
Use of a Knowledge-Based Governance Approach to Plan a Post-COVID-19 Predoctoral Dental Curriculum


Abstract
:1. Introduction
2. Process
3. Findings
3.1. Delivering Didactic Courses Remotely
3.2. Administering Assessments Remotely
3.3. Split Shift in the Preclinical Simulation Lab
3.4. Conversion to Credit/No Credit Grading from a Numerical (4.0) Grading Scale
4. Recommendations and Discussion
4.1. Delivering Didactic Courses Remotely
4.2. Administering Assessments Remotely
4.3. Split Shift in the Preclinical Simulation Lab
4.4. Conversion to Credit/No Credit Grading from a Numerical (4.0) Grading Scale
4.5. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| ALL-FACULTY AND ALL-STUDENT SURVEY RESULTS | ||||||
|---|---|---|---|---|---|---|
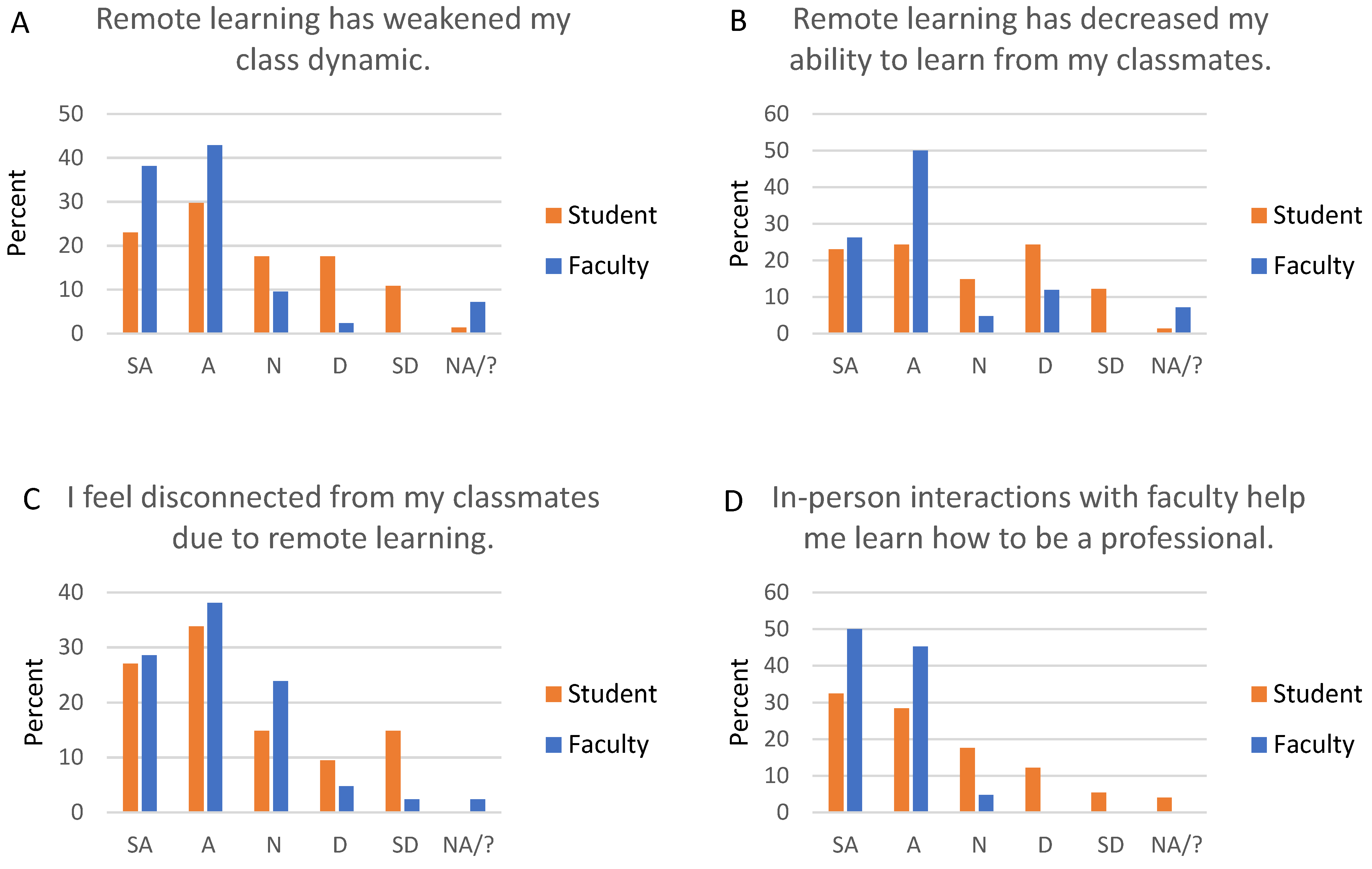
| Statements Related to Social Impacts of Remote Learning. | ||||||
| SA | A | N | D | SD | NA/? | |
| FACULTY | ||||||
| Remote learning has weakened dental student class dynamics. | 16 | 18 | 4 | 1 | 0 | 3 |
| Remote learning has decreased student’s ability to learn from their classmates. | 11 | 21 | 2 | 5 | 0 | 3 |
| I feel disconnected from students due to remote learning. | 12 | 16 | 10 | 2 | 1 | 1 |
| In-person interactions with faculty help students learn how to be a professional. | 21 | 19 | 2 | 0 | 0 | 0 |
| STUDENT | ||||||
| Remote learning has weakened by class dynamic. | 17 | 22 | 13 | 13 | 8 | 1 |
| Remote learning has decreased my ability to learn from my classmates. | 17 | 18 | 11 | 18 | 9 | 1 |
| I feel disconnected from my classmates due to remote learning. | 20 | 25 | 11 | 7 | 11 | 0 |
| I feel disconnected from faculty due to remote learning. | 20 | 13 | 16 | 17 | 8 | 0 |
| I have formed study groups during remote learning. | 13 | 19 | 10 | 18 | 12 | 2 |
| In-person interactions with faculty help me learn how to be a professional. | 24 | 21 | 13 | 9 | 4 | 3 |
| Statements related to didactics. Didactics can be lectures or small group seminars/discussions. Didactics can be in-person, remote synchronous (i.e., Zoom), or remote asynchronous (i.e., pre-recorded). | ||||||
| SA | A | N | D | SD | NA/? | |
| FACULTY | ||||||
