Effect of an Er,Cr:YSGG Laser on the Surface of Implants: A Descriptive Comparative Study of 3 Different Tips and Pulse Energies

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Randomization of Samples
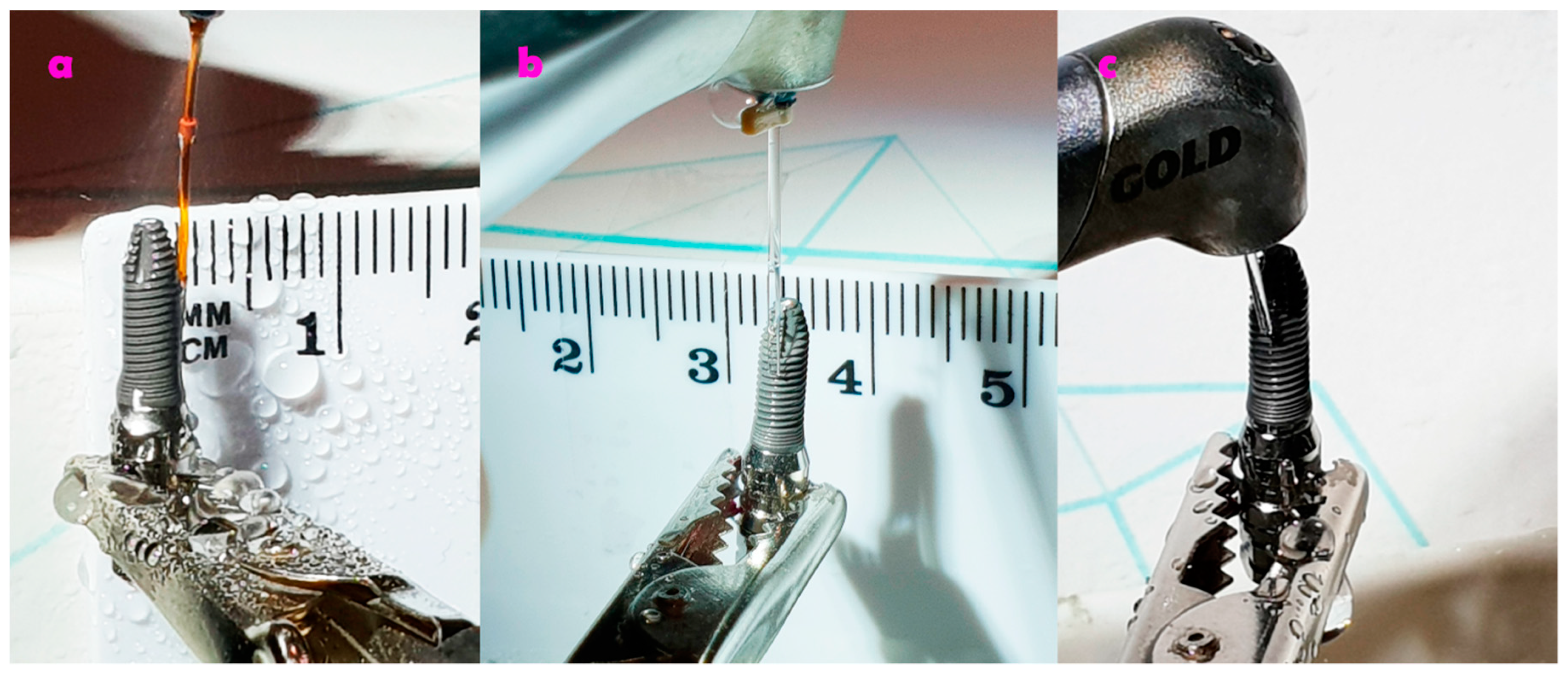
2.2. Irradiation of the Implants
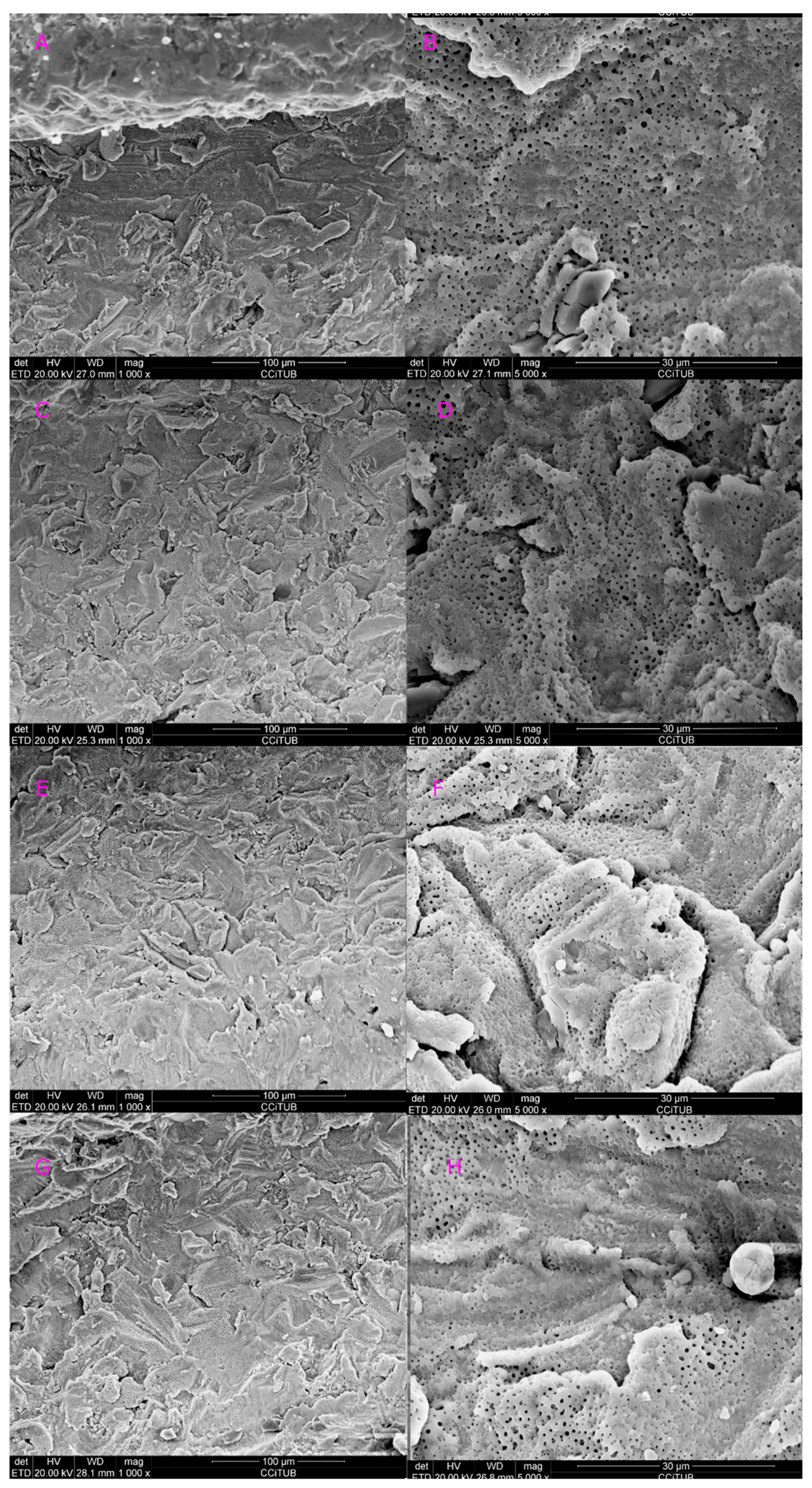
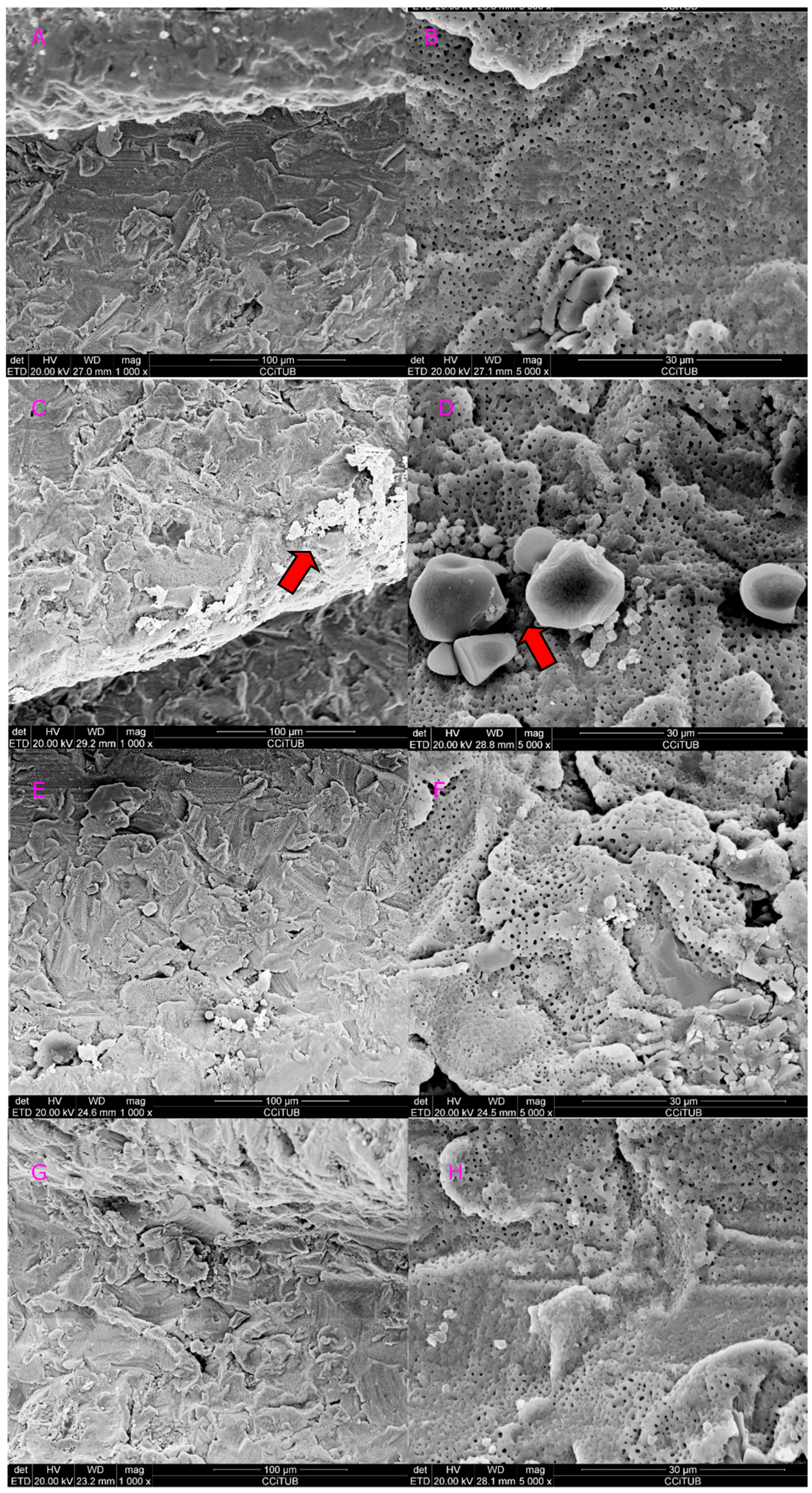
2.3. Scanning Electron Microscope (SEM) Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Moraschini, V.; Poubel, L.A.C.; Ferreira, V.F.; Barboza, E.S.P. Evaluation of survival and success rates of dental implants reported in longitudinal studies with a follow-up period of at least 10 years: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 377–388. [Google Scholar] [CrossRef]
- Gallardo, Y.N.R.; da Silva-Olivio, I.R.; Gonzaga, L.; Sesma, N.; Martin, W. A systematic review of clinical outcomes on patients rehabilitated with complete-arch fixed implant-supported prostheses according to the time of loading. J. Prosthodont. 2019, 28, 958–968. [Google Scholar] [CrossRef]
- Blanco, J.; Figuero, E.; Armitage, G.; Camargo, P.M.; Tomasi, C.; Araujo, M.G.; Avila-Ortiz, G.; Chen, S.; Cochran, D.; Derks, J.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 world workshop on the classification of periodontal and peri-Implant diseases and conditions. J. Prosthodont. 2018, 89, S313–S318. [Google Scholar]
- Derks, J.; Tomasi, C. Peri-implant health and disease. A systematic review of current epidemiology. J. Clin. Periodontol. 2015, 42, S158–S171. [Google Scholar] [CrossRef]
- Cercadillo-Ibarguren, I.; Sánchez-Torres, A.; Figueiredo, R.; Schwarz, F.; Gay-Escoda, C.; Valmaseda-Castellón, E. Immediately loaded implant-supported full-arches: Peri-implant status after 1–9 years in a private practice. J. Dent. 2017, 67, 72–76. [Google Scholar] [CrossRef]
