Comparing the Antimicrobial In Vitro Efficacy of Amoxicillin/Metronidazole against Azithromycin—A Systematic Review

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Eligibility Criteria for Studies
2.4. Data Extraction
3. Results
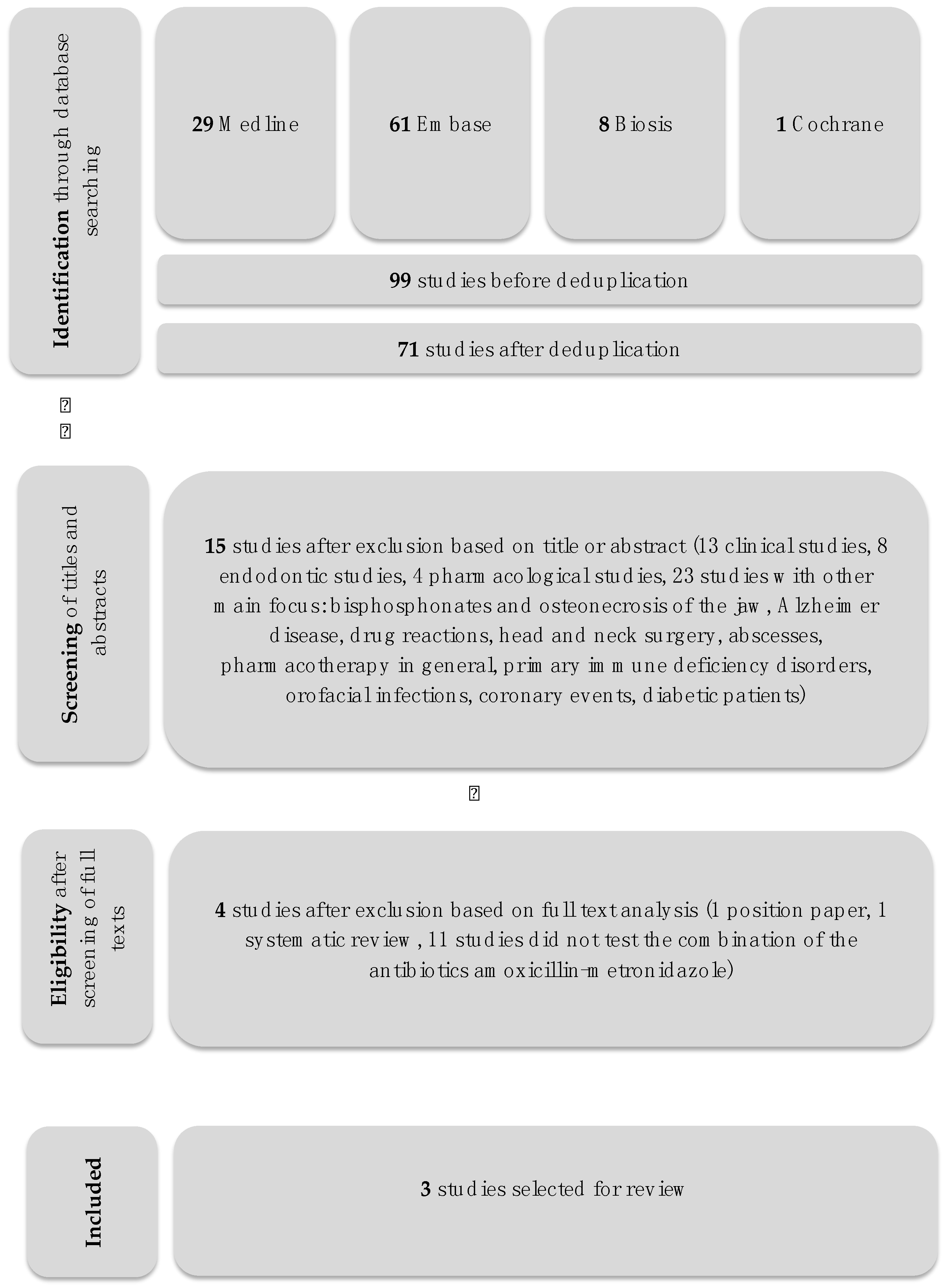
3.1. Search and Screening
3.2. Experimental Methods in the Evaluated Studies
3.3. Antimicrobial Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Harris, R.J. Untreated periodontal disease: A follow-up on 30 cases. J. Periodontol. 2003, 74, 672–678. [Google Scholar] [CrossRef] [PubMed]
- Meyle, J.; Chapple, I. Molecular aspects of the pathogenesis of periodontitis. Periodontology 2000 2015, 69, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Slots, J.; Ting, M. Systemic antibiotics in the treatment of periodontal disease. Periodontology 2000 2002, 28, 106–176. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; Cionca, N.; Almaghlouth, A. Does adjunctive antimicrobial therapy reduce the perceived need for periodontal surgery. Periodontology 2000 2011, 55, 205–216. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A. Microbial colonization of the periodontal pocket and its significance for periodontal therapy. Periodontology 2000 2018, 76, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Buset, L.S.; Zitzmann, N.U.; Weiger, R.; Walter, C. Non-surgical periodontal therapy supplemented with systemically administered azithromycin: A systematic review of RCTs. Clin Oral Investig. 2015, 19, 1763–1775. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; Prisma-p, G. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015, 2015, elaboration and explanation. BMJ 2015, 350, G7647. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forrest, L.J.; Miller, S.A. Evidence-based decision making in action: Part 1—Finding the best clinical evidence. J. Contemp. Dent. Pract. 2002, 3, 10–26. [Google Scholar] [PubMed]
- Hernández-rizzo, G.A. Usefulness of antimicrobial agents in periodontal disease. Inf. Med. 2003, 5, 97–100. [Google Scholar]
- Slots, J. Position paper: Systemic antibiotics in periodontics. J. Periodontol. 2004, 75, 1553–1565. [Google Scholar] [PubMed]
- Alattas, A.H.; Alyami, S.H. Prescription of antibiotics for pulpal and periapical pathology among dentists in southern Saudi Arabia. J. Glob. Antimicrob. Resist. 2017, 9, 82–84. [Google Scholar] [CrossRef] [PubMed]
- Barbosa-ribeiro, M.; De-jesus-soares, A.; Zaia, A.A.; Ferraz, C.C.R.; Almeida, J.F.A.; Gomes, B.P.F.A. Antimicrobial susceptibility and characterization of virulence genes of enterococcus faecalis isolates from teeth with failure of the endodontic treatment. J. Endod. 2016, 42, 1022–1028. [Google Scholar] [CrossRef] [PubMed]
- Bartold, M.P.; Bois, A.H.D.; Gannon, S.; Haynes, D.R.; Hirsch, R.S. Antibacterial and immunomodulatory properties of azithromycin treatment implications for periodontitis. Inflammopharmacology 2013, 21, 321–338. [Google Scholar] [CrossRef] [PubMed]
- Belibasakis, N.G.; Thurnheer, T. Validation of antibiotic efficacy on in vitro subgingival biofilms. J. Periodontol. 2014, 85, 343–348. [Google Scholar] [CrossRef] [PubMed]
- Brook, I. Fusobacterial infections in children. Curr. Infect. Dis. Rep. 2013, 15, 288–294. [Google Scholar] [CrossRef] [PubMed]
- Brook, I. Fusobacterial head and neck infections in children. Int. J. Pediatr. Otorhinolaryngol. 2015, 79, 953–958. [Google Scholar] [CrossRef] [PubMed]
- Carrasco, E.; Martinez, M.; Calbacho, M.; Wilckens, M. In vitro activity of amoxicillin, tetracyclines, azithromycin, ofloxacin and metronidazole against porphyromonas gingivalis, prevotella intermedia and fusobacterium nucleatum strains. Anaerobe 2000, 5, 443–445. [Google Scholar] [CrossRef]
- Chopra, D.; Sharma, V.; Kapoor, R.; Dwivedi, S. An observational study of cutaneous adverse drug reactions in a teaching hospital. Int. J. Clin. Pharm. 2015, 37, 996–999. [Google Scholar] [CrossRef] [PubMed]
