Formative and Pilot Study for an Effectiveness-Implementation Hybrid Cluster Randomized Trial to Incorporate Oral Health Activities into Pediatric Well-Child Visits


Abstract
:1. Background
2. Methods
2.1. Phase I: Formative Work (Focus Groups and Key Informant Interviews)
2.1.1. Design
2.1.2. Analysis
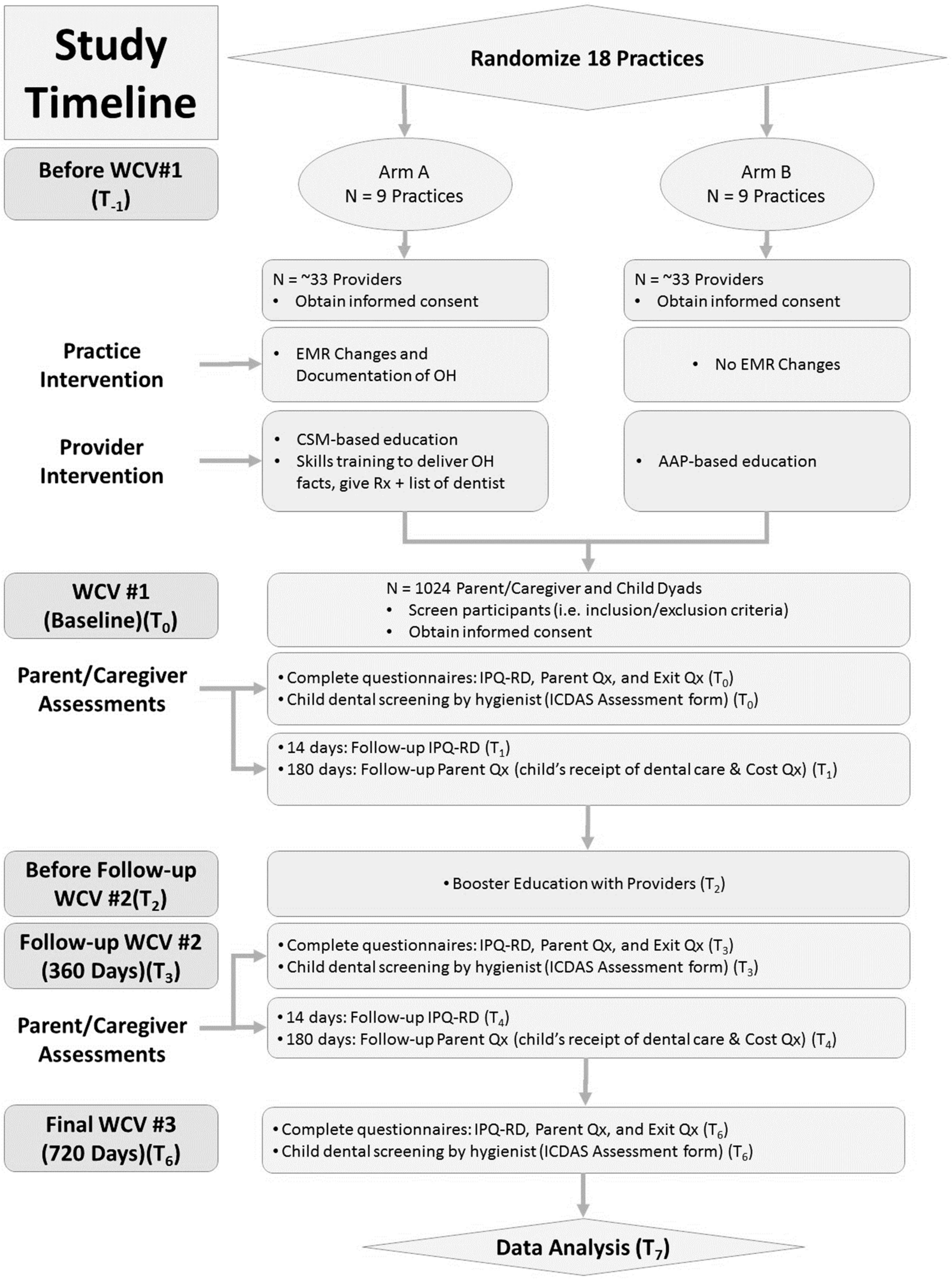
2.2. Phase II: Pilot Study
2.2.1. Study Design and Practice Sites
2.2.2. Practice Intervention
2.2.3. Pediatric Primary Care Providers
2.2.4. Parent/Caregiver Child Dyads
3. Results
3.1. Phase 1: Formative Work (Focus Groups/Key Informant Interviews)
3.1.1. Recruitment
3.1.2. Acceptability
3.1.3. Demand
3.1.4. Implementation and Practicality
3.1.5. Adaptation
3.2. Phase II: Pilot Study
3.2.1. Study Participants
3.2.2. Provider Intervention Training
3.2.3. Practice Intervention
3.2.4. Intervention Fidelity
3.2.5. Results from Parent–Child Pilot Data
3.3. Main Hybrid I Trial
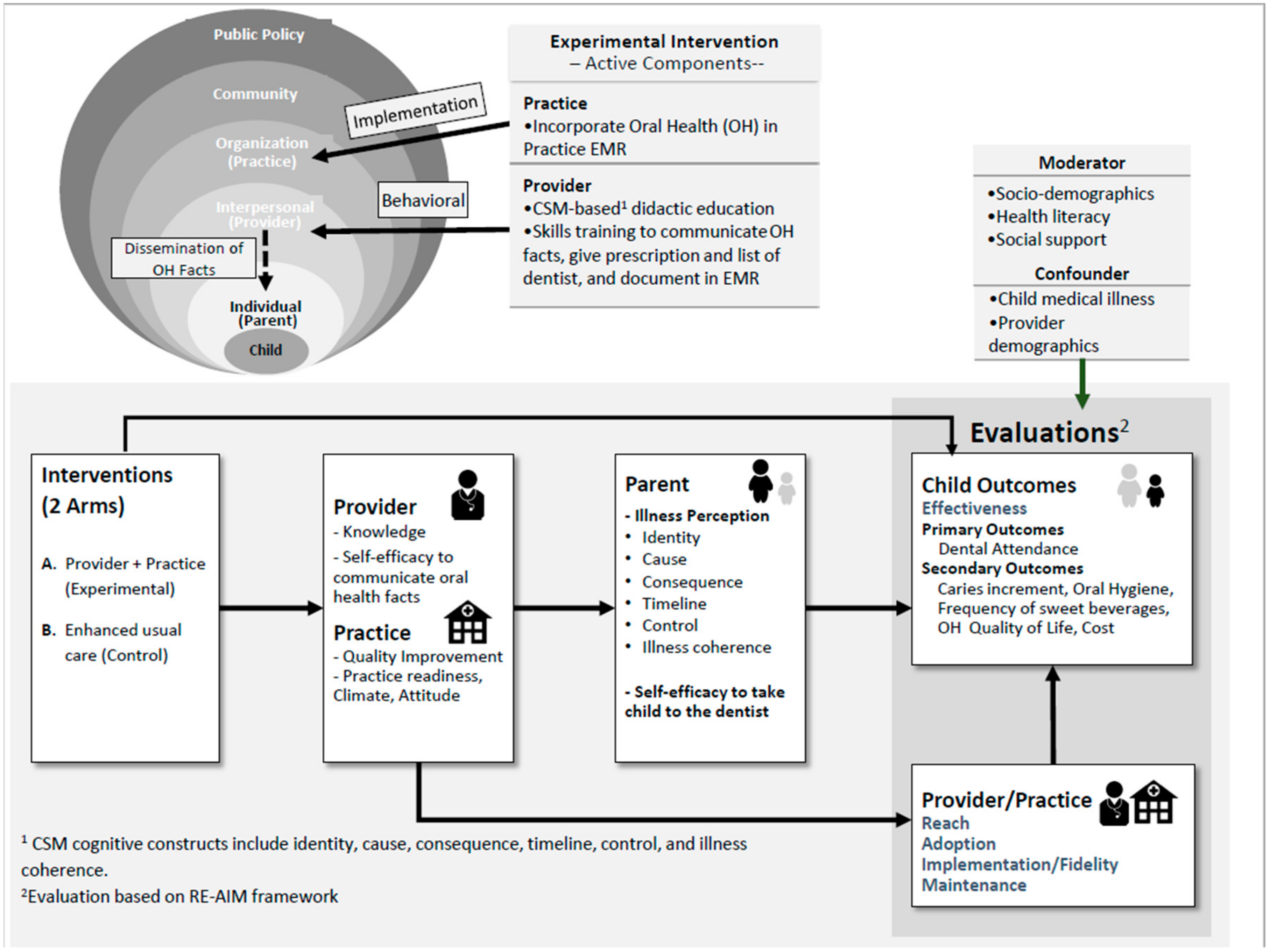
Conceptual Model for the Main Trial
4. Discussion
4.1. Provider Intervention
4.2. Practice Intervention
4.2.1. Recruitment and Retention Strategies
4.2.2. Flow of Intervention Delivery
4.2.3. Other Implementation Considerations
4.2.4. Strengths/Limitations/Challenges
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Ethics Approval and Consent to Participate
Consent for Publication
Availability of Data and Materials
Abbreviations
References
