Adjunctive Use of Lasers in Peri-Implant Mucositis and Peri-Implantitis Treatment: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
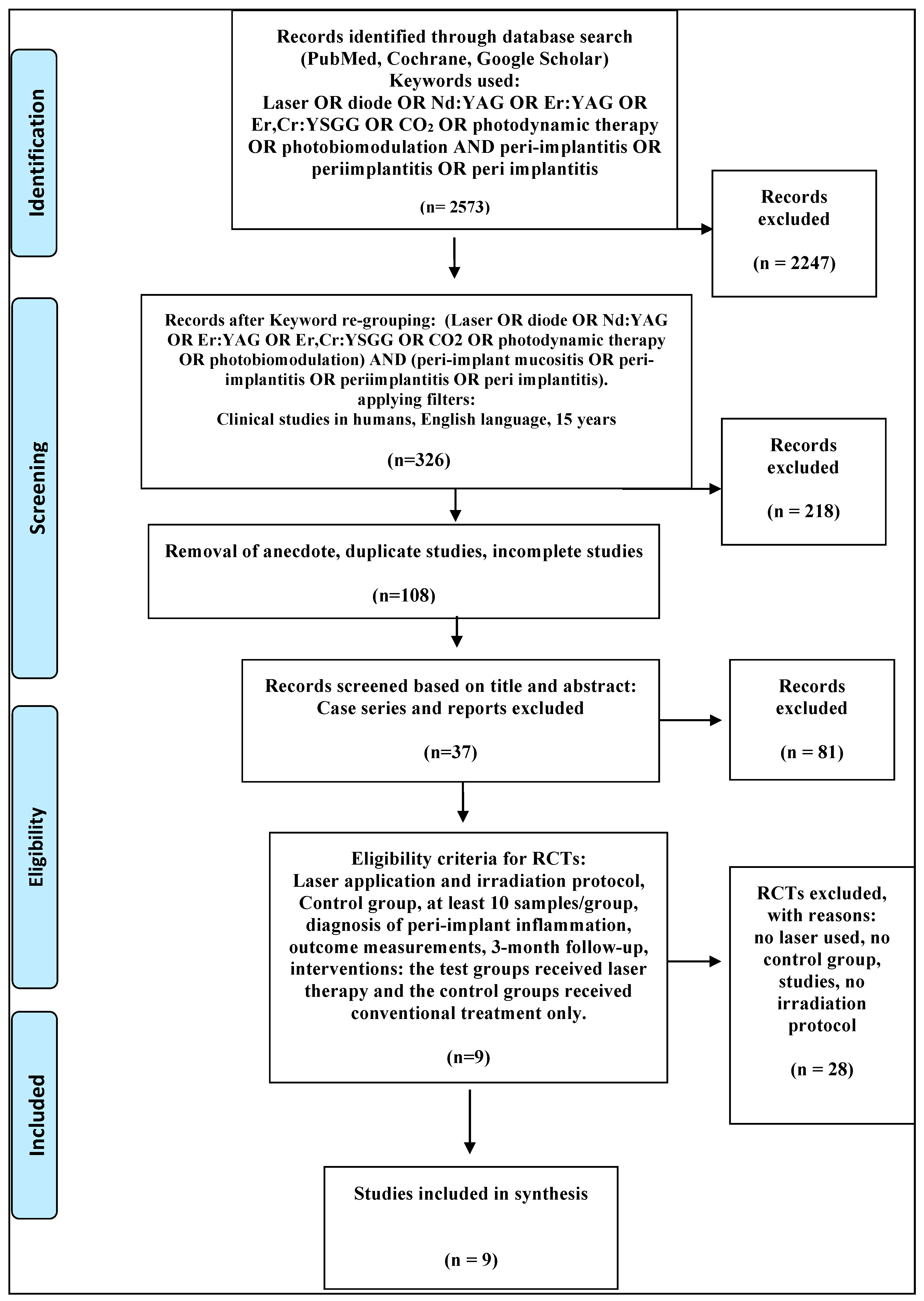
2. Materials and Methods
2.1. Search Strategy
- RCTs;
- At least single blinding applied;
- At least 10 patients with one or more implants each;
- Type of inflammation: mucositis or peri-implantitis and criteria of diagnosis required;
- Laser used in test group;
- Interventions: the test groups received laser therapy additional to conventional treatment and the control groups received conventional treatment only;
- Follow up: at least three months.
- Studies using LEDs as the light source (only applicable to aPDT studies);
- Studies without a control group.
2.2. Data Extraction
- Publication details (authors, year of publication);
- Type of peri-implant inflammation/diagnosis;
- Treatment approach (non-surgical/surgical: regenerative or resective);
- Number of patients/groups of study;
- Number and type of implants;
- Method of implant surface decontamination;
- Wavelength and irradiation protocol;
- Follow-up;
- Bleeding on probing;
- Plaque index;
- Probing depth;
- Clinical attachment level;
- Gingival recession;
- Bone level.
2.3. Quality Paper Assessment
- Population = adults with peri-implantitis or peri-implant mucositis;
- Intervention = Mechanical debridement + Laser (both in surgical and non-surgical modalities);
- Compared with = Mechanical debridement alone (both in surgical and non-surgical modalities);
- Outcome of interest = Pain; Healing; probing pocket depth (PPD), bleeding index (BI), etc.;
- Study type = Randomized Controlled Trials.
- Randomization and blinding;
- Comparability of groups at baseline (e.g., severity of disease);
- Description of treatment and irradiation protocol;
- Clinical measurements at baseline and at follow up;
- Radiographic evaluation at baseline and at follow up.
- (1)
- High quality: 4–5
- (2)
- Medium quality: 2–3
- (3)
- Low quality: 1
2.4. Scientific Evidence
- Strong scientific evidence: the conclusion is corroborated by at least two studies;
- Contradictory scientific evidence: the conclusion is corroborated by studies whose findings contradict each other.
