Integrated Digital and Conventional Treatment Workflow in Guided Complete Mouth Implant Rehabilitation: A Clinical Case Report


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Clinical Implications
Abstract
1. Introduction
2. Case Presentation
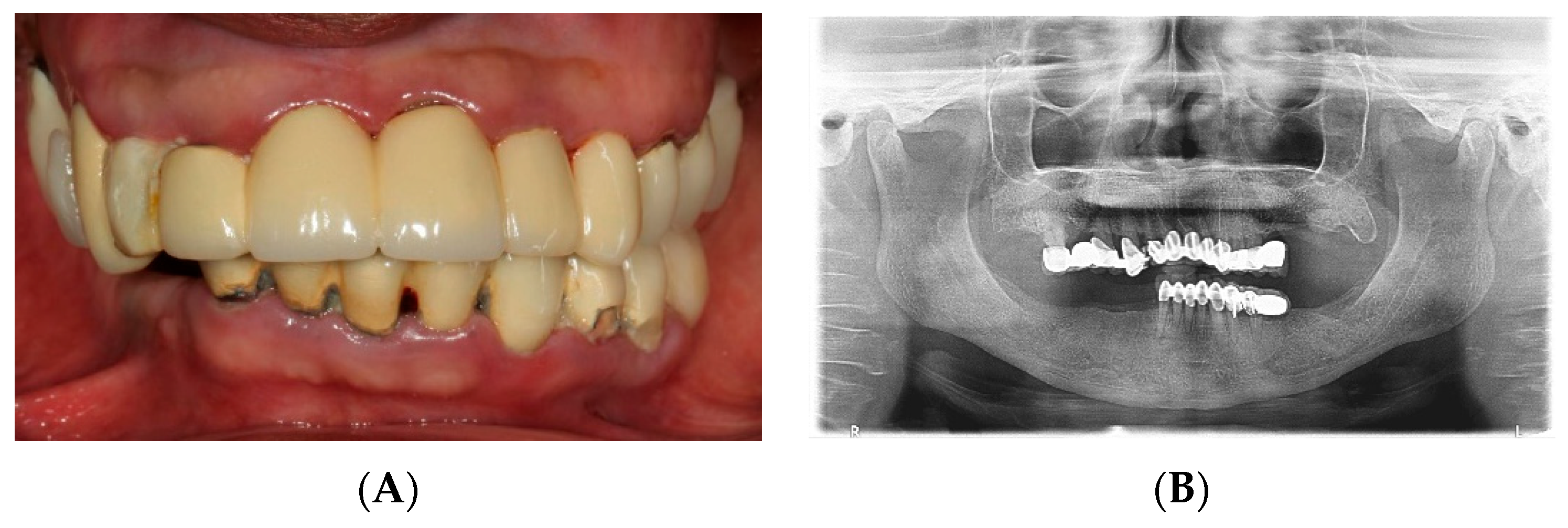
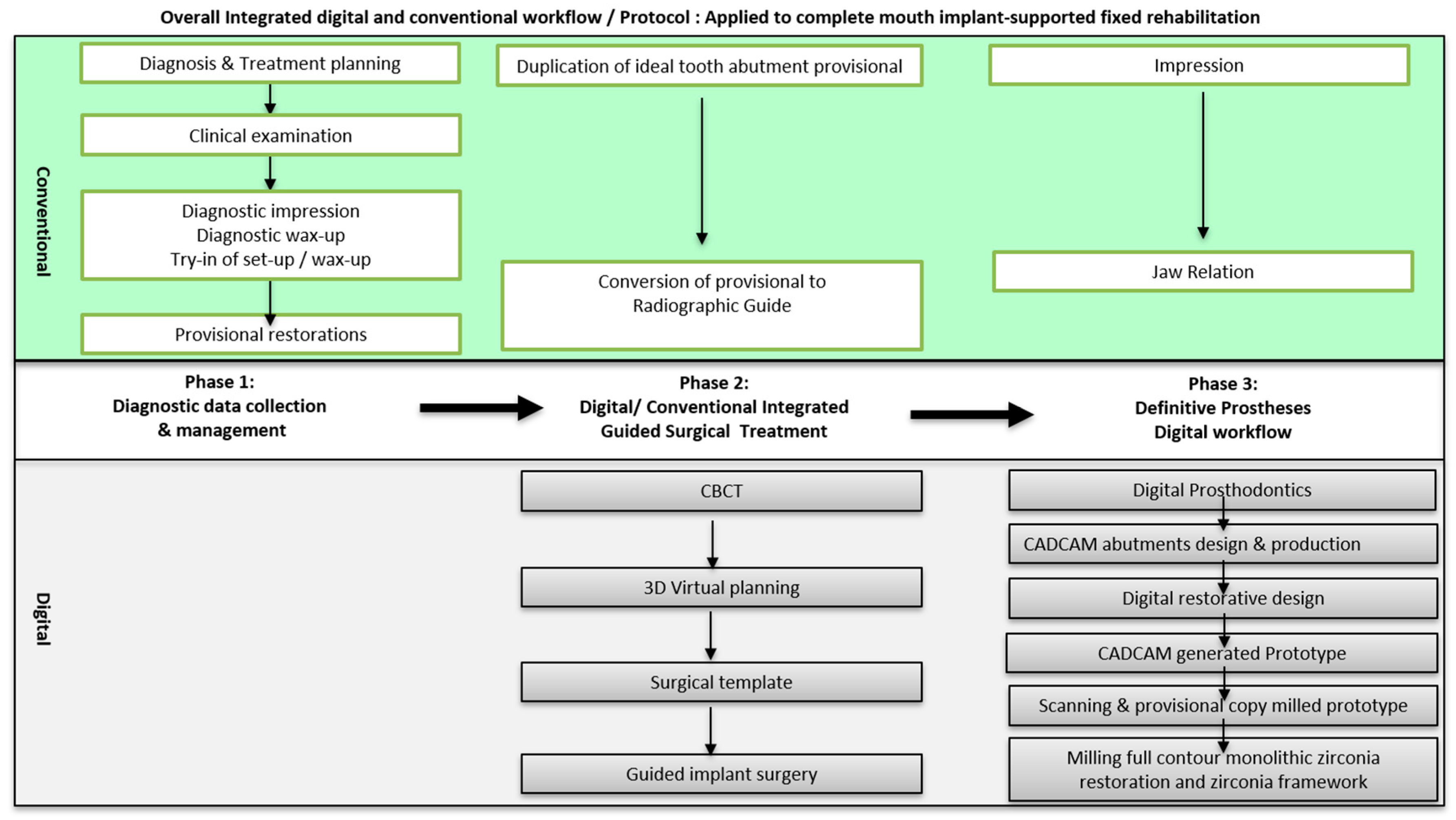
2.1. Diagnostic Phase
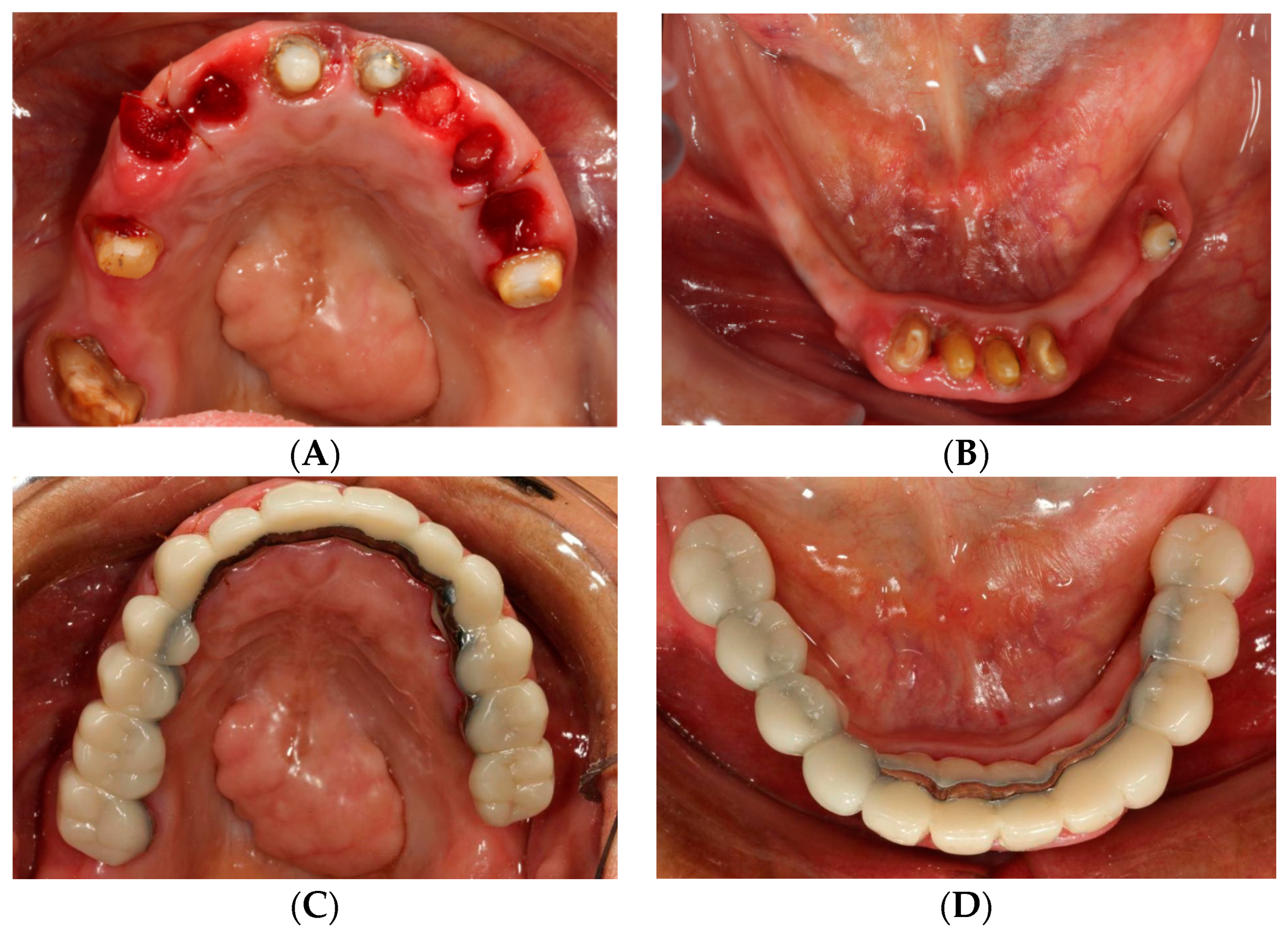
2.2. Foundational Phase: Elimination of Active Disease, Extraction and Fixed Provisional Prosthesis
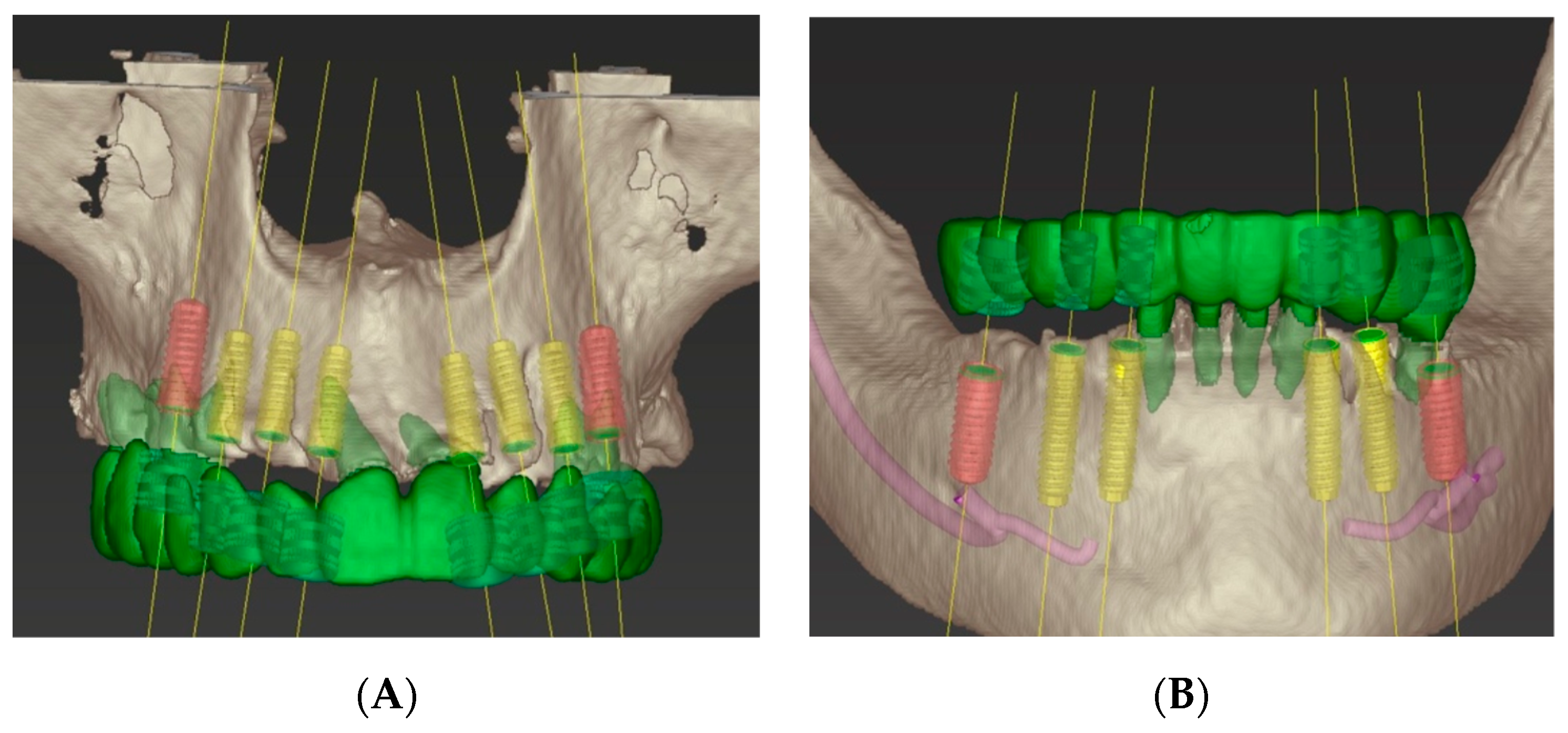
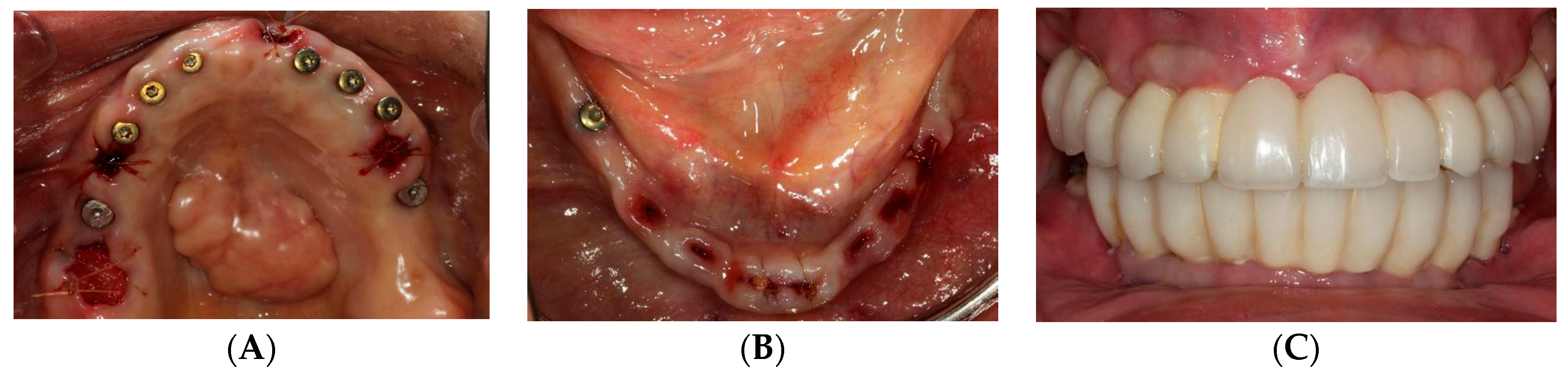
2.3. Surgical Phase: Virtual Planning of Implant Placement and Computer Guided Surgery
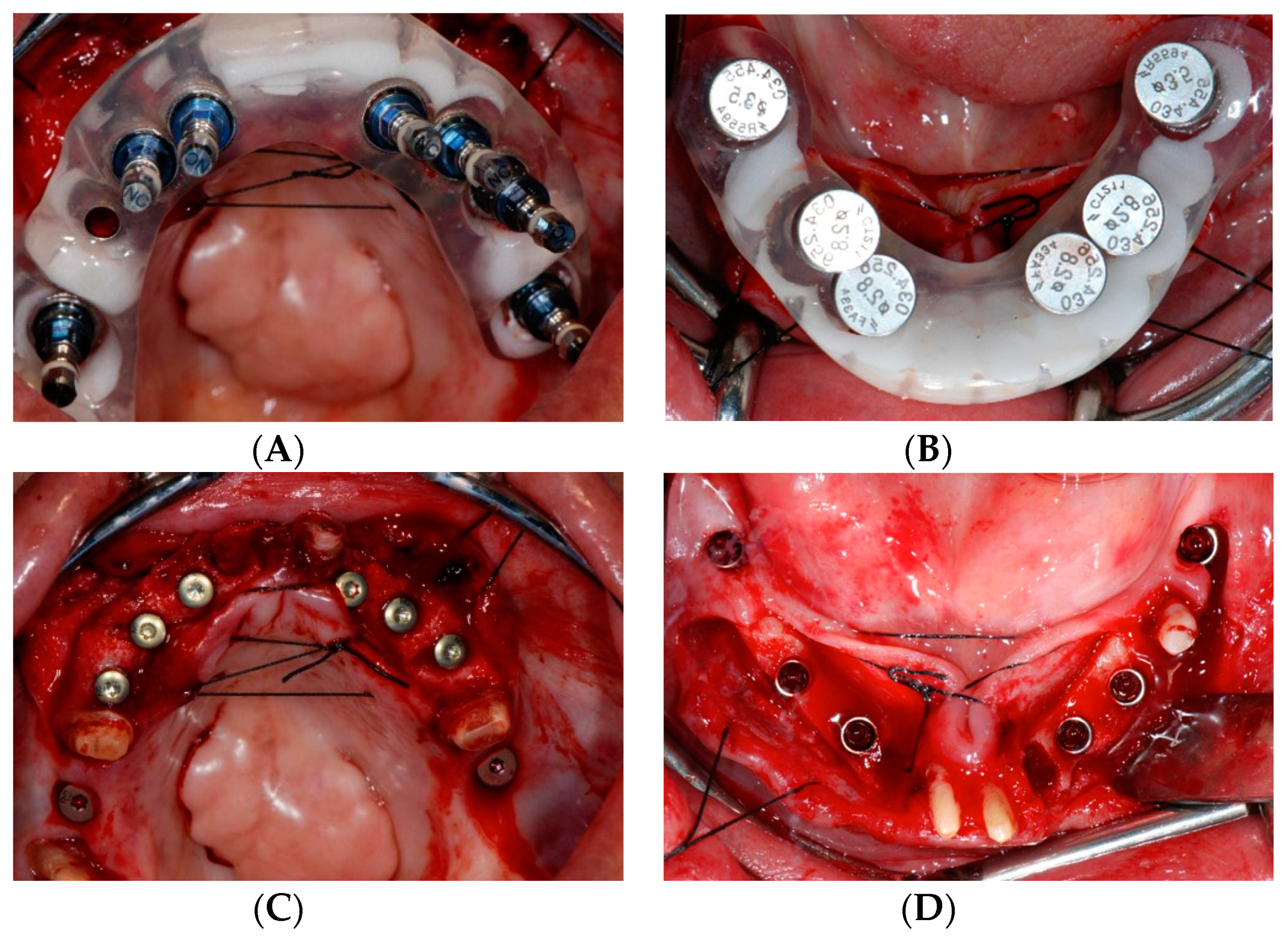
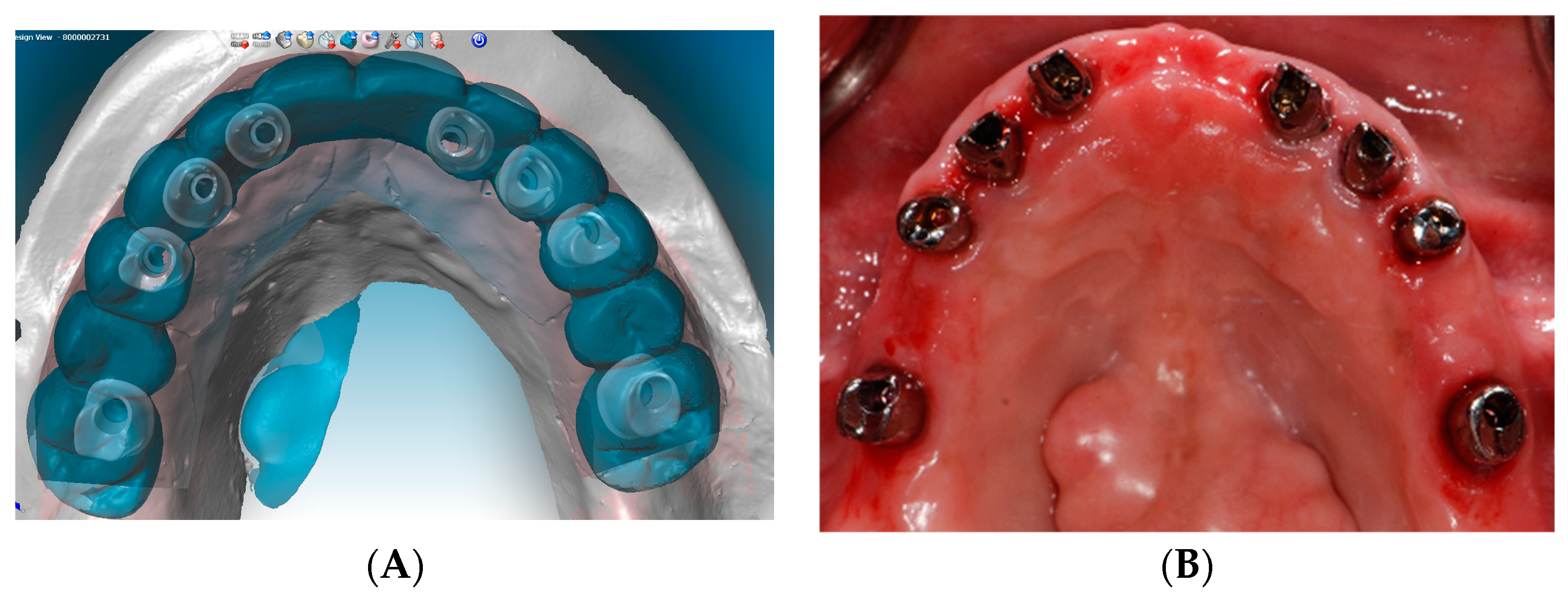
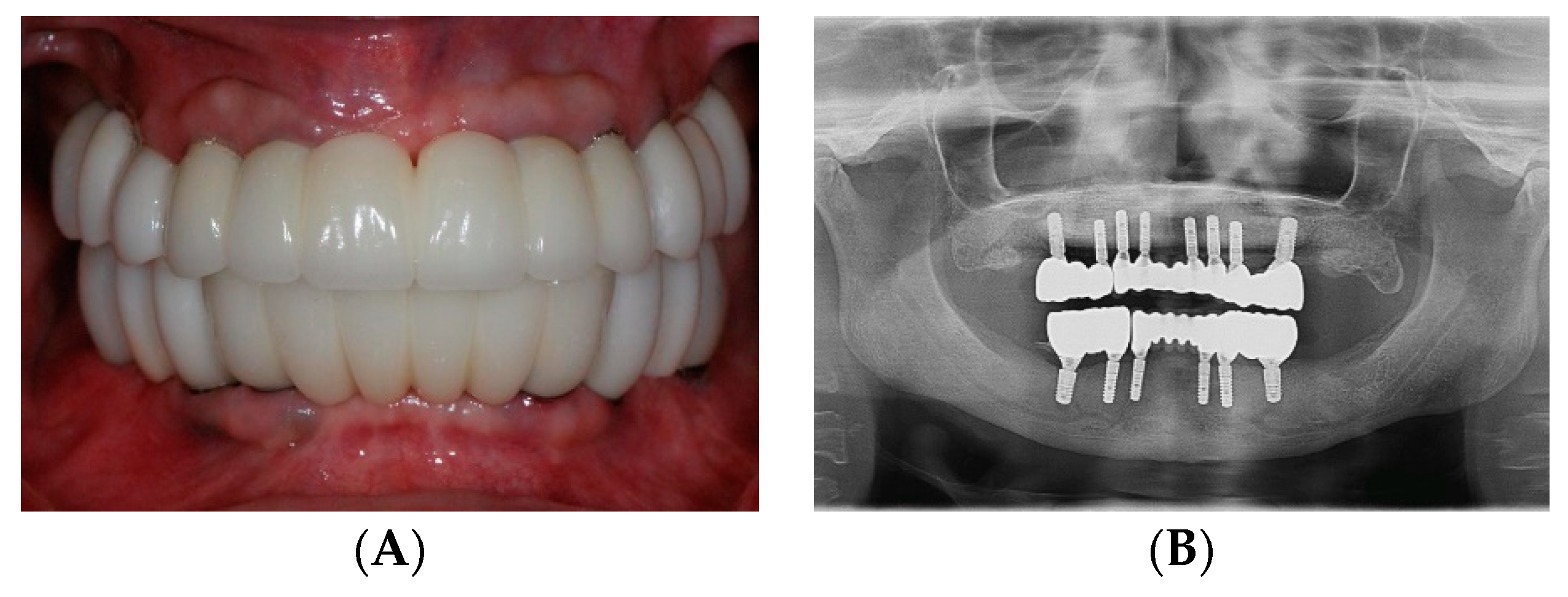
2.4. Restorative Phase: Second Strategic Extraction and Conversion of Provisional Prostheses with Integrated Digital Workflow
3. Discussion
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Adell, R.; Eriksson, B.; Lekholm, U.; Branemark, P.I.; Jemt, T. Long-term follow-up study of osseointegrated implants in the treatment of totally edentulous jaws. Int. J. Oral Maxillofac. Implants 1990, 5, 347–359. [Google Scholar] [PubMed]