- Jackson, S.L.; Vann, W.F.; Kotch, J.B.; Pahel, B.T.; Lee, J.Y. Impact of poor oral health on children’s school attendance and performance. Am. J. Public Health. 2011, 101, 1900–1906. [Google Scholar] [CrossRef] [PubMed]
- Guarnizo-Herreño, C.C.; Wehby, G.L. Children’s dental health, school performance, and psychosocial well-being. J. Pediatr. 2012, 161, 1153–1159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hooley, M.; Skouteris, H.; Boganin, C.; Satur, J.; Kilpatrick, N. Body mass index and dental caries in children and adolescents: A systematic review of literature published 2004 to 2011. Syst. Rev. 2012, 1, 57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayden, C.; Bowler, J.O.; Chambers, S.; Freeman, R.; Humphris, G.; Richards, D.; Cecil, J.E. Obesity and dental caries in children: A systematic review and meta-analysis. Community Dent. Oral Epidemiol. 2013, 41, 289–308. [Google Scholar] [CrossRef]
- Angelopoulou, M.V.; Beinlich, M.; Crain, A. Early childhood caries and weight status: A systematic review and meta-analysis. Int. J. Paediatr. Dent. 2019, 41, 261–270. Available online: https://www.aapd.org/globalassets/media/publications/open-access/s6_261-70.e24-e25.pdf (accessed on 3 August 2020).
- Dye, B.A.; Mitnik, G.L.; Iafolla, T.J.; Vargas, C.M. Trends in dental caries in children and adolescents according to poverty status in the United States from 1999 through 2004 and from 2011 through 2014. J. Am. Dent. Assoc. 2017, 148, 550–565. [Google Scholar] [CrossRef]