| Students log on to my Zoom sessions, but typically do not actively engage in them. | 5 | 11 | 8 | 5 | 2 | 11 |
| I prefer students to have their cameras ON during Zoom sessions. | 18 | 11 | 4 | 0 | 1 | 8 |
| Technical difficulties often hinder my Zoom sessions. | 1 | 4 | 5 | 18 | 5 | 9 |
| I understand students’ level of comprehension better when didactics are in-person. | 13 | 17 | 3 | 2 | 3 | 4 |
| I am able to read the room and adjust my teaching in real time better during in-person didactics. | 16 | 19 | 1 | 1 | 0 | 5 |
| Students are more likely to ask questions or speak up during an in-person didactic session (versus a Zoom session). | 14 | 15 | 3 | 2 | 1 | 6 |
| I like students to be able to ask questions in real time. | 19 | 18 | 3 | 0 | 0 | 2 |
| I appreciate the flexibility of pre-recorded asynchronous lectures. | 6 | 17 | 5 | 5 | 2 | 7 |
| It takes me longer to prepare a quality pre-recorded lecture than it does to deliver an in-person lecture. | 15 | 7 | 7 | 6 | 0 | 7 |
| In general, I prefer in-person didactics. | 17 | 13 | 6 | 3 | 1 | 2 |
| In general, I prefer pre-recorded asynchronous lectures (versus in-person lectures or Zoom lectures). | 0 | 3 | 11 | 15 | 10 | 3 |
| STUDENT | ||||||
| I log on to Zoom sessions, but typically do not actively engage in them. | 22 | 16 | 12 | 15 | 9 | 0 |
| It is difficult to focus during Zoom sessions. | 4 | 16 | 12 | 30 | 12 | 0 |
| I prefer to have my camera OFF during Zoom sessions. | 19 | 29 | 20 | 6 | 0 | 0 |
| I often have technical difficulties that hinder Zoom sessions. | 1 | 5 | 10 | 27 | 31 | 0 |
| Faculty understand my level of comprehension better when didactics are in-person. | 16 | 20 | 11 | 10 | 9 | 8 |
| I am more likely to ask a question or speak up during an in-person didactic session (versus a Zoom session). | 16 | 9 | 7 | 18 | 21 | 3 |
| I like the ability to ask questions in real time. | 19 | 22 | 22 | 9 | 2 | 0 |
| I appreciate the flexibility of pre-recorded asynchronous lectures. | 47 | 18 | 6 | 2 | 1 | 0 |
| In general, I prefer in-person didactics. | 19 | 10 | 14 | 12 | 17 | 2 |
| In general, I prefer pre-recorded asynchronous lectures (versus in-person lectures or Zoom lectures). | 26 | 12 | 19 | 10 | 7 | 0 |
