Decontamination of Dental Implant Surfaces by the Er:YAG Laser Beam: A Comparative in Vitro Study of Various Protocols



Abstract
:1. Introduction
2. Materials and Methods
- Group A: Thirty sterile implants served as the control group. The implants of this group were kept in their own sterile packages, until their examination through EDX and SEM.
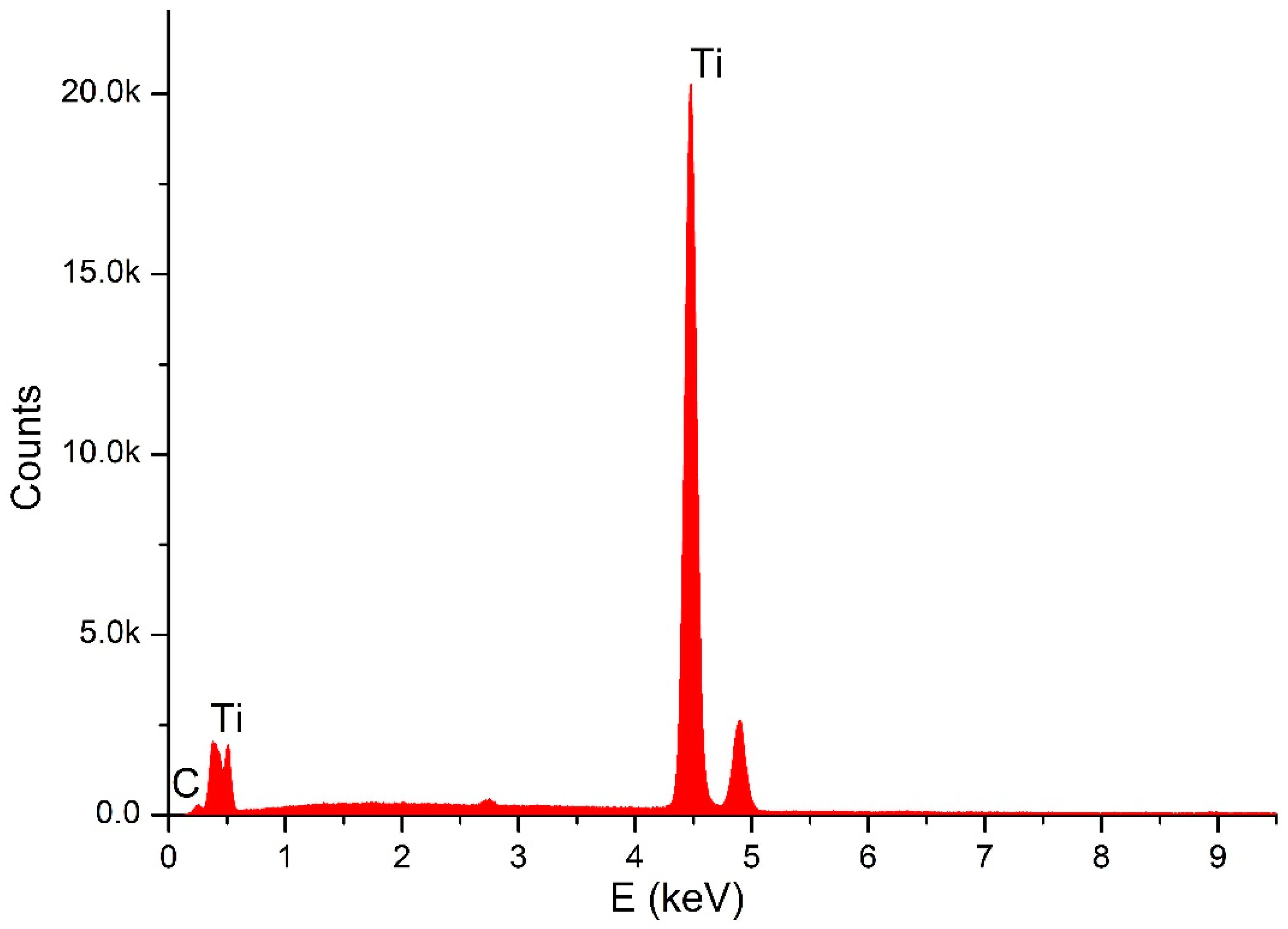
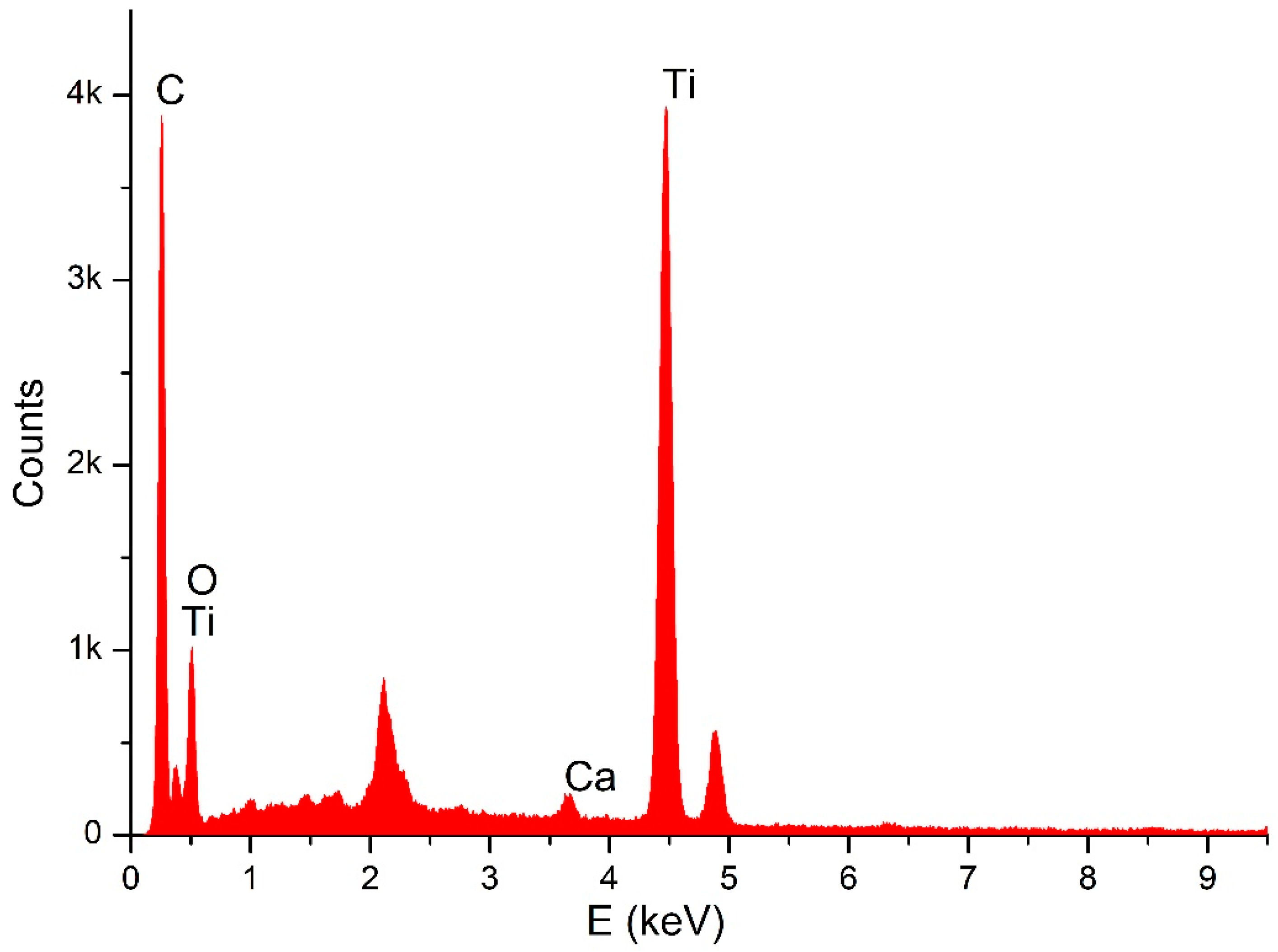
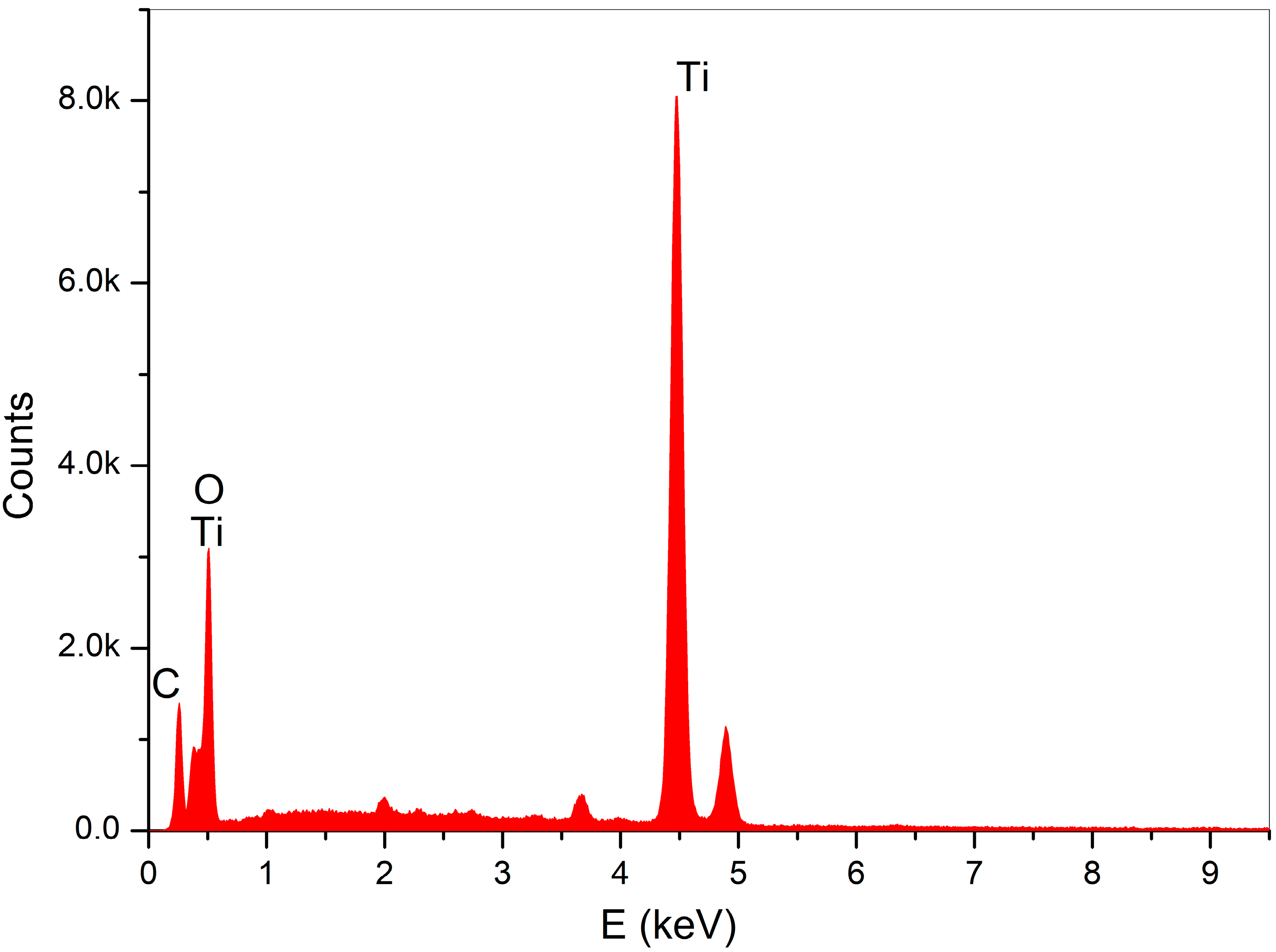
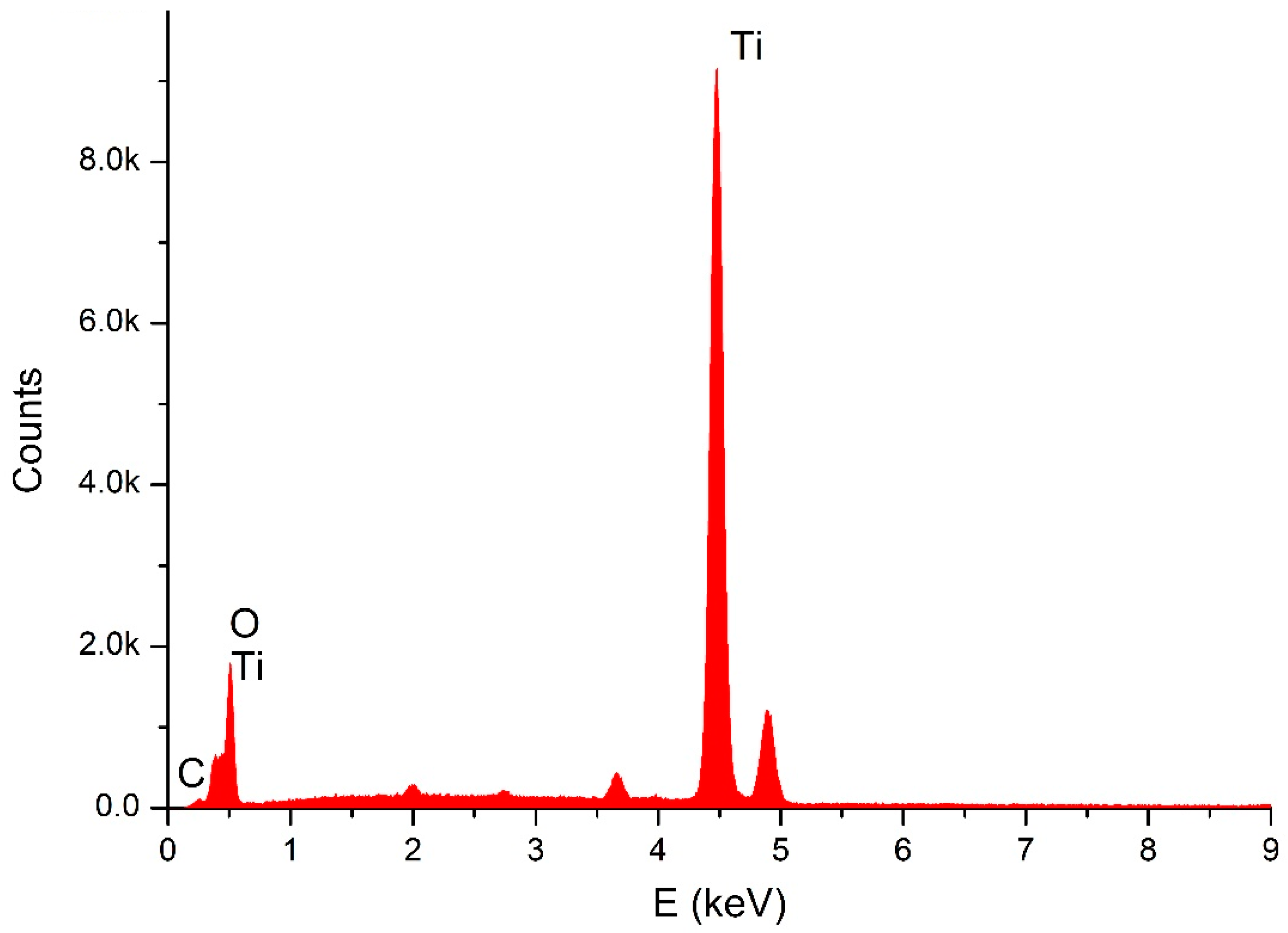
- Group B: Sixty contaminated implants were collected from failed cases of implants. The implants were retrieved from patients previously