Dentoskeletal Class II Malocclusion: Maxillary Molar Distalization with No-Compliance Fixed Orthodontic Equipment

 ,
,  , and
, and
Abstract
:1. Introduction
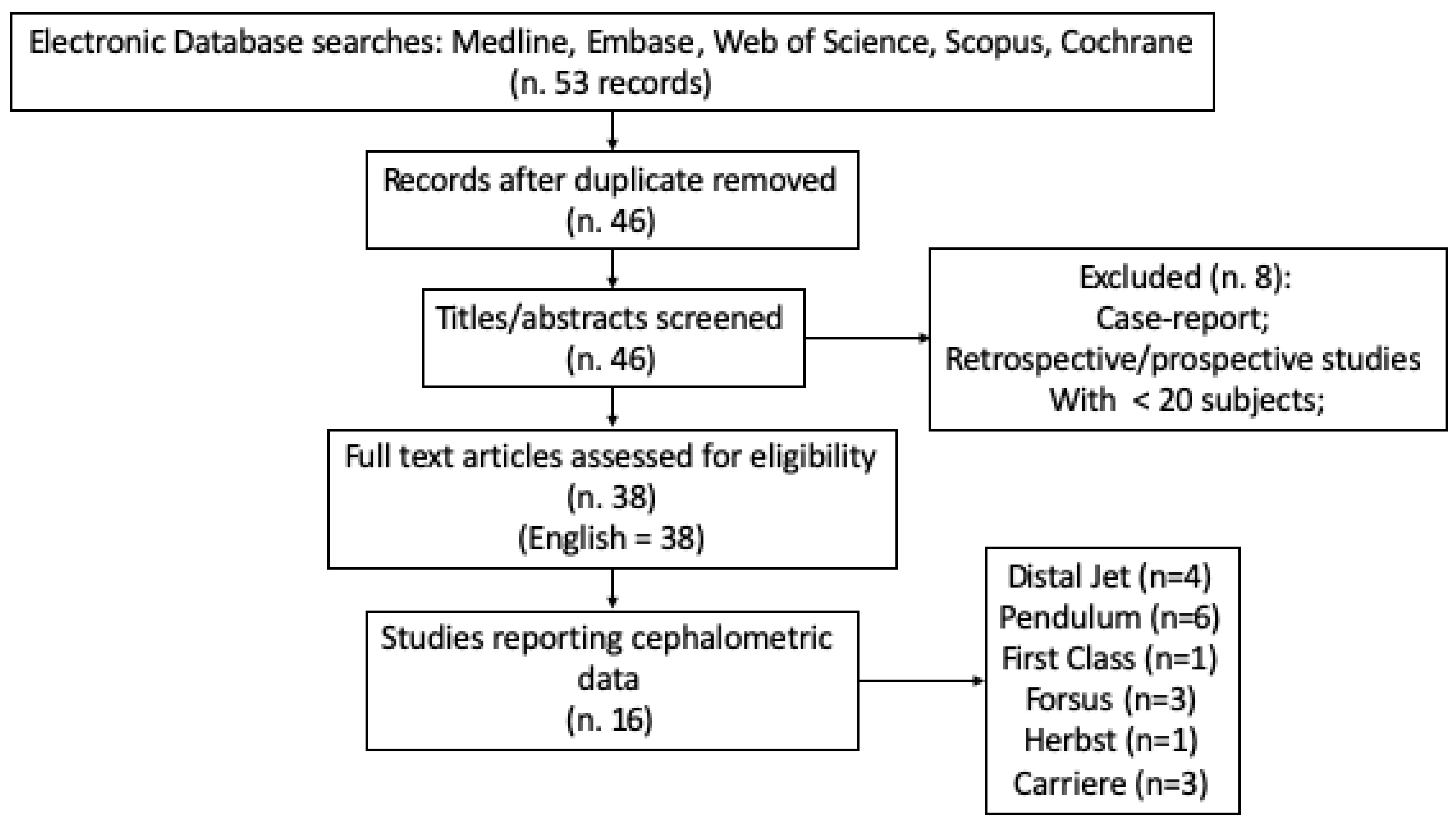
2. Materials and Methods
- -
- Articles published between 2000 and 2019;
- -
- Randomized controlled clinical trials were always included, because they probably contain evidence of acceptable quality;
- -
- Prospective and retrospective studies were accepted only if they included more than 20 treated subjects per intervention group; and with comparisons with an untreated class II malocclusion group, and/or, alternatively, a treated class II malocclusion group;
- -
- Case-reports were also evaluated, and included only if they showed the two basic terms.
