Impact of Local Drug Delivery of Minocycline on the Subgingival Microbiota during Supportive Periodontal Therapy: A Randomized Controlled Pilot Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
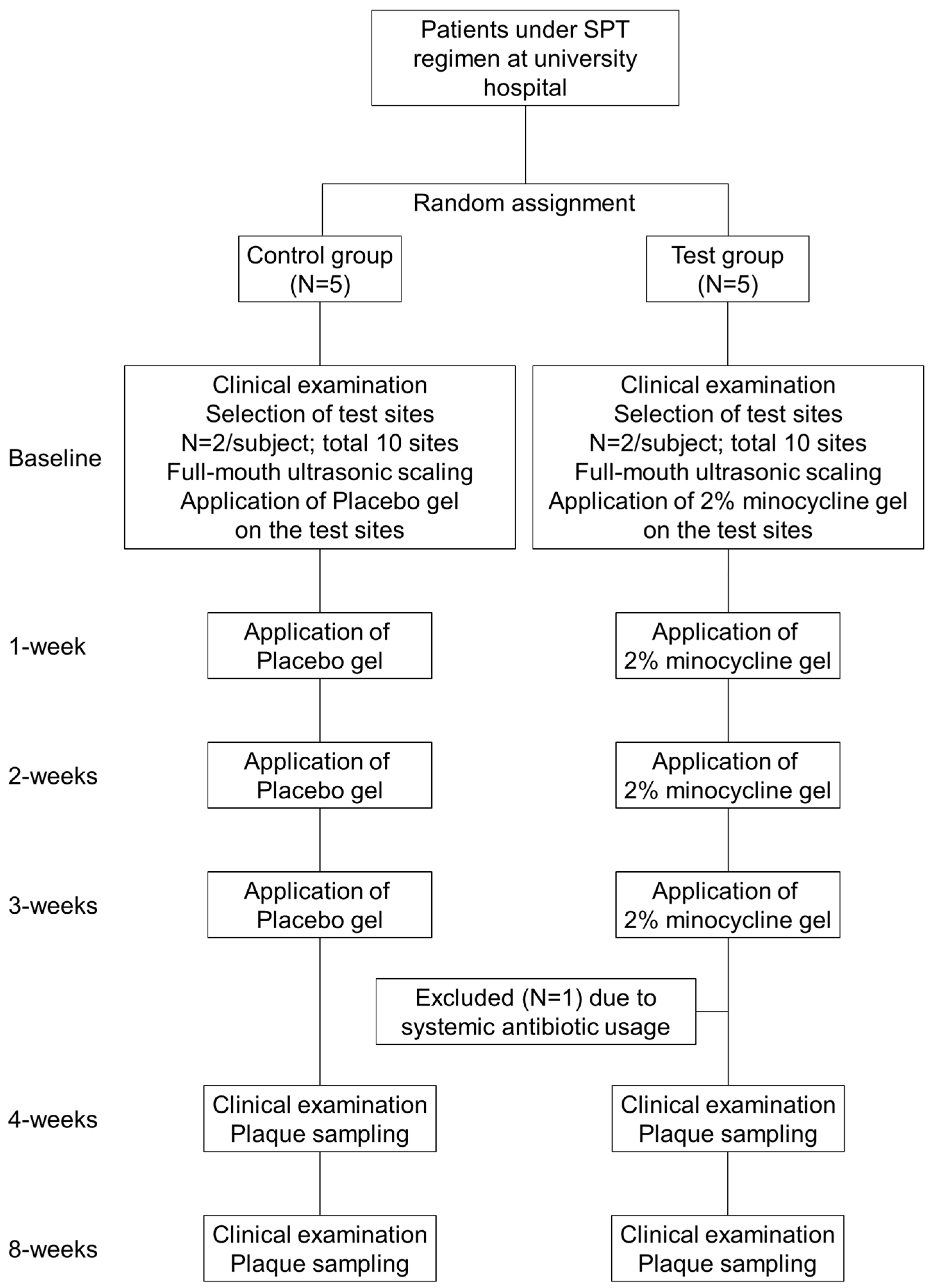
2.1. Study Design
2.2. Clinical Examination and Microbiological Sampling
2.3. Microbiological Assessment of Subgingival Plaque Samples
2.4. Statistical Analysis
3. Results
3.1. Patients
3.2. Periodontal Parameters
3.3. Microbiological Parameters
3.3.1. Quantitative Bacteria
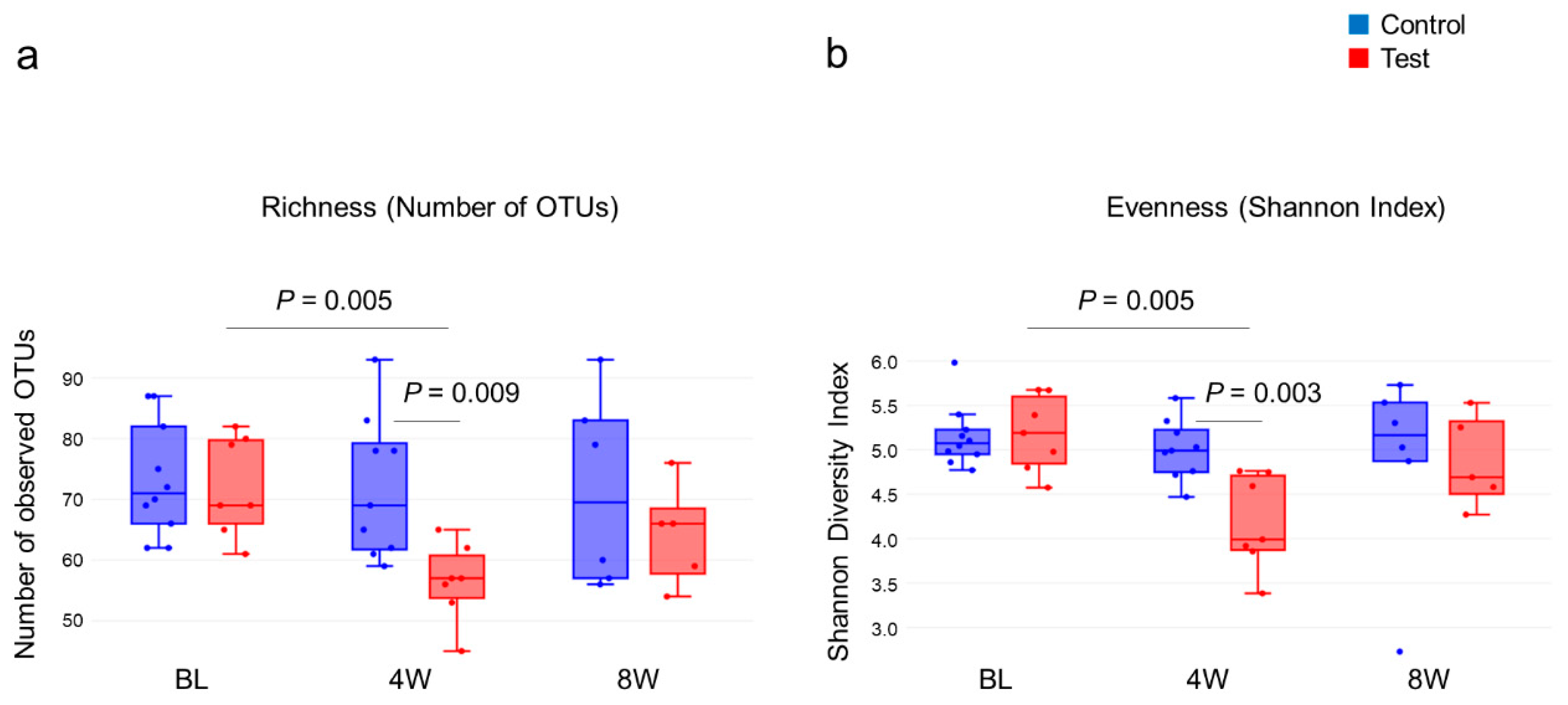
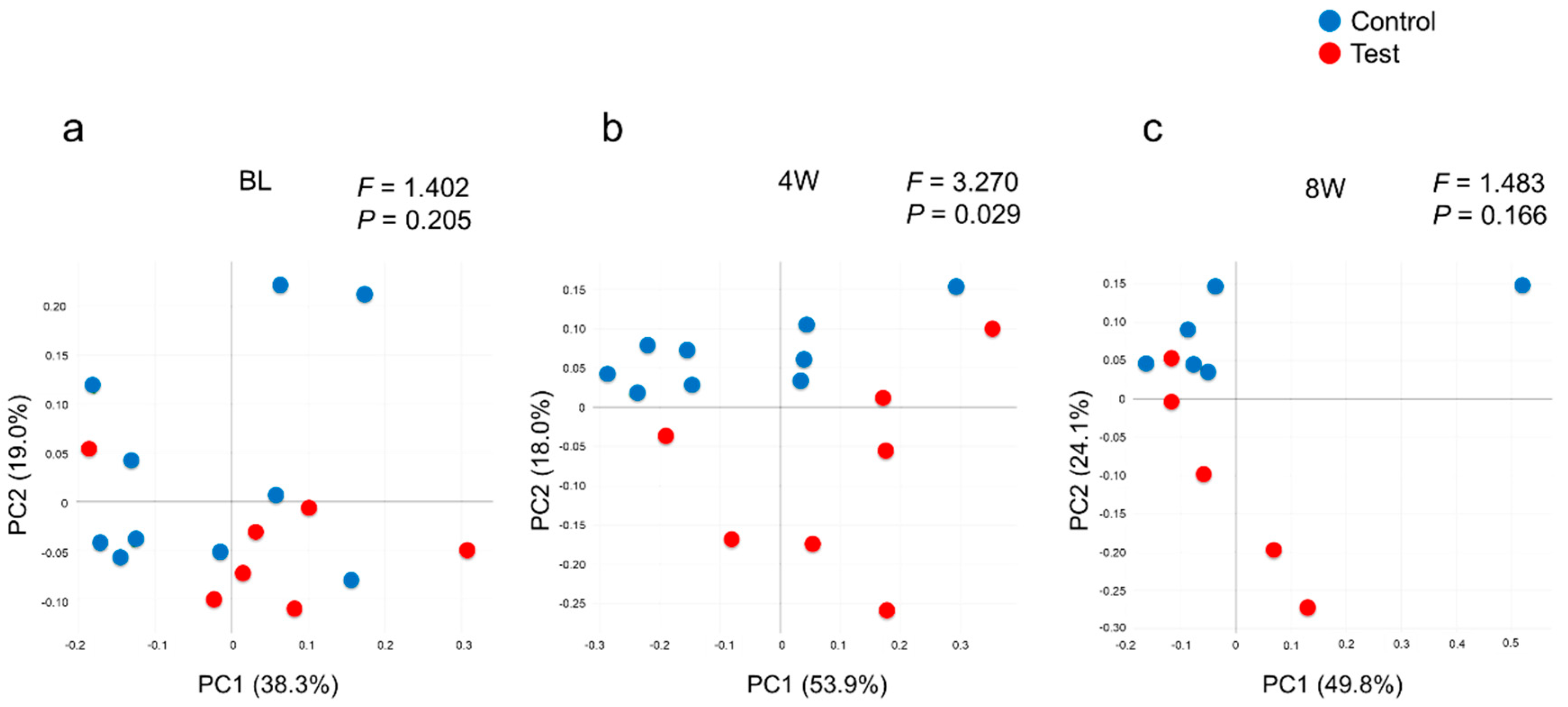
3.3.2. Diversity
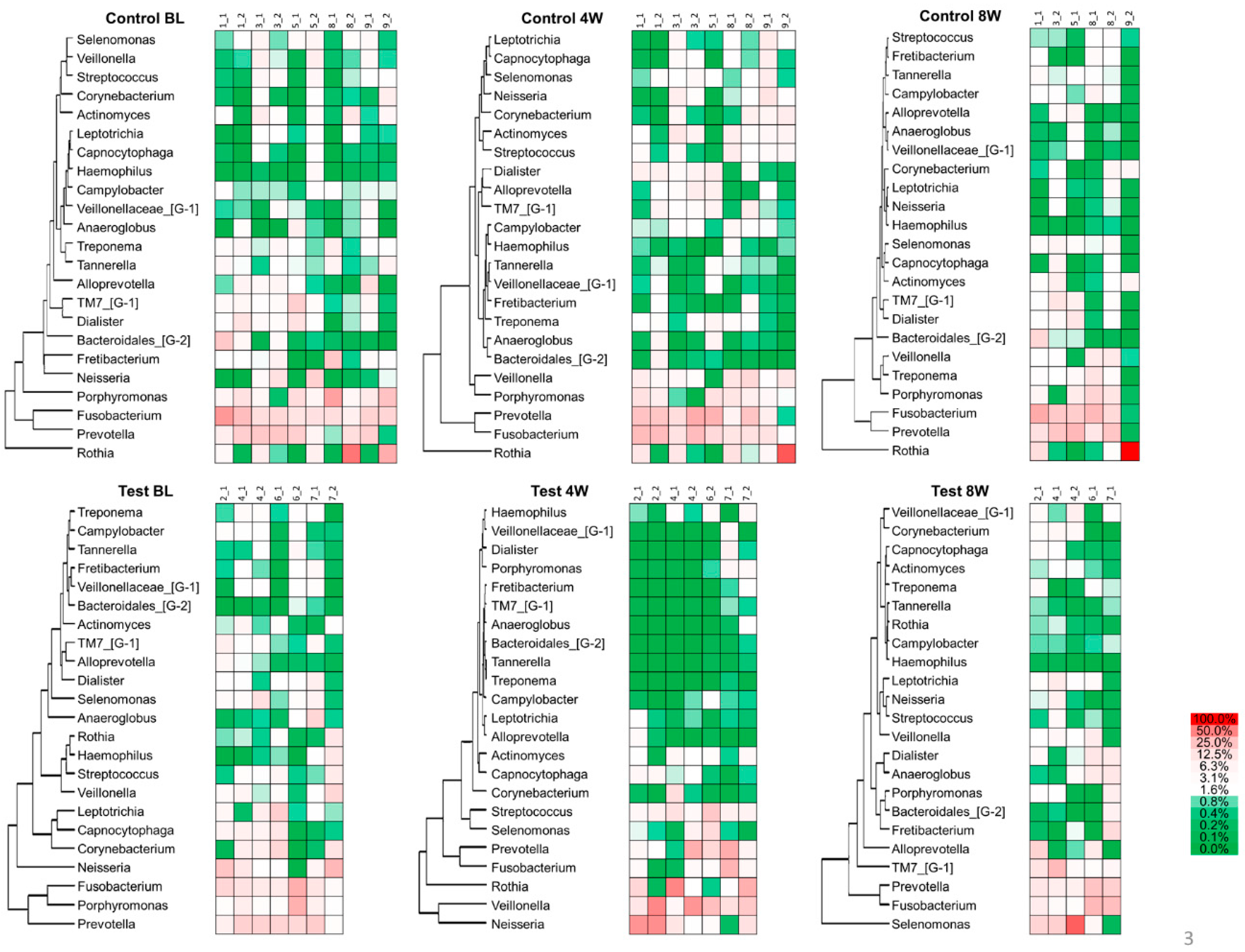
3.3.3. Heatmap Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| BH FDR | Benjamini and Hochberg false discovery rate |
| BOP | Bleeding on probing |
| CAL | Clinical attachment level |
| HOMD | Human oral microbiome database |
| OTUs | Operational taxonomic units |
| PCoA | Principal coordinates analysis |
| PCR | Plaque control record |
| PERMANOVA | Permutational multivariate analysis of variance |
| PPD | Probing pocket depth |
| QIIME | Quantitative insights into microbial ecology |
| SD | Standard deviation |
| SPT | Supportive periodontal therapy |
| TE buffer | Tris-EDTA (ethylene diamine tetra acetic acid) buffer |
References
- Okui, T.; Aoki-Nonaka, Y.; Nakajima, T.; Yamazaki, K. The Role of distinct T cell subsets in periodontitis-Studies from humans and rodent models. Curr. Oral Health Rep. 2014, 1, 114–123. [Google Scholar] [CrossRef] [Green Version]
- Bartold, P.M.; Van Dyke, T.E. An appraisal of the role of specific bacteria in the initial pathogenesis of periodontitis. J. Clin. Periodontol. 2019, 46, 6–11. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G.; Darveau, R.P.; Curtis, M.A. The keystone-pathogen hypothesis. Nat. Rev. Microbiol. 2012, 10, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Haffajee, A.D.; Socransky, S.S. Introduction to microbial aspects of periodontal biofilm communities, development and treatment. Periodontology 2000 2006, 42, 7–12. [Google Scholar] [CrossRef]