- Nelson, S.; Mandelaris, J.; Ferretti, G.; Heima, M.; Spiekerman, C.; Milgrom, P. School screening and parental reminders in increasing dental care for children in need: A retrospective cohort study. J. Public Health Dent. 2012, 72, 45–52. [Google Scholar] [CrossRef]
- Dye, B.A.; Thornton-Evans, G.; Li, X.; Iafolla, T.J. Dental caries and sealant prevalence in children and adolescents in the United States, 2011–2012. NCHS Data Brief 2015, 191, 1–8. [Google Scholar]
- ADA Health Policy Institute. Dental Care Use among Children: 2016. Available online: https://www.ada.org/~/media/ADA/ScienceandResearch/HPI/Files/HPI_Dental_Care_Use_Children_2016.pdf (accessed on 28 January 2019).
- Divaris, K.; Lee, J.Y.; Baker, A.D.; Gizlice, Z.; Rozier, R.G.; DeWalt, D.A.; Vann, W.F. Influence of caregivers and children’s entry into the dental care system. Pediatrics 2014, 133, 1268–1276. [Google Scholar] [CrossRef] [Green Version]
- American Academy of Pediatric Dentistry. Guideline on infant oral health care. Pediatr. Dent. 2014, 37, 146–150. [Google Scholar]
- Bouchery, E. Utilization of dental services among medicaid-enrolled children. Medicare Medicaid Res. Rev. 2013, 3, E1–E16. [Google Scholar] [CrossRef] [PubMed]
- Bouchery, E. Utilization of Well-Child Care among Medicaid-Enrolled Children. Centers for Medicare and Medicaid Services. Available online: https://www.cms.gov/Research-Statistics-Data-and-Systems/Computer-Data-and-Systems/MedicaidDataSourcesGenInfo/Downloads/MAX_IB10_WellChild.pdf (accessed on 17 December 2019).