diagnosed with peri-implantitis. Their removal was not, in any of the cases, related to our study (severe peri-implantitis and bone resorbtion, loss of osteointegration, etc.). Before experimentation and for the purpose of standardization, all contaminated implants were preserved in sterile saline liquid of 0.9% NaCl, at a temperature of 37 °C, for the simulation of the intra-oral in vivo conditions; the solution was changed every 24 h, until experimentation. To assess the efficacy of the laser irradiation, in our study we compared the carbon percentage of the contaminated implant surfaces, before and after the laser irradiation. At the baseline, the sixty implants of Group B were all evaluated (eight points were randomly analyzed per sample), using energy dispersive X-ray analysis (SEM–EDX). After that, the implants were randomly assigned into two equal samples—LX1 and LX3—for the laser irradiation. Sample LX1 was irradiated by one passage and sample LX3, by three passages. Afterward, a second analysis of the carbon content of both samples was done.
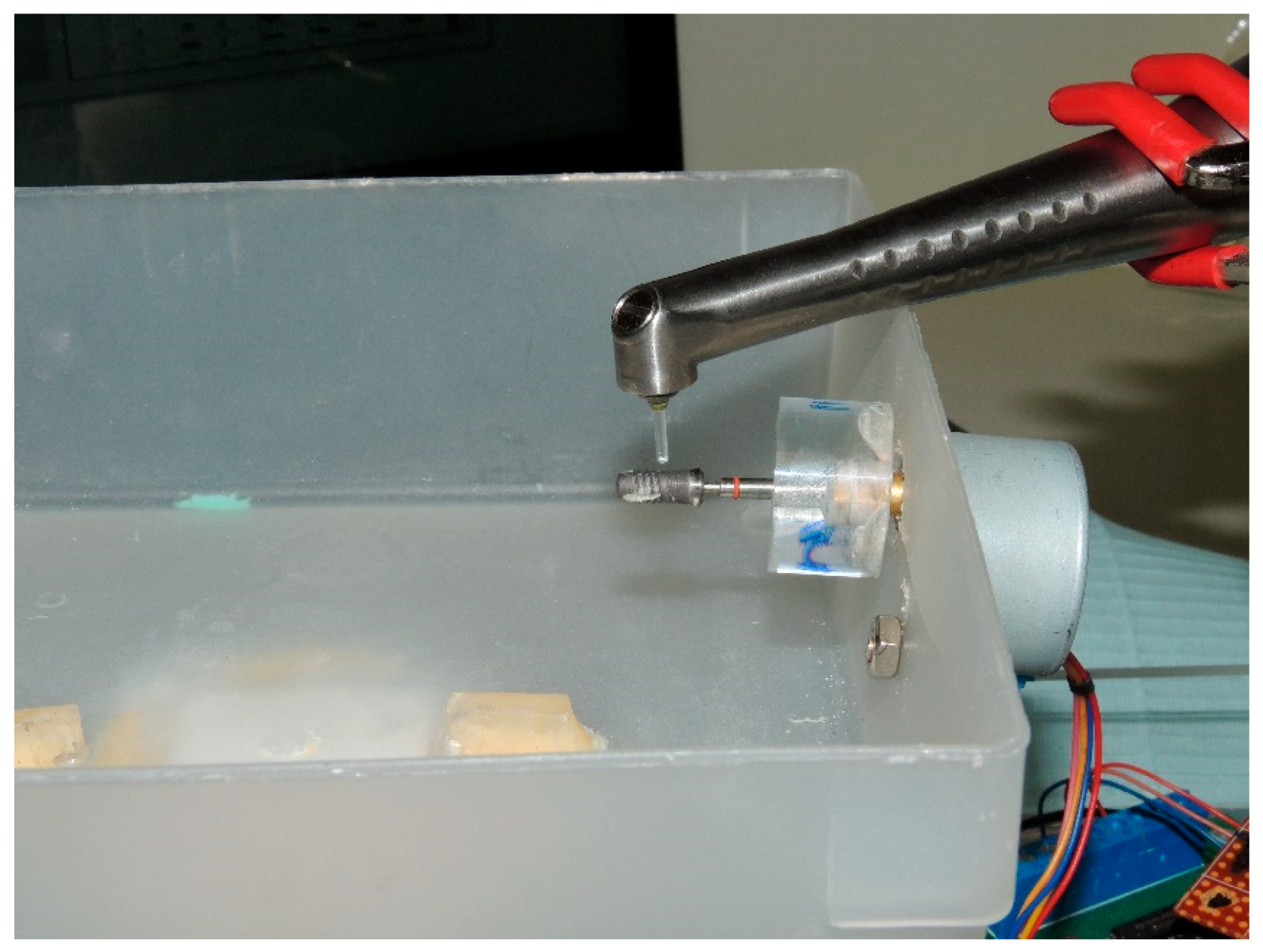
2.1. Decontamination
- (1)
- Standardize the angulation of the laser beam.
- (2)
- Standardize the distance between the tip of the handpiece and the implant surface.
- (3)
- Standardize the exposure time.