- Teles, R.P.; Haffajee, A.D.; Socransky, S.S. Microbiological goals of periodontal therapy. Periodontology 2000 2006, 42, 180–218. [Google Scholar] [CrossRef]
- Mombelli, A. Microbial colonization of the periodontal pocket and its significance for periodontal therapy. Periodontol 2000 2018, 76, 85–96. [Google Scholar] [CrossRef]
- Herrera, D.; Alonso, B.; León, R.; Roldán, S.; Sanz, M. Antimicrobial therapy in periodontitis: The use of systemic antimicrobials against the subgingival biofilm. J. Clin. Periodontol. 2008, 35 (Suppl. S8), 45–66. [Google Scholar] [CrossRef]
- Walker, C.B.; Karpinia, K.; Baehni, P. Chemotherapeutics: Antibiotics and other antimicrobials. Periodontology 2000 2004, 36, 146–165. [Google Scholar] [CrossRef]
- Nakagawa, T.; Yamada, S.; Oosuka, Y.; Saito, A.; Hosaka, Y.; Ishikawa, T.; Okuda, K. Clinical and microbiological study of local minocycline delivery (Periocline) following scaling and root planing in recurrent periodontal pockets. Bull. Tokyo Dent. Coll. 1991, 32, 63–70. [Google Scholar]
- Hsein-Kun, L.; Chong-Ji, C. Efficacy of Subgingivally Applied Minocycline in the Treatment of Chronic Periodontitis. J. Periodontal Res. 2005, 40, 20–27. [Google Scholar] [CrossRef]
- Murayama, Y.; Yamaoka, A.; Ishikawa, I.; Hori, T.; Umemoto, T.; Ueno, K. Local administration of minocycline in periodontal disease: Double blind comparative study of LS-007. Recent Adv. Clin. Periodontol. 1988, 30, 215–218. [Google Scholar]
- O’Leary, T.J.; Drake, R.B.; Naylor, J.E. The plaque control record. J. Periodontol. 1972, 43, 38. [Google Scholar] [CrossRef]