- Chou, R.; Cantor, A.; Zakher, B.; Mitchell, J.P.; Pappas, M. Prevention of Dental Caries in Children Younger than 5 Years Old. Agency for Healthcare Research and Quality (US). Available online: http://0-www-ncbi-nlm-nih-gov.brum.beds.ac.uk/pubmed/24872964 (accessed on 22 June 2017).
- Dela Cruz, G.G.; Rozier, R.G.; Slade, G. Dental screening and referral of young children by pediatric primary care providers. Pediatrics 2004, 114, e642–e652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Quinonez, R.; Kranz, A.; Lewis, C.; Barone, L.; Boulter, S.; O’Connor, K.G.; Keels, M.A. Oral health opinions and practices of pediatricians: Updated results from a National Survey. Acad. Pediatr. 2014, 14, 616–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoeft, K.S.; Barker, J.C.; Masterson, E.E. Maternal beliefs and motivations for first dental visit by low-income Mexican American children in California. Pediatr. Dent. 2011, 33, 392–398. [Google Scholar]
- Lewis, C.W.; Linsenmayer, K.A.; Williams, A. Wanting better: A qualitative study of low-income parents about their children’s oral health. Pediatr. Dent. 2010, 32, 518–524. [Google Scholar]
- Kranz, A.M.; Preisser, J.S.; Rozier, R.G. Effects of physician-based preventive oral health services on dental caries. Pediatrics 2015, 136, 107–114. [Google Scholar] [CrossRef] [Green Version]
- Blackburn, J.; Morrisey, M.A.; Sen, B. Outcomes associated with early preventive dental care among medicaid-enrolled children in Alabama. JAMA Pediatr. 2017, 171, 335–341. [Google Scholar] [CrossRef]
- Hooley, M.; Skouteris, H.; Boganin, C.; Satur, J.; Kilpatrick, N. Parental influence and the development of dental caries in children aged 0–6 years: A systematic review of the literature. J. Dent. 2012, 40, 873–885. [Google Scholar] [CrossRef]
- Leventhal, H.; Benyamini, Y.; Brownlee, S.; Diefenbach, M.; Leventhal, E.; Patrick-Miller, L.; Robitaille, C.; Petrie, K.J.; Weinman, J.A. Illness Representations: Theoretical Foundations. Percept. Health Illn. 1997, 19–45. Available online: https://books.google.co.jp/books?hl=en&lr=&id=Z57ARB4gOasC&oi=fnd&pg=PA19&dq=Illness+representations:+Theoretical+foundations&ots=lxmxH5XNyq&sig=OXjjb3zoX-f0eM0w1OAZthWTatA#v=onepage&q=Illness%20representations%3A%20Theoretical%20foundations&f=false (accessed on 31 August 2020).
- Leventhal, H.; Brissette, I. The common-sense model of self-regulation of health and illness. In The Self-Regulation of Health and Illness Behavior; Cameron, L.D., Ed.; Routledge: London, UK, 2003; pp. 42–65. [Google Scholar]
- Nelson, S.; Slusar, M.B.; Albert, J.M.; Riedy, C.A. Do baby teeth really matter? Changing parental perception and increasing dental care utilization for young children. Contemp. Clin. Trials 2017, 59, 13–21. [Google Scholar] [CrossRef]
- Yevlahova, D.; Satur, J. Models for individual oral health promotion and their effectiveness: A systematic review. Aust. Dent. J. 2009, 54, 190–197. [Google Scholar] [CrossRef]
- Cascaes, A.M.; Bielemann, R.M.; Clark, V.L.; Barros, J.D. Effectiveness of motivational interviewing at improving oral health: A systematic review. Rev. Saude Publ. 2014, 48, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Curran, G.M.; Bauer, M.; Mittman, B.; Pyne, J.D.; Stetler, C. Effectiveness-implementation hybrid designs: Combining elements of clinical effectiveness and implementation research to enhance public health impact. Med. Care 2012, 50, 217–226. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Basch, C.E. Focus group interview: An underutilized research technique for improving theory and practice in health education. Health Educ. Q. 1987, 14, 411–448. [Google Scholar] [CrossRef] [PubMed]
- Sussman, S.; Burton, D.; Dent, C.W.; Stacy, A.W.; Flay, B.R. Use of focus groups in developing an adolescent tobacco use cessation program: Collective norm effects1. J. Appl. Soc. Psychol. 1991, 21, 1772–1782. [Google Scholar] [CrossRef]
- Bowen, D.J.; Kreuter, M.; Spring, B.; Cofta-Woerpel, L.; Linnan, L.; Weiner, D.; Bakken, S.; Kaplan, C.P.; Squiers, L.; Fabrizio, C.; et al. How we design feasibility studies. Am. J. Prev. Med. 2009, 36, 452–457. [Google Scholar] [CrossRef] [Green Version]
- Bailey, D.M.; Jackson, J.M. Qualitative data analysis: Challenges and dilemmas related to theory and method. Am. J. Occup. Ther. 2003, 57, 57–65. [Google Scholar] [CrossRef] [Green Version]
- AAP. Protecting All Children’s Teeth: A Pediatric Oral Health Training Program. Available online: https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/Oral-Health/Pages/Protecting-All-Childrens-Teeth.aspx (accessed on 23 June 2017).