- Coulaud, J.P. Azithromyin: New trends. Pathol. Boil. 1995, 43, 547–550. [Google Scholar]
- Dakic, A.; Boillot, A.; Colliot, C.; Carra, M.C.; Czernichow, S.; Bouchard, P. Detection of porphyromonas gingivalis and aggregatibacter actinomycetemcomitans after systemic administration of amoxicillin plus metronidazole as an adjunct to non-surgical periodontal therapy: A systematic review and meta-analysis. Front. Microbiol. 2016, 7, 1277. [Google Scholar] [CrossRef] [PubMed]
- Ercan, E.; Uzun, B.C.; Ustaoglu, G. Effects of azithromycin versus metronidazole-amoxicillin combination as an adjunct to nonsurgical periodontal therapy of generalized aggressive periodontitis. Niger. J. Clin. Pract. 2015, 18, 506–510. [Google Scholar] [CrossRef] [PubMed]
- Feik, D.; Mortensen, J.E.; Rhoads, S.L.; Egleton, J.; Rams, T.E. Antibiotic susceptibility profile of periodontal streptococcus constellatus. Abstr. Gen. Meet. Am. Soc. Microbiol. 2001, 101, 3–4. [Google Scholar]
- Martinez, M.J.F.; de castro, A.M.B.; Sanchez, E.G.; Sanchez, J.E.G.; Rodriguez, J.A.G. The current state and perspectives on antibiotic treatment for odontogene infections. Rev. Espanola De Quimioter. 1997, 10, 203–211. [Google Scholar]
- Garg, K.A.; Agrawal, N.; Tewari, R.K.; Kumar, A.; Chandra, A. Antibiotic prescription pattern among indian oral healthcare providers: A cross-sectional survey. J. Antimicrob. Chemother. 2014, 69, 526–528. [Google Scholar] [CrossRef] [PubMed]
- Greenstein, G. Efficacy of subantimicrobial-dose doxycycline in the treatment of periodontal diseases: A critical evaluation. Int. J. Periodontics Restor. Dent. 2004, 24, 528–543. [Google Scholar]
- Harris, A.S.; Harris, E.A. Herpes simplex virus type 1 and other pathogens are key causative factors in sporadic alzheimer’s disease. J. Alzheimer’s Dis. 2015, 48, 319–353. [Google Scholar] [CrossRef] [PubMed]
- Herrera, D.; Matesanz, P.; Bascones-martinez, A.; Sanz, M. Local and systemic antimicrobial therapy in periodontics. J. Evid.-Based Dent. Pract. 2012, 12, 50–60. [Google Scholar] [CrossRef]
- Isla, A.A.; Canut, A.; Rodriguez-gascon, P.; Planells, P.; Beltri-orta, J.I.; Salmeron-escobar, A.; Labora, A.; Pedraz, J.L. Antibiotic therapy in odontogenic infections in children and adolescents: Pharmacokinetic/pharmacodynamic analysis. Enferm. Infecc. Microbiol. Clin. 2008, 26, 621–628. [Google Scholar] [CrossRef]
- Jacinto, C.R.; Gomes, B.P.F.A.; Ferraz, C.C.R.; Zaia, A.A.; Filho, F.J.S. Microbiological analysis of infected root canals from symptomatic and asymptomatic teeth with periapical periodontitis and the antimicrobial susceptibility of some isolated anaerobic bacteria. Oral Microbiol. Immunol. 2003, 18, 285–292. [Google Scholar] [CrossRef] [PubMed]
- Japoni, A.; Vasin, A.; Noushadi, S.; Kiany, F.; Japoni, S.; Alborzi, A. Antibacterial susceptibility patterns of porphyromonas gingivalis isolated from chronic periodontitis patients. Med. Oral Patol. Oral Cir. Bucal 2011, 16, e1031-5. [Google Scholar] [CrossRef] [PubMed]
- Jaramillo, A.; Arce, R.M.; Herrera, D.; Betancourth, M.; Botero, J.E.; Contreras, A. Clinical and microbiological characterization of periodontal abscesses. J. Clin. Periodontol. 2005, 32, 1213–1218. [Google Scholar] [CrossRef] [PubMed]
- Jentsch, R.H.F.; Buchmann, A.; Friedrich, A.; Eick, S. Nonsurgical therapy of chronic periodontitis with adjunctive systemic azithromycin or amoxicillin/metronidazole. Clin. Oral Investig. 2016, 20, 1765–1773. [Google Scholar] [CrossRef] [PubMed]
- Keestra, J.J.A.; Grosjean, I.; Coucke, W.; Quirynen, M.; Teughels, W. Non-surgical periodontal therapy with systemic antibiotics in patients with untreated chronic periodontitis: A systematic review and meta-analysis. J. Periodontal Res. 2015, 50, 294–314. [Google Scholar] [CrossRef] [PubMed]