- Maeda, H.; Fujimoto, C.; Haruki, Y.; Maeda, T.; Kokeguchi, S.; Petelin, M.; Arai, H.; Tanimoto, I.; Nishimura, F.; Takashiba, S. Quantitative real-time PCR using TaqMan and SYBR Green for Actinobacillus actinomycetemcomitans, Porphyromonas gingivalis, Prevotella intermedia, tetQ gene and total bacteria. Fems Immunol. Med. Microbiol. 2003, 39, 81–86. [Google Scholar] [CrossRef] [Green Version]
- Morillo, J.M.; Lau, L.; Sanz, M.; Herrera, D.; Silva, A. Quantitative real-time PCR based on single copy gene sequence for detection of Actinobacillus actinomycetemcomitans and Porphyromonas gingivalis. J. Periodontal Res. 2003, 38, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Shelburne, C.E.; Prabhu, A.; Gleason, R.M.; Mullally, B.H.; Coulter, W.A. Quantitation of Bacteroides forsythus in subgingival plaque comparison of immunoassay and quantitative polymerase chain reaction. J. Microbiol. Methods 2000, 39, 97–107. [Google Scholar] [CrossRef]
- Yoshida, A.; Kawada, M.; Suzuki, N.; Nakano, Y.; Oho, T.; Saito, T.; Yamashita, Y. TaqMan real-time polymerase chain reaction assay for the correlation of Treponema denticola numbers with the severity of periodontal disease. Oral Microbiol. Immunol. 2004, 19, 196–200. [Google Scholar] [CrossRef]
- LaMonte, M.J.; Genco, R.J.; Buck, M.J.; McSkimming, D.I.; Li, L.; Hovey, K.M.; Andrews, C.A.; Zheng, W.; Sun, Y.; Millen, A.E.; et al. Composition and diversity of the subgingival microbiome and its relationship with age in postmenopausal women: An epidemiologic investigation. BMC Oral Health 2019, 19, 246. [Google Scholar] [CrossRef] [Green Version]
- Becker, W.; Becker, B.E.; Caffesse, R.; Kerry, G.; Ochsenbein, C.; Morrison, E.; Prichard, J. A longitudinal study comparing scaling, osseous surgery, and modified Widman procedures: Results after 5 years. J. Periodontol. 2001, 72, 1675–1684. [Google Scholar] [CrossRef]