- National Maternal and Child Oral Health Resource Center. A Health Professionals Guide to Pediatric Oral Health Management. Georgetown University: National Maternal and Child Oral Health Resource CenterGeorgetown University. Available online: https://www.mchoralhealth.org/PediatricOH/index.htm (accessed on 29 January 2019).
- Vujicic, M.; Nasseh, K. A decade in dental care utilization among adults and children (2001–2010). Health Serv. Res. 2014, 49, 460–480. [Google Scholar] [CrossRef] [Green Version]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [Green Version]
- Glasgow, R.E.; McKay, H.G.; Piette, J.D.; Reynolds, K.D. The RE-AIM framework for evaluating interventions: What can it tell us about approaches to chronic illness management? Patient Educ. Couns. 2001, 44, 119–127. [Google Scholar] [CrossRef]
- Ismail, A.I.; Nainar, S.M.; Sohn, W. Children’s first dental visit: Attitudes and practices of US pediatricans and family physicians. Pediatr. Dent. 2003, 25, 425–430. [Google Scholar]
- Vann, W.F.; Divaris, K.; Gizlice, Z.; Baker, A.D.; Lee, J.Y. Caregivers’ health literacy and their young children’s oral-health-related expenditures. J. Dent. Res. 2013, 92, S55–S62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duijster, D.; van Loveren, C.; Dusseldorp, E.; Verrips, G.H.W. Modelling community, family, and individual determinants of childhood dental caries. Eur. J. Oral Sci. 2014, 122, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Nelson, S.; Lee, W.; Albert, J.M.; Singer, L.T. Early maternal psychosocial factors are predictors for adolescent caries. J. Dent. Res. 2012, 91, 859–864. [Google Scholar] [CrossRef] [Green Version]
- Chi, D.L.; Raklios, N.A. The relationship between body system-based chronic conditions and dental utilization for Medicaid-enrolled children: A retrospective cohort study. BMC Oral Health 2012, 12, 28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chi, D.L.; Momany, E.T.; Neff, J.; Jones, M.P.; Warren, J.J.; Slayton, R.L.; Weber-Gasparoni, K.; Damiano, P.C. Impact of chronic condition status and severity on the time to first dental visit for newly Medicaid-enrolled children in Iowa. Health Serv. Res. 2011, 46, 572–595. [Google Scholar] [CrossRef]
- Brown, A.H.; Cohen, A.N.; Chinman, M.J.; Kessler, C.; Young, A.S. EQUIP: Implementing chronic care principles and applying formative evaluation methods to improve care for schizophrenia: QUERI series. Implement. Sci. 2008, 3, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cully, J.A.; Breland, J.Y.; Robertson, S.; Utech, A.E.; Hundt, N.; Kunik, M.E.; Petersen, N.J.; Masozera, N.; Rao, R.; Naik, A.D. Behavioral health coaching for rural veterans with diabetes and depression: A patient randomized effectiveness implementation trial. BMC Health Serv. Res. 2014, 14, 191. [Google Scholar] [CrossRef]
- Petrie, K.J.; Cameron, L.D.; Ellis, C.J.; Buick, D.; Weinman, J. Changing illness perceptions after myocardial infarction: An early intervention randomized controlled trial. Psychosom. Med. 2002, 64, 580–586. [Google Scholar] [CrossRef]
- Davies, M.J.; Heller, S.; Skinner, T.C.; Campbell, M.J.; Carey, M.E.; Cradock, S.; Dallosso, H.M.; Daly, H.; Doherty, Y.; Eaton, S.; et al. Effectiveness of the diabetes education and self management for ongoing and newly diagnosed (DESMOND) programme for people with newly diagnosed type 2 diabetes: Cluster randomised controlled trial. BMJ 2008, 336, 491–495. [Google Scholar] [CrossRef] [Green Version]
- Glattacker, M.; Heyduck, K.; Meffert, C. Illness beliefs, treatment beliefs and information needs as starting points for patient information—Evaluation of an intervention for patients with chronic back pain. Patient Educ. Couns. 2012, 86, 378–389. [Google Scholar] [CrossRef]
