Porphyromonas gingivalis, Periodontal and Systemic Implications: A Systematic Review

 ,
,  ,
,  , ,
, , 
Abstract
:1. Introduction
1.1. Rationale
- Host susceptibility;
- Environmental factors;
- Behavioral factors.
1.2. Objectives
2. Materials and Methods
2.1. Protocol and Registration
2.2. Eligibility Criteria
- Inclusion Criteria:
- ○
- Human studies;
- ○
- Information about P. gingivalis and periodontal implication;
- ○
- Information about P. gingivalis and systemic disease;
- ○
- In vitro and in vivo studies about P. gingivalis;
- ○
- Last 10 years studies.
- Exclusion Criteria:
- ○
- In silica studies;
- ○
- Not on human studies;
- ○
- Not in English;
- ○
- Not accessible title or abstract;
- ○
- Not enough information about main question of review.
2.3. Information Sources
2.4. Search
- Are patients who have periodontitis an increased for systemic health status compared with patients without periodontitis?
- Does P. gingivalis influence systemic health in patients who have periodontitis?
2.5. Study Selection
2.6. Data Collection Process
2.7. Data Items
- Summary of items (Table 1):
- ○
- Neurology;
- ○
- Cardiology;
- ○
- Immunology;
- ○
- Rheumatology;
- ○
- Diabetology;
- ○
- Oncology;
- ○
- Biology.
- Investigated data items on articles (Tables 2 and 3):
- ○
- Authors and year–article authors and year of publication (reference have been added);
- ○
- Item–article and authors evaluated items;
- ○
- Outcome–main results of the study;
- ○
- Medical disease–investigated medical disease.
2.8. Risk of Bias in Individual Studies
- Selection bias;
- Performance bias and detection bias;
- Attrition bias;
- Reporting bias;
- Examiner blinding, examiner calibration, standardized follow-up description, standardized residual graft measurement, and standardized radiographic assessment.
2.9. Summary Measures
2.10. Synthesis of Results
2.11. Risk of Bias across the Studies
2.12. Additional Analysis
3. Results
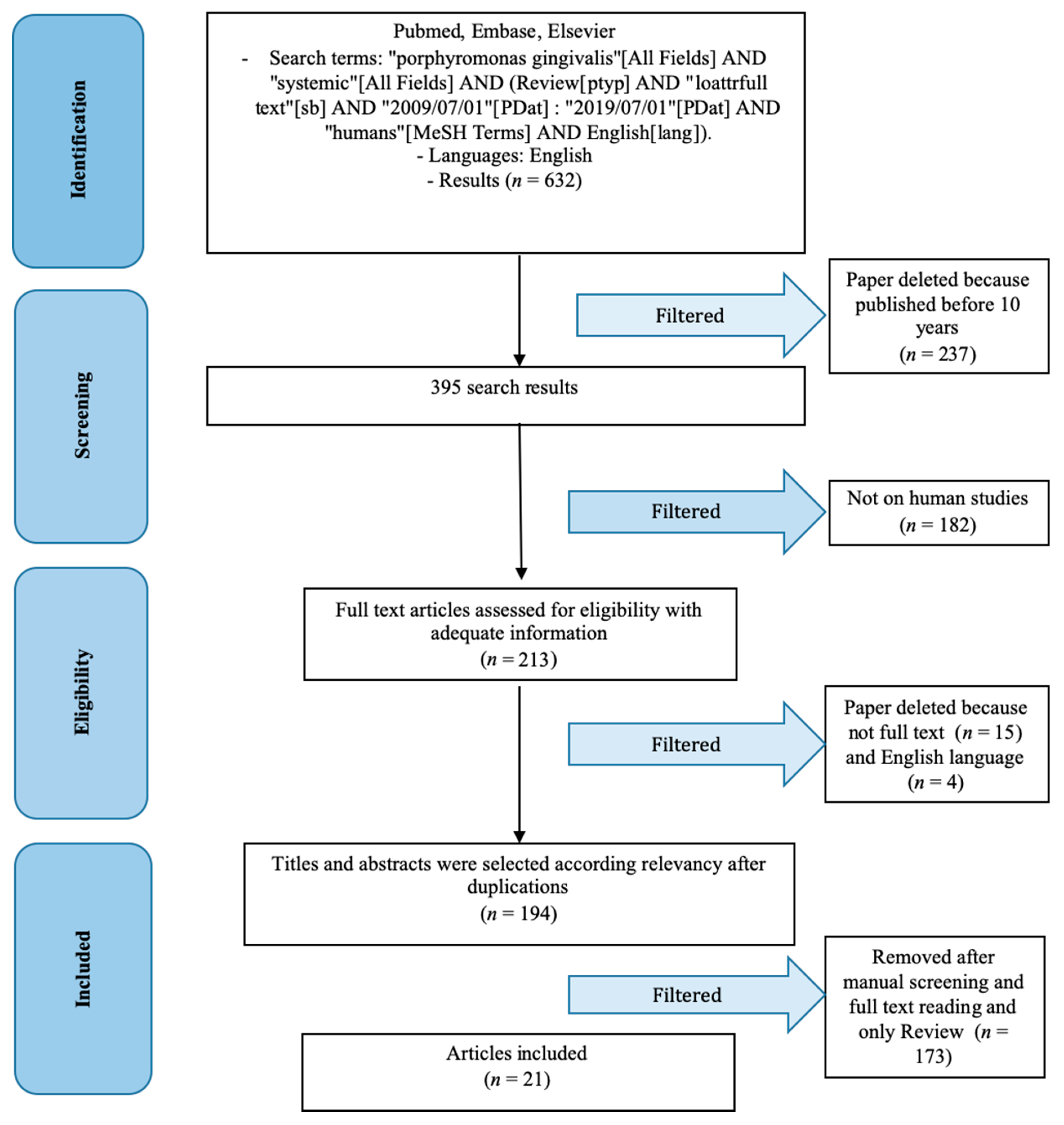
3.1. Study Selection
3.2. Study Characteristics and Results of Individual Studies
3.3. Synthesis of Results
3.4. Risk of Bias
3.5. Additional Analysis
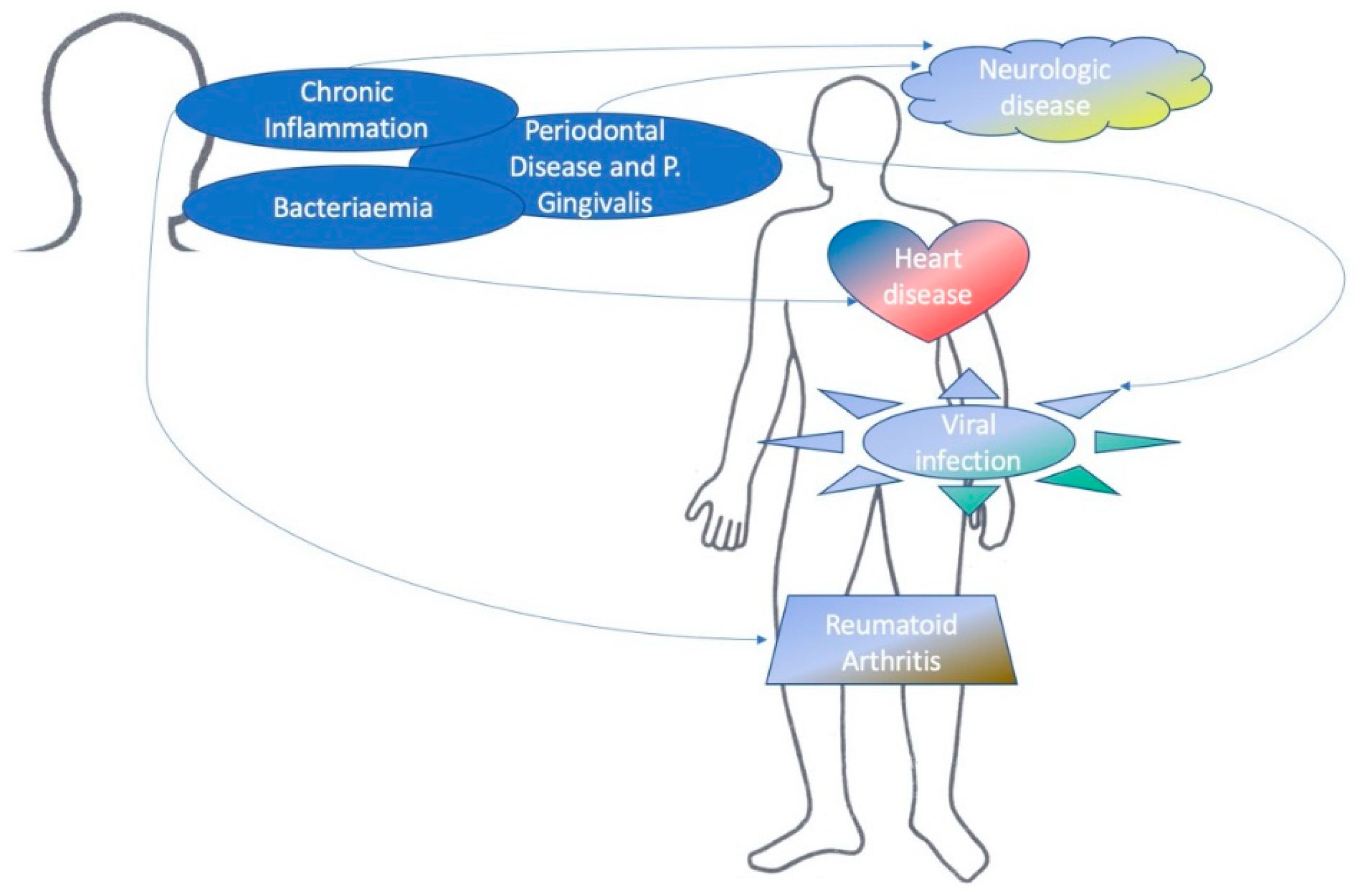
4. Discussion
4.1. Summary of Evidence
4.1.1. Neurology
4.1.2. Cardiology
4.1.3. Rheumatology
4.1.4. Diabetology
4.1.5. Oncology
4.1.6. Biology and Immunology
4.2. Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Putsep, K.; Carlsson, G.; Boman, H.G.; Andersson, M. Deficiency of antibacterial peptides in patients with morbus Kostmann: An observation study. Lancet 2002, 360, 1144–1149. [Google Scholar] [CrossRef]
- Poole, D.F.; Newman, H.N. Dental plaque and oral health. Nature 1971, 234, 329–331. [Google Scholar] [CrossRef] [PubMed]
- Pihlstrom, B.L.; Michalowicz, B.S.; Johnson, N.W. Periodontal diseases. Lancet 2005, 366, 1809–1820. [Google Scholar] [CrossRef] [Green Version]
- Holt, S.C.; Ebersole, J.; Felton, J.; Brunsvold, M.; Kornman, K.S. Implantation of Bacteroides gingivalis in nonhuman primates initiates progression of periodontitis. Science 1988, 239, 55–57. [Google Scholar] [CrossRef]