- Matuliene, G.; Pjetursson, B.E.; Salvi, G.E.; Schmidlin, K.; Brägger, U.; Zwahlen, M.; Lang, N.P. Influence of residual pockets on progression of periodontitis and tooth loss: Results after 11 years of maintenance. J. Clin. Periodontol. 2008, 35, 685–695. [Google Scholar] [CrossRef]
- Loos, B.H.; Needleman, I. Endpoints of active periodontal therapy. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 61–71. [Google Scholar] [CrossRef] [Green Version]
- Tomasi, C.; Wennstrom, J.L. Is the use of differences in the magnitude of CAL gain appropriate for making conclusions on the efficacy of non-surgical therapeutic means? J. Clin. Periodontol. 2017, 44, 601–602. [Google Scholar] [CrossRef]
- Renvert, S.; Persson, G.R. Supportive periodontal therapy. Periodontology 2000 2004, 36, 179–195. [Google Scholar] [CrossRef]
- Tomasi, C.; Schander, K.; Dahlén, G.; Wennström, J.L. Short-term clinical and microbiologic effects of pocket debridement with an Er:YAG laser during periodontal maintenance. J. Periodontol. 2006, 77, 111–118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mongardini, C.; Di Tanna, G.L.; Pilloni, A. Light-activated disinfection using a light-emitting diode lamp in the red spectrum: Clinical and microbiological short-term findings on periodontitis patients in maintenance. A randomized controlled split-mouth clinical trial. Lasers Med. Sci. 2014, 29, 1–8. [Google Scholar] [CrossRef]
- Mdala, I.; Olsen, I.; Haffajee, A.D.; Socransky, S.S.; de Blasio, B.F.; Thoresen, M. Multilevel analysis of bacterial counts from chronic periodontitis after root planing/scaling, surgery, and systemic and local antibiotics: 2-year results. J. Oral Microbiol. 2013, 5, 1–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petelin, M.; Perkič, K.; Seme, K.; Gašpirc, B. Effect of repeated adjunctive antimicrobial photodynamic therapy on subgingival periodontal pathogens in the treatment of chronic periodontitis. Lasers Med. Sci. 2015, 30, 1647–1656. [Google Scholar] [CrossRef] [PubMed]