- Lewis, C.; Lynch, H.; Richardson, L. Fluoride varnish use in primary care: What do providers think? Pediatrics 2005, 115, e69–e76. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bernstein, J.; Gebel, C.; Vargas, C.; Geltman, P.; Walter, A.; Garcia, R.I.; Tinanoff, N. Integration of oral health into the well-child visit at federally qualified health centers: Study of 6 clinics, August 2014–March 2015. Prev. Chronic Dis. 2016, 13, 160066. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kressin, N.R.; Nunn, M.E.; Singh, H.; Orner, M.B.; Pbert, L.; Hayes, C.; Culler, C.; Glicken, S.R.; Palfrey, S.; Geltman, P.L.; et al. Pediatric clinicians can help reduce rates of early childhood caries: Effects of a practice based intervention. Med. Care 2009, 47, 1121–1128. [Google Scholar] [CrossRef] [Green Version]
- Dooley, D.; Moultrie, N.M.; Heckman, B.; Gansky, S.A.; Potter, M.B.; Walsh, M.M. Oral health prevention and toddler well-child care: Routine integration in a safety net system. Pediatrics 2016. [Google Scholar] [CrossRef] [Green Version]
- Nicholson, L.M.; Schwirian, P.M.; Klein, E.G.; Skybo, T.; Murray-Johnson, L.; Eneli, I.; Boettner, B.; French, G.M.; Groner, J.A. Recruitment and retention strategies in longitudinal clinical studies with low-income populations. Contemp. Clin. Trials 2011, 32, 353–362. [Google Scholar] [CrossRef] [Green Version]
- BeLue, R.; Taylor-Richardson, K.D.; Lin, J.; Rivera, A.T.; Grandison, D. African Americans and participation in clinical trials: Differences in beliefs and attitudes by gender. Contemp. Clin. Trials 2006, 27, 498–505. [Google Scholar] [CrossRef]
- Smith, Y.R.; Johnson, A.M.; Newman, L.A.; Greene, A.; Johnson, T.R.B.; Rogers, J.L. Perceptions of clinical research participation among African American women. J. Women’s Health 2007, 16, 423–428. [Google Scholar] [CrossRef] [Green Version]
- Close, K.; Rozier, R.G.; Zeldin, L.P.; Gilbert, A.R. Barriers to the adoption and implementation of preventive dental services in primary medical care. Pediatrics 2010, 125, 509–517. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Feasibility Objective | Recommendations Based on Focus Groups/Key Informant Interviews | Changes Made to the Feasibility/Main Study |
|---|---|---|
| Acceptability | Community members and parent/caregivers suggested that it is important to discuss oral health at the WCV Barriers to caregivers participating in research included:
|
|
| Demand | What primary care providers informed that they do not know about:
|
|
| Implementation | Important OH information to be communicated by providers at WCV:
|
|
| Practicality |
|
|
| Adaptation | OH documentation in EMR should be:
|
|
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nelson, S.; Slusar, M.B.; Curtan, S.; Selvaraj, D.; Hertz, A. Formative and Pilot Study for an Effectiveness-Implementation Hybrid Cluster Randomized Trial to Incorporate Oral Health Activities into Pediatric Well-Child Visits. Dent. J. 2020, 8, 101. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8030101
Nelson S, Slusar MB, Curtan S, Selvaraj D, Hertz A. Formative and Pilot Study for an Effectiveness-Implementation Hybrid Cluster Randomized Trial to Incorporate Oral Health Activities into Pediatric Well-Child Visits. Dentistry Journal. 2020; 8(3):101. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8030101
Chicago/Turabian StyleNelson, Suchitra, Mary Beth Slusar, Shelley Curtan, David Selvaraj, and Andrew Hertz. 2020. "Formative and Pilot Study for an Effectiveness-Implementation Hybrid Cluster Randomized Trial to Incorporate Oral Health Activities into Pediatric Well-Child Visits" Dentistry Journal 8, no. 3: 101. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8030101