- Cortés-Acha, B.; Figueiredo, R.; Blanc, V.; Soler-Ollé, A.; León, R.; Valmaseda-Castellón, E. Development and viability of biofilms grown on experimental abutments mimicking dental implants: An in vivo model. Med. Oral Patol. Oral Cir. Bucal 2019, 24, e511–e517. [Google Scholar] [CrossRef]
- Cortés-Acha, B.; Figueiredo, R.; Seminago, R.; Roig, F.J.; Llorens, C.; Valmaseda-Castellón, E. Microbiota analysis of biofilms on experimental abutments mimicking dental implants: An in vivo model. J. Periodontol. 2017, 88, 1090–1104. [Google Scholar] [CrossRef]
- Figuero, E.; Graziani, F.; Sanz, I.; Herrera, D.; Sanz, M. Management of peri-implant mucositis and peri-implantitis. Periodontol. 2000 2014, 66, 255–273. [Google Scholar] [CrossRef]
- Wakim, R.N.; Namour, M.; Nguyen, H.V.; Peremans, A.; Zeinoun, T.; Vanheusden, A.; Rompen, E.; Nammour, S. Decontamination of dental implant surfaces by the Er:YAG laser beam: A comparative in vitro study of various protocols. Dent. J. 2018, 6, 66. [Google Scholar] [CrossRef] [Green Version]
- Froum, S.H.; Cantor-Balan, R.; Kerbage, C.; Froum, S.J. Thermal testing of titanium implants and the surrounding ex-vivo tissue irradiated with 9.3 um CO2 laser. Implant Dent. 2019, 28, 463–471. [Google Scholar] [CrossRef]
- Persson, G.R.; Salvi, G.E.; Lisa, J.A. Antimicrobial therapy using a local drug delivery system (Arestin) in the treatment of peri-implantitis. I: Microbiological outcomes. Clin. Oral Implants Res. 2006, 17, 386–393. [Google Scholar] [CrossRef]
- Salvi, G.E.; Persson, G.R.; Heitz-mayfield, L.J.A.; Lang, N.P.; Berne, C. Adjunctive local antibiotic therapy in the treatment of peri-implantitis II: Clinical and radiographic outcomes. Clin. Oral Implants Res. 2007, 18, 281–285. [Google Scholar] [CrossRef]
- Kreisler, M.; Christoffers, A. In vitro evaluation of the biocompatibility of contaminated implant surfaces treated with an Er:YAG laser and an air powder system. Clin. Oral Implants Res. 2005, 16, 36–43. [Google Scholar] [CrossRef]
