Continuous Measurement of Three-Dimensional Root Canal Curvature Using Cone-Beam Computed and Micro-Computed Tomography: A Comparative Study

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Teeth Selection Criteria and Preparation
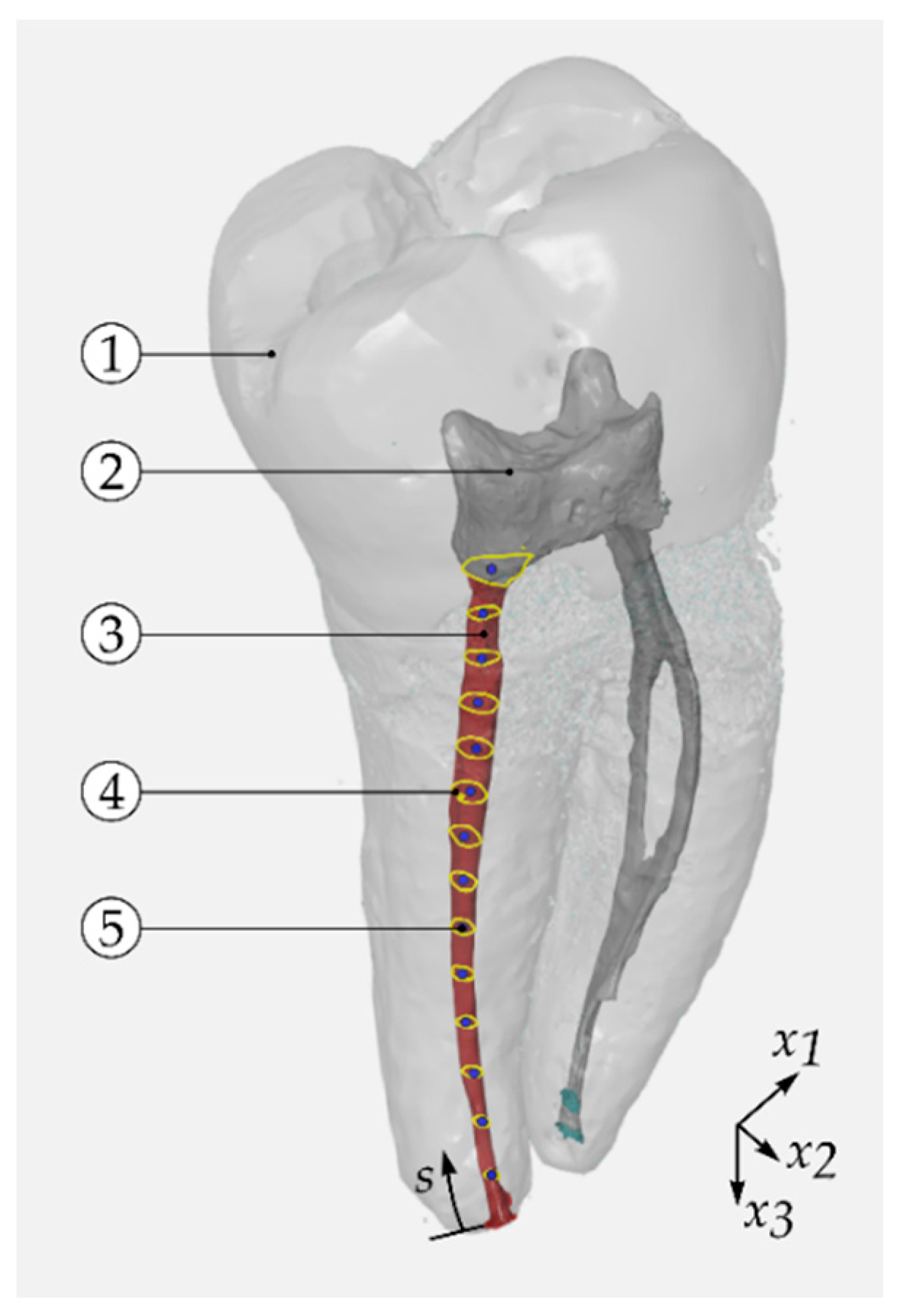
2.2. Imaging Procedures and Evaluation of Centre Line
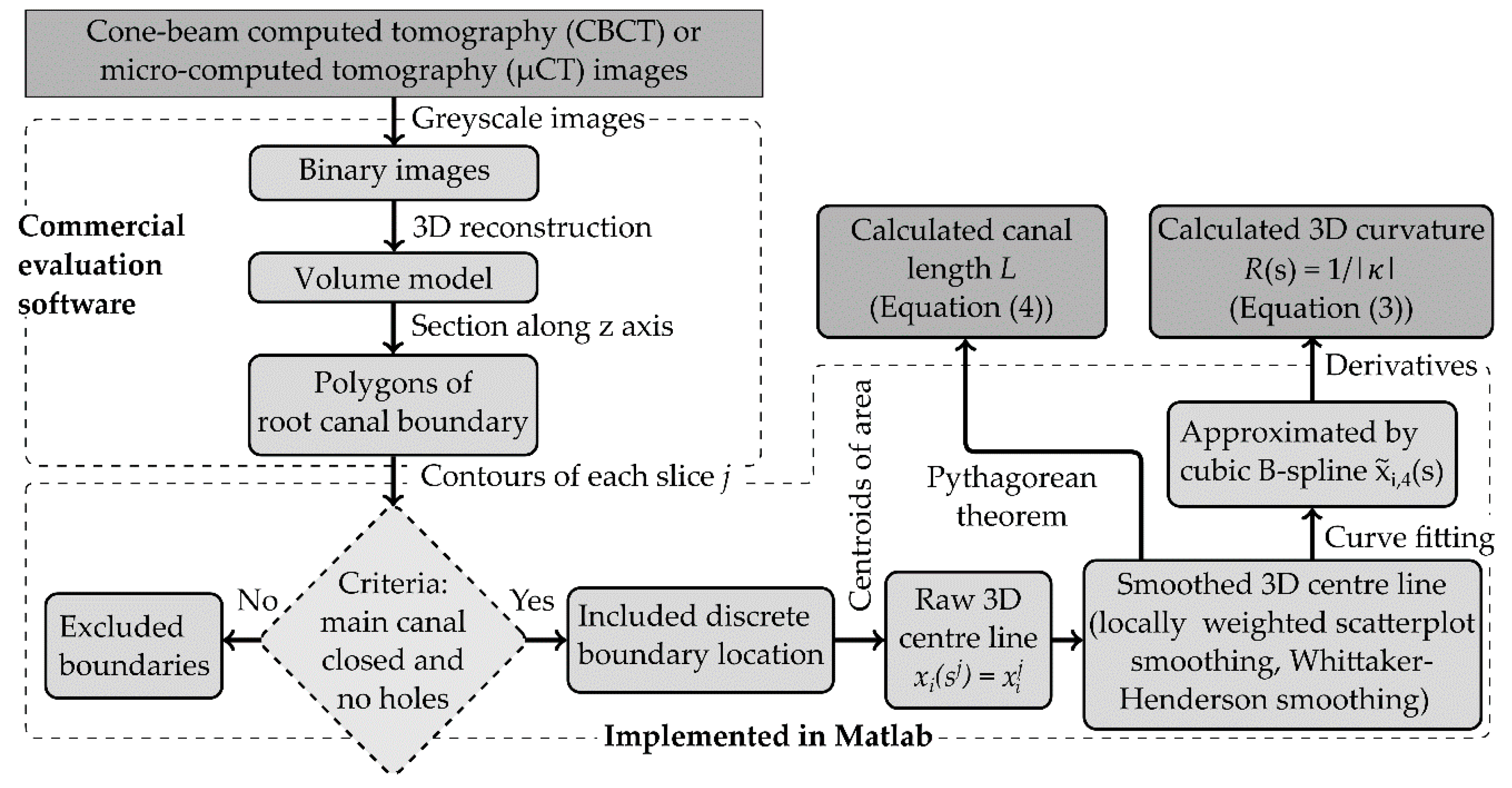
2.3. Filtering and Measurement Algorithm of Centre Line
2.4. Data Analysis
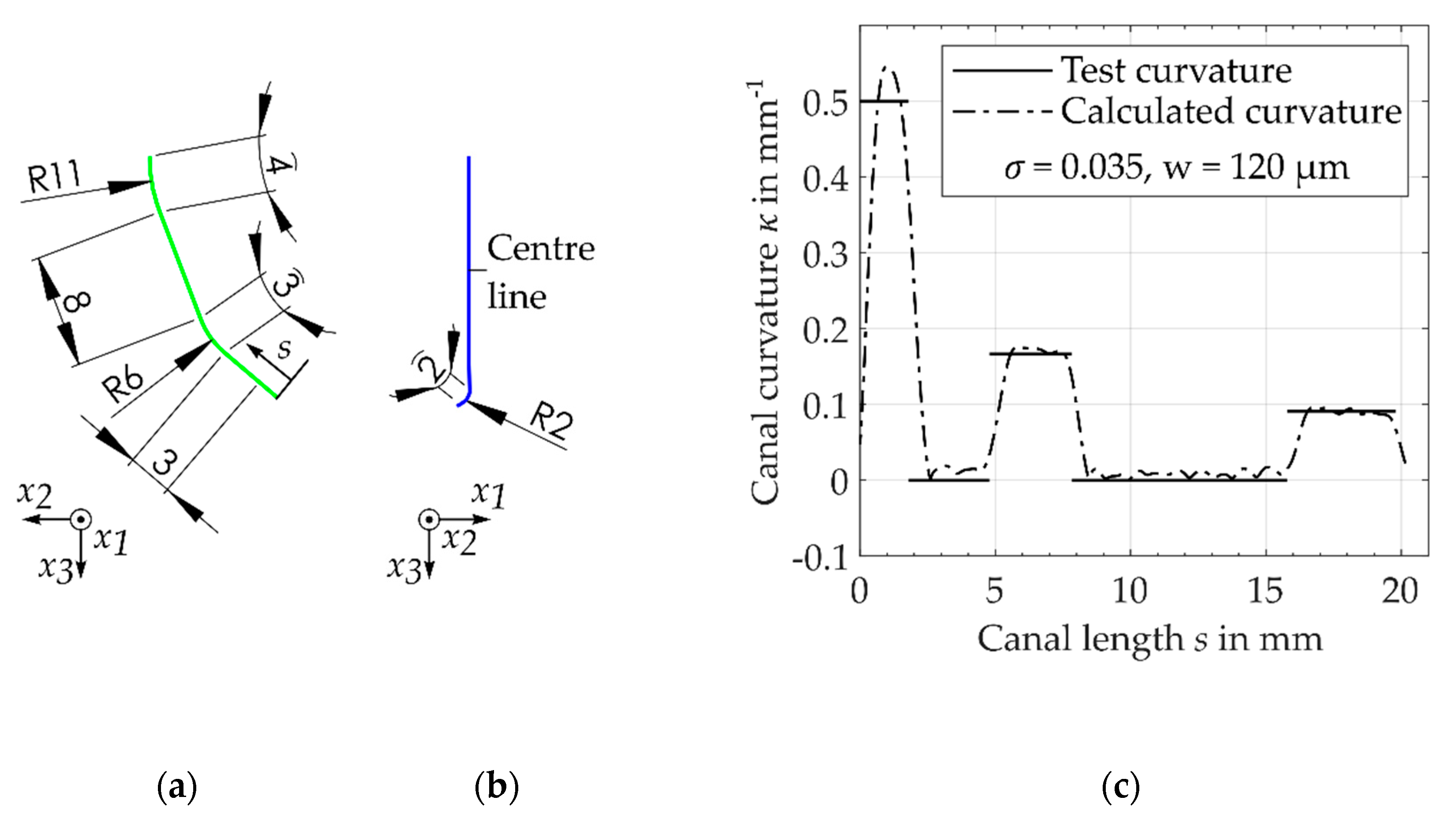
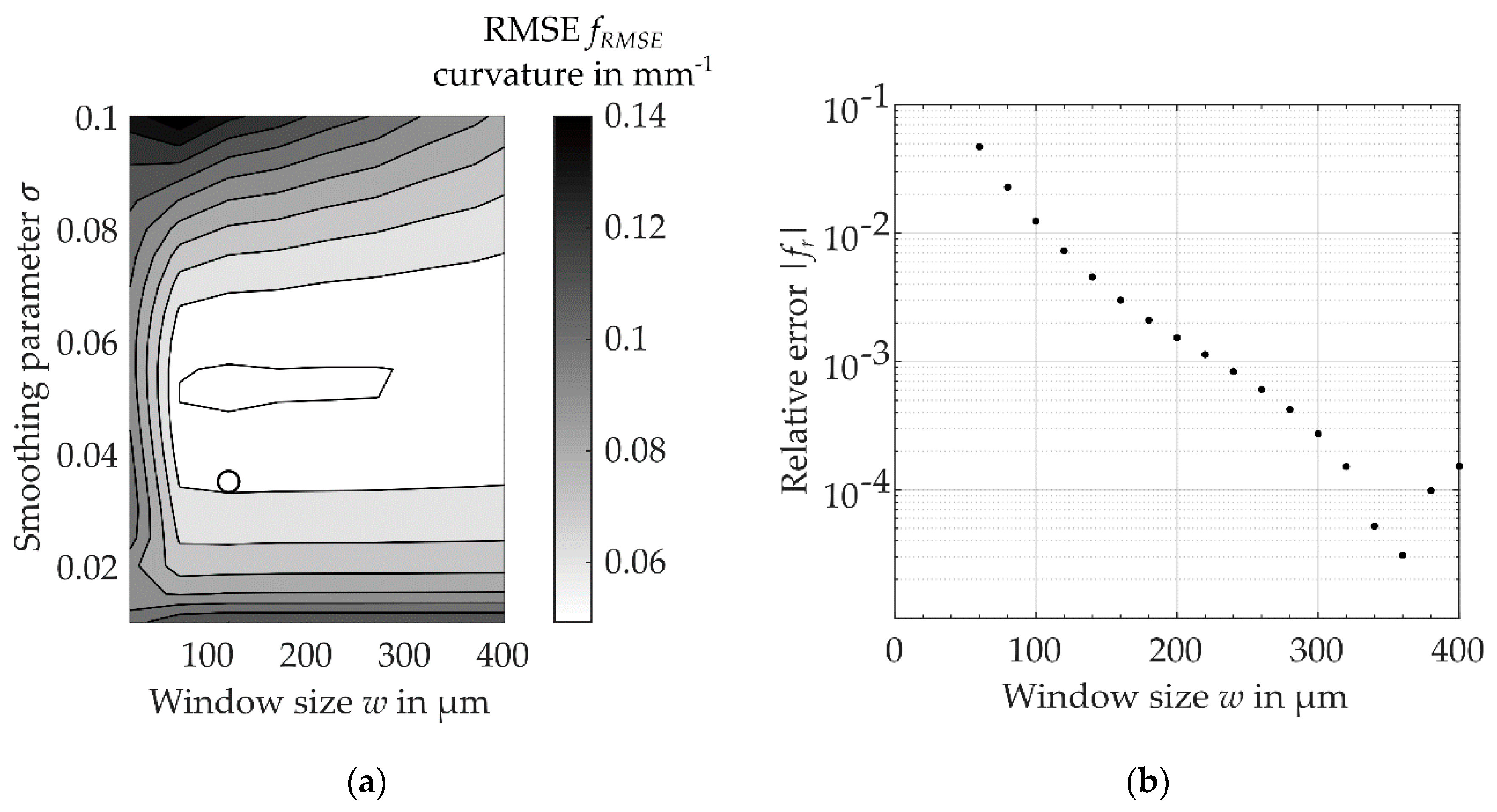
2.5. Algorithm Performance
3. Results
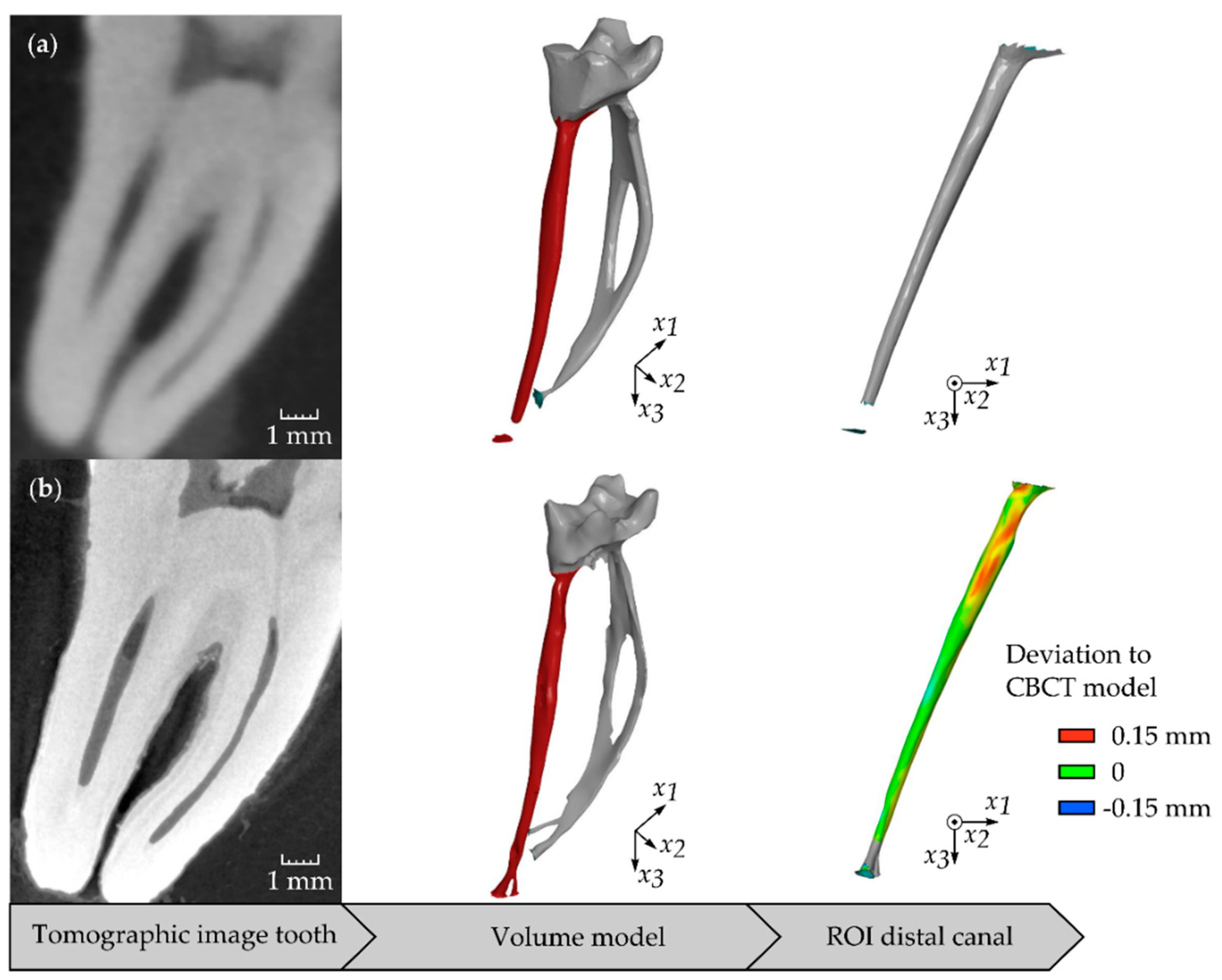
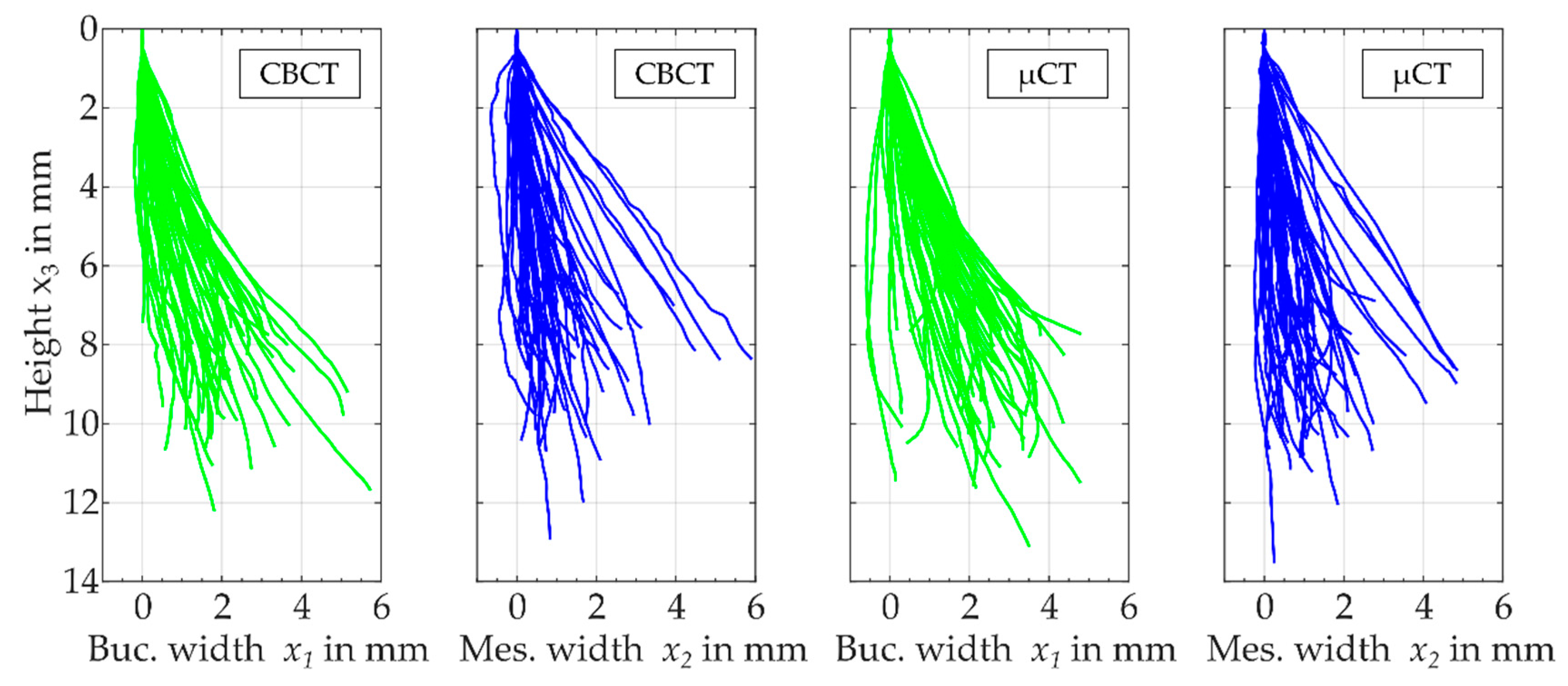
3.1. Comparison of Three-Dimensional Centre Lines
3.2. Radiological Three-Dimensional Root Canal Length
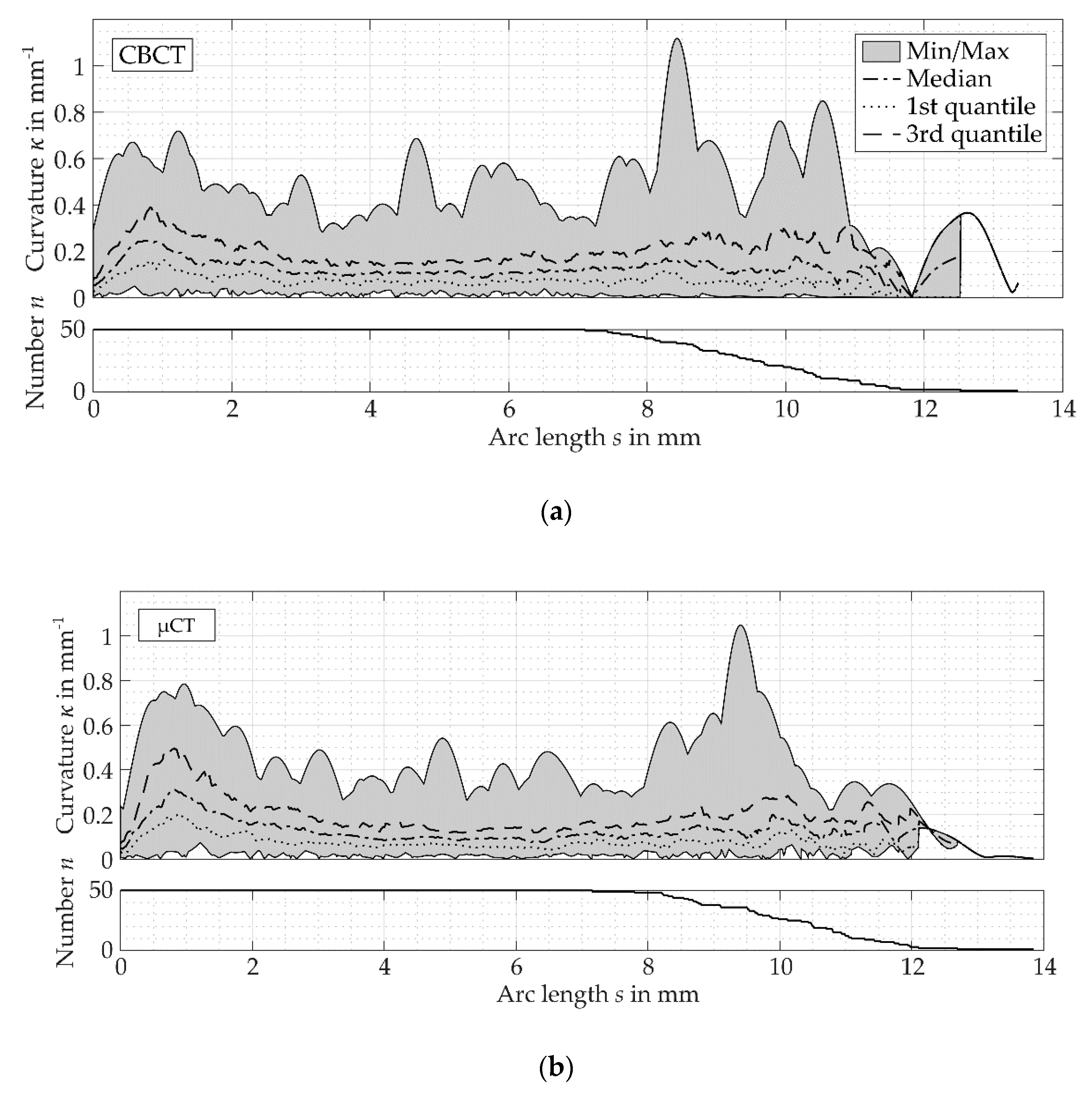
3.3. Curvature Measurements
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Jafarzadeh, H.; Abbott, P.V. Ledge formation: Review of a great challenge in endodontics. J. Endod. 2007, 33, 1155–1162. [Google Scholar] [CrossRef] [PubMed]