| Statements related to remote exams. This could also mean quizzes. | ||||||
| SA | A | N | D | SD | NA/? | |
| FACULTY | ||||||
| Students study less when an exam is open-book. | 10 | 12 | 8 | 6 | 1 | 5 |
| Students learn less when an exam is open-book. | 4 | 10 | 14 | 7 | 2 | 5 |
| I have concerns about academic dishonesty when exams are not proctored. | 8 | 18 | 5 | 6 | 0 | 5 |
| I am comfortable with the use of remote proctoring via a Zoom proctor. | 1 | 6 | 9 | 6 | 6 | 14 |
| I am comfortable with the use of remote proctoring via automated software (e.g., Proctorio). | 1 | 5 | 9 | 7 | 5 | 15 |
| STUDENT | ||||||
| I study less when an exam is open-book. | 6 | 22 | 10 | 28 | 8 | 0 |
| I learn less when an exam is open-book. | 6 | 10 | 10 | 29 | 19 | 0 |
| I have concerns about academic dishonesty when exams are not proctored. | 8 | 16 | 17 | 20 | 12 | 1 |
| I am comfortable with remote proctoring via a Zoom proctor. | 7 | 23 | 15 | 18 | 11 | 0 |
| I am comfortable with remote proctoring via automated software (e.g., Proctorio). | 4 | 17 | 15 | 14 | 22 | 2 |
| It is difficult for me to find a suitable (quiet, private) space to take a remote exam. | 11 | 9 | 11 | 25 | 18 | 0 |
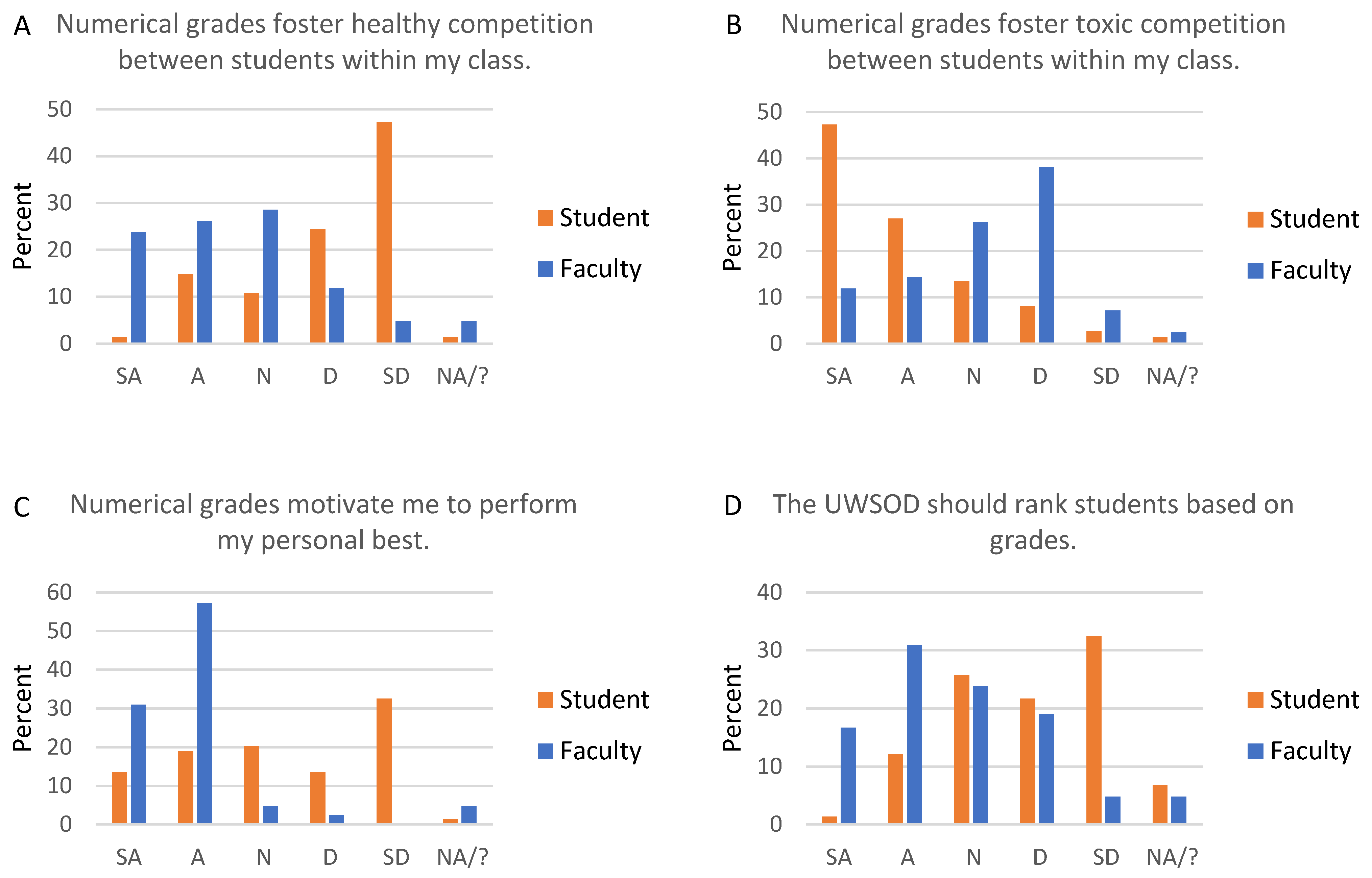
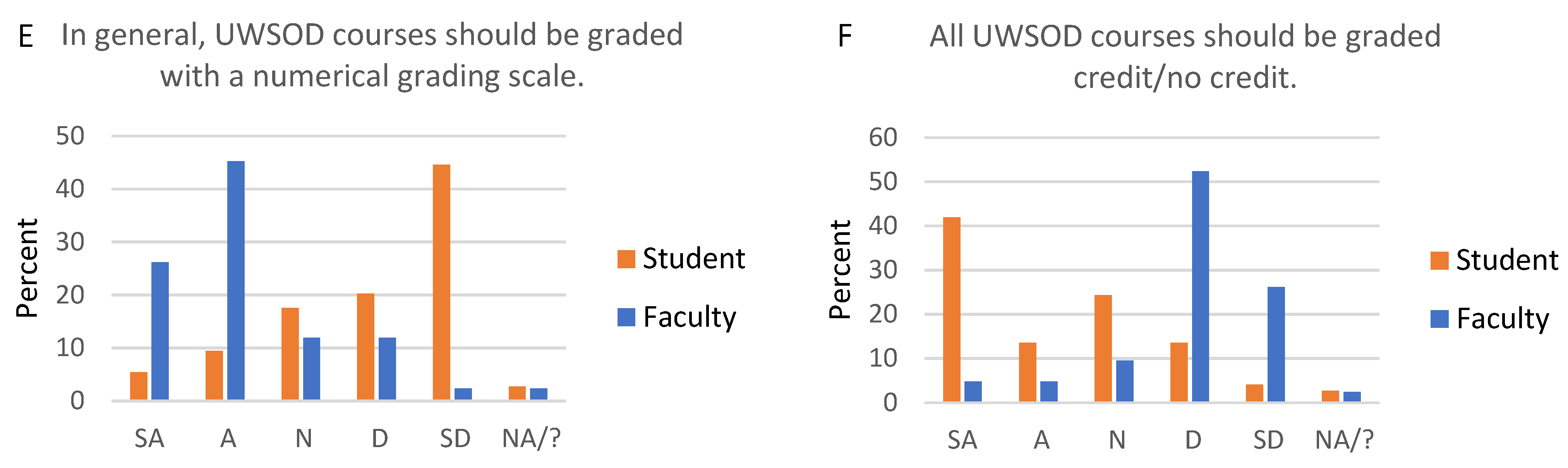
| Statements related to course grading schemes: numerical grades (4.0 scale) versus credit/no credit grades. | ||||||
| SA | A | N | D | SD | NA/? | |
| FACULTY | ||||||
| Numerical grades foster healthy competition between students within a class. | 10 | 11 | 12 | 5 | 2 | 2 |
| Numerical grades foster toxic competition between students within a class. | 5 | 6 | 11 | 16 | 3 | 1 |
| Numerical grades motivate students to perform their personal best. | 13 | 24 | 2 | 1 | 0 | 2 |
| Credit/no credit grades motivate students to perform “good enough”. | 8 | 18 | 11 | 2 | 2 | 1 |
| Students study more in a course with a numerical grading scale. | 16 | 22 | 2 | 0 | 0 | 2 |
| Students learn more in a course with a numerical grading scale. | 6 | 18 | 10 | 1 | 3 | 4 |
| I am concerned credit/no credit grades may impact students’ post-graduation plans. | 11 | 16 | 7 | 3 | 2 | 3 |