3. Results
3.1. Primary Outcome
3.2. Quality Assessment
3.3. Data Presentation
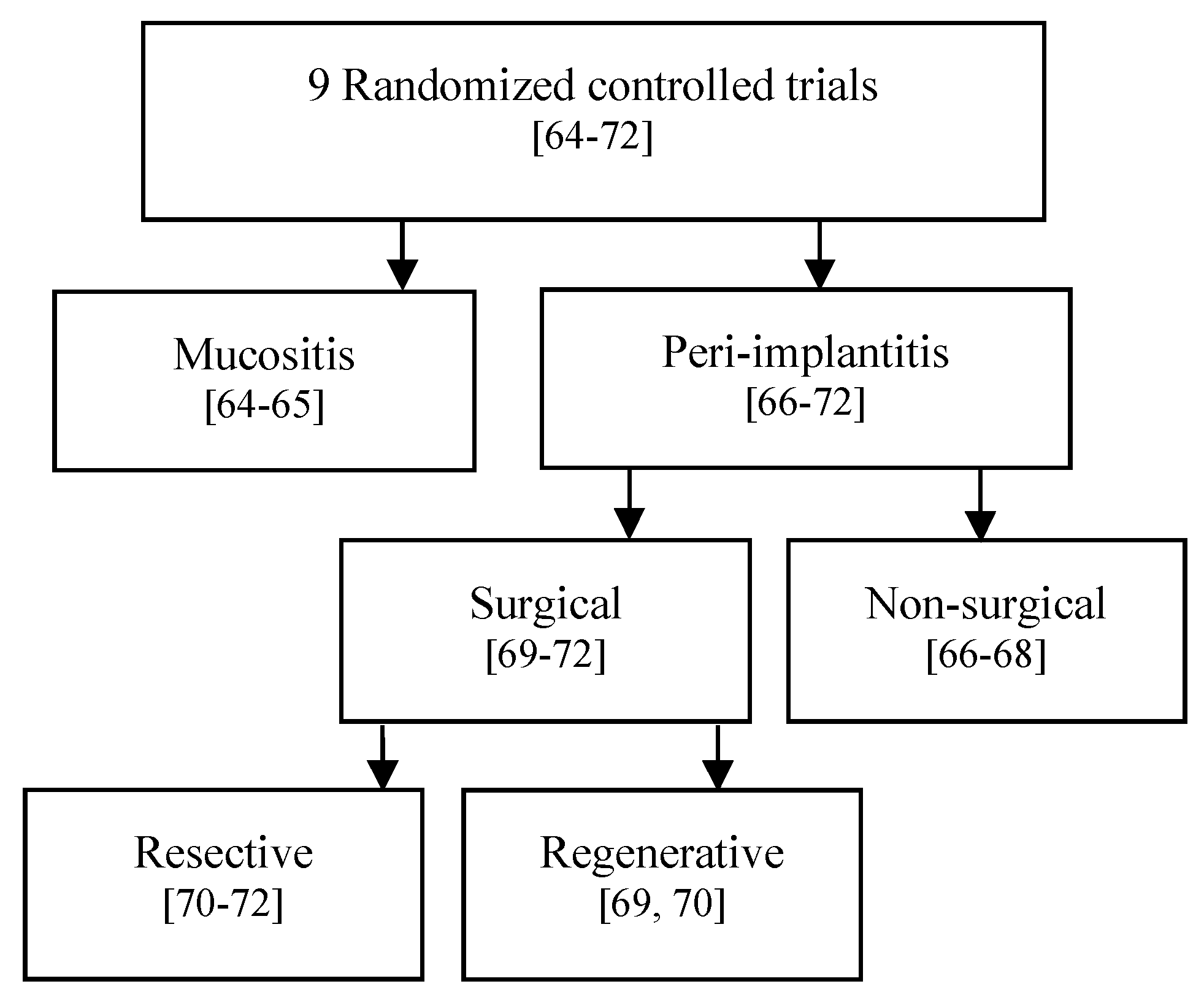
3.3.1. Comparative Assessment per Each Pathological Condition (Figure 2)
- a.
- Mucositis.
- b.
- Non-surgical PI.
- c.
- Surgical PI.
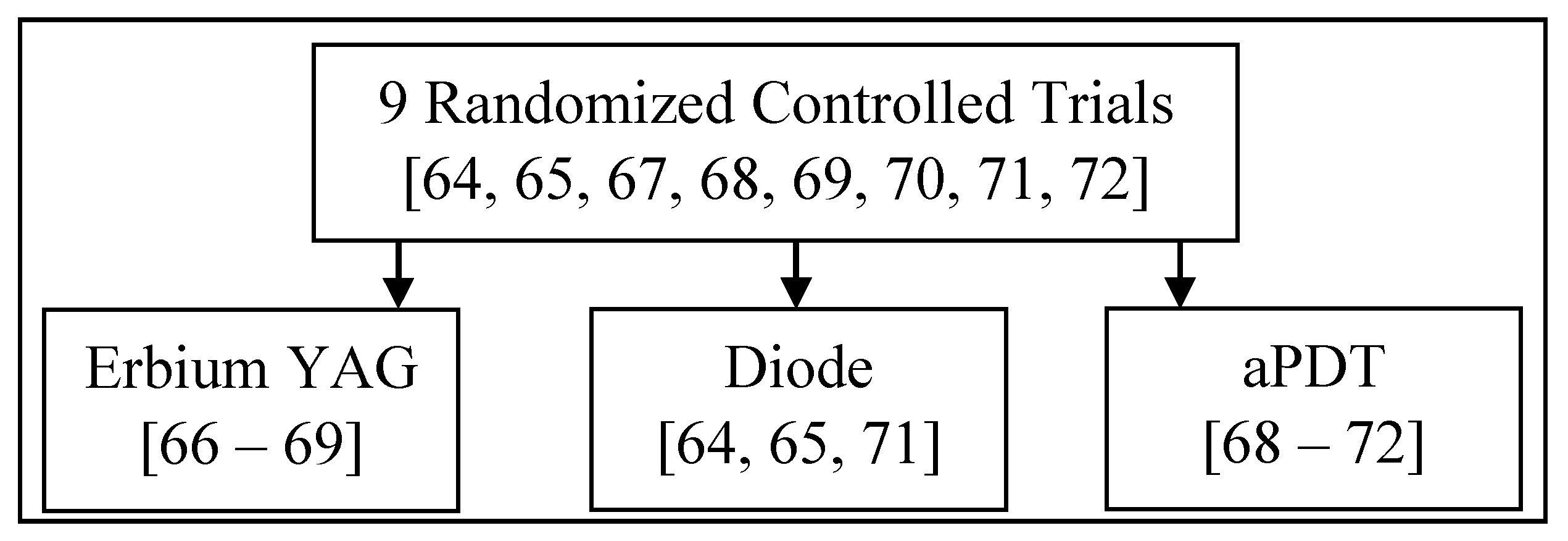
3.3.2. Comparative Assessment per Laser Wavelength/Type of Application (Figure 3)
- a.
- Diode lasers in peri-implant inflamed tissues.
- b.
- Er: YAG lasers in peri-implant inflamed tissues.
- c.
- aPDT application in peri-implant inflamed tissues.
4. Discussion
- Assessment of etiology
- Assessment of implant survivability
- Elimination of biofilm and debridement
- Re-establishment of biocompatibility
- Re-osseointegration as required
- Re-establishment of function
- On-going review and maintenance
4.1. Peri-Implant Mucositis
4.2. Non-Surgical Treatment for PI
4.3. Surgical Procedures for PI
4.3.1. Resective Approach
4.3.2. Regenerative Approach
4.4. Ideal Reporting of Irradiation Protocols
- Intrinsic properties such as laser manufacturer, mode, type of laser, wavelength, delivery system, emission mode, energy distribution and energy delivery.
- Adjustable parameters such as pulse width, average power, pulse repetition rate, on-off- time or continuous mode, tip to tissue distance or in contact mode, focus or defocused mode, beam divergence, fiber or spot diameter at focus, length of treatment and speed of movement.