- Romeo, E.; Chiapasco, M.; Romeo, E. Therapy of peri-implantitis with resective surgery. A 3-year clinical trial on rough screw-shaped oral implants. Part II: Radiographic outcome. Clin. Oral Implants Res. 2007, 18, 179–187. [Google Scholar] [CrossRef]
- Costa-Berenguer, X.; García-García, M.; Sánchez-Torres, A.; Sanz-Alonso, M.; Figueiredo, R.; Valmaseda-Castellón, E. Effect of implantoplasty on fracture resistance and surface roughness of standard diameter dental implants. Clin. Oral Implants Res. 2018, 29, 46–54. [Google Scholar] [CrossRef]
- Renvert, S.; Lindahl, C.; Jansåker, A.M.R.; Persson, R.G. Treatment of peri-implantitis using an Er:YAG laser or an air-abrasive device: A randomized clinical trial. J. Clin. Periodontol. 2011, 38, 65–73. [Google Scholar] [CrossRef]
- Muthukuru, M.; Zainvi, A.; Esplugues, E.O.; Flemmig, T.F. Non-surgical therapy for the management of peri-implantitis: A systematic review. Clin. Oral Implants Res. 2012, 23, 77–83. [Google Scholar] [CrossRef]
- Wennerberg, A.; Albrektsson, T. On implant surfaces: A review of current knowledge and opinions. Int. J. Oral Maxillofac. Implant. 2010, 25, 63–74. [Google Scholar]
- Park, J.H.; Heo, S.J.; Koak, J.Y.; Kim, S.K.; Han, C.H.; Lee, J.H. Effects of laser irradiation on machined an anodized titanium disks. Int. J. Oral Maxillofac. Implant. 2012, 27, 265–272. [Google Scholar]
- Scarano, A.; Nardi, G.; Murmura, G.; Rapani, M.; Mortellaro, C. Evaluation of the removal bacteria on failed titanium implants after irradiation with erbium-doped yttrium aluminium garnet laser. J. Craniofac. Surg. 2016, 27, 1202–1204. [Google Scholar] [CrossRef]