- Alhadainy, H.A. Root perforations. Oral Surg. Oral Med. Oral Pathol. 1994, 78, 368–374. [Google Scholar] [CrossRef]
- Kirsch, J.; Reinauer, K.S.; Meissner, H.; Dannemann, M.; Kucher, M.; Modler, N.; Hannig, C.; Weber, M.-T. Ultrasonic and sonic irrigant activation in endodontics: A fractographic examination. Dtsch. Zahnärztl Z. Int. 2019, 1, 209–221. [Google Scholar] [CrossRef]
- Schneider, S.W. A comparison of canal preparations in straight and curved root canals. Oral Surg. Oral Med. Oral Pathol. 1971, 32, 271–275. [Google Scholar] [CrossRef]
- Balani, P.; Niazi, F.; Rashid, H. A brief review of the methods used to determine the curvature of root canals. J. Res. Dent. 2015, 3, 57. [Google Scholar] [CrossRef]
- Habib, A.A.; Taha, M.I.; Farah, E.M. Methodologies used in quality assessment of root canal preparation techniques: Review of the literature. J. Taibah Univ. Med. Sci. 2015, 10, 123–131. [Google Scholar] [CrossRef] [Green Version]
- Hartmann, R.C.; Fensterseifer, M.; Peters, O.A.; de Figueiredo, J.A.P.; Gomes, M.S.; Rossi-Fedele, G. Methods for measurement of root canal curvature: A systematic and critical review. Int. Endod. J. 2018. [Google Scholar] [CrossRef] [Green Version]