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Berglundh, T.; Persson, L.; Klinge, B. A systematic review of the incidence of biological and technical complications in implant dentistry reported in prospective longitudinal studies of at least 5 years. J. Clin. Periontol. 2002, 29, 197–212. [Google Scholar] [CrossRef] [PubMed]
- Sinjab, K.; Garaicoa-Pazmino, C.; Wang, H. Decision Making for Management of Periimplant Diseases. Implant Dent. 2018, 27, 276–281. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.; Zarb, G. Criteria for success of osseointegrated endosseous implants. J. Prosthet. Dent. 1989, 62, 567–572. [Google Scholar] [CrossRef]
- Mombelli, A.; Müller, N.; Cionca, N. The epidemiology of peri-implantitis. Clin. Oral Implant. Res. 2012, 23, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Smeets, R.; Henningsen, A.; Jung, O.; Heiland, M.; Hammächer, C.; Stein, J. Definition, etiology, prevention and treatment of peri-implantitis-A review. Head Face Med. 2014, 10, 34. [Google Scholar] [CrossRef] [Green Version]
- Degidi, M.; Artese, L.; Piattelli, A.; Scarano, A.; Shibli, J.; Piccirilli, M.; Perrotti, V.; Iezzi, G. Histological and immunohistochemical evaluation of the peri-implant soft tissues around machined and acid-etched titanium healing abutments: A prospective randomised study. Clin. Oral Investig. 2011, 16, 857–866. [Google Scholar] [CrossRef]
- Renvert, S.; Polyzois, I. Clinical approaches to treat peri-implant mucositis and peri-implantitis. Periodontology 2000 2015, 68, 369–404. [Google Scholar] [CrossRef]
- Conrads, G. Aktuelle Aspekte der Periimplantitis–Ätiologie, Risiken, mikrobiologische Diagnostik und antiinfektiöse Therapie. ZWR DDZ 2011, 120, 284–296. [Google Scholar] [CrossRef]
- Wilson, V. An Insight into Peri-Implantitis: A Systematic Literature Review. Prim. Dent. J. 2013, 2, 69–73. [Google Scholar] [CrossRef]
- Schwarz, F.; Becker, J. Periimplantäre Entzündungen. Zahnmed. up2date 2008, 2, 53–69. [Google Scholar] [CrossRef]
- Sorsa, T.; Tervahartiala, T.; Leppilahti, J.; Hernandez, M.; Gamonal, J.; Tuomainen, A.; Lauhio, A.; Pussinen, P.; Mäntylä, P. Collagenase-2 (MMP-8) as a point-of-care biomarker in periodontitis and cardiovascular diseases. Therapeutic response to non-antimicrobial properties of tetracyclines. Pharmacol. Res. 2011, 63, 108–113. [Google Scholar] [CrossRef]
- Lindhe, J.; Meyle, J. Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J. Clin. Periodontol. 2008, 35, 282–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Froum, S.; Rosen, P. Reentry Evaluation Following Treatment of Peri-implantitis with a Regenerative Approach. Int. J. Periodontics Restor. Dent. 2014, 34, 47–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosen, P.; Clem, D.; Cochran, D.; Froum, S.; McAllister, B.; Renvert, S.; Wang, H.L. Academy Report: Peri-Implant Mucositis and Peri-Implantitis: A Current Understanding of Their Diagnoses and Clinical Implications. J. Periodontol. 2013, 84, 436–443. [Google Scholar] [CrossRef]
- Renvert, S.; Roos-Jansåker, A.; Claffey, N. Non-surgical treatment of peri-implant mucositis and peri-implantitis: A literature review. J. Clin. Periodontol. 2008, 35, 305–315. [Google Scholar] [CrossRef] [PubMed]
- Figuero, E.; Graziani, F.; Sanz, I.; Herrera, D.; Sanz, M. Management of peri-implant mucositis and peri-implantitis. Periodontology 2000 2014, 66, 255–273. [Google Scholar] [CrossRef] [PubMed]
- De Paula Eduardo, C.; Aranha, A.; Simões, A.; Bello-Silva, M.; Ramalho, K.; Esteves-Oliveira, M.; De Freitas, P.; Marotti, J.; Tunér, J. Laser treatment of recurrent herpes labialis: A literature review. Lasers Med. Sci. 2014, 29, 1517–1529. [Google Scholar] [CrossRef]
- Kazem Shakouri, S.; Soleimanpour, J.; Salekzamani, Y.; Oskuie, M. Effect of low-level laser therapy on the fracture healing process. Lasers Med. Sci. 2009, 25, 73–77. [Google Scholar] [CrossRef]
- García-Morales, J.; Tortamano-Neto, P.; Todescan, F.; De Andrade, J.; Marotti, J.; Zezell, D. Stability of dental implants after irradiation with an 830-nm low-level laser: A double-blind randomized clinical study. Lasers Med. Sci. 2011, 27, 703–711. [Google Scholar] [CrossRef]
- Eduardo, F.; Mehnert, D.; Monezi, T.; Zezell, D.; Schubert, M.; Eduardo, C.; Marques, M. Cultured epithelial cells response to phototherapy with low intensity laser. Lasers Surg. Med. 2007, 39, 365–372. [Google Scholar] [CrossRef]
- Guzzardella, G.; Torricelli, P.; Nicoli-Aldini, N.; Giardino, R. Osseointegration of endosseous ceramic implants after postoperative low-power laser stimulation: An in vivo comparative study. Clin. Oral Implant. Res. 2003, 14, 226–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pinheiro, A.; Gerbi, M.; Ponzi, E.; Ramalho, L.; Marques, A.; Carvalho, C.; Santos, R.; Oliveira, P.; Nóia, M. Infrared Laser Light Further Improves Bone Healing When Associated with Bone Morphogenetic Proteins and Guided Bone Regeneration: An in Vivo Study in a Rodent Model. Photomed. Laser Surg. 2008, 26, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Dortbudak, O.; Haas, R.; Mailath-Pokorny, G. Effect of low-power laser irradiation on bony implant sites. Clin. Oral Implant. Res. 2002, 13, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Arnabat-Domínguez, J.; Bragado-Novel, M.; España-Tost, A.; Berini-Aytés, L.; Gay-Escoda, C. Advantages and esthetic results of erbium, chromium:yttrium–scandium–gallium–garnet laser application in second-stage implant surgery in patients with insufficient gingival attachment: A report of three cases. Lasers Med. Sci. 2009, 25, 459–464. [Google Scholar] [CrossRef] [PubMed]
- Parker, S. Surgical laser use in implantology and endodontics. Br. Dent. J. 2007, 202, 377–386. [Google Scholar] [CrossRef]