- El Chaar, E.; Almogahwi, M.; Abdalkader, K.; Alshehri, A.; Cruz, S. Decontamination of the Infected Implant Surface: A Scanning Electron Microscope Study. Int. J. Periodontics Restor. Dent. 2020, 40, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Lollobrigida, M.; Fortunato, L.; Serafini, G.; Mazzucchi, G.; Bozzuto, G.; Molinari, A.; Serra, E.; Menchini, F.; Vozza, I.; De Biase, A. The prevention of implant surface alterations in the treatment of peri-implantitis: Comparison of three different mechanical and physical treatments. Int. J. Environ. Res. Public Health 2020, 17, 2624. [Google Scholar] [CrossRef] [Green Version]
- Kubasiewicz-Ross, P.; Hadzik, J.; Gedrange, T.; Fleischer, M.; Pitułaj, A.; Nawrot-Hadzik, I.; Bortkiewicz, O.; Dominiak, M.; Jurczyszyn, K. Evaluation of the three methods of bacterial decontamination on implants with three different surfaces. Adv. Clin. Exp. Med. 2020, 29, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Gholami, G.A.; Karamlou, M.; Fekrazad, R.; Ghanavati, F.; Hakimiha, N.; Romanos, G. Comparison of the effects of Er, Cr: YSGG laser and super-saturated citric acid on the debridement of contaminated implant surfaces. J. Lasers Med. Sci. 2018, 9, 254–260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alagl, A.S.; Madi, M.; Bedi, S.; Onaizan, F. Al, Al-Aql ZS: The effect of Er,Cr:YSGG and diode laser applications on dental implant surfaces contaminated with acinetobacter baumannii and pseudomonas aeruginosa. Materials 2019, 12, 2073. [Google Scholar] [CrossRef] [Green Version]
- Namour, M.; Verspecht, T.; El Mobadder, M.; Teughels, W.; Peremans, A.; Nammour, S.; Rompen, E. Q-Switch Nd:YAG laser-assisted elimination of multi-species biofilm on titanium surfaces. Materials 2020, 13, 1573. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Entered Parameters | Calculated Parameters | ||||||
|---|---|---|---|---|---|---|---|
| Power (W) | Frequency (Hz) | Time (s) | Tip and Diameter (µm) | Tip Radius (cm) | Spot Area (cm2) | Energy Density | Pulse Energy (J) |
