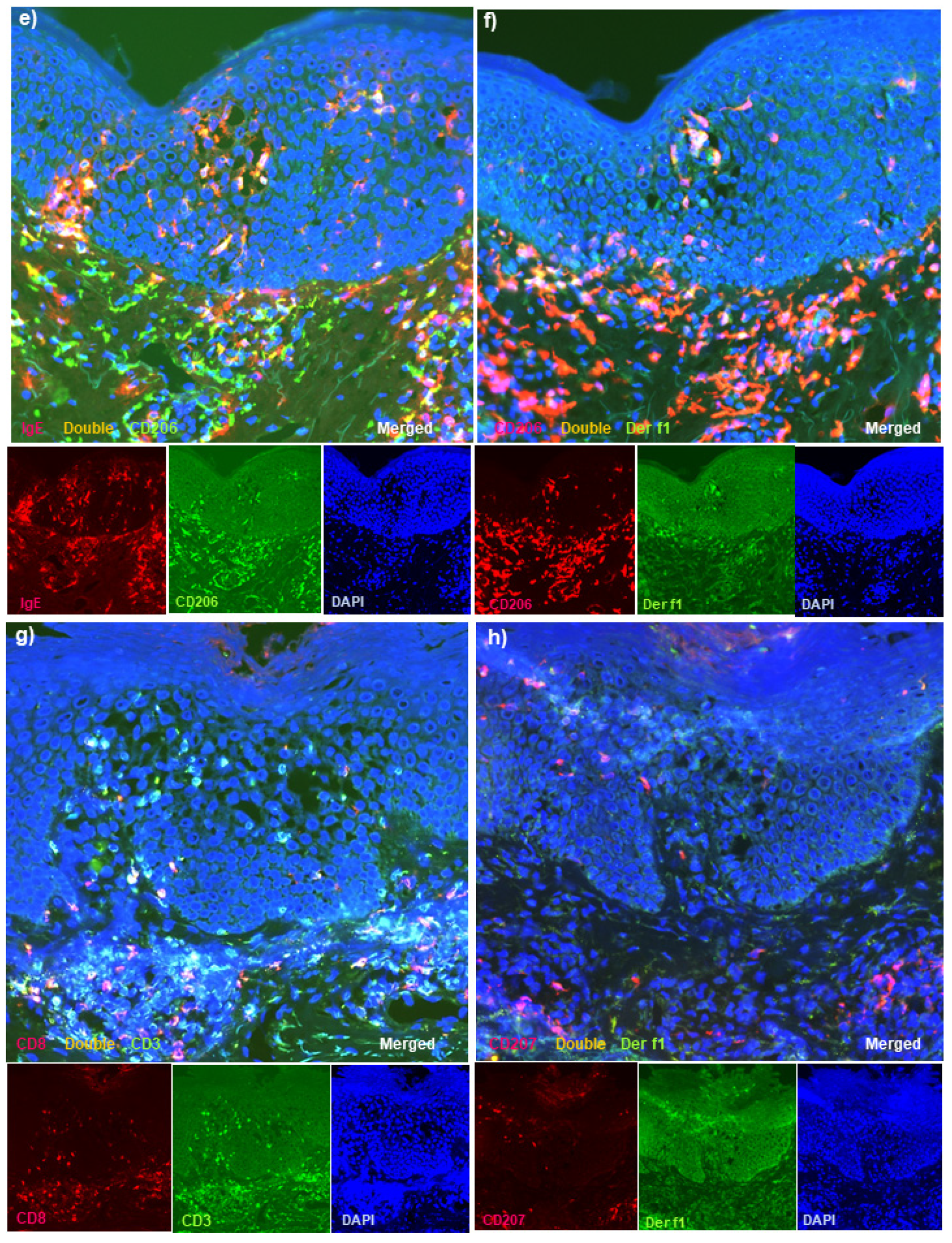
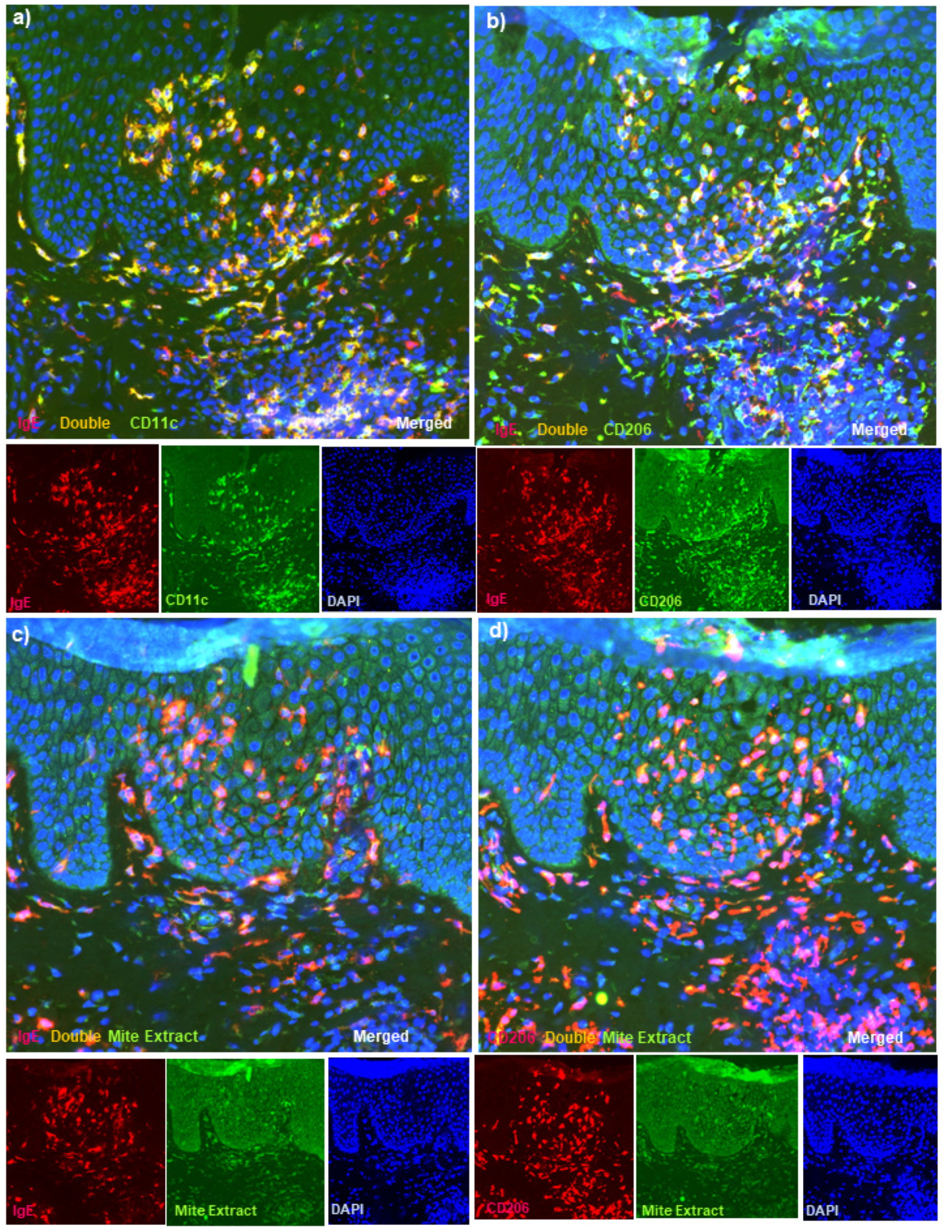
3.4. Double-Immunofluorescence Staining
3.5. Single-Immunohistochemical Staining
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bieber, T. Atopic dermatitis. N. Engl. J. Med. 2008, 358, 1483–1494. [Google Scholar] [CrossRef] [PubMed]
- Leung, D.Y.M.; Guttman-Yassky, E. Deciphering the complexities of atopic dermatitis: Shifting paradigms in treatment approaches. J. Allergy Clin. Immunol. 2014, 134, 769–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Werfel, T.; Allam, J.P.; Biedermann, T.; Eyerich, K.; Gilles, S.; Guttman-Yassky, E.; Hoetzenecker, W.; Knol, E.; Simon, H.-U.; Wollenberg, A.; et al. Cellular and molecular immunologic mechanisms in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2016, 138, 336–349. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wollenberg, A. Inflammatory dendritic epidermal cells. In Handbook of Atopic Eczema, 2nd ed.; Ring, J., Przybilla, B., Ruzicka, T., Eds.; Springer: Berlin, Germany, 2006; pp. 288–295. [Google Scholar]
- Guttman-Yassky, E.; Lowes, M.A.; Fuentes-Duculan, J.; Whynot, J.; Novitskaya, I.; Cardinale, I.; Haider, A.; Khatcherian, A.; Carucci, J.; Bergman, R.; et al. Major differences in inflammatory dendritic cells and their products distinguish atopic dermatitis from psoriasis. J. Allergy Clin. Immunol. 2007, 119, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Stary, G.; Bangert, C.; Stingl, G.; Kopp, T. Dendritic cells in atopic dermatitis: Expression of FcєRI on two distinct inflammation-associated subsets. Int. Arch. Allergy Immunol. 2005, 138, 278–290. [Google Scholar] [CrossRef]
- Wollenberg, A.; Wagner, M.; Günther, S.; Towarowski, A.; Tuma, E.; Moderer, M.; Rothenfusser, S.; Wetzel, S.; Endres, S.; Hartmann, G. Plasmacytoid dendritic cells: A new cutaneous dendritic cell subset with distinct role in inflammatory skin diseases. J. Investig. Dermatol. 2002, 119, 1096–1102. [Google Scholar] [CrossRef] [Green Version]
- Bieber, T. FcεRI-expressing antigen-presenting cells: New players in atopic game. Immunol. Today 1997, 18, 311–313. [Google Scholar] [CrossRef]