- Bjertness, E.; Hansen, B.F.; Berseth, G.; Gronnesby, J.K. Oral hygiene and periodontitis in young adults. Lancet 1993, 342, 1170–1171. [Google Scholar] [CrossRef]
- Hanisch, M.; Hoffmann, T.; Bohner, L.; Hanisch, L.; Benz, K.; Kleinheinz, J.; Jackowski, J. Rare Diseases with Periodontal Manifestations. Int. J. Environ. Res. Public Health 2019, 16, 867. [Google Scholar] [CrossRef]
- Mysak, J.; Podzimek, S.; Sommerova, P.; Lyuya-Mi, Y.; Bartova, J.; Janatova, T.; Prochazkova, J.; Duskova, J. Porphyromonas gingivalis: Major periodontopathic pathogen overview. J. Immunol. Res. 2014, 2014, 476068. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, L.; Moraes, M.F.; Oliveira, P.; Abecasis, P. A train driver with painful legs. Lancet 1999, 353, 2034. [Google Scholar] [CrossRef]
- Katz, J.; Marc, H.; Porter, S.; Ruskin, J. Inflammation, periodontitis, and coronary heart disease. Lancet 2001, 358, 1998. [Google Scholar] [CrossRef]
- Dominy, S.S.; Lynch, C.; Ermini, F.; Benedyk, M.; Marczyk, A.; Konradi, A.; Nguyen, M.; Haditsch, U.; Raha, D.; Griffin, C.; et al. Porphyromonas gingivalis in Alzheimer’s disease brains: Evidence for disease causation and treatment with small-molecule inhibitors. Sci. Adv. 2019, 5, eaau3333. [Google Scholar] [CrossRef] [Green Version]
- Olsen, I.; Yilmaz, Ö. Possible role of Porphyromonas gingivalis in orodigestive cancers. J. Oral. Microbiol. 2019, 11, 1563410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Magana, M.; Sereti, C.; Ioannidis, A.; Mitchell, C.A.; Ball, A.R.; Magiorkinis, E.; Chatzipanagiotou, S.; Hamblin, M.R.; Hadjifrangiskou, M.; Tegos, G.P. Options and Limitations in Clinical Investigation of Bacterial Biofilms. Clin. Microbiol. Rev. 2018, 31, e00084-16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Africa, C.W.J.; Nel, J.; Stemmet, M. Anaerobes and bacterial vaginosis in pregnancy: Virulence factors contributing to vaginal colonisation. Int. J. Environ. Res. Public Health 2014, 11, 6979–7000. [Google Scholar] [CrossRef] [PubMed]
- da Costa Santos, C.M.; de Mattos Pimenta, C.A.; Nobre, M.R. The PICO strategy for the research question construction and evidence search. Rev. Lat. Am. Enferm. 2007, 15, 508–511. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tian, J.H.; Ge, L.; Li, L. The PRISMA Extension Statement. Ann. Intern. Med. 2015, 163, 566. [Google Scholar] [CrossRef]
- Liu, H.; Zhou, X.; Yu, G.; Sun, X. The effects of the PRISMA statement to improve the conduct and reporting of systematic reviews and meta-analyses of nursing interventions for patients with heart failure. Int. J. Nurs. Pr. 2019, 25, e12729. [Google Scholar] [CrossRef]
- Hutton, B.; Salanti, G.; Caldwell, D.M.; Chaimani, A.; Schmid, C.H.; Cameron, C.; Ioannidis, J.P.; Straus, S.; Thorlund, K.; Jansen, J.P.; et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: Checklist and explanations. Ann. Intern. Med. 2015, 162, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Bale, B.F.; Doneen, A.L.; Vigerust, D.J. High-risk periodontal pathogens contribute to the pathogenesis of atherosclerosis. Postgrad. Med. J. 2017, 93, 215–220. [Google Scholar] [CrossRef]