- Müller Campanile, V.S.; Giannopoulou, C.; Campanile, G.; Cancela, J.A.; Mombelli, A. Single or repeated antimicrobial photodynamic therapy as adjunct to ultrasonic debridement in residual periodontal pockets: Clinical, microbiological, and local biological effects. Lasers Med. Sci. 2015, 30, 27–34. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ratka-Krüger, P.; Mahl, D.; Deimling, D.; Mönting, J.S.; Jachmann, I.; Al-Machot, E.; Sculean, A.; Berakdar, M.; Jervøe-Storm, P.M.; Braun, A. Er: YAG laser treatment in supportive periodontal therapy. J. Clin. Periodontol. 2012, 39, 483–489. [Google Scholar]
- Tonetti, M.S.; Lang, N.P.; Cortellini, P.; Suvan, J.E.; Eickholz, P.; Fourmousis, I.; Topoll, H.; Vangsted, T.; Wallkamm, B. Effects of a single topical doxycycline administration adjunctive to mechanical debridement in patients with persistent/recurrent periodontitis but acceptable oral hygiene during supportive periodontal therapy. J. Clin. Periodontol. 2012, 39, 475–482. [Google Scholar] [CrossRef]
- Abusleme, L.; Dupuy, A.K.; Dutzan, N.; Silva, N.; Burleson, J.A.; Strausbaugh, L.D.; Gamonal, J.; Diaz, P.I. The subgingival microbiome in health and periodontitis and its relationship with community biomass and inflammation. ISME J. 2013, 7, 1016–1025. [Google Scholar] [CrossRef] [Green Version]
- Griffen, A.L.; Beall, C.J.; Campbell, J.H.; Firestone, N.D.; Kumar, P.S.; Yang, Z.K.; Podar, M.; Leys, E.J. Distinct and complex bacterial profiles in human periodontitis and health revealed by 16S pyrosequencing. ISME J. 2012, 6, 1176–1185. [Google Scholar] [CrossRef] [Green Version]
- Jünemann, S.; Prior, K.; Szczepanowski, R.; Harks, I.; Ehmke, B.; Goesmann, A.; Stoye, J.; Harmsen, D. Bacterial community shift in treated periodontitis patients revealed by ion torrent 16S rRNA gene amplicon sequencing. PLoS ONE 2012, 7, e41606. [Google Scholar] [CrossRef] [Green Version]