- Kuriyama, T.; Williams, D.W.; Yanagisawa, M.; Iwahara, K.; Shimizu, C.; Nakagawa, K.; Yamamoto, E.; Karasawa, T. Antimicrobial susceptibility of 800 anaerobic isolates from patients with dentoalveolar infection to 13 oral antibiotics. Oral Microbiol. Immunol. 2007, 22, 285–288. [Google Scholar] [CrossRef] [PubMed]
- Kuruvilla, M.; de la morena, M.T. Antibiotic prophylaxis in primary immune deficiency disorders. J. Allergy Clin. Immunol. Pract. 2013, 1, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Leszczyńska, A.; Buczko, P.; Buczko, W.; Pietruska, M. Periodontal pharmacotherapy—An updated review. Adv. Med. Sci. 2011, 56, 123–131. [Google Scholar] [CrossRef] [PubMed]
- Liu, F.P.; Zhu, W.H.; Huang, C.M. Vaccines and photodynamic therapies for oral microbial-related diseases. Curr. Drug Metab. 2009, 10, 90–94. [Google Scholar] [CrossRef] [PubMed]
- Loesche, W.J. The antimicrobial treatment of periodontal disease: Changing the treatment paradigm. Crit. Rev. Oral Boil. Med. 1999, 10, 245–275. [Google Scholar] [CrossRef]
- Maestre, R.J.; Bascones, A.; Sanchez, P.; Matesanz, P.; Aguilar, L.; Gimenez, M.J.; Perez-balcabao, I.; Granizo, J.J.; Prieto, J. Odontogenic bacteria in periodontal disease and resistance patterns to common antibiotics used as treatment and prophylaxis in odontology in Spain. Rev. Esp. Quimioter. Publ. De La Soc. Esp. De Quimioter. 2007, 20, 61–67. [Google Scholar]
- Mahajan, A.; Sharma, V.; Vats, A.; Srivastav, A. Pattern of antibiotic prescription in the management of endodontic infections amongst oral and maxillofacial surgeons and endodontists in Gujarat. Indian J. Public Health Res. Dev. 2012, 3, 1–3. [Google Scholar]
- Mattina, R. Clarithromycin in dental infections. Trends Med. 2007, 7, 71–80. [Google Scholar]
- Mcgowan, K. Insufficient evidence to compare the efficacy of treatments for medication-related osteonecrosis of the jaws. J. Evid. Based Dent. Pract. 2018, 18, 70–72. [Google Scholar] [CrossRef] [PubMed]
- Mouratidou, A.; Karbach, J.; D’hoedt, B.; Al-nawas, B. Antibiotic susceptibility of cocultures in polymicrobial infections such as peri-implantitis or periodontitis: An in vitro model. J. Periodontol. 2011, 82, 1360–1366. [Google Scholar] [CrossRef] [PubMed]
- Muniz, G.F.W.M.; de oliveira, C.C.; Carvalho, R.D.; Moreira, M.M.S.M.; de moraes, M.E.A.; Martins, R.S. Azithromycin: A new concept in adjuvant treatment of periodontitis. Eur. J. Pharmacol. 2013, 705, 135–139. [Google Scholar] [CrossRef] [PubMed]
- Murillo, J. Treatment of bacterial orofacial infections. Med. Oral 2003, 8, 154. [Google Scholar] [PubMed]
- Ong, S.H.; Oettinger-barak, O.; Dashper, S.G.; Darby, I.B.; Tan, K.H.; Reynolds, E.C. Effect of azithromycin on a red complex polymicrobial biofilm. J. Oral Microbiol. 2017, 9, 1339579. [Google Scholar] [CrossRef] [PubMed]
- Paju, S.; Sinisalo, J.; Pussinen, P.J.; Valtonen, V.; Nieminen, M.S. Is periodontal infection behind the failure of antibiotics to prevent coronary events? Atherosclerosis 2007, 193, 193–195. [Google Scholar] [CrossRef] [PubMed]
- Palappallil, S.D.; Ramnath, S.N.; Gangadhar, R. Adverse drug reactions: Two years’ experience from a tertiary teaching hospital in Kerala. Natl. J. Physiol. Pharm. Pharmacol. 2017, 7, 403–411. [Google Scholar] [CrossRef]
- Papathanasiou, E.; Finkelman, M.; Hanley, J.; Parashis, A.O. Prevalence, etiology and treatment of peri-implant mucositis and peri-implantitis: A survey of periodontists in the United States. J. Periodontol. 2016, 87, 493–501. [Google Scholar] [CrossRef] [PubMed]
- Parenti, A.; Paccosi, S.; Cairo, F.; Defraia, E. Treatment of periodontitis for the prevention of endothelial dysfunction: A narrative review. Curr. Vasc. Pharmacol. 2015, 13, 749–758. [Google Scholar] [CrossRef] [PubMed]
- Parnham, M.J. Immunomodulatory approaches to the treatment of infections. Infektol. Glas. 2011, 31, 15–27. [Google Scholar]