- Zarb, G.A.; Schmitt, A. The longitudinal clinical effectiveness of osseointegrated dental implants: The Toronto study. Part III: Problems and complications encountered. J. Prosthet. Dent. 1990, 64, 185–194. [Google Scholar] [CrossRef]
- Zarb, G.A.; Schmitt, A. The longitudinal clinical effectiveness of osseointegrated dental implants: The Toronto Study. Part II: The prosthetic results. J. Prosthet. Dent. 1990, 64, 53–61. [Google Scholar] [CrossRef]
- Zarb, G.A.; Schmitt, A. The longitudinal clinical effectiveness of osseointegrated dental implants: The Toronto study. Part I: Surgical results. J. Prosthet. Dent. 1990, 63, 451–457. [Google Scholar] [CrossRef]
- Schwarz, M.S.; Rothman, S.L.; Rhodes, M.L.; Chafetz, N. Computed tomography: Part II. Preoperative assessment of the maxilla for endosseous implant surgery. Int. J. Oral Maxillofac. Implants 1987, 2, 143–148. [Google Scholar]
- Schwarz, M.S.; Rothman, S.L.; Rhodes, M.L.; Chafetz, N. Computed tomography: Part, I. Preoperative assessment of the mandible for endosseous implant surgery. Int. J. Oral Maxillofac. Implants 1987, 2, 137–141. [Google Scholar]