| Students are more likely to contest individual points on an assessment in a course with a numerical grading scale. | 12 | 22 | 3 | 1 | 0 | 4 |
| I am concerned about calibration of graders in a course with a numerical grading scale. | 5 | 21 | 9 | 4 | 0 | 3 |
| Numerical grades foster academic excellence at the UWSOD. | 11 | 21 | 5 | 3 | 0 | 2 |
| The UWSOD should rank students based on grades. | 7 | 13 | 10 | 8 | 2 | 2 |
| In general, UWSOD courses should be graded with a numerical grading scale. | 11 | 19 | 5 | 5 | 1 | 1 |
| All UWSOD courses should be graded credit/no credit. | 2 | 2 | 4 | 22 | 11 | 1 |
| STUDENT | ||||||
| Numerical grades foster healthy competition between students within my class. | 1 | 11 | 8 | 18 | 35 | 1 |
| Numerical grades foster toxic competition between students within my class. | 35 | 20 | 10 | 6 | 2 | 1 |
| Numerical grades motivate me to perform my personal best. | 10 | 14 | 15 | 10 | 24 | 1 |
| Credit/no credit grades motivate me to perform “good enough”. | 6 | 18 | 7 | 17 | 24 | 2 |
| I study more in a course with a numerical grading scale. | 7 | 17 | 12 | 13 | 21 | 4 |
| I learn more in a course with a numerical grading scale. | 6 | 4 | 10 | 22 | 29 | 3 |
| I am concerned credit/no credit grades may impact my post-graduation plans. | 4 | 9 | 13 | 16 | 30 | 2 |
| I am more likely to contest individual points on an assessment in a course with a numerical grading scale. | 36 | 18 | 10 | 6 | 4 | 0 |
| I am concerned about calibration of graders in a course with a numerical grading scale. | 36 | 22 | 9 | 2 | 1 | 4 |
| The UWSOD should rank students based on grades. | 1 | 9 | 19 | 16 | 24 | 5 |
| I am motivated by class rank. | 4 | 11 | 10 | 12 | 37 | 0 |
| I am more likely to collaborate with my classmates when a course is graded credit/no credit. | 30 | 15 | 12 | 12 | 3 | 2 |
| I typically study for the grade in a course with a numerical grading scale, rather than studying to become a good dentist. | 26 | 24 | 5 | 11 | 7 | 1 |
| In general, UWSOD courses should be graded with a numerical grading scale. | 4 | 7 | 13 | 15 | 33 | 2 |
| All UWSOD courses should be graded credit/no credit. | 31 | 10 | 18 | 10 | 3 | 2 |