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mummolo, S.; Nota, A.; De Felice, M.E.; Marcattili, D.; Tecco, S.; Marzo, G. Periodontal status of buccally and palatally impacted maxillary canines after surgical-orthodontic treatment with open technique. J. Oral Sci. 2018, 60, 552–556. [Google Scholar] [CrossRef]
- Dinoi, M.T.; Mummolo, S.; Monaco, A.; Marchetti, E.; Campanella, V.; Marzo, G. Correction to: Orthodontic treatment of the transposition of a maxillary canine and a first premolar: A case report. J. Med. Case Rep. 2019, 13, 68. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Proffit, W.R.; Fields, H.W.; Moray, L.J. Prevalence of malocclusion and orthodontic treatment need in the United States: Estimates from the NHANES III survey. Int. J. Adult Orthodon. Orthognath. Surg. 1998, 13, 97–106. [Google Scholar]
- Tecco, S.; Festa, F.; Salini, V.; Epifania, E.; D’Attilio, M. Treatment of Joint Pain and Joint Noises Associated with a Recent TMJ Internal Derangement: A Comparison of an Anterior Repositioning Splint, a Full-Arch Maxillary Stabilization Splint, and an Untreated Control Group. Cranio 2004, 22, 209–219. [Google Scholar] [CrossRef]
- Silvestrini-Biavati, A.; Migliorati, M.; Demarziani, E.; Tecco, S.; Silvestrini-Biavati, P.; Polimeni, A.; Saccucci, M. Clinical association between teeth malocclusions, wrong posture and ocular convergence disorders: An epidemiological investigation on primary school children. BMC Pediatr. 2013, 13, 12. [Google Scholar] [CrossRef] [PubMed]
- Mummolo, S.; Tieri, M.; Tecco, S.; Mattei, A.; Albani, F.; Giuca, M.R.; Marzo, G. Clinical evaluation of salivary indices and levels of Streptococcus mutans and Lactobacillus in patients treated with Occlus-o-Guide. Eur. J. Paediatr. Dent. 2014, 15, 367–370. [Google Scholar] [PubMed]
- McNamara, J.A. Components of class II malocclusion in children 8–10 years of age. Angle Orthod. 1981, 51, 177–202. [Google Scholar]
- Alarashi, M.; Franchi, L.; Marinelli, A.; Defraia, E. Morphometric analysis of the transverse dentoskeletal features of class II malocclusion in the mixed dentition. Angle Orthod. 2003, 73, 21–25. [Google Scholar]
- Mummolo, S.; Nota, A.; Caruso, S.; Quinzi, V.; Marchetti, E.; Marzo, G. Salivary Markers and Microbial Flora in Mouth Breathing Late Adolescents. Biomed Res. Int. 2018, 2018, 8698608. [Google Scholar] [CrossRef]
- Franchi, L.; Alvetro, L.; Giuntini, V.; Masucci, C.; Defraia, E.; Baccetti, T. Effectiveness of comprehensive fixed appliance treatment used with the Forsus Fatigue Resistant Device in Class II patients. Angle Orthod. 2011, 81, 678–683. [Google Scholar] [CrossRef] [Green Version]
- Keim, R.G.; Gottlieb, E.L.; Nelson, A.H.; Vogels, D.S. 2008 JCO study of orthodontic diagnosis and treatment procedures, part 1: Results and trends. J. Clin. Orthod. 2008, 42, 625–640. [Google Scholar] [PubMed]
- Dalci, O.; Altug, A.T.; Memikoglu, U.T. Treatment effects of a twin-force bite corrector versus an activator in comparison with an untreated Class II sample: A preliminary report. Aust. Orthod. J. 2014, 30, 45–53. [Google Scholar] [PubMed]
- D’Attilio, M.; Tecco, S.; Filippi, M.R.; Delli Carri, D.; Festa, F. Activation of mandibular growth with the Fräenkel II device: Assessment of effects on the vertical plane | Attivazione della crescita mandibolare mediate il Fräenkel II: Valutazione degli effetti sul piano verticale. Minerva Stomatol. 2001, 50, 247–263. [Google Scholar] [PubMed]