- (4)
- Have a semi-adjustable base on which an implant, connected to an abutment, is attached to a Plexiglass® plate.
- Thirty contaminated implants received one passage of laser (LX1).
- Thirty contaminated implants received three passages of laser (LX3).
2.2. Scanning Electron Microscopy
3. Statistical Analysis
4. Results
4.1. Analytical Results
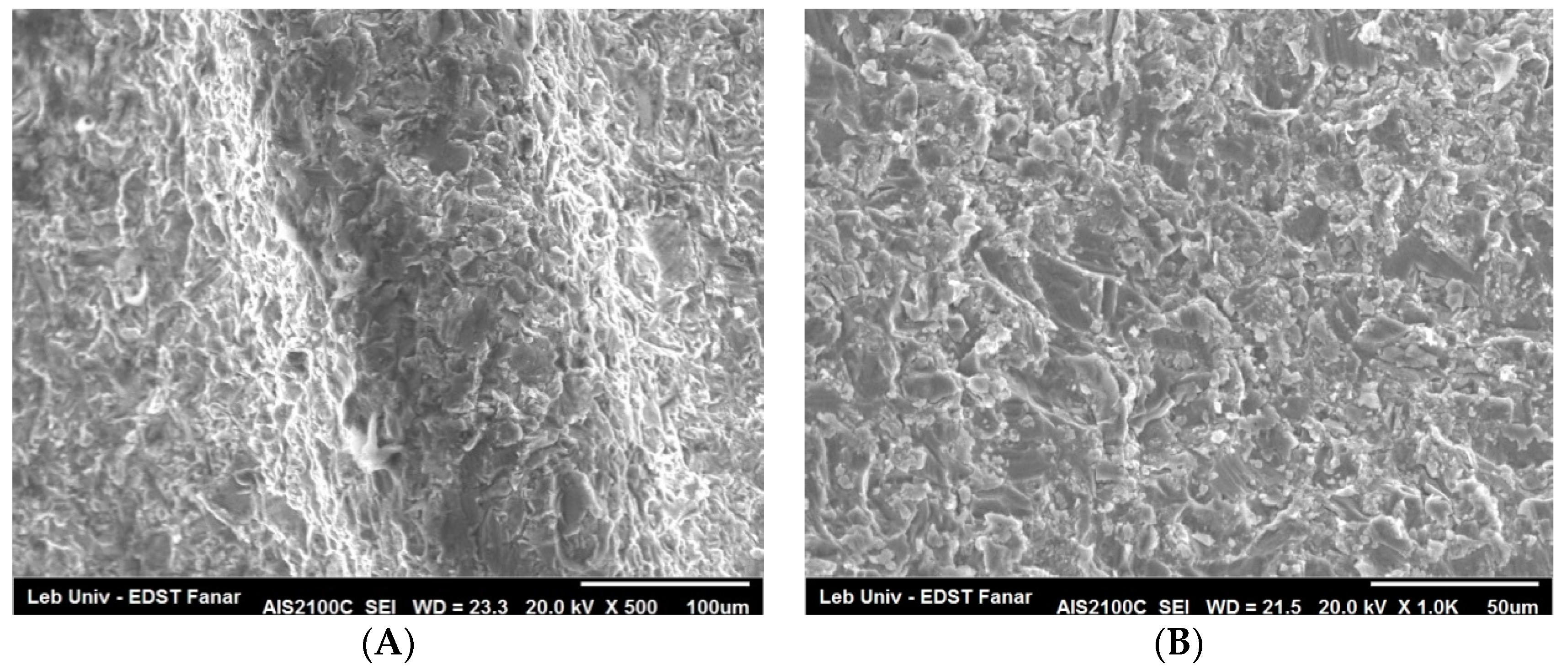
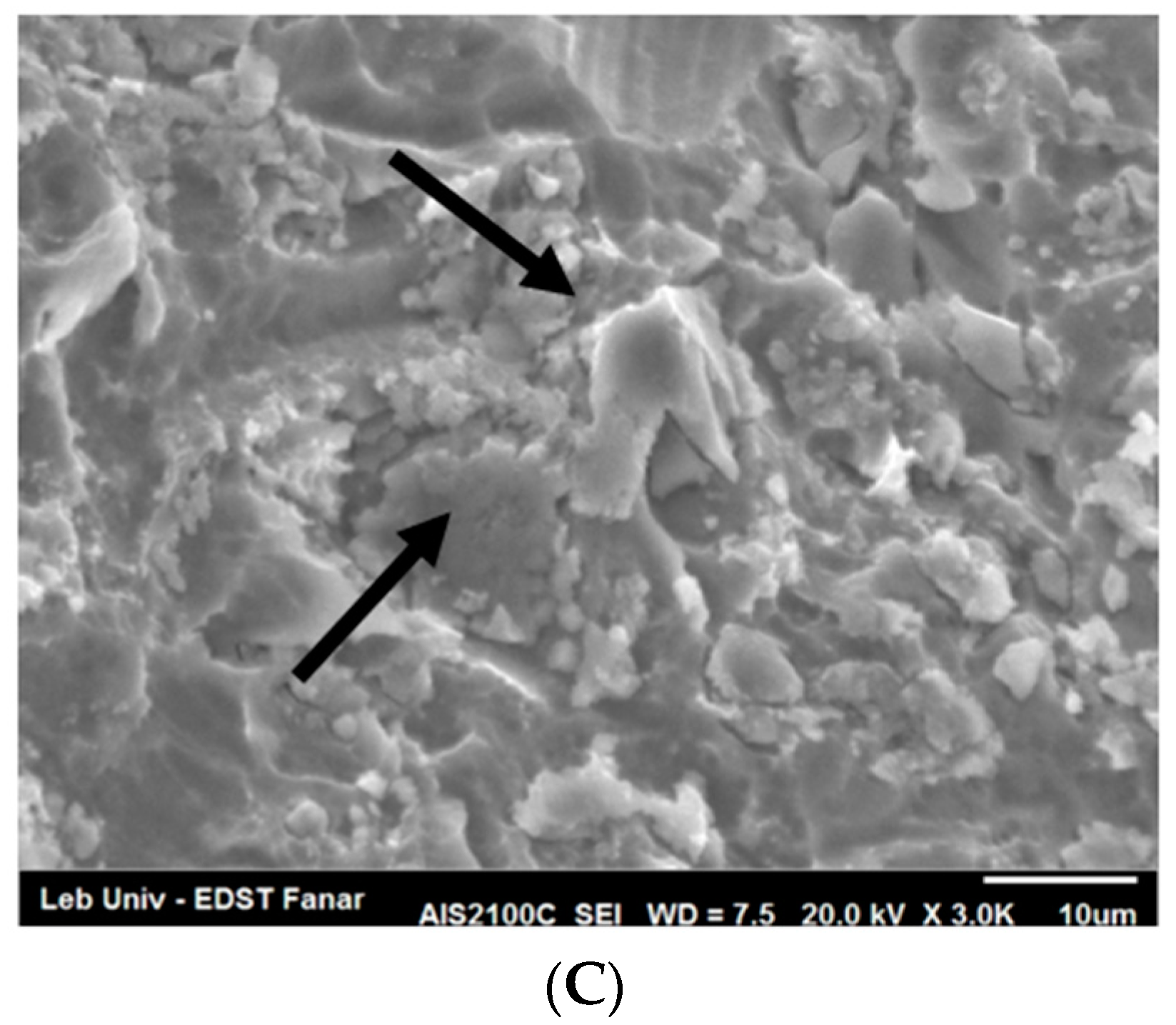
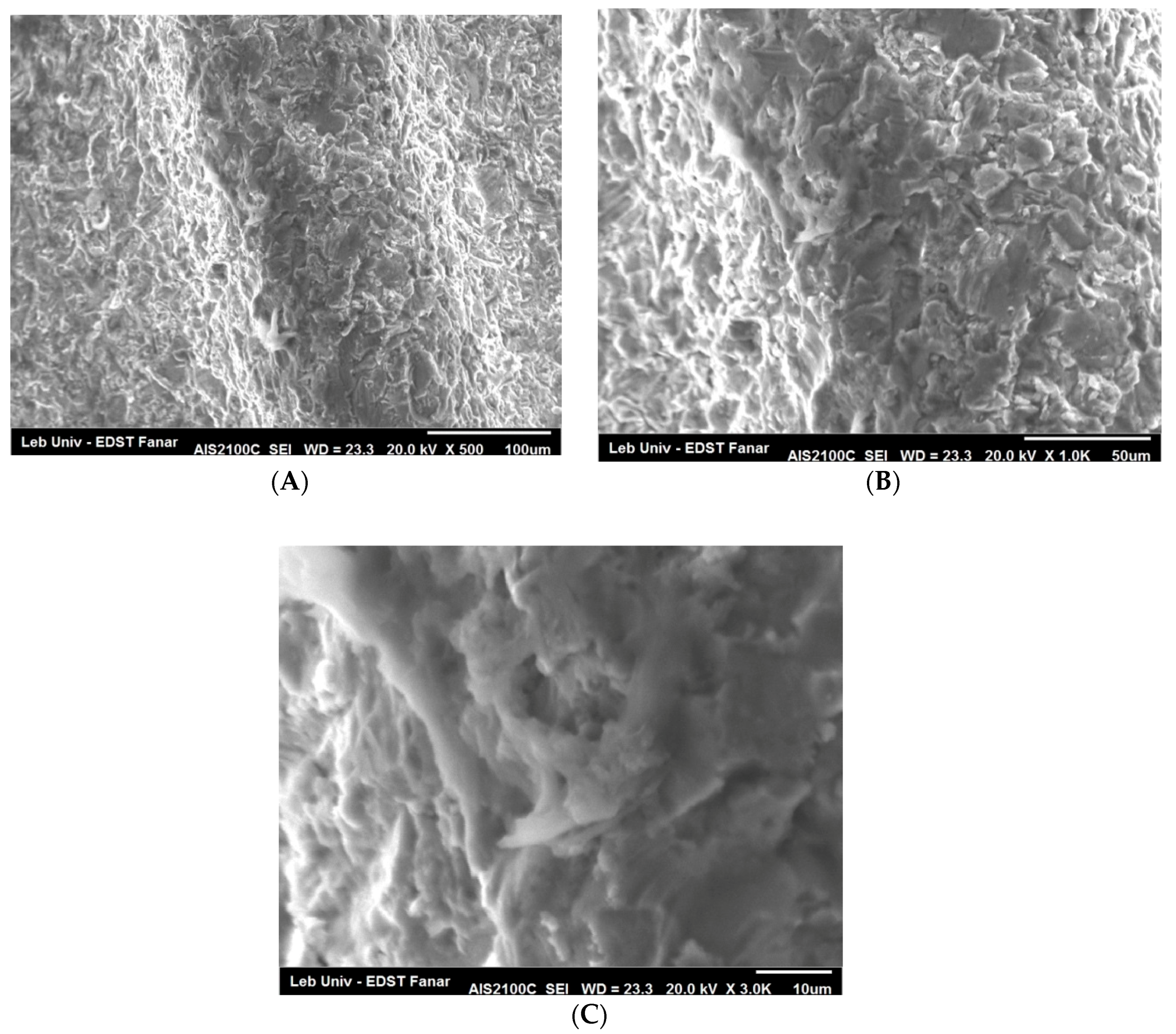
4.2. SEM Observations
5. Discussion
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Huynh-Ba, G. Thematic abstract review: Peri-implantitis: “Tsunami” or Marginal Problem? Int. J. Oral Maxillofac. Implants 2013, 28, 333–337. [Google Scholar]
- Mombelli, A.; Lang, N.P. The diagnosis and treatment of peri-implantitis. Periodontology 2000 1998, 17, 63–76. [Google Scholar] [CrossRef] [PubMed]
- Albrektsson, T.; Isidor, F. Consensus report of session IV. In Proceedings of the 1st European Workshop on Periodontology; Lang, N.P., Karring, T., Eds.; Quintessence Publishing: London, UK, 1994; pp. 365–369. [Google Scholar]
- Berglundh, T.; Persson, L.; Klinge, B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J. Clin. Periodontol. 2002, 29, 197–212. [Google Scholar] [CrossRef] [PubMed]
- Jayachandran Prathapachandran, N.S. Management of peri-implantitis. Dent. Res. J. (Isfahan) 2012, 9, 516–521. [Google Scholar] [CrossRef]
- Sheikh, Z.; Alshahrani, A.M.; Thaventhirarajah, K. Peri-Implantitis: Etiology and Management. EC Dent. Sci. ECO 2016, 1, 12–14. [Google Scholar]
- Kalesinskas, P.; Kačerguis, T.; Ambrozaitis, A.; Peciulienė, V.; Ericson, D. Reducing dental plaque formation and caries development. A review of current methods and implications for novel pharmaceuticals. Stomatol. Balt. Dent. Maxillofac. J. 2014, 16, 44–52. [Google Scholar]
- Romanos, G.E.; Montanaro, N.J.; Sacks, D.; Miller, R.J.; Javed, F.; Calvo-Guirado, J.L.; Delgado-Ruiz, R.A. Various Tip Applications and Temperature Changes of Er,Cr:YSGG-Laser Irradiated Implants In Vitro. Int. J. Periodont. Restor. Dent. 2017, 37, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C. Titanium Implant Osseointegration Problems with Alternate Solutions Using Epoxy/Carbon-Fiber-Reinforced Composite. Metals (Basel) 2014, 4, 549–569. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lausmaa, J.; Kasemo, B.; Mattson, H. Surface spectroscopic chracterization of titanium implant materials. Appl. Surf. Sci. 1990, 44, 133–146. [Google Scholar] [CrossRef]
- Shibli, J.A.; Vitussi, T.R.; Garcia, R.V.; Zenóbio, E.G.; Ota-Tsuzuki, C.; Cassoni, A.; Piattelli, A.; d’Avila, S. Implant surface analysis and microbiologic evaluation of failed implants retrieved from smokers. J. Oral Implantol. 2007, 33, 232–238. [Google Scholar] [CrossRef]
- Berglundh, T.; Abrahamsson, I.; Albouy, J.P.; Lindhe, J. Bone healing at implants with a fluoride-modified surface: An experimental study in dogs. Clin. Oral Implants Res. 2007, 18, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Bolhari, B.; Ehsani, S.; Etemadi, A.; Shafaq, M.; Nosrat, A. Efficacy of Er,Cr:YSGG laser in removing smear layer and debris with two different output powers. Photomed. Laser Surg. 2014, 32, 527–532. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, R.; Ueno, T.; Migita, S.; Tsutsumi, Y.; Doi, H.; Ogawa, T.; Hanawa, T.; Wakabayashi, N. Hydrocarbon Deposition Attenuates Osteoblast Activity on Titanium. J. Dent. Res. 2014, 93, 698–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eick, S.; Meier, I.; Spoerlé, F.; Bender, P.; Aoki, A.; Izumi, Y.; Salvi, G.E.; Sculean, A. In Vitro-Activity of Er:YAG Laser in Comparison with other Treatment Modalities on Biofilm Ablation from Implant and Tooth Surfaces. PLoS ONE 2017, 12, e0171086. [Google Scholar] [CrossRef] [PubMed]