| Statements related to courses in the preclinical simulation lab. | ||||||
| SA | A | N | D | SD | NA/? | |
| FACULTY | ||||||
| There is a disconnect between students in the two lab groups. | 3 | 4 | 2 | 2 | 1 | 30 |
| I am concerned about imbalanced experiences between two groups of students in the lab. | 1 | 3 | 4 | 4 | 1 | 29 |
| Students get greater personal attention from faculty with the split shift in the lab. | 3 | 7 | 3 | 0 | 2 | 27 |
| It is easier for students to use shared equipment with the split shift in the lab. | 2 | 7 | 3 | 0 | 1 | 29 |
| I spend more time preparing and teaching with the split shift in the lab. | 3 | 3 | 3 | 2 | 0 | 31 |
| Teaching the same course twice detracts from my other responsibilities as a faculty member. | 5 | 9 | 3 | 3 | 0 | 22 |
| STUDENT | ||||||
| I feel disconnected from classmates who do not share the same lab time as me. | 32 | 16 | 5 | 6 | 3 | 12 |
| I am concerned about imbalanced experiences between two groups of students in the lab. | 9 | 14 | 11 | 17 | 9 | 14 |
| I get greater personal attention from faculty with the split shift in the lab. | 20 | 16 | 6 | 3 | 4 | 25 |
| It is easier to use shared equipment with the split shift in the lab. | 26 | 17 | 5 | 2 | 2 | 22 |
| GRADUATE PROGRAM DIRECTOR SURVEY RESULTS | ||||||
| SA | A | N | D | SD | NA/? | |
| I consider GPA when assessing applicants to my graduate program. | 4 | 4 | 0 | 0 | 0 | 0 |
| I consider class rank when assessing applicants to my graduate program. | 5 | 2 | 1 | 0 | 0 | 0 |
| It is difficult to assess an applicant who went to a dental school that does not issue grades. | 4 | 4 | 0 | 0 | 0 | 0 |
| I prefer that applicants to my graduate program report GPA. | 6 | 2 | 0 | 0 | 0 | 0 |
| I prefer that applicants to my graduate program report class rank. | 6 | 2 | 0 | 0 | 0 | 0 |
| Class rank is a poor metric for applicants, because students within a class are separated by extremely small differences in GPA. | 0 | 1 | 3 | 3 | 1 | 0 |
| Class rank is a valuable metric for applicants, because GPAs are elevated by grade inflation. | 2 | 3 | 1 | 1 | 0 | 1 |