- Katayama, I.; Tanei, R.; Yokozeki, H.; Nishioka, K.; Dohi, Y. Induction of Eczematous Skin Reaction in Experimentally Induced Hyperplastic Skin of Balb/C Mice by Monoclonal Anti-DNP IgE Antibody: Possible Implications for Skin Lesion Formation in Atopic Dermatitis. Int. Arch. Allergy Immunol. 1990, 93, 148–154. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Haruna, T.; Yasui, K.; Takahashi, H.; Iduhara, M.; Takaki, S.; Deguchi, M.; Arimura, A. A Novel Atopic Dermatitis Model Induced by Topical Application with Dermatophagoides Farinae Extract in NC/Nga Mice. Allergol. Int. 2007, 56, 139–148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hanifin, J.M.; Rajka, G. Diagnostic features of atopic dermatitis. Acta Derm. (Stockh.) 1980, 92, 44–47. [Google Scholar]
- Hanifin, J.M.; Thurston, M.; Omoto, M.; Cherill, R.; Tofte, S.J.; Graeberet, M. The eczema area and severity index (EASI): Assessment of reliability in atopic dermatitis. Exp. Dermatol. 2001, 10, 11–18. [Google Scholar] [CrossRef]
- Tanei, R.; Hasegawa, Y. Double-positive immunoglobulin E+ and Dermatophagoides farinae antigen + dendritic cells are observed in skin lesions of older adults with atopic dermatitis: An immunohistological study. Dermatol. Clin. Res. 2017, 3, 134–150. [Google Scholar]
- Tanei, R.; Hasegawa, Y.; Sawabe, M. Abundant immunoglobulin E-positive cells in skin lesions support an allergic etiology of atopic dermatitis in the elderly. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 952–960. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arlian, L.G.; Platts-Mills, T.A.E. The biology of dust mites and the remediation of mite allergens in allergic disease. J. Allergy Clin. Immunol. 2001, 107, S406–S413. [Google Scholar] [CrossRef] [PubMed]
- Kanda, Y. Investigation of the freely available easy-to-use software “EZR” for medical statistics. Bone Marrow Transpl. 2013, 48, 452–458. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scalabrin, D.M.F.; Bavbek, S.; Perzanowski, M.S.; Wilson, B.B.; Platts-Mills, T.A.; Wheatley, L.M. Use of specific IgE in assessing the relevance of fungal and dust mite allergens to atopic dermatitis: A comparison with asthmatic and nonasthmatic control subjects. J. Allergy Clin. Immunol. 1999, 104, 1273–1279. [Google Scholar] [CrossRef]
- Tanei, R. Clinical Characteristics, Treatments, and Prognosis of Atopic Eczema in the Elderly. J. Clin. Med. 2015, 4, 979–997. [Google Scholar] [CrossRef]