- Peters, O.A.; Laib, A.; Rüegsegger, P.; Barbakow, F. Three-dimensional analysis of root canal geometry by high-resolution computed tomography. J. Dent. Res. 2000, 79, 1405–1409. [Google Scholar] [CrossRef]
- Lee, J.-K.; Ha, B.-H.; Choi, J.-H.; Heo, S.-M.; Perinpanayagam, H. Quantitative three-dimensional analysis of root canal curvature in maxillary first molars using micro-computed tomography. J. Endod. 2006, 32, 941–945. [Google Scholar] [CrossRef]
- Lee, J.K.; Yoo, Y.J.; Perinpanayagam, H.; Ha, B.H.; Lim, S.M.; Oh, S.R.; Gu, Y.; Chang, S.W.; Zhu, Q.; Kum, K.Y. Three-dimensional modelling and concurrent measurements of root anatomy in mandibular first molar mesial roots using micro-computed tomography. Int. Endod. J. 2015, 48, 380–389. [Google Scholar] [CrossRef]
- Park, P.-S.; Kim, K.-D.; Perinpanayagam, H.; Lee, J.-K.; Chang, S.W.; Chung, S.H.; Kaufman, B.; Zhu, Q.; Safavi, K.E.; Kum, K.-Y. Three-dimensional analysis of root canal curvature and direction of maxillary lateral incisors by using cone-beam computed tomography. J. Endod. 2013, 39, 1124–1129. [Google Scholar] [CrossRef] [PubMed]