| I am concerned that a switch to credit/no credit grades at UWSOD may impact our students’ matriculation to graduate programs. | 3 | 5 | 0 | 0 | 0 | 0 |
| I am concerned that eliminating class rank at UWSOD may impact our students’ matriculation to graduate programs. | 4 | 3 | 0 | 1 | 0 | 0 |
| Class rank | GPA | Standardized test score | ||||
| If you could have only one piece of objective data when assessing applicants to your graduate program, which would it be? | 5 | 3 | 0 | |||
References
- Advancing Through Innovation in a Challenging Time. J. Dent. Educ. 2021, 85, 877. [CrossRef]
- Escontrias, O.A.; Istrate, E.C.; Stewart, D.C.L. Resilient Dental Schools, Better Oral Health Care for the Underserved: The Impact of the COVID-19 Pandemic on U.S. Dental Schools; ADEA Policy Research Series; American Dental Education Association: Washington, DC, USA, 2021. [Google Scholar]
- Quinn, B.; Field, J.; Gorter, R.; Akota, I.; Manzanares, M.C.; Paganelli, C.; Davies, J.; Dixon, J.; Gabor, G.; Mendes, R.A.; et al. COVID-19: The immediate response of european academic dental institutions and future implications for dental education. Eur. J. Dent. Educ. 2020, 24, 811–814. [Google Scholar] [CrossRef] [PubMed]
- Iyer, P.; Aziz, K.; Ojcius, D.M. Impact of COVID-19 on dental education in the United States. J. Dent. Educ. 2020, 84, 718–722. [Google Scholar] [CrossRef] [PubMed]
- Hattar, S.; AlHadidi, A.; Sawair, F.A.; Alraheam, I.A.; El-Ma’Aita, A.; Wahab, F.K. Impact of COVID-19 pandemic on dental education: Online experience and practice expectations among dental students at the University of Jordan. BMC Med. Educ. 2021, 21, 151. [Google Scholar] [CrossRef] [PubMed]
- Association Forum. Professional Practice Statement on Association Strategic Governance, Part II: Characteristics; Association Forum: Chilago, IL, USA, 2015. [Google Scholar]
- Schwella, E. Knowledge Based Governance, Governance as Learning: The Leadership Implications. Int. J. Leadersh. Public Serv. 2014, 10. [Google Scholar] [CrossRef]
- Tecker International. Knowledge-Based Decision Making. 2012. Available online: http://www.tecker.com/wp-content/uploads/2012/10/TIKBDMJan12.pdf (accessed on 4 April 2021).