- Teplitsky, V.; Mumcuoglu, K.Y.; Babai, I.; Dalal, I.; Cohen, R.; Tanay, A. House dust mites on skin, clothes, and bedding of atopic dermatitis patients. Int. J. Dermatol. 2008, 47, 790–795. [Google Scholar] [CrossRef]
- Yasueda, H.; Saito, A.; Nishioka, K.; Kutsuwada, K.; Akiyama, K. Measurement of Dermatophagoides mite allergens on bedding and human skin surfaces. Clin. Exp. Allergy 2003, 33, 1654–1658. [Google Scholar] [CrossRef]
- Darsow, U.; Ring, J. Immunoglobulin e-mediated allergy plays a role in atopic eczema as shown in the atopy patch test. World Allergy Organ. J. 2008, 1, 51–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Landheer, J.; Giovannone, B.; Mattson, J.D.; Tjabringa, S.; Bruijnzeel-Koomen, C.A.F.M.; McClanahan, T.; de Waal Malefyt, R.; Knol, E.; Hijnen, D. Epicutaneous application of house dust mite induces thymic stromal lymphopoietin in nonlesional skin of patients with atopic dermatitis. J. Allergy Clin. Immunol. 2013, 132, 1252–1254. [Google Scholar] [CrossRef]
- Maeda, K.; Yamamoto, K.; Tanaka, Y.; Anan, S.; Yoshida, H. House dust mite (HDM) antigen in naturally occurring lesions of atopic dermatitis (AD): The relationship between HDM antigen in the skin and HDM antigen-specific IgE antibody. J. Dermatol. Sci. 1992, 3, 73–77. [Google Scholar] [CrossRef]
- Yoshida, K.; Kubo, A.; Fujita, H.; Yokouchi, M.; Ishii, K.; Kawasaki, H.; Nomura, T.; Shimizu, H.; Kouyama, K.; Ebihara, T.; et al. Distinct behavior of human Langerhans cells and inflammatory dendritic epidermal cells at tight junctions in patients with atopic dermatitis. J. Allergy Clin. Immunol. 2014, 134, 856–864. [Google Scholar] [CrossRef]
- Nograles, K.E.; Zaba, L.C.; Shemer, A.; Fuentes-Duculan, J.; Cardinale, I.; Kikuchi, T.; Ramon, M.; Bergman, R.; Krueger, J.G.; Guttman-Yassky, E. IL-22-producing "T22" T cells account for upregulated IL-22 in atopic dermatitis despite reduced IL-17-producing TH17 T cells. J. Allergy Clin. Immunol. 2009, 123, 1244–1252. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Novak, N.; Valenta, R.; Bohle, B.; Laffer, S.; Haberstok, J.; Kraft, S.; Bieber, T. Fc epsilon RI engagement of Langerhans cell-like dendritic cells and inflammatory dendritic epidermal cell-like dendritic cells induces chemotactic signals and different T-cell phenotypes in vitro. J. Allergy Clin. Immunol. 2004, 113, 949–957. [Google Scholar] [CrossRef] [PubMed]