| r = d/2/10,000 | A = π r2 | Ed = E/A; J/cm2 | Ep = Pm/f | ||||
| 1.5 | 30 | 60 | Conical (415) | 0.02 | 0.0012 | 41.66 | 0.05 |
| 2.5 | 30 | 60 | Conical (415) | 0.02 | 0.0012 | 66.66 | 0.08 |
| 1.5 | 30 | 60 | Cylindrical (600) | 0.03 | 0.0028 | 17.85 | 0.05 |
| 2.5 | 30 | 60 | Cylindrical (600) | 0.03 | 0.0028 | 28.57 | 0.08 |
| 1.5 | 30 | 60 | Lateral (800) | 0.04 | 0.0050 | 10 | 0.05 |
| 2.5 | 30 | 60 | Lateral (800) | 0.04 | 0.0050 | 16 | 0.08 |
| Entered Parameters | Surface Alterations Classification | |||
|---|---|---|---|---|
| Power (W) | Frequency (Hz) | Time (s) | Tip and Diameter (µm) | |
| 1.5 | 30 | 60 | Conical (415) | Class A |
| 2.5 | 30 | 60 | Conical (415) | Class C |
| 1.5 | 30 | 60 | Cylindrical (600) | Class B |
| 2.5 | 30 | 60 | Cylindrical (600) | Class B |
| 1.5 | 30 | 60 | Lateral (800) | Class A |
| 2.5 | 30 | 60 | Lateral (800) | Class B |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chegeni, E.; España-Tost, A.; Figueiredo, R.; Valmaseda-Castellón, E.; Arnabat-Domínguez, J. Effect of an Er,Cr:YSGG Laser on the Surface of Implants: A Descriptive Comparative Study of 3 Different Tips and Pulse Energies. Dent. J. 2020, 8, 109. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8040109
Chegeni E, España-Tost A, Figueiredo R, Valmaseda-Castellón E, Arnabat-Domínguez J. Effect of an Er,Cr:YSGG Laser on the Surface of Implants: A Descriptive Comparative Study of 3 Different Tips and Pulse Energies. Dentistry Journal. 2020; 8(4):109. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8040109
Chicago/Turabian StyleChegeni, Ehsan, Antonio España-Tost, Rui Figueiredo, Eduard Valmaseda-Castellón, and Josep Arnabat-Domínguez. 2020. "Effect of an Er,Cr:YSGG Laser on the Surface of Implants: A Descriptive Comparative Study of 3 Different Tips and Pulse Energies" Dentistry Journal 8, no. 4: 109. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8040109