- Eyrich, G.; Sailer, H.; Nubler-Moritz, M.; Bruder, E. Hard tissue cutting and drilling with lasers. Int. J. Oral Maxillofac. Surg. 1999, 28, 115–116. [Google Scholar] [CrossRef]
- Kimura, Y.; Yu, D.; Fujita, A.; Yamashita, A.; Murakami, Y.; Matsumoto, K. Effects of Erbium, Chromium:YSGG Laser Irradiation on Canine Mandibular Bone. J. Periodontol. 2001, 72, 1178–1182. [Google Scholar] [CrossRef]
- Schwarz, F.; Olivier, W.; Herten, M.; Sager, M.; Chaker, A.; Becker, J. Influence of implant bed preparation using an Er:YAG laser on the osseointegration of titanium implants: A histomorphometrical study in dogs. J. Oral Rehabil. 2007, 34, 273–281. [Google Scholar] [CrossRef]
- Sohn, D.; Lee, J.; An, K.; Romanos, G. Erbium, chromium:yttrium–scandium–gallium–garnet laser-assisted sinus graft procedure. Lasers Med. Sci. 2009, 24, 673–677. [Google Scholar] [CrossRef]
- Romanos, G.; Everts, H.; Nentwig, G. Effects of Diode and Nd: YAG Laser Irradiation on Titanium Discs: A Scanning Electron Microscope Examination. J. Periodontol. 2000, 71, 810–815. [Google Scholar] [CrossRef]
- Schwarz, F.; Sculean, A.; Rothamel, D.; Schwenzer, K.; Georg, T.; Becker, J. Clinical evaluation of an Er: YAG laser for nonsurgical treatment of peri-implantitis: A pilot study. Clin. Oral Implant. Res. 2004, 16, 44–52. [Google Scholar] [CrossRef]
- Kreisler, M.; Al Haj, H.; Götz, H.; Duschner, H.; D’Hoedt, B. Effect of simulated CO2 and GaAlAs laser surface decontamination on temperature changes in Ti-plasma sprayed dental implants. Lasers Surg. Med. 2002, 30, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Kreisler, M.; Kohnen, W.; Christoffers, A.; Götz, H.; Jansen, B.; Duschner, H.; D’Hoedt, B. In vitro evaluation of the biocompatibility of contaminated implant surfaces treated with an Er: YAG laser and an air powder system. Clin. Oral Implant. Res. 2004, 16, 36–43. [Google Scholar] [CrossRef] [PubMed]
- Marotti, J.; Tortamano Neto, P.; Toyota de Campos, T.; Ana, C.C.A.; Weingart, D.; Wolfart, S.; Haselhuhn, K. Recent Patents of Lasers in Implant Dentistry. Recent Pat. Biomed. Eng. 2011, 4, 103–109. [Google Scholar] [CrossRef]
- Takasaki, A.; Aoki, A.; Mizutani, K.; Schwarz, F.; Sculean, A.; Wang, C.; Koshy, G.; Romanos, G.; Ishikawa, I.; Izumi, Y. Application of antimicrobial photodynamic therapy in periodontal and peri-implant diseases. Periodontology 2000 2009, 51, 109–140. [Google Scholar] [CrossRef] [PubMed]
- Hayek, R.; Araújo, N.; Gioso, M.; Ferreira, J.; Baptista-Sobrinho, C.; Yamada, A.; Ribeiro, M. Comparative Study Between the Effects of Photodynamic Therapy and Conventional Therapy on Microbial Reduction in Ligature-Induced Peri-Implantitis in Dogs. J. Periodontol. 2005, 76, 1275–1281. [Google Scholar] [CrossRef]
- Junker, R.; Dimakis, A.; Thoneick, M.; Jansen, J. Effects of implant surface coatings and composition on bone integration: A systematic review. Clin. Oral Implant. Res. 2009, 20, 185–206. [Google Scholar] [CrossRef] [PubMed]
- Faeda, R.; Spin-Neto, R.; Marcantonio, E.; Guastaldi, A.; Marcantonio, E. Laser ablation in titanium implants followed by biomimetic hydroxyapatite coating: Histomorphometric study in rabbits. Microsc. Res. Tech. 2012, 75, 940–948. [Google Scholar] [CrossRef]
- Faeda, R.; Tavares, H.; Sartori, R.; Guastaldi, A.; Marcantonio Jr., E. Evaluation of titanium implants with surface modification by laser beam: Biomechanical study in rabbit tibias. Braz. Oral Res. 2009, 23, 137–143. [Google Scholar] [CrossRef] [Green Version]
- Crespi, R.; Barone, A.; Covani, U.; Ciaglia, R.; Romanos, G. Effects of CO2 Laser Treatment on Fibroblast Attachment to Root Surfaces. A Scanning Electron Microscopy Analysis. J. Periodontol. 2002, 73, 1308–1312. [Google Scholar] [CrossRef]
- Aoki, A.; Mizutani, K.; Schwarz, F.; Sculean, A.; Yukna, R.; Takasaki, A.; Romanos, G.; Taniguchi, Y.; Sasaki, K.; Zeredo, J.; et al. Periodontal and peri-implant wound healing following laser therapy. Periodontology 2000 2015, 68, 217–269. [Google Scholar] [CrossRef] [PubMed]
- Ohshiro, T.; Caldenhead, R. Development of Low Reactive-Level Laser Therapy and Its Present Status. J. Clin. Laser Med. Surg. 1991, 9, 267–275. [Google Scholar] [CrossRef] [PubMed]
- Maruyama, H.; Aoki, A.; Sasaki, K.; Takasaki, A.; Iwasaki, K.; Ichinose, S.; Oda, S.; Ishikawa, I.; Izumi, Y. The effect of chemical and/or mechanical conditioning on the Er: YAG laser-treated root cementum: Analysis of surface morphology and periodontal ligament fibroblast attachment. Lasers Surg. Med. 2008, 40, 211–222. [Google Scholar] [CrossRef] [PubMed]
- Izumi, Y.; Aoki, A.; Yamada, Y.; Kobayashi, H.; Iwata, T.; Akizuki, T.; Suda, T.; Nakamura, S.; Wara-Aswapati, N.; Ueda, M.; et al. Current and future periodontal tissue engineering. Periodontology 2000 2011, 56, 166–187. [Google Scholar] [CrossRef]
- Wolfe, W.; Zissis, J.G. The Infrared Handbook, Environmental Research Institute of Michigan for the Office of Naval Research; Department of the Navy: Washington, DC, USA, 1985. [Google Scholar]
- Rechmann, P.; Sadegh, H.; Goldin, D.; Hennig, T. Surface changes of implants after laser irradiation. Lasers Dent. V 1999, 3593, 102–109. [Google Scholar] [CrossRef]
- Persson, G.; Roos-Jansåker, A.; Lindahl, C.; Renvert, S. Microbiologic Results After Non-Surgical Erbium-Doped:Yttrium, Aluminum, and Garnet Laser or Air-Abrasive Treatment of Peri-Implantitis: A Randomized Clinical Trial. J. Periodontol. 2011, 82, 1267–1278. [Google Scholar] [CrossRef]
- Schwarz, F.; Sahm, N.; Iglhaut, G.; Becker, J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: A randomized controlled clinical study. J. Clin. Periodontol. 2011, 38, 276–284. [Google Scholar] [CrossRef]