- Sager, N.; Feldmann, A.; Schilling, G.; Kreitsch, P.; Neumann, C. House dust mite-specific T cells in the skin of subjects with atopic dermatitis: Frequency and lymphokine profile in the allergen patch test. J. Allergy Clin. Immunol. 1992, 89, 801–810. [Google Scholar] [CrossRef]
- Trautmann, A.; Akdis, M.; Kleemann, D.; Altznauer, F.; Simon, H.U.; Graeve, T.; Noll, M.; Bröcker, E.-B.; Blaser, K.; Akdis, C.A. T cell-mediated Fas-induced keratinocyte apoptosis plays a key pathogenetic role in eczematous dermatitis. J. Clin. Investig. 2000, 106, 25–35. [Google Scholar] [CrossRef] [Green Version]
- Yawalkar, N.; Schmid, S.; Braathen, L.R.; Pichler, W.J. Perforin and granzyme B may contribute to skin inflammation in atopic dermatitis and psoriasis. Br. J. Dermatol. 2001, 144, 1133–1139. [Google Scholar] [CrossRef]
- Frings, V.G.; Böer-Auer, A.; Breuer, K. Histomorphology and Immunophenotype of Eczematous Skin Lesions Revisited—Skin Biopsies Are Not Reliable in Differentiating Allergic Contact Dermatitis, Irritant Contact Dermatitis, and Atopic Dermatitis. Am. J. Dermatopathol. 2018, 40, 7–16. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case | Age/Sex | Disease | Onset [Approximate Age] | Biopsy Site | Topical Steroid Treatment † | Serum Total IgE (IU/mL) | Allergen-Specific IgEs against HDMs ‡ | EASI |
|---|---|---|---|---|---|---|---|---|
| 1 | 78/M | AD | Late adulthood | Forearm | Strong | 28,715 | High titer against | 42.1 |
| [47 y.o.] | 2 months | Der f and Der p | ||||||
| 2 | 61/F | AD | Adolescence | Forearm | Not used | 10,198 | High titer against | 29.4 |
| [15 y.o.] | Der f and Der p | |||||||
| 3 | 83/F | AD | Childhood | Thigh | Mild | 11,571 | High titer against | 33.5 |
| [Elementary school age] | 4 months | Der f § | ||||||
| 4 | 49/M | AD | Early childhood | Abdomen | Not used | 124,515 | High titer against | 54.5 |
| [2 to 3 y.o.] | Der f and Der p | |||||||
| 5 | 84/M | AD | Late adulthood | Upper back | Not used | 19,757 | High titer against | 15.5 |
| [50 y.o.] | Der f and Der p | |||||||
| 6 | 40/M | AD | Early childhood | Chest | Very strong | 8181 | High titer against | 33.8 |
| [6 y.o.] | 2 months | Der f and Der p | ||||||
| 7 | 78/M | EGPA | Elderly | Lower leg | Not used | 3007 | Doubtful reaction | NA |
| against Der f § | ||||||||
| 8 | 83/M | DH | Elderly | Back | Very strong | 3101 | Negative § | NA |