- Dannemann, M.; Kucher, M.; Kirsch, J.; Binkowski, A.; Modler, N.; Hannig, C.; Weber, M.-T. An Approach for a Mathematical Description of Human Root Canals by Means of Elementary Parameters. J. Endod. 2017, 43, 536–543. [Google Scholar] [CrossRef] [PubMed]
- Benyó, B. Identification of dental root canals and their medial line from micro-CT and cone-beam CT records. Biomed. Eng. Online 2012, 11, 81. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Benyó, B.; Szilagyi, L.; Haidegger, T.; Kovacs, L.; Nagy-Dobo, C. Detection of the root canal’s centerline from dental micro-CT records. In Proceedings of the 31st Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 2–6 September 2009; pp. 3517–3520. [Google Scholar] [CrossRef]
- Bergmans, L.; van Cleynenbreugel, J.; Wevers, M.; Lambrechts, P. A methodology for quantitative evaluation of root canal instrumentation using microcomputed tomography. Int. Endod. J. 2001, 34, 390–398. [Google Scholar] [CrossRef] [PubMed]
- Eaton, J.A.; Clement, D.J.; Lloyd, A.; Marchesan, M.A. Micro-Computed Tomographic Evaluation of the Influence of Root Canal System Landmarks on Access Outline Forms and Canal Curvatures in Mandibular Molars. J. Endod. 2015, 41, 1888–1891. [Google Scholar] [CrossRef]
- Choi, M.-R.; Moon, Y.-M.; Seo, M.-S. Prevalence and features of distolingual roots in mandibular molars analyzed by cone-beam computed tomography. Imaging Sci. Dent. 2015, 45, 221–226. [Google Scholar] [CrossRef] [Green Version]
- Nagy, C.D.; Szabó, J.; Szabó, J. A mathematically based classification of root canal curvatures on natural human teeth. J. Endod. 1995, 21, 557–560. [Google Scholar] [CrossRef]
- Dobó-Nagy, C.; Keszthelyi, G.; Szabó, J.; Sulyok, P.; Ledeczky, G. A computerized method for mathematical description of three-dimensional root canal axis. J. Endod. 2000, 26, 639–643. [Google Scholar] [CrossRef]
- Sonntag, D.; Stachniss-Carp, S.; Stachniss, C.; Stachniss, V. Determination of root canal curvatures before and after canal preparation (part II): A method based on numeric calculus. Aust. Endod. J. 2006, 32, 16–25. [Google Scholar] [CrossRef]