- Rams, E.T.; Feik, D.; Mortensen, J.E.; Degener, J.E.; van winkelhoff, A.J. Antibiotic susceptibility of periodontal streptococcus constellatus and streptococcus intermedius clinical isolates. J. Periodontol. 2014, 85, 1792–1798. [Google Scholar] [CrossRef] [PubMed]
- Ramu, C.; Padmanabhan, T.V. Indications of antibiotic prophylaxis in dental practice-review. Asian Pac. J. Trop. Biomed. 2012, 2, 749–754. [Google Scholar] [CrossRef]
- Ranganathan, A.T.; Gita, B.; Ramya, V. Role of systemic antibiotics in the management of periodontal diseases. Biomed. Pharmacol. J. 2015, 8SE, 691–694. [Google Scholar] [CrossRef]
- De sousa, E.L.R.; Ferraz, C.C.R.; Gomes, B.P.F.D.; Pinheiro, E.T.; Teixeira, F.B.; de souza-filho, F.J. Bacteriological study of root canals associated with periapical abscesses. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 96, 332–339. [Google Scholar] [CrossRef]
- Ryan, M.E. Nonsurgical approaches for the treatment of periodontal diseases. Dent. Clin. N. Am. 2005, 49, 611–636. [Google Scholar] [CrossRef] [PubMed]
- Saleh, A.; Rincon, J.; Tan, A.; Firth, M. Comparison of adjunctive azithromycin and amoxicillin/metronidazole for patients with chronic periodontitis: Preliminary randomized control trial. Aust. Dent. J. 2016, 61, 469–481. [Google Scholar] [CrossRef] [PubMed]
- Santos, L.C.M.M.; Lira, R.; Fischer, R.G.; Santos, A.P.P.; Oliveira, B.H. Systemic antibiotics in periodontal treatment of diabetic patients: A systematic review. PLoS ONE 2015, 10, doi. [Google Scholar] [CrossRef] [PubMed]
- Segura-egea, J.J.; Velasco-ortega, E.; Torres-lagares, D.; Velasco-ponferrada, M.C.; Monsalve-guil, L.; Llamas-carreras, J.M. Pattern of antibiotic prescription in the management of endodontic infections amongst Spanish oral surgeons. Int. Endod. J. 2010, 43, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Serrano, C.; Torres, N.; Valdivieso, C.; Castano, C.; Barrera, M.; Cabrales, A. Antibiotic resistance of periodontal pathogens obtained from frequent antibiotic users. Acta Odontol. Latinoam. AOL 2009, 22, 99–104. [Google Scholar] [PubMed]
- Sgolastra, F.; Severino, M.; Petrucci, A.; Gatto, R.; Monaco, A. Effectiveness of metronidazole as an adjunct to scaling and root planing in the treatment of chronic periodontitis: A systematic review and meta-analysis. J. Periodontal Res. 2014, 49, 10–19. [Google Scholar] [CrossRef] [PubMed]
- Shannon, J.; Shannon, J.; Modelevsky, S.; Grippo, A.A. Bisphosphonates and osteonecrosis of the jaw. J. Am. Geriatr. Soc. 2011, 59, 2350–2355. [Google Scholar] [CrossRef] [PubMed]
- Arora, A.; Khattri, S.; Ismail, N.M.; Nagraj, S.K.; Prashanti, E. School dental screening programmes for oral health. Cochrane Database Syst. Rev. 2017, 12, CD012595. [Google Scholar] [PubMed]
- Siqueira, F.J.; Rôças, I.N. Microbiology and treatment of acute apical abscesses. Clin. Microbiol. Rev. 2013, 26, 255–273. [Google Scholar] [CrossRef] [PubMed]
- Soares, S.G.M.; Teles, F.; Starr, J.R.; Feres, M.; Patel, M.; Martin, L.; Teles, R. Effects of azithromycin, metronidazole, amoxicillin, and metronidazole plus amoxicillin on an in vitro polymicrobial subgingival biofilm model. Antimicrob. Agents Chemother. 2015, 59, 2791–2798. [Google Scholar] [CrossRef] [PubMed]
- Somma, F.; Castagnola, R.; Bollino, D.; Marigo, L. Oral inflammatory process and general health part 2011, 2, how does the periapical inflammatory process compromise general health? Eur. Rev. Med. Pharmacol. Sci. 2011, 15, 35–51. [Google Scholar] [PubMed]
- Sousa, R.E.L.; Gomes, B.P.F.A.; Jacinto, R.C.; Zaia, A.A.; Ferraz, C.C.R. Microbiological profile and antimicrobial susceptibility pattern of infected root canals associated with periapical abscesses. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2013, 32, 573–580. [Google Scholar] [CrossRef] [PubMed]