- Mish, C.E. Dental Implant Prosthetics, 2nd ed.; Churchill Livingstone; Elsevier: Amsterdam, The Netherlands, 2014. [Google Scholar]
- Heitz-Mayeld, L.J.A.; Salvi, G.E.; Mombelli, A.; Faddy, M.; Lang, N.P. Anti-infective surgical therapy of peri-implantitis. A 12-month prospective clinical study. Clin. Oral Implants Res. 2012, 23, 205–210. [Google Scholar] [CrossRef] [PubMed]
- Lang, N.P.; Wilson, T.G.; Corbet, E.F. Biological complications with dental implants: Their prevention, diagnosis and treatment Note. Clin. Oral Implants Res. 2000, 11 (Suppl. 1), 146–155. [Google Scholar] [CrossRef] [PubMed]
- Meffert, R.M. How to treat ailing and failing implants. Implant Dent. 1992, 1, 25–26. [Google Scholar] [CrossRef] [PubMed]
- Mombelli, A.; Feloutzis, A.; Bragger, U.; Lang, N.P. Treatment of peri-implantitis by local delivery of tetracycline. Clinical, microbiological and radiological results. Clin. Oral Implants Res. 2001, 12, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Roos-Jansaker, A.M.; Claffey, N. Non-surgical treatment of peri-implant mucositis and peri-implantitis: A literature review. J. Clin. Periodontol. 2008, 35 (Suppl. 8), 305–315. [Google Scholar] [CrossRef] [PubMed]
- Schenk, G.; Flemmig, T.F.; Betz, T.; Reuther, J.; Klaiber, B. Controlled local delivery of tetracycline HCl in the treatment of periimplant mucosal hyperplasia and mucositis. A controlled case series. Clin. Oral Implants Res. 1997, 8, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Talreja, P.S.; Gayathri, G.V.; Mehta, D.S. Treatment of an early failing implant by guided bone regeneration using resorbable collagen membrane and bioactive glass. J. Indian Soc. Periodontol. 2013, 17, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Weinlaender, M.; Kenney, E.B.; Lekovic, V.; Beumer, J., 3rd; Moy, P.K.; Lewis, S. Histomorphometry of bone apposition around three types of endosseous dental implants. Int. J. Oral Maxillofac. Implants 1992, 7, 491–496. [Google Scholar] [PubMed]
- Yamamoto, A.; Tanabe, T. Treatment of peri-implantitis around TiUnite-surface implants using Er:YAG laser microexplosions. Int. J. Periodont. Restor. Dent. 2013, 33, 21–30. [Google Scholar] [CrossRef]
- Zablotsky, M.H. Chemotherapeutics in implant dentistry. Implant Dent. 1993, 2, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Dmytiyk, J.J.; Fox, S.C.; Moriarty, J.D. The Effects of Scaling Titanium Implant Surfaces With Metal and Plastic Instruments on Cell Attachment. J. Periodontol. 1990, 61, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Fox, S.C.; Moriarty, J.D.; Kusy, R.P. The effects of scaling a titanium implant surface with metal and plastic instruments: An in vitro study. J. Periodontol. 1990, 61, 485–490. [Google Scholar] [CrossRef] [PubMed]
- Größner-Schreiber, B.; Herzog, M.; Hedderich, J.; Dück, A.; Hannig, M.; Griepentrog, M. Focal adhesion contact formation by fibroblasts cultured on surface-modified dental implants: An in vitro study. Clin. Oral Implants Res. 2006, 17, 736–745. [Google Scholar] [CrossRef] [PubMed]