- Bover-Ramos, F.; Vina-Almunia, J.; Cervera-Ballester, J.; Penarrocha-Diago, M.; Garcia-Mira, B. Accuracy of Implant Placement with Computer-Guided Surgery: A Systematic Review and Meta-Analysis Comparing Cadaver, Clinical, and in Vitro Studies. Int. J. Oral Maxillofac. Implants 2018, 33, 101–115. [Google Scholar] [CrossRef]
- Cristache, C.M.; Gurbanescu, S. Accuracy Evaluation of a Stereolithographic Surgical Template for Dental Implant Insertion Using 3D Superimposition Protocol. Int. J. Dent. 2017, 2017, 4292081. [Google Scholar] [CrossRef]
- van Steenberghe, D.; Glauser, R.; Blomback, U.; Andersson, M.; Schutyser, F.; Pettersson, A.; Wendelhag, I. A computed tomographic scan-derived customized surgical template and fixed prosthesis for flapless surgery and immediate loading of implants in fully edentulous maxillae: A prospective multicenter study. Clin. Implant. Dent. Relat Res. 2005, 7, S111–S120. [Google Scholar] [CrossRef]
- Weiss, R., 2nd; Read-Fuller, A. Cone Beam Computed Tomography in Oral and Maxillofacial Surgery: An Evidence-Based Review. Dent. J. 2019, 7, 52. [Google Scholar] [CrossRef]
- Verstreken, K.; Van Cleynenbreugel, J.; Marchal, G.; Naert, I.; Suetens, P.; van Steenberghe, D. Computer-assisted planning of oral implant surgery: A three-dimensional approach. Int. J. Oral Maxillofac. Implants 1996, 11, 806–810. [Google Scholar] [PubMed]