- Souto, S.M.L.; Rovai, E.S.; Ganhito, J.A.; Holzhausen, M.; Chambrone, L.; Pannuti, C.M. Efficacy of systemic antibiotics in nonsurgical periodontal therapy for diabetic subjects: A systematic review and meta-analysis. Int. Dent. J. 2018, 68, 207–220. [Google Scholar] [CrossRef] [PubMed]
- Sweeny, C.L.; Dave, J.; Chambers, P.A.; Heritage, J. Antibiotic resistance in general dental practice—A cause for concern? J. Antimicrob. Chemother. 2004, 53, 567–576. [Google Scholar] [CrossRef] [PubMed]
- Tarullo, A.; Tattoli, M.; Cagiano, R. Persistent eradication of helicobacter pylori after systemic politherapy associated with periodontal pockets treatment with metronidazole and calcium sulphate. Eur. Rev. Med. Pharmacol. Sci. 2001, 5, 127–129. [Google Scholar] [PubMed]
- Teughels, W.; Dhondt, R.; Dekeyser, C.; Quirynen, M. Treatment of aggressive periodontitis. Periodontology 2000 2014, 65, 107–133. [Google Scholar] [CrossRef] [PubMed]
- Tomas, I.; Tomas, M.; Alvarez, M.; Velasco, D.; Potel, C.; Limeres, J.; Diz, P. Susceptibility of oral obligate anaerobes to telithromycin, moxifloxacin and a number of commonly used antibacterials. Oral Microbiol. Immunol. 2007, 22, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Van den wyngaert, T.; Huizing, M.T.; Vermorken, J.B. Osteonecrosis of the jaw related to the use of bisphosphonates. Curr. Opin. Oncol. 2007, 19, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Van winkelhoff, A.J.; Herrera, D.; Winkel, E.G.; Dellemijn-kippuw, N.; Vandenbroucke-grauls, C.M.; Sanz, M. Antibiotic resistance in the subgingival microflora in patients with adult periodontitis. A comparative survey between Spain and The Netherlands. Antibiot. De Subgingivale Microflora Patienten Met Adulte Parod. Een Vgl. Onderz. Tussen Spanje En Ned. 1999, 106, 290–294. [Google Scholar]
- Van Winkelhoff, A.J.; Gonzales, D.H.; Winkel, E.G.; Dellemijn-kippuw, N.; Vandenbroucke-grauls, C.M.; Sanz, M. Antimicrobial resistance in the subgingival microflora in patients with adult periodontitis. A comparison between The Netherlands and Spain. J. Clin. Periodontol. 2000, 27, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Van Winkelhoff, A.J.; Herrera, D.; Oteo, A.; Sanz, M. Antimicrobial profiles of periodontal pathogens isolated from periodontitis patients in The Netherlands and Spain. J. Clin. Periodontol. 2005, 32, 893–898. [Google Scholar] [CrossRef] [PubMed]
- Veloo, M.A.C.; Seme, K.; Raangs, E.; Rurenga, P.; Singadji, Z.; Wekema-mulder, G.; van winkelhoff, A.J. Antibiotic susceptibility profiles of oral pathogens. Int. J. Antimicrob. Agents 2012, 40, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Voils, A.S.; Evans, M.E.; Lane, M.T.; Schosser, R.H.; Rapp, R.P. Use of macrolides and tetracyclines for chronic inflammatory diseases. Ann. Pharmacother. 2005, 39, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Zandbergen, D.; Slot, D.E.; Cobb, C.M.; van der weijden, F.A. The clinical effect of scaling and root planing and the concomitant administration of systemic amoxicillin and metronidazole: A systematic review. J. Periodontol. 2013, 84, 332–351. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zheng, Y.; Bian, X. Clinical effect of azithromycin as an adjunct to non-surgical treatment of chronic periodontitis: A meta-analysis of randomized controlled clinical trials. J. Periodontal Res. 2016, 51, 275–283. [Google Scholar] [CrossRef] [PubMed]
- Ammann, W.T.; Bostanci, N.; Belibasakis, G.N.; Thurnheer, T. Validation of a quantitative real-time PCR assay and comparison with fluorescence microscopy and selective agar plate counting for species-specific quantification of an in vitro subgingival biofilm model. J. Periodontal Res. 2013, 48, 517–526. [Google Scholar] [CrossRef] [PubMed]