- London, R.M.; Roberts, F.A.; Baker, D.A.; Rohrer, M.D.; O’Neal, R.B. Histologic comparison of a thermal dual-etched implant surface to machined, TPS, and HA surfaces: Bone contact in vivo in rabbits. Int. J. Oral Maxillofac. Implants 2002, 17, 369–376. [Google Scholar] [PubMed]
- Park, J.Y.; Davies, J.E. Red blood cell and platelet interactions with titanium implant surfaces. Clin. Oral Implants Res. 2000, 11, 530–539. [Google Scholar] [CrossRef] [PubMed]
- Zabtotsky, M.H.; Diedrich, D.L.P.; Meffert, R.M. Detoxification of endotoxin-contaminated titanium and hydroxyapatite-coated surfaces utilizing various chemotherapeutic and mechanical modalities. Implant Dent. 1992, 1, 154–158. [Google Scholar] [CrossRef]
- Alshehri, F.A. The role of lasers in the treatment of peri-implant diseases: A review. Saudi Dent. J. 2016, 28, 103–108. [Google Scholar] [CrossRef] [PubMed]
- Romanos, G.E. Current concepts in the use of lasers in periodontal and implant dentistry. J. Indian Soc. Periodontol. 2015, 19, 490–494. [Google Scholar] [CrossRef] [PubMed]
- Kamel, M.S.; Khosa, A.; Tawse-Smith, A.; Leichter, J. The use of laser therapy for dental implant surface decontamination: A narrative review of in vitro studies. Lasers Med. Sci. 2014, 29, 1977–1985. [Google Scholar] [CrossRef] [PubMed]
- Kreisler, M.; Gatz, H.; Duschner, H.; Dâhoedt, B. Effect of Nd:YAG, Ho:YAG, Er:YAG, CO2, and GaAlAs irradiation on surface properties of endosseous dental implants. Int. J. Oral Maxillofac. Implants 2002, 17, 202–211. [Google Scholar] [PubMed]
- Romanos, G.E.; Weitz, D. Therapy of peri-implant diseases. Where is the evidence? J. Evid. Based Dent. Pract. 2012, 12, 204–208. [Google Scholar] [CrossRef]
- Matsuyama, T.; Aoki, A.; Oda, S.; Yoneyama, T.; Ishikawa, I. Effects of the Er:YAG laser irradiation on titanium implant materials and contaminated implant abutment surfaces. J. Clin. Laser Med. Surg. 2003, 21, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Valderrama, P.; Blansett, J.; Gonzalez, M.; Cantu, M.; Wilson, T. Detoxification of Implant Surfaces Affected by Peri-Implant Disease: An Overview of Non-surgical Methods. Open Dent. J. 2014, 8, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Stubinger, S.; Etter, C.; Miskiewicz, M.; Homann, F.; Saldamli, B.; Wieland, M. Surface alterations of polished and sandblasted and acid-etched titanium implants after Er:YAG, carbon dioxide, and diode laser irradiation. Int. J. Oral Maxillofac. ImplantsS 2010, 25, 104–111. [Google Scholar]
- Shin, S.I.; Lee, E.K.; Kim, J.H.; Lee, J.H.; Kim, S.H.; Kwon, Y.H.; Herr, Y.; Chung, J.H. The effect of Er:YAG laser irradiation on hydroxyapatite-coated implants and fluoride-modified TiO2-blasted implant surfaces: A microstructural analysis. Lasers Med. Sci. 2013, 28, 823–831. [Google Scholar] [CrossRef] [PubMed]
- Quaranta, A.; Maida, C.; Scrascia, A.; Campus, G.; Quaranta, M. Er:YAG Laser application on titanium implant surfaces contaminated by Porphyromonas gingivalis: An histomorphometric evaluation. Minerva Stomatol. 2009, 58, 317–330. [Google Scholar] [PubMed]
- Romanos, G.E. Treatment of peri-implant lesions using different laser systems. J. Oral Laser 2002, 2, 75–81. [Google Scholar]