- Koretsi, V.; Zymperdikas, V.F.; Papageorgiou, S.N.; Papadopoulos, M.A. Treatment effects of removable functional appliances in patients with Class II malocclusion: A systematic review and meta-analysis. Eur. J. Orthod. 2015, 37, 418–434. [Google Scholar] [CrossRef]
- Cozza, P.; Baccetti, T.; Franchi, L.; De Toffol, L.; McNamara, J.A. Mandibular changes produced by functional appliances in Class II malocclusion: A systematic review. Am. J. Orthod. Dentofacial Orthop. 2006, 129, 599.e1–12, discussion e1-6. [Google Scholar] [CrossRef] [Green Version]
- Tecco, S.; Baldini, A.; Nakaš, E.; Primozic, J. Interceptive Orthodontics and Temporomandibular Joint Adaptations: Such Evidences? Biomed Res. Int. 2017, 2017, 8953572. [Google Scholar] [CrossRef]
- Tecco, S.; Baldini, A.; Nakaš, E.; Primozic, J. Orthodontics in Growing Patients: Clinical/Biological Evidence and Technological Advancement 2018. Biomed Res. Int. 2018, 2018, 7281846. [Google Scholar] [CrossRef]
- Silvestrini Biavati, A.; Tecco, S.; Migliorati, M.; Festa, F.; Marzo, G.; Gherlone, E.; Tetè, S. Three-dimensional tomographic mapping related to primary stability and structural miniscrew characteristics. Orthod. Craniofac. Res. 2011, 14, 88–99. [Google Scholar] [CrossRef]
- Tecco, S.; Farronato, G.; Salini, V.; Di Meo, S.; Filippi, M.R.; Festa, F.; D’Attilio, M. Evaluation of cervical spine posture after functional therapy with FR-2: A longitudinal study. Cranio 2005, 23, 53–66. [Google Scholar] [CrossRef]
- Tecco, S.; Caputi, S.; Festa, F. Evaluation of cervical posture following palatal expansion: A 12-month follow-up controlled study. Eur. J. Orthod. 2007, 29, 45–51. [Google Scholar] [CrossRef] [Green Version]
- Tecco, S.; Mummolo, S.; Marchetti, E.; Tetè, S.; Campanella, V.; Gatto, R.; Gallusi, G.; Tagliabue, A.; Marzo, G. SEMG activity of masticatory, neck, and trunk muscles during the treatment of scoliosis with functional braces. A longitudinal controlled study. J. Electromyogr. Kinesiol. 2011, 21, 885–892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ciuffolo, F.; Manzoli, L.; Ferritto, A.L.; Tecco, S.; D’Attilio, M.; Festa, F. Surface electromyographic response of the neck muscles to maximal voluntary clenching of the teeth. J. Oral. Rehabil. 2005, 32, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Giuca, M.R.; Pasini, M.; Tecco, S.; Marchetti, E.; Giannotti, L.; Marzo, G. Skeletal maturation in obese patients. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Quinzi, V.; Scibetta, E.T.; Marchetti, E.; Mummolo, S.; Giannì, A.B.; Romano, M.; Beltramini, G.; Marzo, G. Analyze my face. J. Biol. Regul. Homeost. Agents. 2019, 32, 149–158. [Google Scholar]
- Mummolo, S.; Marchetti, E.; Giuca, M.R.; Gallusi, G.; Tecco, S.; Gatto, R.; Marzo, G. In-office bacteria test for a microbial monitoring during the conventional and self-ligating orthodontic treatment. Head Face Med. 2013, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Marure, P.S.; Patil, R.U.; Reddy, S.; Prakash, A.; Kshetrimayum, N.; Shukla, R. The effectiveness of pendulum, K-loop, and distal jet distalization techniques in growing children and its effects on anchor unit: A comparative study. J. Indian Soc. Pedod. Prev. Dent. 2011, 34, 331–340. [Google Scholar]