- Socransky, S.S.; Haffajee, A.D.; Smith, C.; Martin, L.; Haffajee, J.A.; Uzel, N.G.; Goodson, J.M. Use of checkerboard DNA-DNA hybridization to study complex microbial ecosystems. Oral Microbiol. Immunol. 2004, 19, 352–362. [Google Scholar] [CrossRef] [PubMed]
- Socransky, S.S.; Haffajee, A.D. Dental biofilms: Difficult therapeutic targets. Periodontology 2000 2002, 28, 12–55. [Google Scholar] [CrossRef] [PubMed]
- Greenwood, D. Antimicrobial Drugs; Oxford University Press: Oxford, UK, 2008. [Google Scholar]
- Gomi, K.; Yashima, A.; Iino, F.; Kanazashi, M.; Nagano, T.; Shibukawa, N.; Ohshima, T.; Maeda, N.; Arai, T. Drug concentration in inflamed periodontal tissues after systemically administered azithromycin. J. Periodontol. 2007, 78, 918–923. [Google Scholar] [CrossRef] [PubMed]
- Haffajee, D.A.; Patel, M.; Socransky, S.S. Microbiological changes associated with four different periodontal therapies for the treatment of chronic periodontitis. Oral Microbiol. Immunol. 2008, 23, 148–157. [Google Scholar] [CrossRef] [PubMed]
- López-boado, S.Y.; Rubin, B.K. Macrolides as immunomodulatory medications for the therapy of chronic lung diseases. Curr. Opin. Pharmacol. 2008, 8, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Schreiber, F.; Szewzyk, U. Environmentally relevant concentrations of pharmaceuticals influence the initial adhesion of bacteria. Aquat. Toxicol. 2008, 87, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Hardy, J.D.; Hensey, D.M.; Beyer, J.M.; Vojtko, C.; Mcdonald, E.J.; Fernandes, P.B. Comparative in vitro activities of new 14-, 15-, and 16-membered macrolides. Antimicrob. Agents Chemother. 1988, 32, 1710–1719. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.B.; Sundareshan, V.; Cory, T.J.; Hayes, D.; Anstead, M.I.; Feola, D.J. Azithromycin alters macrophage phenotype. J. Antimicrob. Chemother. 2008, 61, 554–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Winkel, G.E.; van winkelhoff, A.J.; Timmerman, M.F.; van der velden, U.; van der weijden, G.A. Amoxicillin plus metronidazole in the treatment of adult periodontitis patients. A double-blind placebo-controlled study. J. Clin. Periodontol. 2001, 28, 296–305. [Google Scholar] [CrossRef] [PubMed]
- Beikler, T.; Karch, H.; Flemmig, T.F. Adjuvante antibiotika in der parodontitistherapie. Dtsch Zahnärztl 2003, 58, 263–265. [Google Scholar]
- Kleinfelder, W.J.; Müller, R.F.; Lange, D.E. Antibiotic susceptibility of putative periodontal pathogens in advanced periodontitis patients. J. Clin. Periodontol. 1999, 26, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Heekin, D.R.; Shorter, D.; Kosten, T.R. Current status and future prospects for the development of substance abuse vaccines. Expert Rev. Vaccines 2017, 16, 1067–1077. [Google Scholar] [CrossRef] [PubMed]
- Pähkla, R.E.; Koppel, T.; Saag, M.; Pähkla, R. Metronidazole concentrations in plasma, saliva and periodontal pockets in patients with periodontitis. J. Clin. Periodontol. 2005, 32, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Jain, N.; Lai, P.C.; Walters, J.D. Effect of gingivitis on azithromycin concentrations in gingival crevicular fluid. J. Periodontol. 2012, 83, 1122–1128. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Reference | Category | Exclusion Criteria | |
|---|---|---|---|
| 1) | 2004 Position paper [10] | pharma | description of systemic antibiotics in periodontics in general, not specifically in vitro |
| 2) | 2017 Alattas et al. [11] | endo | reporting about prescription of antibiotics usus in southern Saudi Arabia focusing endodontic pathology |
| 3) | 2016 Barbosa-Ribeiro et al. [12] | endo | focusing antimicrobial susceptibility after failure of endodontic treatment |
| 4) | 2013 Bartold et al. [13] | other | focusing only AZM |
| 5) | 2014 Belibasakis & Thurnheer [14] | in-vitro | |
| 6) | 2013 Brook [15] | other | focus on head and neck infections in general rather than periodontal aspects |