- Tiantian, M.; Xin, L. Promotion of Porphyromonas gingivalis to viral disease. Hua Xi Kou Qiang Yi Xue Za Zhi Huaxi Kouqiang Yixue Zazhi West China J. Stomatol. 2016, 34, 425–428. [Google Scholar]
- Gholizadeh, P.; Eslami, H.; Yousefi, M.; Asgharzadeh, M.; Aghazadeh, M.; Kafil, H.S. Role of oral microbiome on oral cancers, a review. Biomed. Pharmacother. Biomed. Pharmacother. 2016, 84, 552–558. [Google Scholar] [CrossRef]
- Chistiakov, D.A.; Orekhov, A.N.; Bobryshev, Y.V. Links between atherosclerotic and periodontal disease. Exp. Mol. Pathol. 2016, 100, 220–235. [Google Scholar] [CrossRef]
- Alfakry, H.; Malle, E.; Koyani, C.N.; Pussinen, P.J.; Sorsa, T. Neutrophil proteolytic activation cascades: A possible mechanistic link between chronic periodontitis and coronary heart disease. Innate Immun. 2016, 22, 85–99. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xie, H. Biogenesis and function of Porphyromonas gingivalis outer membrane vesicles. Future Microbiol. 2015, 10, 1517–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, Z.; Nakanishi, H. Connection between periodontitis and Alzheimer’s disease: Possible roles of microglia and leptomeningeal cells. J. Pharmacol. Sci. 2014, 126, 8–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervino, G.; Terranova, A.; Briguglio, F.; De Stefano, R.; Famà, F.; D’Amico, C.; Amoroso, G.; Marino, S.; Gorassini, F.; Mastroieni, R.; et al. Diabetes: Oral health related quality of life and oral alterations. BioMed Res. Int. 2019, 2019. [Google Scholar] [CrossRef] [Green Version]
- Scher, J.U.; Bretz, W.A.; Abramson, S.B. Periodontal disease and subgingival microbiota as contributors for rheumatoid arthritis pathogenesis: Modifiable risk factors? Curr. Opin. Rheumatol. 2014, 26, 424–429. [Google Scholar] [CrossRef] [Green Version]
- Grover, V.; Kapoor, A.; Malhotra, R.; Kaur, G. Porphyromonas gingivalis antigenic determinants-potential targets for the vaccine development against periodontitis. Infect. Disord. Drug Targets 2014, 14, 1–13. [Google Scholar] [CrossRef]
- Brusca, S.B.; Abramson, S.B.; Scher, J.U. Microbiome and mucosal inflammation as extra-articular triggers for rheumatoid arthritis and autoimmunity. Curr. Opin. Rheumatol. 2014, 26, 101–107. [Google Scholar] [CrossRef] [Green Version]
- Reyes, L.; Herrera, D.; Kozarov, E.; Roldan, S.; Progulske-Fox, A. Periodontal bacterial invasion and infection: Contribution to atherosclerotic pathology. J. Clin. Periodontol. 2013, 40 (Suppl. 14), S30–S50. [Google Scholar] [CrossRef]
- Michaud, D.S. Role of bacterial infections in pancreatic cancer. Carcinogenesis 2013, 34, 2193–2197. [Google Scholar] [CrossRef]