- Ayobian-Markazi, N.; KFarimi, M.; Safar-Hajhosseini, A. Effects of Er: YAG laser irradiation on wettability, surface roughness, and biocompatibility of SLA titanium surfaces: An in vitro study. Lasers Med. Sci. 2015, 30, 561–566. [Google Scholar] [CrossRef] [PubMed]
- Dostalova, T.; Jelinkova, H. Lasers in dentistry: Overview and perspectives. Photomed. Laser Surg. 2013, 31, 147–149. [Google Scholar] [CrossRef] [PubMed]
- Hibst, R. Lasers for Caries Removal and Cavity Preparation: State of the Art and Future Directions. J. Oral Laser Appl. 2002, 2, 203–211. [Google Scholar]
- Licata, M.E.; Albanese, A.; Campisi, G.; Geraci, D.M.; Russo, R.; Gallina, G. Effectiveness of a new method of disinfecting the root canal, using Er, Cr:YSGG laser to kill Enterococcus faecalis in an infected tooth model. Lasers Med. Sci. 2015, 30, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Luong, E.; Shayegan, A. Assessment of microleakage of class V restored by resin composite and resin-modified glass ionomer and pit and fissure resin-based sealants following Er:YAG laser conditioning and acid etching: In vitro study. Clin. Cosmet. Investig. Dent. 2018, 10, 83–92. [Google Scholar] [CrossRef] [PubMed]
- Kotsakis, G.A.; Konstantinidis, I.; Karoussis, I.K.; Ma, X.; Chu, H. Systematic review and meta-analysis of the effect of various laser wavelengths in the treatment of peri-implantitis. J. Periodontol. 2014, 85, 1203–1213. [Google Scholar] [CrossRef] [PubMed]
- Galli, C.; Macaluso, G.M.; Elezi, E.; Ravanetti, F.; Cacchioli, A.; Gualini, G.; Passeri, G. The effects of Er:YAG laser treatment on titanium surface profile and osteoblastic cell activity: An in vitro study. J. Periodontol. 2011, 82, 1169–1177. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, F.; Rothamel, D.; Becker, J.; Schwarz Monatsschr, Z. Influence of an Er:YAG laser on the surface structure of titanium implants. Schweiz Monatsschr. Zahnmed. 2003, 113, 660–671. [Google Scholar] [PubMed]
- Sennhenn-Kirchner, S.; Schwarz, P.; Schliephake, H.; Konietschke, F.; Brunner, E.; Borg-von Zepelin, M. Decontamination efficacy of erbium:yttrium-aluminium-garnet and diode laser light on oral Candida albicans isolates of a 5-day in vitro biofilm model. Lasers Med. Sci. 2009, 24, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Herr, Y.; Chung, J.H.; Shin, S.I.; Kwon, Y.H. The effect of erbium-doped: Yttrium, aluminium and garnet laser irradiation on the surface microstructure and roughness of double acid-etched implants. J. Periodont. Implant Sci. 2011, 41, 234–241. [Google Scholar] [CrossRef] [PubMed]
- Matys, J.; Dominiak, M.; Flieger, R. Energy and Power Density: A Key Factor in Lasers Studies. J. Clin. Diagn. Res. 2015, 9, ZL01–ZL02. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, Y.; Aoki, A.; Mizutani, K.; Takeuchi, Y.; Ichinose, S.; Takasaki, A.A.; Schwarz, F.; Izumi, Y. Optimal Er:YAG laser irradiation parameters for debridement of microstructured fixture surfaces of titanium dental implants. Lasers Med. Sci. 2013, 28, 1057–1068. [Google Scholar] [CrossRef] [PubMed]
- Visuri, S.R.; Walsh, J.T., Jr.; Wigdor, H.A. Erbium laser ablation of dental hard tissue: Effect of water cooling. Lasers Surg. Med. 1996, 18, 294–300. [Google Scholar] [CrossRef]