| 7) | 2015 Brook [16] | other | focus on head and neck infections in general rather than periodontal aspects |
| 8) | 2000 Carrasco et al. [17] | in-vitro | the combination of the antibiotics AMX-MTZ wasn’t tested |
| 9) | 2015 Chopra et al. [18] | other | focus on cutaneous adverse drug reactions |
| 10) | 1995 Coulaud [19] | other | focusing only AZM |
| 11) | 2016 Dakic et al. [20] | clin | clinical study, AZM wasn’t tested, systematic review and meta-analysis |
| 12) | 2015 Ercan et al. [21] | clin | clinical study, patients with chronic periodontitis |
| 13) | 2001 Feik et al. [22] | in-vitro | the combination of the antibiotics AMX-MTZ wasn’t tested |
| 14) | 1997 Fresnadillo et al. [23] | clin | clinical study |
| 15) | 2014 Garg et al. [24] | other | survey |
| 16) | 2004 Greenstein et al. [25] | clin | clinical study |
| 17) | 2015 Harris et al. [26] | other | focus on HSV-1 and Alzheimer disease |
| 18) | 2003 Hernandez-rizzo [9] | in-vitro | full text wasn’t available until data |
| 19) | 2012 Herrera et al. [27] | clin | clinical study |
| 20) | 2008 Isla et al. [28] | other | focus on odontogenic infections in general rather than periodontitis |
| 21) | 2003 Jacinto et al. [29] | endo | focus on analysis of infected root canals |
| 22) | 2011 Japoni et al. [30] | in-vitro | the combination of the antibiotics AMX-MTZ wasn’t tested |
| 23) | 2005 Jaramillo et al. [31] | other | clin and in vitro, but focus on abscesses |
| 24) | 2016 Jentsch et al. [32] | clin | clinical study |
| 25) | 2015 Keestra et al. [33] | clin | clinical study, systematic review and meta-analysis |
| 26) | 2007 Kuriyama et al. [34] | in-vitro | the combination of the antibiotics AMX-MTZ wasn’t tested |
| 27) | 2013 Kuruvilla et al. [35] | other | focus on primary immune deficiency disorders |
| 28) | 2011 Leszczyńska et al. [36] | pharma | updated review, focus on periodontal pharmacotherapy in general |
| 29) | 2009 Liu et al. [37] | other | focus on vaccines and PDT |
| 30) | 1999 Loesche [38] | other | critical review, focus on antimicrobial treatment of periodontal disease |
| 31) | 2007 Maestre et al. [39] | in-vitro | the combination of the antibiotics AMX-MTZ wasn’t tested |
| 32) | 2012 Mahajan et al. [40] | endo | focus on management of endodontic infections |
| 33) | 2007 Mattina [41] | other | focus on Clarithromycin |
| 34) | 2018 McGowan et al. [42] | clin | clinical study, AZM wasn’t tested, systematic review and meta-analysis of RCTs |
| 35) | 2011 Mouratidou et al. [43] | in-vitro | the combination of the antibiotics AMX-MTZ wasn’t tested |
| 36) | 2013 Muniz et al. [44] | other | focusing only AZM |
| 37) | 2003 Murillo [45] | clin | focus on orofacial infections |
| 38) | 2017 Ong et al. [46] | in-vitro | |
| 39) | 2007 Paju et al. [47] | other | focus on coronary events |
| 40) | 2017 Palappallil et al. [48] | pharma | focus on adverse drug reactions |
| 41) | 2016 Papathanasiou et al. [49] | other | a survey of periodontists in the US |
| 42) | 2015 Parenti et al. [50] | other | narrative review with focus on endothelial dysfunction |
| 43) | 2011 Parnham [51] | other | focus on immunology in general |
| 44) | 2014 Rams et al. [52] | in-vitro | the combination of the antibiotics AMX-MTZ wasn’t tested |
| 45) | 2012 Ramu et al. [53] | other | practice review on antibiotic prophylaxis |
| 46) | 2015 Ranganathan et al. [54] | clin | clinical study |
| 47) | 2003 Rolim De Sousa et al. [55] | endo | bacteriological study of root canals associated with periapical abscesses |
| 48) | 2005 Ryan [56] | clin | clinical study |
| 49) | 2016 Saleh et al. [57] | clin | clinical study, patients with chronic periodontitis |
| 50) | 2015 Santos et al. [58] | other | focus on diabetic patients, systematic review |
| 51) | 2010 Segura-Egea et al. [59] | endo | focus on management of endodontic infections amongst Spanish oral surgeons |