- Han, Y.W.; Wang, X. Mobile microbiome: Oral bacteria in extra-oral infections and inflammation. J. Dent. Res. 2013, 92, 485–491. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- El-Shinnawi, U.; Soory, M. Associations between periodontitis and systemic inflammatory diseases: Response to treatment. Recent Pat. Endocr. Metab. Immune Drug Discov. 2013, 7, 169–188. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Ochiai, K. Role of histone modification on transcriptional regulation and HIV-1 gene expression: Possible mechanisms of periodontal diseases in AIDS progression. J. Oral Sci. 2011, 53, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huck, O.; Saadi-Thiers, K.; Tenenbaum, H.; Davideau, J.L.; Romagna, C.; Laurent, Y.; Cottin, Y.; Roul, J.G. Evaluating periodontal risk for patients at risk of or suffering from atherosclerosis: Recent biological hypotheses and therapeutic consequences. Arch. Cardiovasc. Dis. 2011, 104, 352–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNicol, A.; Israels, S.J. Mechanisms of oral bacteria-induced platelet activation. Can. J. Physiol. Pharmacol. 2010, 88, 510–524. [Google Scholar] [CrossRef] [PubMed]
- Inaba, H.; Amano, A. Roles of oral bacteria in cardiovascular diseases—From molecular mechanisms to clinical cases: Implication of periodontal diseases in development of systemic diseases. J. Pharmacol. Sci. 2010, 113, 103–109. [Google Scholar] [CrossRef] [Green Version]
- Hayashi, C.; Gudino, C.V.; Gibson, F.C., 3rd; Genco, C.A. Review: Pathogen-induced inflammation at sites distant from oral infection: Bacterial persistence and induction of cell-specific innate immune inflammatory pathways. Mol. Oral Microbiol. 2010, 25, 305–316. [Google Scholar] [CrossRef] [Green Version]
- Detert, J.; Pischon, N.; Burmester, G.R.; Buttgereit, F. The association between rheumatoid arthritis and periodontal disease. Arthritis Res. Ther. 2010, 12, 218. [Google Scholar] [CrossRef] [Green Version]
- Fiorillo, L. Oral Health: The First Step to Well-Being. Medicina 2019, 55, 676. [Google Scholar] [CrossRef] [Green Version]
- Lindhe, J. Parodontologia Clinica E Implantologia Orale, 5th ed.; Edi Ermes: Milano, Italy, 2009; Volume 1. [Google Scholar]
- Lombardi, T.; Bernardello, F.; Berton, F.; Porrelli, D.; Rapani, A.; Camurri Piloni, A.; Fiorillo, L.; Di Lenarda, R.; Stacchi, C. Efficacy of Alveolar Ridge Preservation after Maxillary Molar Extraction in Reducing Crestal Bone Resorption and Sinus Pneumatization: A Multicenter Prospective Case-Control Study. BioMed Res. Int. 2018, 2018. [Google Scholar] [CrossRef] [Green Version]
- Isola, G.; Cicciù, M.; Fiorillo, L.; Matarese, G. Association between odontoma and impacted teeth. J. Craniofac. Surg. 2017, 28, 755–758. [Google Scholar] [CrossRef] [PubMed]
- Cervino, G.; Romeo, U.; Lauritano, F.; Bramanti, E.; Fiorillo, L.; D’Amico, C.; Milone, D.; Laino, L.; Campolongo, F.; Rapisarda, S.; et al. Fem and Von Mises Analysis of OSSTEM(r) Dental Implant Structural Components: Evaluation of Different Direction Dynamic Loads. Open Dent. J. 2018, 12, 219–229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bramanti, E.; Matacena, G.; Cecchetti, F.; Arcuri, C.; Cicciù, M. Oral health-related quality of life in partially edentulous patients before and after implant therapy: A 2-year longitudinal study. ORAL Implantol. 2013, 6, 37–42. [Google Scholar] [CrossRef]