- Kato, A.; Ziegler, A.; Utsumi, M.; Ohno, K.; Takeichi, T. Three-dimensional imaging of internal tooth structures: Applications in dental education. J. Oral Biosci. 2016, 58, 100–111. [Google Scholar] [CrossRef] [Green Version]
- Dong, J.; Hong, S.Y.; Hasselgren, G. Theories and algorithms for 3-D root canal model construction. Comput.-Aided Des. 2005, 37, 1177–1189. [Google Scholar] [CrossRef]
- MathWorks, Inc. MATLAB Documentation, Version 9.5 (R2018b); MathWorks, Inc.: Natick, MA, USA, 2018. [Google Scholar]
- Weinert, H.L. Efficient computation for Whittaker–Henderson smoothing. Comput. Stat. Data Anal. 2007, 52, 959–974. [Google Scholar] [CrossRef]
- Peters, O.A.; Peters, C.I.; Schönenberger, K.; Barbakow, F. ProTaper rotary root canal preparation: Effects of canal anatomy on final shape analysed by micro CT. Int. Endod. J. 2003, 36, 86–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Unit | CBCT | µCT |
|---|---|---|---|
| Resolution | mm/pixel | 0.08 | 0.021 |
| Tube voltage | kV | 70 | 80 |
| Tube current | mA | 3 | 0.08 |
| Exposure time | s | 17.5 | 900 |
| Source object distance | mm | 500 | 150 |
| Imaging Technique | Apical Third | Medial Third | Coronal Third | Overall |
|---|---|---|---|---|
| CBCT | 0.15 {0.05} (6.7 {2.2}) | 0.1 {0.03} (10 {2.3}) | 0.12 {0.02} (8.5 {1.7}) | 0.12 {0.02} (8.1 {1.5}) |
| µCT | 0.16 {0.06} (6.3 {2.3}) | 0.09 {0.02} (10.6 {2.6}) | 0.12 {0.02} (8.4 {1.8}) | 0.12 {0.02} (8.5 {1.8}) |
| Imaging Technique | Maximum Curvature | Apical Third | Medial Third | Coronal Third | Location in mm |
|---|---|---|---|---|---|
| CBCT | 0.38 {0.13} (2.6 {0.7}) | 56% | 6% | 38% | 2.5 {3.3} |
| µCT | 0.47 {0.16} (2.1 {0.8}) | 68% | 8% | 24% | 1.4 {2.5} |
| Imaging Technique | Maximum Curvature | Location in mm |
|---|---|---|
| Apical third | ||
| CBCT | 0.33 {0.11} (3 {1}) | 1.2 {0.7} |
| µCT | 0.38 {0.13} (2.6 {0.8}) | 0.9 {0.4} |
| Medial third | ||
| CBCT | 0.21 {0.05} (4.7 {1.2}) | 5 {1.1} |
| µCT | 0.18 {0.04} (5.4 {1.1}) | 5 {1.2} |
| Coronal third | ||
| CBCT | 0.31 {0.08} (3.2 {1.3}) | 8.2 {1.1} |
| µCT | 0.27 {0.08} (3.7 {1.3}) | 9.1 {1} |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kucher, M.; Dannemann, M.; Modler, N.; Haim, D.; Hannig, C.; Weber, M.-T. Continuous Measurement of Three-Dimensional Root Canal Curvature Using Cone-Beam Computed and Micro-Computed Tomography: A Comparative Study. Dent. J. 2020, 8, 16. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8010016
Kucher M, Dannemann M, Modler N, Haim D, Hannig C, Weber M-T. Continuous Measurement of Three-Dimensional Root Canal Curvature Using Cone-Beam Computed and Micro-Computed Tomography: A Comparative Study. Dentistry Journal. 2020; 8(1):16. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8010016
Chicago/Turabian StyleKucher, Michael, Martin Dannemann, Niels Modler, Dominik Haim, Christian Hannig, and Marie-Theres Weber. 2020. "Continuous Measurement of Three-Dimensional Root Canal Curvature Using Cone-Beam Computed and Micro-Computed Tomography: A Comparative Study" Dentistry Journal 8, no. 1: 16. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8010016