| 51) | 2009 Serrano et al. [60] | other | focus on antibiotic resistance of periodontal pathogens |
| 52) | 2012 Sgolastra et al. [61] | clin | clinical study, AZM wasn’t tested, systematic review and meta-analysis |
| 53) | 2011 Shannon et al. [62] | other | focus on Bisphosphonates and osteonecrosis of the jaw |
| 54) | 2017 Shivi et al. [63] | clin | clinical study |
| 55) | 2013 Siqueira et al. [64] | other | focus on abscesses |
| 56) | 2015 Soares et al. [65] | in-vitro | |
| 57) | 2011 Somma et al. [66] | endo | focus on endo and general health |
| 58) | 2013 Sousa et al. [67] | endo | focus on antimicrobial susceptibility pattern of infected root canals |
| 59) | 2018 Souto et al. [68] | clin | clinical study, focus on diabetic subjects, systematic review and meta-analysis |
| 60) | 2004 Sweeny et al. [69] | other | focus on antibiotic resistance in the dental practice |
| 61) | 2001 Tarullo et al. [70] | clin | focus on Helicobacter pylori |
| 62) | 2014 Teughels et al. [71] | clin | clinical study, patients with aggressive periodontitis |
| 63) | 2007 Tomas et al. [72] | in-vitro | the combination of the antibiotics AMX-MTZ wasn’t tested |
| 64) | 2007 Van Den Wyngaert et al. [73] | other | focus on osteonecrosis of the jaw and bisphosphonates |
| 65a),65b) | 1999, 2000 van Winkelhoff et al. [74,75] | in-vitro | the combination of the antibiotics AMX-MTZ wasn’t tested |
| 66) | 2005 van Winkelhoff et al. [76] | in-vitro | the combination of the antibiotics AMX-MTZ wasn’t tested |
| 67) | 2012 Veloo et al. [77] | in-vitro | the combination of the antibiotics AMX-MTZ wasn’t tested |
| 68) | 2005 Voils et al. [78] | clin | clinical study |
| 69) | 2013 Zandbergen et al. [79] | clin | clinical study, AZM wasn’t tested, systematic review |
| 70) | 2016 Zhang et al. [80] | clin | clinical study, the combination of the antibiotics AMX-MTZ wasn’t tested, meta-analysis of RCTs |
| Reference | Tested Outcome Parameters | Antibiotic | Results | Difference (Δ parameter:AMX/MTZ - AZM) |
|---|---|---|---|---|
| 2014 Belibasakis and Thurnheer Validation of antibiotic efficacy on in vitro subgingival biofilms. [14] | Log10 Reduction (TBC) Reduction of biofilm in % | Azithromycin | 0.4 log 60% | Δ 0.5 log Δ 27% |
| Amoxicillin/ Metronidazole | 0.9 log 87% | |||
| 2017 Ong et al. Effect of azithromycin on a red complex polymicrobial biofilm. [46] | MIC MBIC | Azithromycin | MIC 1.52 mg/L MBIC 10.6 mg/L | Δ MIC 1.35 mg/L Δ MBIC 9.3 mg/L |
| Amoxicillin/ Metronidazole | MIC 0.17 mg/L MBIC 1.3 mg/L | |||
| 2015 Soares et al. Effects of azithromycin, metronidazole, amoxicillin, and metronidazole plus amoxicillin on an in vitro polymicrobial subgingival biofilm model. Antimicrobial agents and chemotherapy. [65] | Reduction of metabolic activity in % | Azithromycin | 17% | Δ 67% |
| Amoxicillin/ Metronidazole | 84% |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaufmann, M.; Lenherr, P.; Walter, C.; Thurnheer, T.; Attin, T.; Wiedemeier, D.B.; Schmidlin, P.R. Comparing the Antimicrobial In Vitro Efficacy of Amoxicillin/Metronidazole against Azithromycin—A Systematic Review. Dent. J. 2018, 6, 59. https://0-doi-org.brum.beds.ac.uk/10.3390/dj6040059
Kaufmann M, Lenherr P, Walter C, Thurnheer T, Attin T, Wiedemeier DB, Schmidlin PR. Comparing the Antimicrobial In Vitro Efficacy of Amoxicillin/Metronidazole against Azithromycin—A Systematic Review. Dentistry Journal. 2018; 6(4):59. https://0-doi-org.brum.beds.ac.uk/10.3390/dj6040059
Chicago/Turabian StyleKaufmann, Manuela, Patrik Lenherr, Clemens Walter, Thomas Thurnheer, Thomas Attin, Daniel B. Wiedemeier, and Patrick R. Schmidlin. 2018. "Comparing the Antimicrobial In Vitro Efficacy of Amoxicillin/Metronidazole against Azithromycin—A Systematic Review" Dentistry Journal 6, no. 4: 59. https://0-doi-org.brum.beds.ac.uk/10.3390/dj6040059