- Lo Giudice, G.; Cutroneo, G.; Centofanti, A.; Artemisia, A.; Bramanti, E.; Militi, A.; Rizzo, G.; Favaloro, A.; Irrera, A.; Lo Giudice, R.; et al. Dentin morphology of root canal surface: A quantitative evaluation based on a scanning electronic microscopy study. BioMed Res. Int. 2015, 2015. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Germano, F.; Bramanti, E.; Arcuri, C.; Cecchetti, F.; Cicciù, M. Atomic force microscopy of bacteria from periodontal subgingival biofilm: Preliminary study results. Eur. J. Dent. 2013, 7, 152–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maiorana, C.; Beretta, M.; Grossi, G.B.; Santoro, F.; Herford, A.S.; Nagursky, H.; Cicciù, M. Histomorphometric evaluation of anorganic bovine bone coverage to reduce autogenous grafts resorption: Preliminary results. Open Dent. J. 2011, 5, 71–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luongo, G.; Oteri, G. A noninterventional study documenting use and success of implants with a new chemically modified titanium surface in daily dental practice. J. Oral Implantol. 2010, 36, 305–314. [Google Scholar] [CrossRef]
- Herford, A.S.; Lu, M.; Akin, L.; Cicciù, M. Evaluation of a porcine matrix with and without platelet-derived growth factor for bone graft coverage in pigs. Int. J. Oral Maxillofac. Implant. 2012, 27, 1351–1358. [Google Scholar]
- Cervino, G.; Fiorillo, L.; Herford, A.S.; Romeo, U.; Bianchi, A.; Crimi, S.; D’Amico, C.; De Stefano, R.; Troiano, G.; Santoro, R.; et al. Molecular Biomarkers Related to Oral Carcinoma: Clinical Trial Outcome Evaluation in a Literature Review. Dis. Markers 2019, 2019, 11. [Google Scholar] [CrossRef]
- Crimi, S.; Fiorillo, L.; Bianchi, A.; D’Amico, C.; Amoroso, G.; Gorassini, F.; Mastroieni, R.; Marino, S.; Scoglio, C.; Catalano, F.; et al. Herpes Virus, Oral Clinical Signs and QoL: Systematic Review of Recent Data. Viruses 2019, 11, 463. [Google Scholar] [CrossRef] [Green Version]
- Cervino, G.; Fiorillo, L.; Monte, I.P.; De Stefano, R.; Laino, L.; Crimi, S.; Bianchi, A.; Herford, A.S.; Biondi, A.; Cicciù, M. Advances in Antiplatelet Therapy for Dentofacial Surgery Patients: Focus on Past and Present Strategies. Materials 2019, 12, 1524. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Öğrendik, M. Periodontal Pathogens in the Etiology of Pancreatic Cancer. Gastrointest. Tumors 2017, 3, 125–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Neurology | Chronic inflammation and Alzheimer’s Disease (AD) |
| P. gingivalis and AD | |
| Cardiology | Atherosclerosis risk factor and periodontal disease. |
| PD and Cardiovascular Disease (CVD), Age, Smoking, Diabetes | |
| Chronic infection and Coronary Heart disease (CHD) | |
| Periodontal Bacteria and atherosclerosis | |
| Cytokines and coronary heart disease | |
| Immunology | Periodontitis an immune response |
| Antigenic target for P. gingivalis | |
| Microbiome, Periodontal disease | |
| Serum lipoprotein concentration, endothelial permeability, lipoprotein binding in intimate | |
| Periodontal disease and AIDS progression | |
| Rheumatology | Rheumatoid Arthritis |
| Osteoporosis | |