- Masella, R.S. The hidden curriculum: Value added in dental education. J. Dent. Educ. 2006, 70, 279–283. [Google Scholar] [CrossRef] [PubMed]
- Schlenz, M.A.; Schmidt, A.; Wöstmann, B.; Krämer, N.; Schulz-Weidner, N. Students’ and lecturers’ perspective on the implementation of online learning in dental education due to SARS-CoV-2 (COVID-19): A cross-sectional study. BMC Med. Educ. 2020, 20, 354. [Google Scholar] [CrossRef] [PubMed]
- Shrivastava, K.J.; Nahar, R.; Parlani, S.; Murthy, V.J. A cross-sectional virtual survey to evaluate the outcome of online dental education system among undergraduate dental students across India amid COVID-19 pandemic. Eur. J. Dent. Educ. 2021. [Google Scholar] [CrossRef] [PubMed]
- Varvara, G.; Bernardi, S.; Bianchi, S.; Sinjari, B.; Piattelli, M. Dental Education Challenges during the COVID-19 Pandemic Period in Italy: Undergraduate Student Feedback, Future Perspectives, and the Needs of Teaching Strategies for Professional Development. Healthcare 2021, 9, 454. [Google Scholar] [CrossRef] [PubMed]
- Bartlett, T. Online Learning: What Does the Reserach Say? In Online 2.0: How to Lead a Large-Scale Transformation of Virtual Learning; The Chronicle of Higher Education: Congers, NY, USA, 2020. [Google Scholar]
- Zmiyiwsky, M.; Allen, N.; Yoon, T.; Zeller, K.; Lamichhane, P. Individual Preferences on Grading Systems in Dental Schools. Online J. Dent. Oral Health 2018, 1. [Google Scholar] [CrossRef]
- Jham, B.C.; Cannella, D.; Adibi, S.; Austin, K.; Allareddy, V.; Petrie, C.S. Should Pass/Fail Grading Be Used Instead of Traditional Letter Grades in Dental Education? Two Viewpoints: Viewpoint 1: Pass/Fail Grading Improves Learning Experiences for Students and Viewpoint 2: Traditional Letter Grading Provides Objective Evaluation for Dental Education. J. Dent. Educ. 2018, 82, 1258–1264. [Google Scholar] [PubMed] [Green Version]
- Ramaswamy, V.; Veremis, B.; Nalliah, R.P. Making the case for pass-fail grading in dental education. Eur. J. Dent. Educ. 2020, 24, 601–604. [Google Scholar] [CrossRef] [PubMed]
- Cuculino, L. How Pass/Fail Grading Can Impact the Dental School Experience. ASDA Blog. December 2019. Available online: https://www.asdablog.com/how-pass-fail-grading-can-impact-the-dental-school-experience/ (accessed on 4 April 2021).
- McCarty, B. P’s Get Degrees: Pass/Fail Grading in Dental School. ASDA Blog. March 2015. Available online: https://www.asdablog.com/ps-get-degrees-pass-fail-grading-in-dental-school/ (accessed on 4 April 2021).
- Oak, S. A Review of Dental School Pass/Fail Curriculum. ASDA Blog. July 2020. Available online: https://www.asdablog.com/a-review-of-the-dental-school-pass-fail-curriculum/ (accessed on 4 April 2021).
- Valachovic, R. Making the Grade in a Pass/Fail Environment: What It Means for Students. ADEA Charting Progress. December 2014. Available online: https://adeachartingprogress.wordpress.com/2014/12/15/making-the-grade-in-a-passfail-environment-what-it-means-for-students/ (accessed on 4 April 2021).
- Valachovic, R. Making the Grade in a Pass/Fail Environment: Challenges for Advanced Dental Education Programs. ADEA Charting Progress. January 2015. Available online: https://adeachartingprogress.wordpress.com/2015/01/ (accessed on 4 April 2021).