| 0.5 month | ||||||||
| 9 | 75/M | BP | Elderly | Buttock | Very strong | 6235 | Negative § | NA |
| 2 months | ||||||||
| 10 | 84/M | BP | Elderly | Abdomen | Weak | 14,195 | Negative § | NA |
| 0.5 month | ||||||||
| 11 | 80/M | BP | Elderly | Abdomen | Strongest | 128,839 | Moderate titer | NA |
| 1 month | against Der f § | |||||||
| 12 | 85/M | MPE | Elderly | Abdomen | Very strong | 12,516 | Negative § | NA |
| 3 months | ||||||||
| 13 | 73/M | NE | Elderly | Lower leg | Strong | 25 | Negative § | 9.6 |
| 2 months | ||||||||
| 14 | 59/M | ICD | Late adulthood | Forearm | Not used | 46 | Low titer | 0.8 |
| against Der f § | ||||||||
| 15 | 83/F | EE | Elderly | Back | Not used | 97 | Negative § | 21.6 |
| 16 | 82/M | EE | Elderly | Forearm | Not used | 1429 | Negative § | 33.9 |
| 17 | 77/M | BP with ES | Elderly | Sole | Not used | 469 | NT | NA |
| Category | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Case | Disease | Double-Immunofluorescence † | Immunohistochemistry ‡ | ||||||||||||
| Epidermis | Dermis | Epidermis | Dermis | ||||||||||||
| IgE+ | IgE+ | IgE− | IgE+ | CD206+ | CD207+ | IgE+ | CD206+ | IgE+ | IgE+ | IgE− | CD11c+ | CD207+ | CD11c+ | ||
| CD11c+ | CD206+ | CD206+ | Der f1+ | Der f1+ | Der f1+ | Mite ext.+ | Mite ext.+ | CD11c+ | Der f1+ | Der f1+ | Cells | Cells | Cells | ||
| Cells | Cells | Cells | Cells | Cells | Cells | Cells | Cells | Cells | Cells | Cells | |||||
| AD | |||||||||||||||
| 1 | AD | 43 | 28 | 6 | 13 | 10 | 10 | 11 | 9 | 44 | 9 | 11 | 45 | 46 | 83 |
| 2 | AD | 50 | 52 | 1 | 11 | 7 | 3 | 8 | 23 | 60 | 14 | 16 | 35 | 26 | 96 |
| 3 | AD | 12 | 21 | 3 | 5 | 1 | 3 | 5 | 2 | 41 | 14 | 18 | 42 | 30 | 85 |
| 4 | AD | 23 | 6 | 1 | 0 | 2 | 0 | 0 | 0 | 70 | 5 | 4 | 45 | 45 | 68 |
| 5 | AD | 11 | 11 | 0 | 23 | 8 | 14 | NA | NA | 40 | 12 | 15 | 6 | 27 | 22 |
| 6 | AD | 21 | 15 | 1 | 6 | 8 | 2 | 8 | 12 | 44 | 15 | 14 | 11 | 10 | 60 |
| Mean (±SD) ¶ | 26.7 (±16.2) *,** | 22.2 (±16.5) *,** | 2.0 (±2.2) | 9.7 (±8.0) *,** | 6.0 (±3.6) *,** | 5.3 (±5.4) | 6.4 (±4.2) § *,** | 9.2 (±9.1) § | 49.8 (±12.3) *,** | 11.5 (±3.8) *,** | 13 (±5.0) *,** | 30.7 (±17.6) * | 30.7 (±13.4) | 69 (±26.4) | |
| Non-eczematous inflammatory skin disorders with serum hyper-IgE | |||||||||||||||
| 7 | EGPA | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 6 | 20 | 39 |