| Diabetology | Diabetes mellitus |
| Insulin resistance | |
| Oncology | P. gingivalis and Oral Cancer (OC) |
| Bacterial infection and Pancreatic Cancer (PC) | |
| Biology | Virus and periodontal disease correlation |
| Bacteriaemias and systemic disease | |
| Periodontal disease and Systemic diseases | |
| P. gingivalis biology | |
| Oral bacteria and extraoral infections |
| Authors and Year | Items | Outcomes |
|---|---|---|
| Dominy et al., 2019 [10] | P. gingivalis and Alzheimer’s disease | P. gingivalis and gingipains were identified in the brain of Alzheimer’s patients. Gingipain inhibition reduced the bacterial load of P. gingivalis infection. |
| Bale et al., 2017 [18] | Serum lipoprotein concentration, endothelial permeability, lipoprotein binding in intima | This study supports that Periodontal disease (PD) could be associated with arterial disease |
| Tiantian et al., 2016 [19] | Virus and periodontal disease correlation | P. gingivalis can interact with a variety of bacterium viruses which may be the reason for chronic periodontitis and systemic disease |
| Gholizadeh et al., 2016 [20] | P. gingivalis and Oral Cancer (OC) | PD, systemic condition and head and neck cancer (HNC) could be correlated |
| Chistiakov et al., 2016 [21] | PD and Cardiovascular Disease (CVD), Age, Smoking, Diabetes | Periodontal pathogens, virulence factors and bacterial endotoxins are correlated with CVD development as endothelial dysfunction, systemic inflammation, oxidative stress, lipid accumulation, vascular remodeling, and atherothrombosis. |
| Alfakry et al., 2016 [22] | Chronic infection and Coronary Heart disease (CHD) | Inflammation activates endogenous degradation pathways mediated by immune responses and it takes to destructive cellular mechanism. Matrix metalloproteinases (MMPs) can activate immune response, with extracellular matrix components degradation. These mechanisms could lead to CHD. |
| Xie 2015 [23] | P. gingivalis biology | P. gingivalis outer membrane produces vesicles. These vesicles can communicate with other member of microbial biofilm and with host cells. |
| Wu et al., 2014 [24] | Chronic inflammation and Alzheimer’s disease (AD) | Systemic inflammations are correlated with neuroinflammation and inflammation of the brain. Diabetes [25], cardiovascular disease, or PD could be implicated with AD. Chronic periodontitis can be a significant source of systemic inflammation and so AD too. |
| Scher et al., 2014 [26] | Periodontitis an immune response | There is a correlation between PD a rheumatoid arthritis (RA). Circulating antibodies against periodontopathic bacteria, as P. gingivalis, and their associated inflammatory response have been found in RA affected patients. Smoke habits seems to be a co-associated factor for RA development. |
| Grover et al., 2014 [27] | Antigenic target for P. gingivalis | Microbial genome sequencing and bioinformatics could lead to a vaccine development for P. gingivalis. |
| Brusca et al., 2014 [28] | Microbiome and RA | Presence of bacteria in mucosal surfaces can alter local and systemic immune responses and could cause joint inflammation |