- Vercruyssen, M.; Laleman, I.; Jacobs, R.; Quirynen, M. Computer-supported implant planning and guided surgery: A narrative review. Clin. Oral Implants Res. 2015, 26, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Schneider, D.; Marquardt, P.; Zwahlen, M.; Jung, R.E. A systematic review on the accuracy and the clinical outcome of computer-guided template-based implant dentistry. Clin. Oral Implants Res. 2009, 20, 73–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Haese, J.; Ackhurst, J.; Wismeijer, D.; De Bruyn, H.; Tahmaseb, A. Current state of the art of computer-guided implant surgery. Periodontol. 2000 2017, 73, 121–133. [Google Scholar] [CrossRef] [PubMed]
- Al Mortadi, N.; Eggbeer, D.; Lewis, J.; Williams, R.J. CAD/CAM/AM applications in the manufacture of dental appliances. Am. J. Orthod Dentofacial Orthop. 2012, 142, 727–733. [Google Scholar] [CrossRef] [PubMed]
- Davidowitz, G.; Kotick, P.G. The use of CAD/CAM in dentistry. Dent. Clin. N. Am. 2011, 55, 559–570. [Google Scholar] [CrossRef] [PubMed]
- Cordaro, L.; Torsello, F.; Ribeiro, C.A. Transition from a failing dentition to a removable implant-supported prosthesis: A staged approach. Quintessence Int. 2010, 41, 371–378. [Google Scholar]