- Ott, S.J.; Musfeldt, M.; Wenderoth, D.F.; Hampe, J.; Brant, O.; Fölsch, U.R.; Timmis, K.N.; Schreiber, S. Reduction in diversity of the colonic mucosa associated bacterial microflora in patients with active inflammatory bowel disease. Gut 2004, 53, 685–693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hedin, C.; van der Gast, C.J.; Rogers, G.B.; Cuthbertson, L.; McCartney, S.; Stagg, A.J.; Lindsay, J.O.; Whelan, K. Siblings of patients with Crohn’s disease exhibit a biologically relevant dysbiosis in mucosal microbial metacommunities. Gut 2016, 65, 944–953. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, Y.; He, J.; He, Z.; Zhou, Y.; Yuan, M.; Xu, X.; Sun, F.; Liu, C.; Li, J.; Xie, W.; et al. Phylogenetic and functional gene structure shifts of the oral microbiomes in periodontitis patients. ISME J. 2014, 8, 1879–1891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Szafranski, S.P.; Wos-Oxley, M.L.; Vilchez-Vargas, R.; Jáuregui, R.; Plumeier, I.; Klawonn, F.; Tomasch, J.; Meisinger, C.; Kühnisch, J.; Sztajer, H.; et al. High-resolution taxonomic profiling of the subgingival microbiome for biomarker discovery and periodontitis diagnosis. Appl. Environ. Microbiol. 2015, 81, 1047–1058. [Google Scholar] [CrossRef] [Green Version]
- Wang, Q.; Jotwani, R.; Le, J.; Krauss, J.L.; Potempa, J.; Coventry, S.C.; Uriarte, S.M.; Richard, J.; Lamont, R.J. Filifactor alocis infection and inflammatory responses in the mouse subcutaneous chamber model. Infect. Immun. 2014, 82, 1205–1212. [Google Scholar] [CrossRef] [Green Version]
- Bedree, J.K.; Bor, B.; Cen, L.; Edlund, A.; Lux, R.; McLean, J.S.; Shi, W.; He, X.; Bedree, J.K. Quorum sensing modulates the epibiotic-parasitic relationship between Actinomyces odontolyticus and its Saccharibacteria epibiont, a nanosynbacter lyticus strain, TM7x. Front. Microbiol. 2018, 24, 2049. [Google Scholar] [CrossRef] [Green Version]