| Reyes et al., 2013 [29] | Periodontal Bacteria and atherosclerosis | Periodontal bacteria can disseminate from oral cavity to systemic vascular tissue, could live in those tissues and damage cells. These bacteria can induce atherosclerosis. |
| Michaud 2013 [30] | Bacterial infection and Pancreatic Cancer (PC) | Helicobacter pylor may be a risk factor for PC, other bacteria that should be considered is P. gingivalis. Periodontal disease and P. gingivalis play a role on carcinogenesis of pancreas. Systemic inflammation markers can be found due to oral bacteria in the blood. |
| Han et al., 2013 [31] | Oral bacteria and extraoral infections | Oral commensals and pathogens could support extra-oral infections and inflammations. Some of these conditions are represented by CVD, adverse pregnancy outcomes, RA, inflammatory bowel disease, colorectal cancer, respiratory infection, and organ inflammation or infections |
| El-Shinnawi et al., 2013 [32] | Cytokines and coronary heart disease | TNF-alpha gene polymorphism is linked to periodontal attachment loss in patients with CHD. P. gingivalis and oral inflammation could be associated to insulin resistance and arthritis too. |
| Imai et al., 2011 [33] | Periodontal disease and AIDS progression | Epigenetic regulation is involved in maintenance and reactivation of HIV-1 by periodontopathic bacteria. |
| Huck et al., 2011 [34] | Atherosclerosis risk factor and periodontal disease. | PD negatively influences cardiovascular status. Severe form of Atherosclerosis is associated to P. gingivalis. |
| McNicol et al., 2010 [35] | Bacteriaemias and systemic disease | Atherothrombotic disorders may be due to persistent bacteriaemia and oral infection. Bacteriaemias occur frequently in PD patients. Some bacteria, as P. gingivalis can activate platelets in vitro. |
| Inaba et al., 2010 [36] | Periodontal disease and systemic diseases | Periodontal disease is associated with CVD, preterm delivery of low birth weight, diabetes mellitus, respiratory diseases, and osteoporosis. |
| Hayashi et al., 2010 [37] | Periodontal disease and systemic diseases | P. gingivalis induce a chronic inflammation, this status could lead to infection, that is correlated with systemic diseases as diabetes, preterm birth, stroke, and CVD. P. gingivalis stimulate chronic inflammation and plaque accumulation and has a role on Toll-like receptors signaling. |
| Detert et al., 2010 [38] | Periodontal disease and rheumatoid arthritis | The existence of rheumatic or other inflammatory disease may promote periodontal disease, and periodontal disease maintains systemic diseases. P. gingivalis plays an important role on citrullination. |
| Authors and Year | Items | Medical Disease |
|---|---|---|
| Bale et al., 2017 [18] | Serum lipoprotein concentration, endothelial permeability, lipoprotein binding in intima | Cardiology |
| Chistiakov et al., 2016 [21] | PD and cardiovascular disease (CVD), age, smoking, diabetes | |
| Alfakry et al., 2016 [22] | Chronic infection and coronary heart disease (CHD) | |