- Drew, H.J.; Alnassar, T.; Gluck, K.; Rynar, J.E. Considerations for a staged approach in implant dentistry. Quintessence Int. 2012, 43, 29–36. [Google Scholar]
- el Attar, M.S.; el Shazly, D.; Osman, S.; el Domiati, S.; Salloum, M.G. Study of the effect of using mini-transitional implants as temporary abutments in implant overdenture cases. Implant Dent. 1999, 8, 152–158. [Google Scholar] [CrossRef]
- Gallucci, G.O.; Finelle, G.; Papadimitriou, D.E.; Lee, S.J. Innovative approach to computer-guided surgery and fixed provisionalization assisted by screw-retained transitional implants. Int. J. Oral Maxillofac. Implants 2015, 30, 403–410. [Google Scholar] [CrossRef]
- Jivraj, S.; Reshad, M.; Chee, W.W. Transitioning patients from teeth to implants utilizing fixed restorations. J. Calif. Dent. Assoc. 2008, 36, 599–606. [Google Scholar] [PubMed]
- Petrungaro, P.S.; Windmiller, N. Using transitional implants during the healing phase of implant reconstruction. Gen. Dent. 2001, 49, 46–51. [Google Scholar] [PubMed]
- Cordaro, L.; Torsello, F.; Ercoli, C.; Gallucci, G. Transition from failing dentition to a fixed implant-supported restoration: A staged approach. Int. J. Periodontics Restorative Dent. 2007, 27, 481–487. [Google Scholar] [PubMed]