- Matsuyama, T.; Aoki, A.; Oda, S.; Yoneyama, T.; Ishikawa, I. Effects of the Er:YAG Laser Irradiation on Titanium Implant Materials and Contaminated Implant Abutment Surfaces. J. Clin. Laser Med. Surg. 2003, 21, 7–17. [Google Scholar] [CrossRef]
- Park, K.; Koak, J.; Kim, S.; Han, C.; Heo, S. The Effect of Ultraviolet-C Irradiation Via a Bactericidal Ultraviolet Sterilizer on an Anodized Titanium Implant: A Study in Rabbits. Int. J. Oral Maxillofac. Implant. 2013, 28, 57–66. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, F.; Rothamel, D.; Sculean, A.; Georg, T.; Scherbaum, W.; Becker, J. Effects of an Er: YAG laser and the VectorR ultrasonic system on the biocompatibility of titanium implants in cultures of human osteoblast-like cells. Clin. Oral Implant. Res. 2003, 14, 784–792. [Google Scholar] [CrossRef]
- Taniguchi, Y.; Aoki, A.; Mizutani, K.; Takeuchi, Y.; Ichinose, S.; Takasaki, A.; Schwarz, F.; Izumi, Y. Optimal Er:YAG laser irradiation parameters for debridement of microstructured fixture surfaces of titanium dental implants. Lasers Med. Sci. 2012, 28, 1057–1068. [Google Scholar] [CrossRef]
- Akram, Z.; Al-Shareef, S.; Daood, U.; Asiri, F.; Shah, A.; AlQahtani, M.; Vohra, F.; Javed, F. Bactericidal Efficacy of Photodynamic Therapy Against Periodontal Pathogens in Periodontal Disease: A Systematic Review. Photomed. Laser Surg. 2016, 34, 137–149. [Google Scholar] [CrossRef] [PubMed]
- Akram, Z.; Abduljabbar, T.; Sauro, S.; Daood, U. Effect of photodynamic therapy and laser alone as adjunct to scaling and root planing on gingival crevicular fluid inflammatory proteins in periodontal disease: A systematic review. Photodiagnosis Photodyn. Ther. 2016, 16, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Abduljabbar, T.; Vohra, F.; Javed, F.; Akram, Z. Antimicrobial photodynamic therapy adjuvant to non-surgical periodontal therapy in patients with diabetes mellitus: A meta-analysis. Photodiagnosis Photodyn. Ther. 2017, 17, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Vohra, F.; Akram, Z.; Bukhari, I.; Sheikh, S.; Javed, F. Short-term effects of adjunctive antimicrobial photodynamic therapy in obese patients with chronic periodontitis: A randomized controlled clinical trial. Photodiagnosis Photodyn. Ther. 2018, 21, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Akram, Z.; Hyder, T.; Al-Hamoudi, N.; Binshabaib, M.; Alharthi, S.; Hanif, A. Efficacy of photodynamic therapy versus antibiotics as an adjunct to scaling and root planing in the treatment of periodontitis: A systematic review and meta-analysis. Photodiagnosis Photodyn. Ther. 2017, 19, 86–92. [Google Scholar] [CrossRef]
- Vohra, F.; Akram, Z.; Safii, S.; Vaithilingam, R.; Ghanem, A.; Sergis, K.; Javed, F. Role of antimicrobial photodynamic therapy in the treatment of aggressive periodontitis: A systematic review. Photodiagnosis Photodyn. Ther. 2016, 13, 139–147. [Google Scholar] [CrossRef]
- Javed, F.; Abduljabbar, T.; Carranza, G.; Gholamiazizi, E.; Mazgaj, D.; Kellesarian, S.; Vohra, F. Efficacy of periimplant mechanical debridement with and without adjunct antimicrobial photodynamic therapy in the treatment of periimplant diseases among cigarette smokers and non-smokers. Photodiagnosis Photodyn. Ther. 2016, 16, 85–89. [Google Scholar] [CrossRef]
- Javed, F.; BinShabaib, M.; Alharthi, S.; Qadri, T. Role of mechanical curettage with and without adjunct antimicrobial photodynamic therapy in the treatment of peri-implant mucositis in cigarette smokers: A randomized controlled clinical trial. Photodiagnosis Photodyn. Ther. 2017, 18, 331–334. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement (Reprinted from Annals of Internal Medicine). PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Methley, A.M.; Campbell, S.; Chew-Graham, C.; McNally, R.; Cheraghi-Sohi, S. PICO, PICOS and SPIDER: A comparison study of specificity and sensitivity in three search tools for qualitative systematic reviews. BMC Health Serv. Res. 2014, 14, 579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aimetti, M.; Mariani, G.; Ferrarotti, F.; Ercoli, E.; Liu, C.; Romano, F. Adjunctive efficacy of diode laser in the treatment of peri-implant mucositis with mechanical therapy: A randomized clinical trial. Clin. Oral Implant. Res. 2019, 30, 429–438. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Martos, R.; Samman, A.; Bouazza-Juanes, K.; Díaz-Fernández, J.; Arias-Herrera, S. Clinical effect of diode laser on peri-implant tissues during non-surgical peri-implant mucositis therapy: Randomized controlled clinical study. J. Clin. Exp. Dent. 2020, 12, e13–e21. [Google Scholar] [CrossRef] [PubMed]
- Renvert, S.; Lindahl, C.; Roos Jansåker, A.; Persson, G. Treatment of peri-implantitis using an Er: YAG laser or an air-abrasive device: A randomized clinical trial. J. Clin. Periodontol. 2010, 38, 65–73. [Google Scholar] [CrossRef] [PubMed]
- Abduljabbar, T.; Javed, F.; Kellesarian, S.; Vohra, F.; Romanos, G. Effect of Nd:YAG laser-assisted non-surgical mechanical debridement on clinical and radiographic peri-implant inflammatory parameters in patients with peri-implant disease. J. Photochem. Photobiol. B Biol. 2017, 168, 16–19. [Google Scholar] [CrossRef] [PubMed]
- Romeo, U.; Nardi, G.; Libotte, F.; Sabatini, S.; Palaia, G.; Grassi, F. The Antimicrobial Photodynamic Therapy in the Treatment of Peri-Implantitis. Int. J. Dent. 2016, 2016, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, F.; John, G.; Schmucker, A.; Sahm, N.; Becker, J. Combined surgical therapy of advanced peri-implantitis evaluating two methods of surface decontamination: A 7-year follow-up observation. J. Clin. Periodontol. 2017, 44, 337–342. [Google Scholar] [CrossRef]