| 8 | DH | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 3 | 0 | 0 | 1 | 26 | 61 |
| 9 | BP | 3 | 2 | 0 | 0 | 0 | 0 | 0 | 0 | 3 | 2 | 4 | 0 | 13 | 46 |
| 10 | BP | 0 | 0 | 0 | 0 | 0 | 2 | 0 | 0 | 4 | 0 | 0 | 1 | 9 | 68 |
| 11 | BP | 1 | 1 | 1 | 0 | 0 | 8 | 0 | 0 | 11 | 0 | 4 | 3 | 31 | 30 |
| 12 | MPE | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 9 | 4 | 4 | 1 | 36 | 38 |
| Mean (±SD) ¶ | 0.7 (±1.2) | 0.5 (±0.8) | 0.2 (±0.4) | 0 (±0) | 0.2 (±0.4) | 1.7 (±3.2) | 0 (±0) | 0 (±0) | 5.2 (±3.9) | 1 (±1.7) | 2 (±2.2) | 2 (±2.2) | 22.5 (±10.4) | 47 (±14.6) | |
| Inflammatory skin disorders with spongiotic tissue within the epidermis | |||||||||||||||
| 13 | NE | 0 | 0 | 54 | 0 | 0 | 0 | 0 | 1 | 2 | 0 | 0 | 78 | 12 | 81 |
| 14 | ICD | 0 | 0 | 25 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 1 | 37 | 16 | 82 |
| 15 | EE | 0 | 0 | 15 | 0 | 0 | 4 | 0 | 0 | 0 | 0 | 0 | 22 | 43 | 130 |
| 16 | EE | 0 | 0 | 11 | 0 | 0 | 1 | 1 | 0 | 2 | 0 | 0 | 21 | 40 | 56 |
| 17 | BP with ES | 0 | 0 | 12 | 0 | 0 | 2 | 0 | 0 | 0 | 0 | 0 | 66 | 28 | 49 |
| Mean (±SD) ¶ | 0 (±0) | 0 (±0) | 23.4 (±18.0) | 0 (±0) | 0 (±0) | 1.8 (±1.5) | 0.2 (±0.4) | 0.2 (±0.4) | 0.8 (±1.1) | 0 (±0) | 0.2 (±0.4) | 44.8 (±25.9) | 27.8 (±13.9) | 79.6 (±31.8) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tanei, R.; Hasegawa, Y. Immunohistopathological Analysis of Immunoglobulin E-Positive Epidermal Dendritic Cells with House Dust Mite Antigens in Naturally Occurring Skin Lesions of Adult and Elderly Patients with Atopic Dermatitis. Dermatopathology 2021, 8, 426-441. https://0-doi-org.brum.beds.ac.uk/10.3390/dermatopathology8030045
Tanei R, Hasegawa Y. Immunohistopathological Analysis of Immunoglobulin E-Positive Epidermal Dendritic Cells with House Dust Mite Antigens in Naturally Occurring Skin Lesions of Adult and Elderly Patients with Atopic Dermatitis. Dermatopathology. 2021; 8(3):426-441. https://0-doi-org.brum.beds.ac.uk/10.3390/dermatopathology8030045
Chicago/Turabian StyleTanei, Ryoji, and Yasuko Hasegawa. 2021. "Immunohistopathological Analysis of Immunoglobulin E-Positive Epidermal Dendritic Cells with House Dust Mite Antigens in Naturally Occurring Skin Lesions of Adult and Elderly Patients with Atopic Dermatitis" Dermatopathology 8, no. 3: 426-441. https://0-doi-org.brum.beds.ac.uk/10.3390/dermatopathology8030045