- Ghosh, J.; Nanda, R.S. Evaluation of an intraoral maxillary molar distalization technique. Am. J. Orthod. Dentofacial Orthop. 1996, 110, 639–646. [Google Scholar] [CrossRef]
- Byloff, F.K.; Darendeliler, M.A.; Clar, E.; Darendeliler, A. Distal molar movement using the pendulum appliance. Part 2: The effects of maxillary molar root uprighting bends. Angle Orthod. 1997, 67, 261–270. [Google Scholar]
- Bussick, T.J.; McNamara, J.A. Dentoalveolar and skeletal changes associated with the pendulum appliance. Am. J. Orthod. Dentofacial Orthop. 2000, 117, 333–343. [Google Scholar] [CrossRef]
- Chaqués-Asensi, J.; Kalra, V. Effects of the pendulum appliance on the dentofacial complex. J. Clin. Orthod. 2001, 35, 254–257. [Google Scholar]
- Fuziy, A.; Rodrigues de Almeida, R.; Janson, G.; Angelieri, F.; Pinzan, A. Sagittal, vertical, and transverse changes consequent to maxillary molar distalization with the pendulum appliance. Am. J. Orthod. Dentofacial Orthop. 2006, 130, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Kalra, V. The K-loop molar distalizing appliance. J. Clin. Orthod. 1995, 29, 298–301. [Google Scholar] [PubMed]
- Ngantung, V.; Nanda, R.S.; Bowman, S.J. Posttreatment evaluation of the distal jet appliance. Am. J. Orthod. Dentofacial Orthop. 2001, 120, 178–185. [Google Scholar] [CrossRef] [PubMed]
- Bolla, E.; Muratore, F.; Carano, A.; Bowman, S.J. Evaluation of maxillary molar distalization with the distal jet: A comparison with other contemporary methods. Angle Orthod. 2002, 72, 481–494. [Google Scholar] [PubMed]
- Chiu, P.P.; McNamara, J.A.; Franchi, L. A comparison of two intraoral molar distalization appliances: Distal jet versus pendulum. Am. J. Orthod. Dentofacial Orthop. 2005, 128, 353–365. [Google Scholar] [CrossRef]
- Ravera, S.; Castroflorio, T.; Garino, F.; Daher, S.; Cugliari, G.; Deregibus, A. Maxillary molar distalization with aligners in adult patients: A multicenter retrospective study. Prog. Orthod. 2016, 17, 12. [Google Scholar] [CrossRef] [Green Version]
- Yin, K.; Han, E.; Guo, J.; Yasumura, T.; Grauer, D.; Sameshima, G. Evaluating the treatment effectiveness and efficiency of Carriere Distalizer: A cephalometric and study model comparison of Class II appliances. Prog. Orthod. 2019, 20, 24. [Google Scholar] [CrossRef]
- Bowman, A.C.; Saltaji, H.; Flores-Mir, C.; Preston, B.; Tabbaa, S. Patient experiences with the Forsus Fatigue Resistant Device. Angle Orthod. 2013, 83, 437–446. [Google Scholar] [CrossRef]
- Sandifer, C.L.; English, J.D.; Colville, C.D.; Gallerano, R.L.; Akyalcin, S. Treatment effects of the Carrière distalizer using lingual arch and full fixed appliances. J. World Fed. Orthod. 2014, 3, e49–e54. [Google Scholar] [CrossRef]
- Fontana, M.; Cozzani, M.; Mutinelli, S.; Spena, R.; Caprioglio, A. Maxillary molar distalization therapy in adult patients: A multicentre study. Orthod. Craniofac. Res. 2015, 18, 221–231. [Google Scholar] [CrossRef]
- Caruso, S.; Nota, A.; Ehsani, S.; Maddalone, E.; Ojima, K.; Tecco, S. Impact of molar teeth distalization with clear aligners on occlusal vertical dimension: A retrospective study. BMC Oral Health 2019, 19, 182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hamilton, C.F.; Saltaji, H.; Preston, C.B.; Flores-Mir, C.; Tabbaa, S. Adolescent patients’ experience with the Carriere distalizer appliance. Eur. J. Paediatr. Dent. 2013, 14, 219–224. [Google Scholar] [PubMed]