- Deppe, H.; Horch, H.-H.; Neff, A. Conventional versus CO2 laser-assisted treatment of peri-implant defects with the concomitant use of pure-phase beta-tricalcium phosphate: A 5-year clinical report. Int. J. Oral Maxillofac. Implant. 2007, 22, 79–86. [Google Scholar]
- Papadopoulos, C.; Vouros, I.; Menexes, G.; Konstantinidis, A. The utilization of a diode laser in the surgical treatment of peri-implantitis. A randomized clinical trial. Clin. Oral Investig. 2015, 19, 1851–1860. [Google Scholar] [CrossRef]
- Albaker, A.; ArRejaie, A.; Alrabiah, M.; Al-Aali, K.; Mokeem, S.; Alasqah, M.; Vohra, F.; Abduljabbar, T. Effect of antimicrobial photodynamic therapy in open flap debridement in the treatment of peri-implantitis: A randomized controlled trial. Photodiagnosis Photodyn. Ther. 2018, 23, 71–74. [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H. Peri-implantitis. J. Periodontol. 2018, 89, S267–S290. [Google Scholar] [CrossRef] [PubMed]
- Jepsen, S.; Berglundh, T.; Genco, R.; Aass, A.M.; Demirel, K.; Derks, J.; Figuero, E.; Giovannoli, J.L.; Goldstein, M.; Lambert, F.; et al. Primary Prevention of Peri-Implantitis: Managing Peri-Implant Mucositis. J. Clin. Periodontol. 2015, 42, S152–S157. [Google Scholar] [CrossRef] [Green Version]
- Ting, M.; Craig, J.; Balkin, B.; Suzuki, J. Peri-implantitis: A Comprehensive Overview of Systematic Reviews. J. Oral Implantol. 2018, 44, 225–247. [Google Scholar] [CrossRef] [PubMed]
- Arısan, V.; Karabuda, Z.; Arıcı, S.; Topçuoğlu, N.; Külekçi, G. A Randomized Clinical Trial of an Adjunct Diode Laser Application for the Nonsurgical Treatment of Peri-Implantitis. Photomed. Laser Surg. 2015, 33, 547–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Birang, E.; Talebi Ardekani, M.; Rajabzadeh, M.; Sarmadi, G.; Birang, R.; Gutknecht, N. Evaluation of Effectiveness of Photodynamic Therapy with Low-level Diode Laser in Nonsurgical Treatment of Peri-implantitis. J. Lasers Med. Sci. 2017, 8, 136–142. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schär, D.; Ramseier, C.; Eick, S.; Arweiler, N.; Sculean, A.; Salvi, G. Anti-infective therapy of peri-implantitis with adjunctive local drug delivery or photodynamic therapy: Six-month outcomes of a prospective randomized clinical trial. Clin. Oral Implant. Res. 2012, 24, 104–110. [Google Scholar] [CrossRef]
- Schwarz, F.; John, G.; Mainusch, S.; Sahm, N.; Becker, J. Combined surgical therapy of peri-implantitis evaluating two methods of surface debridement and decontamination. A two-year clinical follow up report. J. Clin. Periodontol. 2012, 39, 789–797. [Google Scholar] [CrossRef]
- Geminiani, A.; Caton, J.; Romanos, G. Temperature Increase During CO2 and Er: YAG Irradiation on Implant Surfaces. Implant Dent. 2011, 20, 379–382. [Google Scholar] [CrossRef] [PubMed]
- Carinci, F.; Roncati, M.; Lucchese, A. Non-surgical treatment of peri-implantitis with the adjunctive use of an 810-nm diode laser. J. Indian Soc. Periodontol. 2000 2013, 17, 812. [Google Scholar] [CrossRef]
- Mettraux, G.; Sculean, A.; Bürgin, W.; Salvi, G. Two-year clinical outcomes following non-surgical mechanical therapy of peri-implantitis with adjunctive diode laser application. Clin. Oral Implant. Res. 2015, 27, 845–849. [Google Scholar] [CrossRef]
- Lerario, F.; Roncati, M.; Gariffo, A.; Attorresi, E.; Lucchese, A.; Galanakis, A.; Palaia, G.; Romeo, U. Non-surgical periodontal treatment of peri-implant diseases with the adjunctive use of diode laser: Preliminary clinical study. Lasers Med. Sci. 2015, 31, 1–6. [Google Scholar] [CrossRef]
- Norton, M. Efficacy of Er:YAG Laser in the Decontamination of Peri-implant Disease: A One-Year Prospective Closed Cohort Study. Int. J. Periodontics Restor. Dent. 2017, 37, 781–788. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pommer, B.; Haas, R.; Mailath-Pokorny, G.; Fürhauser, R.; Watzek, G.; Busenlechner, D.; Müller-Kern, M.; Kloodt, C. Periimplantitis Treatment. Implant Dent. 2016, 25, 646–649. [Google Scholar] [CrossRef] [PubMed]
- John, G.; Becker, J.; Schmucker, A.; Schwarz, F. Non-surgical treatment of peri- implant mucositis and peri-implantitis at two-piece zirconium implants: A clinical follow-up observation after up to 3 years. J. Clin. Periodontol. 2017, 44, 756–761. [Google Scholar] [CrossRef] [PubMed]
- Deppe, H.; Mücke, T.; Wagenpfeil, S.; Kesting, M.; Sculean, A. Nonsurgical antimicrobial photodynamic therapy in moderate vs severe peri-implant defects: A clinical pilot study. Quintessence Int. 2013, 44, 609–618. [Google Scholar] [CrossRef]
- Kotsakis, G.; Konstantinidis, I.; Karoussis, I.; Ma, X.; Chu, H. Systematic Review and Meta-Analysis of the Effect of Various Laser Wavelengths in the Treatment of Peri-Implantitis. J. Periodontol. 2014, 85, 1203–1213. [Google Scholar] [CrossRef]
- Albaker, A.; ArRejaie, A.; Alrabiah, M.; Abduljabbar, T. Effect of photodynamic and laser therapy in the treatment of peri -implant mucositis: A systematic review. Photodiagnosis Photodyn. Ther. 2018, 21, 147–152. [Google Scholar] [CrossRef] [PubMed]
- Al-Falaki, R.; Cronshaw, M.; Hughes, F. Treatment outcome following use of the erbium, chromium:yttrium, scandium, gallium, garnet laser in the non-surgical management of peri-implantitis: A case series. Br. Dent. J. 2014, 217, 453–457. [Google Scholar] [CrossRef]
- Qadri, T.; Poddani, P.; Javed, F.; Tunér, J.; Gustafsson, A. A Short-Term Evaluation of Nd:YAG Laser as an Adjunct to Scaling and Root Planing in the Treatment of Periodontal Inflammation. J. Periodontol. 2010, 81, 1161–1166. [Google Scholar] [CrossRef]
- Schwarz, F.; Sahm, N.; Bieling, K.; Becker, J. Surgical regenerative treatment of peri-implantitis lesions using a nanocrystalline hydroxyapatite or a natural bone mineral in combination with a collagen membrane: A four-year clinical follow-up report. J. Clin. Periodontol. 2009, 36, 807–814. [Google Scholar] [CrossRef]
