Loxoprofen Sodium Versus Diclofenac Potassium for Post-Dental Extraction Pain Relief: A Randomized, Triple-Blind, Clinical Trial

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Setting and Sample Size Calculation
2.2. Ethics Considerations
2.3. Patients’ Recruitment and Inclusion and Exclusion Criteria
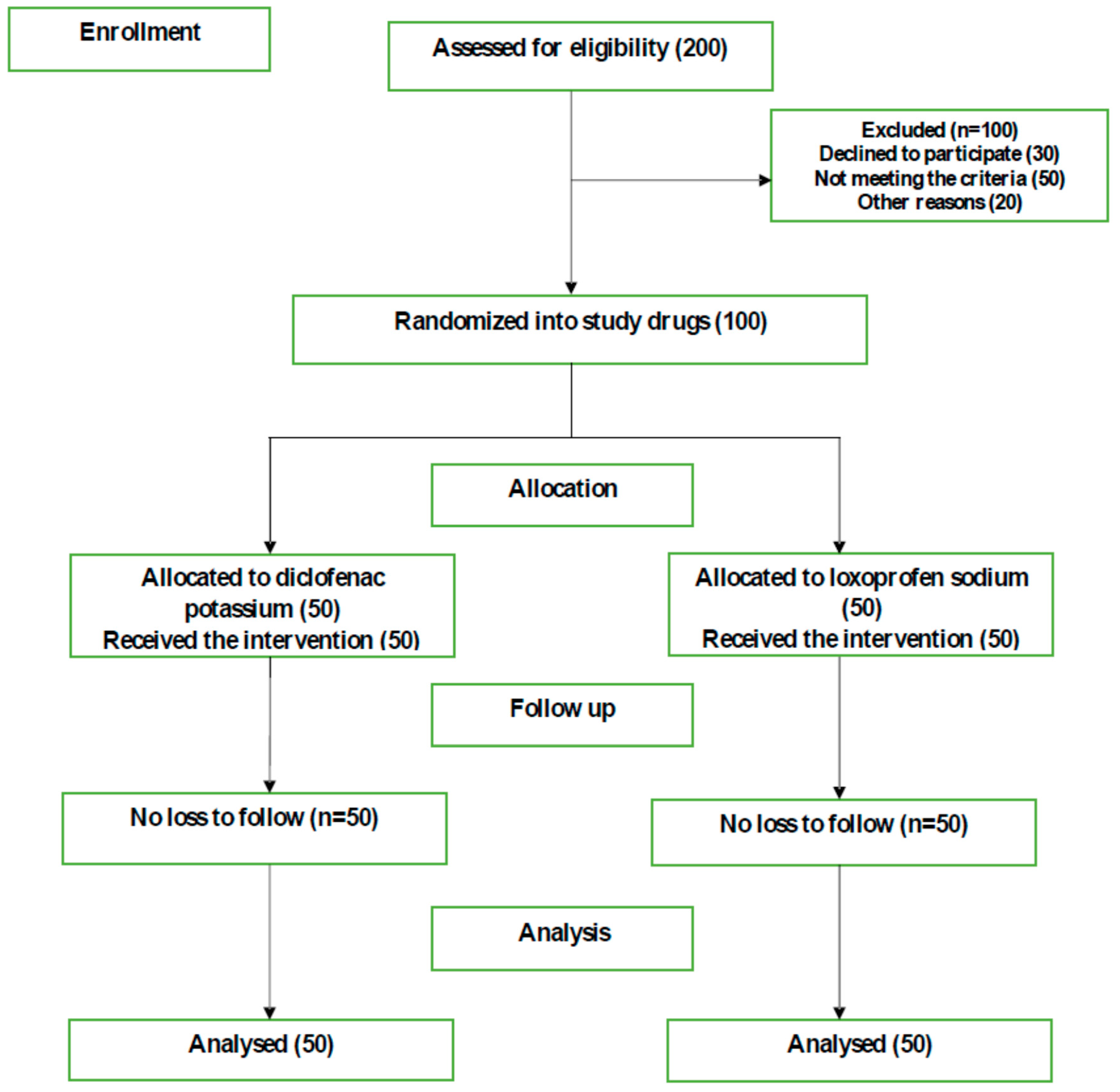
2.4. Randomization and Allocation into the Intervention
2.5. Procedure of Extraction
2.6. Assessment of Post-Operative Dental Pain
2.7. Data Analysis
3. Results
3.1. Sample Characteristics
3.2. Descriptive and Bivariate Comparisons of Loxoprofen and Diclofenac Post-Operative Pain Relief
3.3. Pain Perception within Each Drug Group (Male, Female)
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Taiwo, A.O.; Ibikunle, A.A.; Braimah, R.O.; Sulaiman, O.A.; Gbotolorun, O.M. Tooth extraction: Pattern and etiology from extreme Northwestern Nigeria. Eur. J. Dent. 2017, 11, 335–339. [Google Scholar] [CrossRef] [PubMed]
- Lexander, M.; Krishnan, B.; Shenoy, N. Diabetes mellitus and odontogenic infections—An exaggerated risk? Oral Maxillofac. Surg. 2008, 12, 129. [Google Scholar] [CrossRef] [PubMed]
- Rakhshan, V. Common risk factors for postoperative pain following the extraction of wisdom teeth. J. Korean Assoc. Oral Maxillofac. Surg. 2015, 41, 59–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Moore, R.A.; Derry, S.; McQuay, H.J.; Wiffen, P.J. Single dose oral analgesics for acute postoperative pain in adults. Cochrane Database Syst. Rev. 2011, 9, CD008659. [Google Scholar]
- Neychev, D.; Chenchev, I.; Simitchiev, K. Analysis of Postoperative Pain after Extraction of Impacted Mandibular Third Molars and Administration of Preemptive Analgesia. J. IMAB Annu. Proc. (Sci. Pap.) 2017, 23, 1697–1701. [Google Scholar] [CrossRef] [Green Version]