- Eidelman, A.S.; Whitmer, T. Is the Advanced Dental Admission Test (ADAT) the Metric Needed to Assist with Postgraduate Admissions? Two Viewpoints: Viewpoint 1: The ADAT Provides a Viable Solution to Help Postgraduate Programs Differentiate Applicants and Viewpoint 2: The ADAT Has Questionable Utility and Value for Postgraduate Admissions. J. Dent. Educ. 2017, 81, 685–690. [Google Scholar] [PubMed] [Green Version]
- Bell, L.T.; Sukotjo, C.; Yuan, J.C.-C.; Johnson, B.R. Applicant selection procedures in endodontic specialty programs in the United States: Program director’s perspective. J. Endod. 2014, 40, 797–804. [Google Scholar] [CrossRef] [PubMed]
- Justema, R.B.; Majewski, R.F.; Salzmann, L.; Murdoch-Kinch, C.A.; Boynton, J.R. Contemporary appraisal of factors influencing pediatric dental program directors’ selection of residents. J. Dent. Educ. 2020, 84, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Carmosino, A.J.; Yuan, J.C.-C.; Lucchiari, N.; Kawar, N.; Sukotjo, C. Postdoctoral Periodontal Program Directors’ Perspectives of Resident Selection. J. Periodontol. 2015, 86, 177–184. [Google Scholar] [CrossRef] [PubMed]



| Students | Faculty |
|---|---|
| Class of 2021 | Foundations faculty |
| Class of 2022 | Preclinical faculty |
| Class of 2023 | Clerkship Directors |
| Class of 2024 | Graduate Program Directors |
| Staff | Administration |
| Scheduler | Associate Dean of Academic Affairs and |
| Director of Information Technology Educational Technology Specialist Preclinical Lab Support | Associate Dean of Student Services and Admissions |
| Faculty Demographics | Student Demographics |
|---|---|
| Total faculty responses, n = 42 | Total student responses, n = 74 |
| Regular faculty appointments, n = 33 | Class of 2021, n = 8 |
| Affiliate faculty appointments, n = 9 | Class of 2022, n = 23 |
| Time worked in dental education: | Class of 2023, n = 12 |
| 0–5 years, n = 8 | Class of 2024, n = 31 |
| 6–10 years, n = 4 | Students reporting age, n = 55 |
| 11–20 years, n = 10 | Median age = 25 years |
| >20 years, n = 20 | Mean age = 26 years |
| Teach in these predoc settings: | Age range = 21–44 years |
| Foundations, n = 9 | Students reporting gender identity, n = 55 |
| Preclinical dental courses, n = 21 | Female/woman, n = 32 |
| Clinical dental courses, n = 21 | Male/man, n = 22 |
| Clinic, n = 18 | Genderqueer/non-binary, n = 1 |
| Other, n = 1 | |
| Do not teach predoc, n = 3 | |
| Teach in >1 predoc setting, n = 18 | |
| Course director for predoc course, n = 22 | |
| Faculty reporting age, n = 30 | |
| Median age = 57 years | |
| Mean age = 55 years | |
| Age range = 29–75 years | |
| Faculty reporting gender identity, n = 29 | |
| Female/woman, n = 13 | |
| Male/man, n = 16 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Flake, N.M.; Chan, D.C.N.; DiMarco, A.C.; Silverstein, B.D. Use of a Knowledge-Based Governance Approach to Plan a Post-COVID-19 Predoctoral Dental Curriculum. Dent. J. 2021, 9, 142. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9120142
Flake NM, Chan DCN, DiMarco AC, Silverstein BD. Use of a Knowledge-Based Governance Approach to Plan a Post-COVID-19 Predoctoral Dental Curriculum. Dentistry Journal. 2021; 9(12):142. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9120142
Chicago/Turabian StyleFlake, Natasha M., Daniel C. N. Chan, Arthur C. DiMarco, and Bruce D. Silverstein. 2021. "Use of a Knowledge-Based Governance Approach to Plan a Post-COVID-19 Predoctoral Dental Curriculum" Dentistry Journal 9, no. 12: 142. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9120142