| Reyes et al., 2013 [29] | Periodontal bacteria and atherosclerosis | |
| El-Shinnawi et al., 2013 [32] | Cytokines and coronary heart disease | |
| Huck et al., 2011 [34] | Atherosclerosis risk factor and periodontal disease. | |
| McNicol et al., 2010 [35] | Bacteriaemias and systemic disease | |
| Inaba et al., 2010 [36] | Periodontal disease and systemic diseases | |
| Hayashi et al., 2010 [37] | Periodontal disease and systemic diseases | |
| Scher et al., 2014 [26] | Periodontitis an immune response | Rheumatology |
| Han et al., 2013 [31] | Oral bacteria and extraoral infections | |
| El-Shinnawi et al., 2013 [32] | Cytokines and coronary heart disease | Diabetology |
| Gholizadeh et al., 2016 [20] | P. gingivalis and oral cancer (OC) | Oncology |
| Tiantian et al., 2016 [19] | Virus and periodontal disease correlation | Biology and Immunology |
| Grover et al., 2014 [27] | Antigenic target for P. gingivalis | |
| Michaud 2013 [30] | Bacterial infection and pancreatic cancer (PC) | |
| Brusca et al., 2014 [28] | Microbiome and RA | |
| Imai et al., 2011 [33] | Periodontal disease and AIDS progression | |
| Dominy et al., 2019 [10] | P. gingivalis and Alzheimer’s disease | Neurology |
| Wu et al., 2014 [24] | Chronic inflammation and Alzheimer’s disease (AD) |
| Authors and Year | Risk of Bias | |||
|---|---|---|---|---|
| Unclear | Low | Moderate | High | |
| Dominy et al., 2019 [10] | ✓ | |||
| Bale et al., 2017 [18] | ✓ | |||
| Tiantian et al., 2016 [19] | ✓ | |||
| Gholizadeh et al., 2016 [20] | ✓ | |||
| Chistiakov et al., 2016 [21] | ✓ | |||
| Alfakry et al., 2016 [22] | ✓ | |||
| Xie 2015 [23] | ✓ | |||
| Wu et al., 2014 [24] | ✓ | |||
| Scher et al., 2014 [26] | ✓ | |||
| Grover et al., 2014 [27] | ✓ | |||
| Brusca et al., 2014 [28] | ✓ | |||
| Reyes et al., 2013 [29] | ✓ | |||
| Michaud 2013 [30] | ✓ | |||
| Han et al., 2013 [31] | ✓ | |||
| El-Shinnawi et al., 2013 [32] | ✓ | |||
| Imai et al., 2011 [33] | ✓ | |||
| Huck et al., 2011 [34] | ✓ | |||
| McNicol et al., 2010 [35] | ✓ | |||
| Inaba et al., 2010 [36] | ✓ | |||
| Hayashi et al., 2010 [37] | ✓ | |||
| Detert et al., 2010 [38] | ✓ | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fiorillo, L.; Cervino, G.; Laino, L.; D’Amico, C.; Mauceri, R.; Tozum, T.F.; Gaeta, M.; Cicciù, M. Porphyromonas gingivalis, Periodontal and Systemic Implications: A Systematic Review. Dent. J. 2019, 7, 114. https://0-doi-org.brum.beds.ac.uk/10.3390/dj7040114
Fiorillo L, Cervino G, Laino L, D’Amico C, Mauceri R, Tozum TF, Gaeta M, Cicciù M. Porphyromonas gingivalis, Periodontal and Systemic Implications: A Systematic Review. Dentistry Journal. 2019; 7(4):114. https://0-doi-org.brum.beds.ac.uk/10.3390/dj7040114
Chicago/Turabian StyleFiorillo, Luca, Gabriele Cervino, Luigi Laino, Cesare D’Amico, Rodolfo Mauceri, Tolga Fikret Tozum, Michele Gaeta, and Marco Cicciù. 2019. "Porphyromonas gingivalis, Periodontal and Systemic Implications: A Systematic Review" Dentistry Journal 7, no. 4: 114. https://0-doi-org.brum.beds.ac.uk/10.3390/dj7040114