- Park, S.Y.; Kim, K.H.; Shin, S.Y.; Koo, K.T.; Lee, Y.M.; Chung, C.P.; Seol, Y.J. Decontamination methods using a dental water jet and dental floss for microthreaded implant fixtures in regenerative periimplantitis treatment. Implant Dent. 2015, 24, 307–316. [Google Scholar] [CrossRef] [PubMed]
- Lukac, M.; Marincek, M.; Grad, L. Super VSP Er:YAG Pulses for Fast and Precise Cavity Preparation. J. Oral Laser Appl. 2004, 4, 171–173. [Google Scholar]
- Perhavec, T.; Diaci, J. Comparison of Er:YAG and Er,Cr:YSGG dental lasers. J. Oral Laser Appl. 2008, 8, 87–94. [Google Scholar]
- Folwaczny, M.; Thiele, L.; Mehl, A.; Hickel, R. The effect of working tip angulation on root substance removal using Er:YAG laser radiation: An in vitro study. J. Clin. Periodontol. 2001, 28, 220–226. [Google Scholar] [CrossRef] [PubMed]
- Hauser-Gerspach, I.; Mauth, C.; Waltimo, T.; Meyer, J.; Stübinger, S. Effects of Er:YAG laser on bacteria associated with titanium surfaces and cellular response in vitro. Lasers Med. Sci. 2014, 29, 1329–1337. [Google Scholar] [CrossRef] [PubMed]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups | Surface |
|---|---|
| A (sterile) (n = 30) | Control: No contamination/No irradiation |
| B (n = 60) | Contaminated implants |
| LX1 (n = 30) | Decontamination by irradiation: one passage |
| LX3 (n = 30) | Decontamination by irradiation: multiple passages |
| Groups | Contaminated | L X1 50 mJ; 30 Hz | L X3 50 mJ; 30 Hz | Sterile |
|---|---|---|---|---|
| Number of values | 230 | 235 | 235 | 235 |
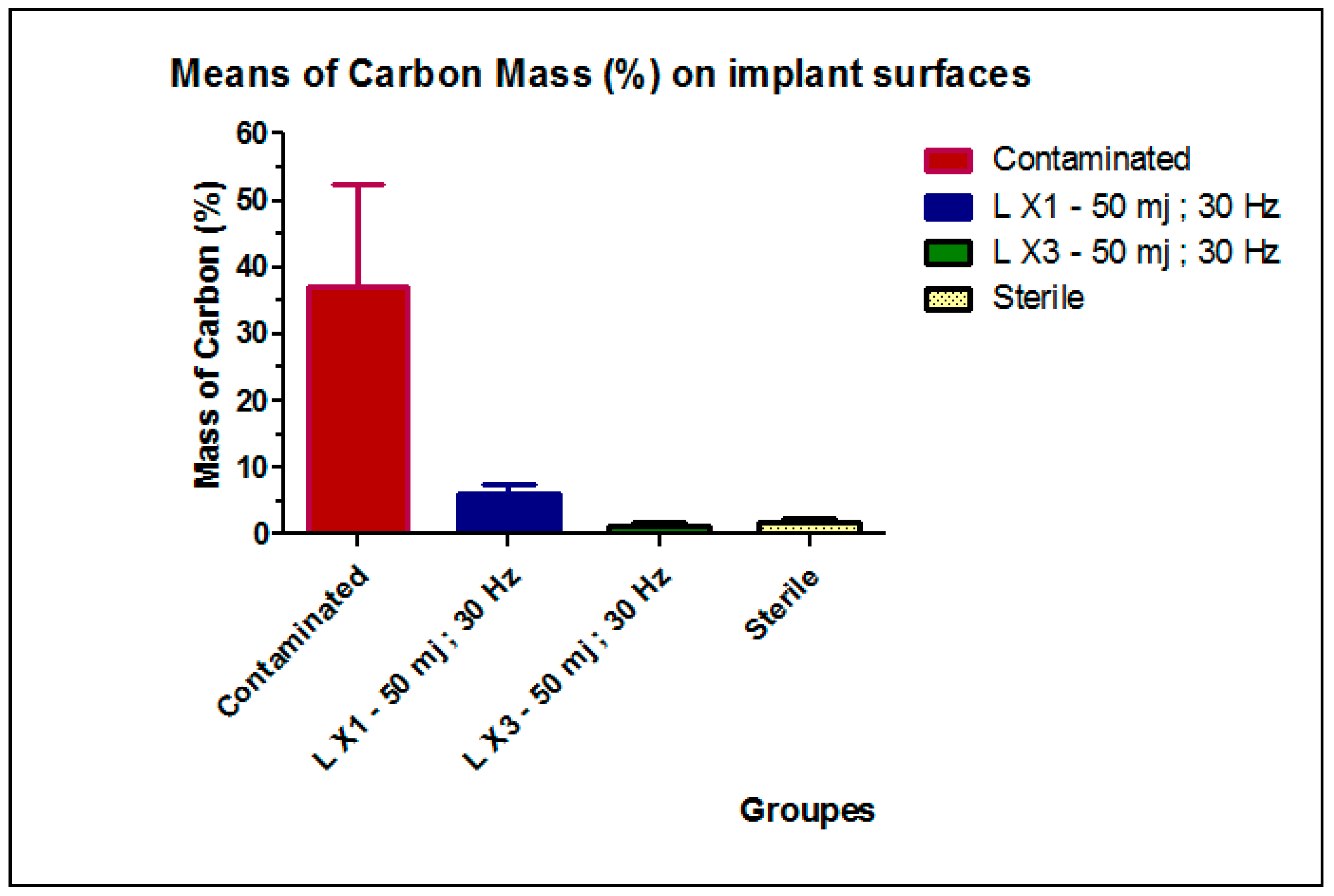
| Mean (SD) | 37.18 (15.31) a | 6.17 (1.45) b | 1.43 (0.41) c | 1.86 (0.68) c |
| 95% CI | 34.24–40.11 | 5.06–7.28 | 0.92–1.93 | 1.64–2.08 |
| p Value Summary | *** | |||
|---|---|---|---|---|
| Do the variances differ signif. (p < 0.05) | Yes | |||
| ANOVA Table | SS | Df | MS | |
| Treatment (between columns) | 65,790 | 3 | 21,930 | |
| Residual (within columns) | 3129 | 116 | 26.97 | |
| Total | 68,920 | 119 | ||
| Newman-Keuls Multiple Comparison Test | Mean Diff. | Q | Significant? p < 0.05? | Summary |
| L X3-50 mj; 30 Hz vs. Contaminated | −55.82 | 58.87 | Yes | *** |
| L X3-50 mj; 30 Hz vs. L X1-50 mj; 30 Hz | −5.213 | 5.498 | Yes | *** |
| L X3-50 mj; 30 Hz vs. Sterile | −0.6283 | 0.6627 | No | ns |
| Sterile vs. Contaminated | −55.19 | 58.21 | Yes | *** |
| L X1-50 mj; 30 Hz vs. Sterile | −4.585 | 4.836 | Yes | *** |
| L X1-50 mj; 30 Hz vs. Contaminated | −50.61 | 53.37 | Yes | *** |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nejem Wakim, R.; Namour, M.; Nguyen, H.V.; Peremans, A.; Zeinoun, T.; Vanheusden, A.; Rompen, E.; Nammour, S. Decontamination of Dental Implant Surfaces by the Er:YAG Laser Beam: A Comparative in Vitro Study of Various Protocols. Dent. J. 2018, 6, 66. https://0-doi-org.brum.beds.ac.uk/10.3390/dj6040066
Nejem Wakim R, Namour M, Nguyen HV, Peremans A, Zeinoun T, Vanheusden A, Rompen E, Nammour S. Decontamination of Dental Implant Surfaces by the Er:YAG Laser Beam: A Comparative in Vitro Study of Various Protocols. Dentistry Journal. 2018; 6(4):66. https://0-doi-org.brum.beds.ac.uk/10.3390/dj6040066
Chicago/Turabian StyleNejem Wakim, Rima, Melanie Namour, Hoang Viet Nguyen, Andre Peremans, Toni Zeinoun, Alain Vanheusden, Eric Rompen, and Samir Nammour. 2018. "Decontamination of Dental Implant Surfaces by the Er:YAG Laser Beam: A Comparative in Vitro Study of Various Protocols" Dentistry Journal 6, no. 4: 66. https://0-doi-org.brum.beds.ac.uk/10.3390/dj6040066