- Greenstein, G.; Cavallaro, J., Jr. Serial extraction protocol: Transitioning a hopeless dentition to a full-arch reconstruction. Compend. Contin. Educ. Dent. 2008, 29, 526–534. [Google Scholar] [PubMed]
- Wittneben, J.G.; Avdic, M.; Wright, R.F.; Radics, A.; Gallucci, G.O.; Weber, H.P. Fixed mandibular and maxillary implant rehabilitation in a fully edentulous patient: A case report. Int. J. Periodontics Restorative Dent. 2009, 29, 615–623. [Google Scholar]
- Allen, P.F.; McMillan, A.S. A review of the functional and psychosocial outcomes of edentulousness treated with complete replacement dentures. J. Can. Dent. Assoc. 2003, 69, 662. [Google Scholar]
- Cho, S.C.; Shetty, S.; Froum, S.; Elian, N.; Tarnow, D. Fixed and removable provisional options for patients undergoing implant treatment. Compend. Contin. Educ. Dent. 2007, 28, 604–608. [Google Scholar]
- Lee, S.J.; Gallucci, G.O. Digital vs. conventional implant impressions: Efficiency outcomes. Clin. Oral Implants Res. 2013, 24, 111–115. [Google Scholar] [CrossRef]
- Bozini, T.; Petridis, H.; Garefis, K.; Garefis, P. A meta-analysis of prosthodontic complication rates of implant-supported fixed dental prostheses in edentulous patients after an observation period of at least 5 years. Int. J. Oral Maxillofac. Implants 2011, 26, 304–318. [Google Scholar]
- Stawarczyk, B.; Ozcan, M.; Schmutz, F.; Trottmann, A.; Roos, M.; Hammerle, C.H. Two-body wear of monolithic, veneered and glazed zirconia and their corresponding enamel antagonists. Acta Odontol. Scand. 2013, 71, 102–112. [Google Scholar] [CrossRef]
- Zhang, Y.; Lee, J.J.; Srikanth, R.; Lawn, B.R. Edge chipping and flexural resistance of monolithic ceramics. Dent. Mater. 2013, 29, 1201–1208. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Preis, V.; Weiser, F.; Handel, G.; Rosentritt, M. Wear performance of monolithic dental ceramics with different surface treatments. Quintessence Int. 2013, 44, 393–405. [Google Scholar] [PubMed]
- Sripetchdanond, J.; Leevailoj, C. Wear of human enamel opposing monolithic zirconia, glass ceramic, and composite resin: An in vitro study. J. Prosthet. Dent. 2014, 112, 1141–1150. [Google Scholar] [CrossRef] [PubMed]
- Karakoca, S.; Yilmaz, H. Influence of surface treatments on surface roughness, phase transformation, and biaxial flexural strength of Y-TZP ceramics. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 91, 930–937. [Google Scholar] [CrossRef] [PubMed]