- Gazal, G.; Al-Samadani, K.H. Comparison of paracetamol, ibuprofen, and diclofenac potassium for pain relief following dental extractions and deep cavity preparations. Saudi Med. J. 2017, 38, 284–291. [Google Scholar] [CrossRef] [PubMed]
- Mehlisch, D.R.; Sollecito, W.A.; Heffrick, J.F.; Leibold, D.G.; Markowitz, R.; Schow, C.E., Jr.; Shultz, R.; Waite, D.E. Multicenter Clinical Trial of Ibuprofen and Acetaminophen in the Treatment of Postoperative Dental Pain. J. Am. Dent. Assoc. 1990, 121, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Morgan, C.R.; Rodd, H.D.; Clayton, N.; Davis, J.B.; Boissonade, F.M. Vanilloid receptor 1 expression in human tooth pulp in relation to caries and pain. J. Orofac. Pain 2005, 19, 248–260. [Google Scholar] [PubMed]
- Moore, R.A.; Derry, S.; Aldington, D.; Wiffen, P.J. Single dose oral analgesics for acute postoperative pain in adults—An overview of Cochrane reviews. Cochrane Database Syst. Rev. 2015, 9, CD008659. [Google Scholar] [CrossRef] [PubMed]
- Meissner, W.; Coluzzi, F.; Fletcher, D.; Huygen, F.; Morlion, B.; Neugebauer, E.; Montes, A.; Pergolizzi, J. Improving the management of post-operative acute pain: Priorities for change. Curr. Med Res. Opin. 2015, 31, 2131–2143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Miller, C.; Newton, S. Pain Perception and Expression: The Influence of Gender, Personal Self-Efficacy, and Lifespan Socialization. Pain Manag. Nurs. 2006, 7, 148–152. [Google Scholar] [CrossRef] [PubMed]
- SAJA PHARMA SAJpcl. ROXONIN® 60 mg Tablets. Available online: https://www.sajapharma.com/roxonin/ (accessed on 24 December 2019).
- Dean, A.G.; Sullivan, K.M.; Soe, M.M. Open Source Epidemiologic Statistics for Public Health: OpenEpi. 2013. Available online: www.OpenEpi.com (accessed on 6 April 2013).
- ASA Physical Status Classification System: American Society of Anesthesiologists. 2014. Available online: https://www.asahq.org/standards-and-guidelines/asa-physical-status-classification-system (accessed on 15 October 2014).