- Miralda, I.; Vashishta, A.; Rogers, M.N.; Rouchka, E.C.; Li, X.; Waigel, S.; Lamont, R.J.; Uriarte, S.M. Whole Transcriptome analysis reveals that filifactor alocis Modulates TNFα-Stimulated MAPK Activation in human neutrophils. Front. Immunol. 2020, 16, 497. [Google Scholar] [CrossRef]
- Satomi, A.; Uracuchi, R.; Noguchi, T.; Ishikawa, I.; Tamura, H.; Kitamura, M. Minocycline HCl concentration in periodontal pocket after administration of LS-007. J. Jpn. Assoc. Periodontol. 1987, 29, 937–943. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean ± SD | Control (n = 5) | Test (n = 4) | p-Value |
|---|---|---|---|
| Age (years) | 67.4 ± 11.1 | 65.5 ± 2.1 | 0.72 |
| Gender, female (%) | 80 | 75 | 1.00 |
| Whole-mouth PPD (mm) | 2.41 ± 0.30 | 2.13 ± 0.36 | 0.32 |
| Whole-mouth CAL (mm) | 3.05 ± 0.57 | 2.88 ± 0.29 | 0.63 |
| Whole-mouth BOP (%) | 5.36 ± 3.43 | 5.09 ± 3.49 | 0.92 |
| Whole-mouth PCR (%) | 3.75 ± 2.93 | 14.39 ± 16.35 | 0.34 |
| Control (n = 10) | Test (n = 8) | p-Value 1 | ||
|---|---|---|---|---|
| PPD (mm) | BL | 6.20 ± 1.32 | 5.50 ± 0.53 | 0.315 |
| mean ± sd | 4W | 6.20 ± 1.32 | 5.38 ± 0.74 | 0.237 |
| 8W | 6.20 ± 1.14 | 5.13 ± 0.99 | 0.101 | |
| p-value 2 | 1.000 | 0.607 | ||
| CAL (mm) | BL | 6.90 ± 1.37 | 5.88 ± 0.83 | 0.122 |
| mean ± sd | 4W | 6.70 ± 1.25 | 5.38 ± 0.74 | 0.027 |
| 8W | 6.80 ± 1.23 | 5.63 ± 0.74 | 0.043 | |
| p-value | 0.549 | 0.171 | ||
| BOP (positive %) | BL | 100 | 100 | 1.000 |
| 4W | 90 | 13 ** | 0.003 | |
| 8W | 80 | 13 ** | 0.015 | |
| p-value | 0.368 | 0.002 | ||
| PCR (positive %) | BL | 20 | 25 | 1.000 |
| 4W | 20 | 13 | 1.000 | |
| 8W | 10 | 13 | 1.000 | |
| p-value | 0.717 | 0.717 |
| Control | Test | p-Value 1 | ||
|---|---|---|---|---|
| Total bacteria | BL | 6.30 ± 1.00 | 6.85 ± 0.72 | 0.408 |
| 4W | 5.67 ± 1.92 | 4.97 ± 2.44 | 0.515 | |