- Schou, S.; Berglundh, T.; Lang, N.P. Surgical Treatment of Peri-Implantitis. Int. J. Oral Maxillofac. Implant. 2004, 19, 140–149. [Google Scholar]
- Klinge, B.; Meyle, J.; Claffey, N.; Flemmig, T.; Flemming, I.; Mombelli, A.; Naert, I.; Renvert, S.; Rocchietta, I.; Schou, S.; et al. Peri-implant tissue destruction. The Third EAO Consensus Conference 2012. Clin. Oral Implants Res. 2012, 23, 108–110. [Google Scholar] [CrossRef] [PubMed]
- Behneke, A.; Behneke, N.; d’Hoedt, B. Treatment of peri-implantitis defects with autogenous bone grafts: Six-month to 3-year results of a prospective study in 17 patients. Int. J. Oral Maxillofac. Implant. 2000, 15, 125–138. [Google Scholar]
- Parker, S.; Cronshaw, M.; Anagnostaki, E.; Bordin-Aykroyd, S.; Lynch, E. Systematic Review of Delivery Parameters Used in Dental Photobiomodulation Therapy. Photobiomodulation Photomed. Laser Surg. 2019, 37, 784–797. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Authors Number of Implants/Patients | Laser/Irradiation Protocol/Treatment Protocol | Type of a/Implant b/Characteristics of Surface/Decontamination-Smoothening | BOP/PI CAL/PD | Outcome Follow Up | Comment |
|---|---|---|---|---|---|
| Aimetti et al. (2019) [63] RCT 220 implants/220 pts. | Diode (DL) 980 nm. Non-surgical approach Group 1: Debridement curettes/US Group 2: Debridement curettes/US DL + 3% H2O2 for 10 s. | a/Not mentioned b/Group 1: Mechanical debridement, Group 2: Mechanical debridement + Laser decontamination + Peroxide. | Peri-implant mucositis (PD ≥ 4 mm) BOP/PD/PI measured. | 1 mth—BOP ↑ DL group (p < 0.01).3 mths—both groups ↓ BOP (p > 0.05), PI (p < 0.001) and PD (p < 0.001). | DL no statistically significant clinical benefit at 3 mths. Complete resolution obtained 38/110 (34.5%) implants in test group cf 34/110 (30.9%) implants in control group. |
| Sánchez-Martos et al. (2020) [64] RCT 68 implants/68 pts. | Diode (DL) 810 nm. Group 1: Debridement + CHX + 0.05% cetylpyridinium chloride (Control) Group 2: Debridement + CHX + 0.05% cetylpyridinium chloride + DL (Laser Group). | a/3i (62) int. hex/screwed abutments. Straumann (6). b/DL AP 1.0 W (Gated)/30 sec/surface with 1 cm diffuser. 300 μ tip into sulcus for 30 secs. | Mucositis. Gr 1 av. BOP of 1.176 ± 0.700, 0.264 ± 0.220 (6 wks), 0.568 ± 0.282 (3 mths). Gr 2 BOP 1.175 ± 0.795, 0.148 ± 0.150 (6 wks), 0.264 ± 167 (3 mths). Stat. sig. 95% (t-Student p = 0.001) between groups at 3-month. Gr 1 av PI 0.676 ± 0.374, 0.588 ± 0.526 (6 wks), 0.509 ± 0.370 (3 mths). Gr 2 av. 0.824 ± 0.541, 0.248 ± 0.3155 (6 wks), 0.480 ± 0.336 (3 mths). Stat. sig. 95% (t-Student p = 0.041) groups at 6 weeks. CAL No stat. sig. 95% throughout the study. Gr 1 PD 1.303 ± 0.409 mm, 1.137 ± 0.222 mm (6 wks), 1.166 ± 0.263 mm (3 mths). On the other hand, the Gr 2 1.277 ± 0.347 mm, 0.833 ± 0.374 mm (6 wks), 1.068 ± 0.103 mm (3 mths). Stat. sig. 95% (t-Student p = 0.041) 6 weeks. | A better response of the gingival index was obtained, especially in bleeding on probing, which avoids a significant decrease of the inflammation in the peri-implant tissues. | The use of diode laser as an adjunctive therapy to the conventional treatment of peri-implant mucositis showed promising results, being more effective reducing the inflammation of the peri-implant tissue, positioning itself as a valuable tool for the treatment of peri-implant pathologies. |
| Authors Number of Implants/Patients | Laser/Irradiation Protocol/Treatment Protocol | Type of a/Implant b/Characteristics of Surface/Decontamination-Smoothening | BOP/PI CAL/PD | Outcome Follow Up | Comment |
|---|---|---|---|---|---|
| Renvert et al. (2011) [65] Blinded RCT 86 implants—42 patients Non-surgical. | Er:YAG 2940 nm. Grp 1: Perio Flow Device, Grp 2: Er:YAG 100 mJ/pulse/10 Hz. Fluence 12.7 J/cm2. | a/Air -abrasive Group: machined surface: 29, medium rough surface: 16. Laser Group: machined surface: 41, medium rough surface: 14. Instrument tip was used in a parallel mode using a semi-circular motion around the circumferential pocket area of the implant. | Peri-implantitis. BOP ↓ sig. in both groups (p < 0.001). No differences in changes of BOP by study intervention groups (p = 0.22). 6 mths ↓plaque at implants in air-abrasive group (p < 0.05). CAL—Not measured PD ↓ in laser group 0.8 mm (SD ± 0.5), PD ↓ in air-abrasive group 0.9 mm (SD ± 0.8). No differences in PD by study group intervention (p = 0.55). | PI results of therapy at 6 mths similar Er:YAG or air- abrasive for debridement of implants. Both methods ↓ PD and BOP. The overall clinical improvement was limited. | No sig. diff. PD > =5 mm, BOP and suppuration at 6 mths. No sig diff in alveolar bone at 6 months in both groups. |
| Abduljabbar et al. (2017) [66] RCT 63 pts/79 implants Non-surgical. | Nd: YAG 1064 nm 60 to 120 s. Av p. 4 W 80 mJ 50 Hz. Pulse width 350 msecs + air/water. | a/Platform-switched with moderately rough surfaces b/Grp 1 = MD only, Grp 2 = MD with 1 appl Nd: YAG laser. | Peri-implantitis: BOP at >30% of PI sites, PD ≥ 4 mm and/or ≥ 3 mm bone loss/implant. 3 mths BOP ↑ MD + Nd:YAG Grp cf MD Grp. 6 mth BOP comparable in both groups. 3 mth PI ↑ MD + Nd:YAG Grp cf MD Grp. 6 mth PI comparable in both groups. CAL not measured. | No statistically significant difference in CBL among patients in groups 1 and 2 at 3- and 6-month. | Nd:YAG + MD non-surgical more effective in PI cf MD but not maintained at 6 mths. Soft tissue healing sig faster MD + Nd:YAG cf MD. |