- Salem, S.; Namnakani, A.; Saad, I. Cognizance of Undergraduate Students toward Periodontal Ligament Injection in Exodontia. J. Adv. Med. Med. Res. 2018, 25, 1–9. [Google Scholar] [CrossRef]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthritis Care Res. 2011, 63 (Suppl. 11), S240–S252. [Google Scholar]
- Haefeli, M.; Elfering, A. Pain assessment. Eur. Spine J. 2006, 15 (Suppl. 1), S17–S24. [Google Scholar] [CrossRef] [PubMed]
- Kaler, N.; Makkar, S.; Mann, N.; Pasricha, S.; Dhawan, R. Efficacy of ibuprofen and paracetamol and diclofenac sodium and paracetamol combination on postoperative pain following root canal preparation in a randomized placebo-controlled study. Indian J. Oral Sci. 2012, 3, 19. [Google Scholar] [CrossRef]
- Woo, A.; Lechner, B.; Fu, T.; Wong, C.S.; Chiu, N.; Lam, H.; Pulenzas, N.; Soliman, H.; DeAngelis, C.; Chow, E. Cut points for mild, moderate, and severe pain among cancer and non-cancer patients: A literature review. Ann. Palliat. Med. 2015, 4, 176–183. [Google Scholar] [PubMed]
- World Health Organisation. Cancer Pain Relief: A Guide to Opioid Availability; World Health Organisation: Geneva, Switzerland, 1996. [Google Scholar]
- Whitehead, P.B. Oral NSAIDs versus other oral analgesic agents for acute soft tissue injury. Int. J. Evid. Based Healthc. 2016, 14, 138–139. [Google Scholar] [CrossRef] [PubMed]
- Akinbade, A.O.; Ndukwe, K.C.; Owotade, F.J. Comparative analgesic efficacy and tolerability of celecoxib and tramadol on postoperative pain after mandibular third molar extraction: A double blind randomized controlled trial. Niger. J. Clin. Pract. 2019, 22, 796–800. [Google Scholar] [CrossRef] [PubMed]
- Akbulut, N.; Ustuner, E.; Atakan, C.; Colok, G. Comparison of the effect of Naproxen, Etodolac and Diclofenac on postoperative sequelsfollowing third molar surgery: A randomised, double-blind, crossover study. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e149–e156. [Google Scholar] [CrossRef] [PubMed]
- Martins, L.D.; Rezende, M.; Loguercio, A.D.; Bortoluzzi, M.C.; Reis, A. Analgesic efficacy of ketorolac associated with a tramadol/acetaminophen combination after third molar surgery—A randomized, triple-blind clinical trial. Med. Oral Patol. Oral Cir. Bucal 2018, 24, e96–e102. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Total F (%) | Loxoprofen Sodium F (%) | Diclofenac Potassium F (%) | p-Value a |
|---|---|---|---|---|
| Gender | ||||
| Male | 54 (54) | 26 (52) | 28 (56) | 0.668 |
| Female | 46 (46) | 24 (48) | 22 (44) | |
| Age | ||||
| 18–30 years old | 26 (26) | 14 (28) | 12 (24) | |
| 31–40 years old | 24 (24) | 11 (22) | 13 (26) | 0.499 |
| 41–50 years old | 29 (29) | 17 (34) | 12 (24) | |
| 51+ years old | 21 (21) | 8 (16) | 13 (26) | |
| Type of Extraction | ||||
| Simple | 80 (80) | 38 (76) | 42 (84) | 0.317 |
| Surgical b | 20 (20) | 12 (24) | 8 (16) |
| Variable | No Pain † | Pain ∞ | p-Value |
|---|---|---|---|
| 6 h after extraction | |||
| Loxoprofen Sodium | 31 (62.0) | 19 (38.0) | 0.398 a |
| Diclofenac Potassium | 35 (70.0) | 15 (30.0) | |
| 24 h after extraction | |||
| Loxoprofen Sodium | 36 (72.0) | 14 (28.0) | 0.148 a |
| Diclofenac Potassium | 42 (84.0) | 8 (16.0) | |
| 36 h after extraction | |||
| Loxoprofen Sodium | 33 (66.0) | 17 (34.0) | 0.019 a |
| Diclofenac Potassium | 43 (86.0) | 7 (14.0) | |
| 48 h after extraction | |||
| Loxoprofen Sodium | 41(82.0) | 9 (18.0) | 0.065 a |
| Diclofenac Potassium | 47 (94.0) | 3 (6.0) | |
| 60 h after extraction | |||
| Loxoprofen Sodium | 43 (86.0) | 7 (14.0) | 0.182 a |
| Diclofenac Potassium | 47 (94.0) | 3 (6.0) | |
| 72 h after extraction | |||
| Loxoprofen Sodium | 44 (88.0) | 6 (12.0) | 0.112 b |
| Diclofenac potassium | 49 (98.0) | 1 (2.0) | |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nourwali, I.; Namnakani, A.; Almutairi, M.; Alaufi, A.; Aljohani, Y.; Kassim, S. Loxoprofen Sodium Versus Diclofenac Potassium for Post-Dental Extraction Pain Relief: A Randomized, Triple-Blind, Clinical Trial. Dent. J. 2020, 8, 2. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8010002
Nourwali I, Namnakani A, Almutairi M, Alaufi A, Aljohani Y, Kassim S. Loxoprofen Sodium Versus Diclofenac Potassium for Post-Dental Extraction Pain Relief: A Randomized, Triple-Blind, Clinical Trial. Dentistry Journal. 2020; 8(1):2. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8010002
Chicago/Turabian StyleNourwali, Ibrahim, Arwa Namnakani, Majd Almutairi, Anas Alaufi, Yasser Aljohani, and Saba Kassim. 2020. "Loxoprofen Sodium Versus Diclofenac Potassium for Post-Dental Extraction Pain Relief: A Randomized, Triple-Blind, Clinical Trial" Dentistry Journal 8, no. 1: 2. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8010002