{kind=link}
| Distal Jet | Pendulum | Pendulum K | Pendulum BaPa | First Class (Leone) | Forsus Appliance | Herbst Appliance | Carriere Appliance | |
|---|---|---|---|---|---|---|---|---|
| U6 distalization (mm) | 1.9/3.7 [26,33,34,35] | 4 [26,28,29,30,35] (on average) | 4 [26,28,29,31] (on average) | 5.4 [26,28,29,31] (on average) | 4 [40] (on average) | 1.45 [10,38,40] (on average) | 0.2/2.7 [27] | 1.6/2.5 [37,39,42] |
| U6 tip distal (degree) | 3.1/7.3 [26,33,34,35] | 6 [26,28,29,30,35] (on average) | −0.83/+5.89 [26,28,29,31] | - | 4.6 [40] (on average) | 23.92 [10,38,40] (on average) | 5.3/7.9 [27] | 0.2/3.7 [37,39,42] |
| L6 Mesialization (mm) | - | - | - | - | - | 1.7/2.4 [10,38,40] | 1.3/1.7 [27] | 0.9/3.1 [37,39,42] |
| L6 mesioinclination (degree) | - | - | - | - | - | 1.9/4.6 [10,38,40] | 1.2/2.2 [27] | 2.2/6.1 [37,39,42] |
| U1 lingual version (mm) | - | - | - | - | 3.16 [10,38,40] (on average) | 1.1/2.3 [27] | 0.6/2.4 [37,39,42] | |
| U1 lingual inclination (degree) | - | - | - | - | - | 8.94 [10,38,40] (on average) | 7.5/9.6 [27] | 5.4/6.8 [37,39,42] |
| L1 vestibule version (mm) | - | - | - | - | - | 2.34 [10,38,40] (on average) | 1.3/2.4 [27] | 1.9/2.7 [37,39,42] |
| L1 vestibular inclination (degree) | - | - | - | - | - | 9.29 [10,38,40] (on average) | 3.6/8.3 [27] | 6.3 [37,39,42] (on average) |
| U5 mesialization (mm) | 0.4/3 [26,33,34,35] | 1 [26,28,29,30,35] (on average) | 1 [26,28,29,31] (on average) | - | 1.7 [40] (on average) | - | - | - |
| U6 mesial space (mm) | 2.3/6.7 [26,33,34,35] | 5 [26,28,29,30,35] (on average) | 5 [26,28,29,31] (on average) | 5.4 [26,28,29,31] (on average) | 5.7 [40] (on average) | - | - | - |
| U1 vestibular version (mm) | 1.7 [26,33,34,35] (on average) | 1.6 [26,28,29,30,35] (on average) | 0.8 [26,28,29,31] (on average) | - | 0.9 [40] (on average) | - | - | - |
| U5 distalization (mm) | - | - | - | 3.8 [26,28,29,31] (on average) | - | - | - | - |
| U1 vestibular inclination (degree) | - | - | - | - | 2.6 [40] (on average) | - | - | - |
| U1 anchor loss (mm) | - | - | - | 0 [26,28,29,31] (on average) | - | - | - | - |
| U6 = upper first molarL 6 = lower first molar U1 = upper first incisor L1 = lower first incisor U5 = upper second bicuspid | ||||||||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quinzi, V.; Marchetti, E.; Guerriero, L.; Bosco, F.; Marzo, G.; Mummolo, S. Dentoskeletal Class II Malocclusion: Maxillary Molar Distalization with No-Compliance Fixed Orthodontic Equipment. Dent. J. 2020, 8, 26. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8010026
Quinzi V, Marchetti E, Guerriero L, Bosco F, Marzo G, Mummolo S. Dentoskeletal Class II Malocclusion: Maxillary Molar Distalization with No-Compliance Fixed Orthodontic Equipment. Dentistry Journal. 2020; 8(1):26. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8010026
Chicago/Turabian StyleQuinzi, Vincenzo, Enrico Marchetti, Luigi Guerriero, Floriana Bosco, Giuseppe Marzo, and Stefano Mummolo. 2020. "Dentoskeletal Class II Malocclusion: Maxillary Molar Distalization with No-Compliance Fixed Orthodontic Equipment" Dentistry Journal 8, no. 1: 26. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8010026