| 8W | 5.44 ± 2.14 | 5.12 ± 2.83 | 0.897 | |
| p-value 2 | 0.836 | 0.607 | ||
| Porphyromonas gingivalis | BL | 3.80 ± 1.67 | 3.97 ± 1.98 | 0.696 |
| 4W | 3.36 ± 1.47 | 1.73 ± 1.57 * | 0.043 | |
| 8W | 2.50 ± 1.81 | 1.77 ± 1.64 | 0.360 | |
| p-value | 0.117 | 0.006 | ||
| Tannerella forsythia | BL | 4.64 ± 1.78 | 4.72 ± 1.98 | 0.762 |
| 4W | 3.66 ± 1.86 | 1.81 ± 1.21 ** | 0.043 | |
| 8W | 3.68 ± 2.05 | 2.29 ± 1.55 ** | 0.122 | |
| p-value | 0.067 | 0.002 | ||
| Treponema denticola | BL | 3.06 ± 1.85 | 2.82 ± 1.74 | 0.7623 |
| 4W | 2.98 ± 1.60 | 1.26 ± 0.59 * | 0.006 | |
| 8W | 2.83 ± 1.66 | 2.01 ± 1.62 | 0.274 | |
| p-value | 0.641 | 0.050 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miyazawa, H.; Nakajima, T.; Horimizu, M.; Okuda, K.; Sugita, N.; Yamazaki, K.; Li, L.; Hayashi-Okada, Y.; Arita, T.; Nishimoto, M.; et al. Impact of Local Drug Delivery of Minocycline on the Subgingival Microbiota during Supportive Periodontal Therapy: A Randomized Controlled Pilot Study. Dent. J. 2020, 8, 123. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8040123
Miyazawa H, Nakajima T, Horimizu M, Okuda K, Sugita N, Yamazaki K, Li L, Hayashi-Okada Y, Arita T, Nishimoto M, et al. Impact of Local Drug Delivery of Minocycline on the Subgingival Microbiota during Supportive Periodontal Therapy: A Randomized Controlled Pilot Study. Dentistry Journal. 2020; 8(4):123. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8040123
Chicago/Turabian StyleMiyazawa, Haruna, Takako Nakajima, Makoto Horimizu, Kazuhiro Okuda, Noriko Sugita, Kyoko Yamazaki, Lu Li, Yoshiko Hayashi-Okada, Takuya Arita, Misa Nishimoto, and et al. 2020. "Impact of Local Drug Delivery of Minocycline on the Subgingival Microbiota during Supportive Periodontal Therapy: A Randomized Controlled Pilot Study" Dentistry Journal 8, no. 4: 123. https://0-doi-org.brum.beds.ac.uk/10.3390/dj8040123