| Romeo et al. (2016) [67] RCT 40 pts/123 implants Non-surgical. | DL 670 nm + MBO. Fluence 25.54 J/cm2, Total energy 1592 J/cm2. | a/Not mentioned b/Grp 1: MD Group 2: MD +aPDT. | Peri-implantitis: BOP, PD ≥4 mm, and suppuration. BOP ceased Grp 2 at 24 wks. PI Grp 2 17% at 24 wks. Control PI of 25%. No sig. diff. between grps. CAL Not measured PD Grp 2 (MD and aPDT) better with av. 2 mm cf Grp 1(3 mm). The readings remained constant at 24 weeks. | The results obtained in this study suggest that photodynamic therapy could be considered an effective method for bacterial reduction on implant surfaces. | Group 2 showed after 24 weeks a better value in terms of PD, BOP, and PI, with an average pocket depth value of 2 mm, if compared with group 1 (3 mm). |
| Authors No. of Implants/Patients | Laser/Irradiation Protocol/Treatment Protocol | Type of a/Implant b/Characteristics of Surface/Decontamination-Smoothening | BOP/SBI (Sulcus Bleed)/PI CAL/PD/DIB (Implant Shoulder to Bone) | Outcome Follow Up | Comment |
|---|---|---|---|---|---|
| Schwarz et al. (2017) [68] RCT 15 implants—15 patients. | Er:YAG 2940 nm CPS Grp: Plastic curettes+ Cotton pellets + Sterile saline/Peri—implantitis/Open flap/GBR ERL Grp: Laser Decontamination 100 mJ/pulse/10 Hz (12.7 J/cm2). | a/AST, BRA, CAM, ITI, KSI, REP, TSV, XIV, NI b/Mechanical or Laser decontamination. | Both grps, BOP ↓ 91.65 ± 11.08% and 66.7% at Class Ib + II defects, 88.88 ± 13.60% and 100 ± 0.0% at Class Ic + II, and 91.65 ± 11.80% and 83.30 ± 23.61% at Class Ie + II defects. SBI: Not measured. PI ↑ CPS at 83.0 mths. PD CPS ↓ + CAL ↑ 2.00 ± 0.70 mm/1.80 ± 0.70 mm at Class Ib + II defects, 3.15 ± 1.91 mm/3.25 ± 2.40 mm at Class Ic + II defects, and 1.30 ± 0.70 mm/2.25 ± 0.07 mm at Class Ie + II. ERL PD ↓ and CAL ↑ 1.17 mm/1.50 mm at the Class Ib + II defect, 1.90 ± 0.98 mm/3.60 ± 1.83 mm at Class Ic + II defects, and 0.55 ± 2.61 mm/2.30 ± 2.12 mm at Class Ie + II. | 7 years ERL + CPS similar BOP ↓ CPS: 89.99 ± 11.65% vs. ERL: 86.66 ± 18.26%). CAL gains (CPS: 2.76 ± 1.92 mm vs. ERL: 2.06 ± 2.52 mm). | Combined surgical resective/regenerative therapy of advanced peri-implantitis was effective on the long-term but the clinical outcomes were not influenced by the initial method of surface decontamination. |
| Schwarz et al. (2017) [69] RCT 73 implants—32 patients. | CO2 10,600 nm 4 Grps: Grp 1 = MD + implants, Grp 2 = MD + implants/augmented bone, Grp 3 = laser + implants, Grp 4 = laser + implants/augmented bone. | 2.5 W CW. Fluence 175 Jcm–2 × 5 sec × 12 a/IMZ, Frialit-2 b/air-powder abrasive + CO2. | SBI ↓ 4 mths all groups. DIB laser no sig. Diff. Among grps during 5 yrs. PI ↓ 4 months. At 4 mths + 5 yrs stat sig. diff. between grps 1 and 3. Grp 2 and 4(GBR), stat sig diff. at 4 mths but not 5 yrs. PD no stat diff in grps 1 and 3 at 5 years. No stat diff in grps 2 and 4 (GBR) at 5 years (cf 4 mths). | 5 years Clinical + X-Ray indicate CO2 + soft tissue resection effective against bone resorption. | 1 pt (Grp 2) loss of 4 implants. 1 pt (Grp 4) loss of 4 implants. With respect to augmentation procedures, the method used for decontamination seems to play a subordinate role. |
| Papadopoulos et al. (2015) [70] RCT 19 patients. | DL 980 nm 2 Grps. C Grp: Cotton soaked in saline L Grp: Cotton in saline + DL PD ≥6 mm at least 1 implant + BOP + bone loss ≥2 mm Open flap debridement. | a/Not mentioned b/C Group: MD L Group: MD + Laser. | BOP 72.9% 3 mths/66.7% 6 mths (p < 0.05). SBI: Not measured. PI ↓ in C group at 3 mhs from 37.5 to 6.3%. No stat sig diff (p < 0.05) at 6 mths. CAL ↑ Laser grp 5.25 mm to 4.54 mm 3–6 mths (p < 0.05). PD ↓ 1.19 mm (control) + 1.38 mm (laser) (p < 0.05). | 6 months Surgical PI Tx + flaps ↑ all clinical parameters studied. DL doesn’t have extra beneficiary effect. | Diode laser in the surgical treatment of peri-implantitis does not seem to have any additional clinical benefit. |
| Albaker et al. (2018) [71] RCT 24 patients. | DL 670 nm + MBO. Group 1: OFD alone Group 2:OFD and aPDT. | MBL ≥2 mm bone level 1 yr following implant or ≥3 mm PD (PA Rads) + PD ≥5 mm + BOP/open flap debridement- no GBR a/Not mentioned b/Grp 1: OFD Grp 2: OFD and aPDT BOP 6 mths ↓ 35.9–24.3% in aPDT group (p < 0.05). 26.5–21.6% OFD grp (p < 0.05). 12 mths ↓ 24.3% to 17.4% (p < 0.05) in aPDT and 21.6–14.8% (p < 0.05) in OFD grp. | SBI/DIB Not measured. PI in aPDT grp ↓ 44.7% to 21.2% (p < 0.05) at 6 mths and 48.3–19.5% (p < 0.05) in OFD group. 12 mths, PI further ↓ 21.2–16.4% (p < 0.05) in aPDT group and 19.5–11.6% (p < 0.05) in OFD group. CAL Not measured PD ↓ 6 months sig. in both groups. 5.2 mm to 3.9 mm aPDT grp (p < 0.05) and 5.4 mm–4.1 mm OFD group (p < 0.05). | 12 months Both groups reduced PI, BOP, PD and MBL. However, there was no significant difference between aPDT and OFD groups over time. | Within the limits of the present RCT, it is concluded that single application of aPDT as an adjunct to OFD does not provide additional benefit in improving clinical and radiographic peri-implant parameters in peri-implantitis. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chala, M.; Anagnostaki, E.; Mylona, V.; Chalas, A.; Parker, S.; Lynch, E. Adjunctive Use of Lasers in Peri-Implant Mucositis and Peri-Implantitis Treatment: A Systematic Review. Dent. J. 2020, 8, 68. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8030068
Chala M, Anagnostaki E, Mylona V, Chalas A, Parker S, Lynch E. Adjunctive Use of Lasers in Peri-Implant Mucositis and Peri-Implantitis Treatment: A Systematic Review. Dentistry Journal. 2020; 8(3):68. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8030068
Chicago/Turabian StyleChala, Marianna, Eugenia Anagnostaki, Valina Mylona, Anastasios Chalas, Steven Parker, and Edward Lynch. 2020. "Adjunctive Use of Lasers in Peri-Implant Mucositis and Peri-Implantitis Treatment: A Systematic Review" Dentistry Journal 8, no. 3: 68. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8030068