- Preis, V.; Schmalzbauer, M.; Bougeard, D.; Schneider-Feyrer, S.; Rosentritt, M. Surface properties of monolithic zirconia after dental adjustment treatments and in vitro wear simulation. J. Dent. 2015, 43, 133–139. [Google Scholar] [CrossRef]










© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, J.D.; Jung, S.; Wang, C.-W.; Lee, S.J. Integrated Digital and Conventional Treatment Workflow in Guided Complete Mouth Implant Rehabilitation: A Clinical Case Report. Dent. J. 2019, 7, 100. https://0-doi-org.brum.beds.ac.uk/10.3390/dj7040100
Lee JD, Jung S, Wang C-W, Lee SJ. Integrated Digital and Conventional Treatment Workflow in Guided Complete Mouth Implant Rehabilitation: A Clinical Case Report. Dentistry Journal. 2019; 7(4):100. https://0-doi-org.brum.beds.ac.uk/10.3390/dj7040100
Chicago/Turabian StyleLee, Jason D., Soomin Jung, Chin-Wei Wang, and Sang J. Lee. 2019. "Integrated Digital and Conventional Treatment Workflow in Guided Complete Mouth Implant Rehabilitation: A Clinical Case Report" Dentistry Journal 7, no. 4: 100. https://0-doi-org.brum.beds.ac.uk/10.3390/dj7040100