
Survival Rate of Zygomatic Implants for Fixed Oral Maxillary Rehabilitations: A Systematic Review and Meta-Analysis Comparing Outcomes between Zygomatic and Regular Implants

 ,
,  ,
,
Abstract
:1. Introduction
- Class I: teeth present.
- Class II: immediate post-extraction socket.
- Class III: edentulous ridge with adequate height and width of bone.
- Class IV: knife-edge ridge, adequate bone height but inadequate in width.
- Class V: flat bone ridge, bone inadequate in width and height.
- Class VI: depressed-form ridge, basal bone resorption.
2. Materials and Methods
2.1. Database Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Papers Selection Procedure
2.4. Study Assessment
2.5. Risk of Bias Assessment
2.6. Comparative Meta-Analysis
3. Results
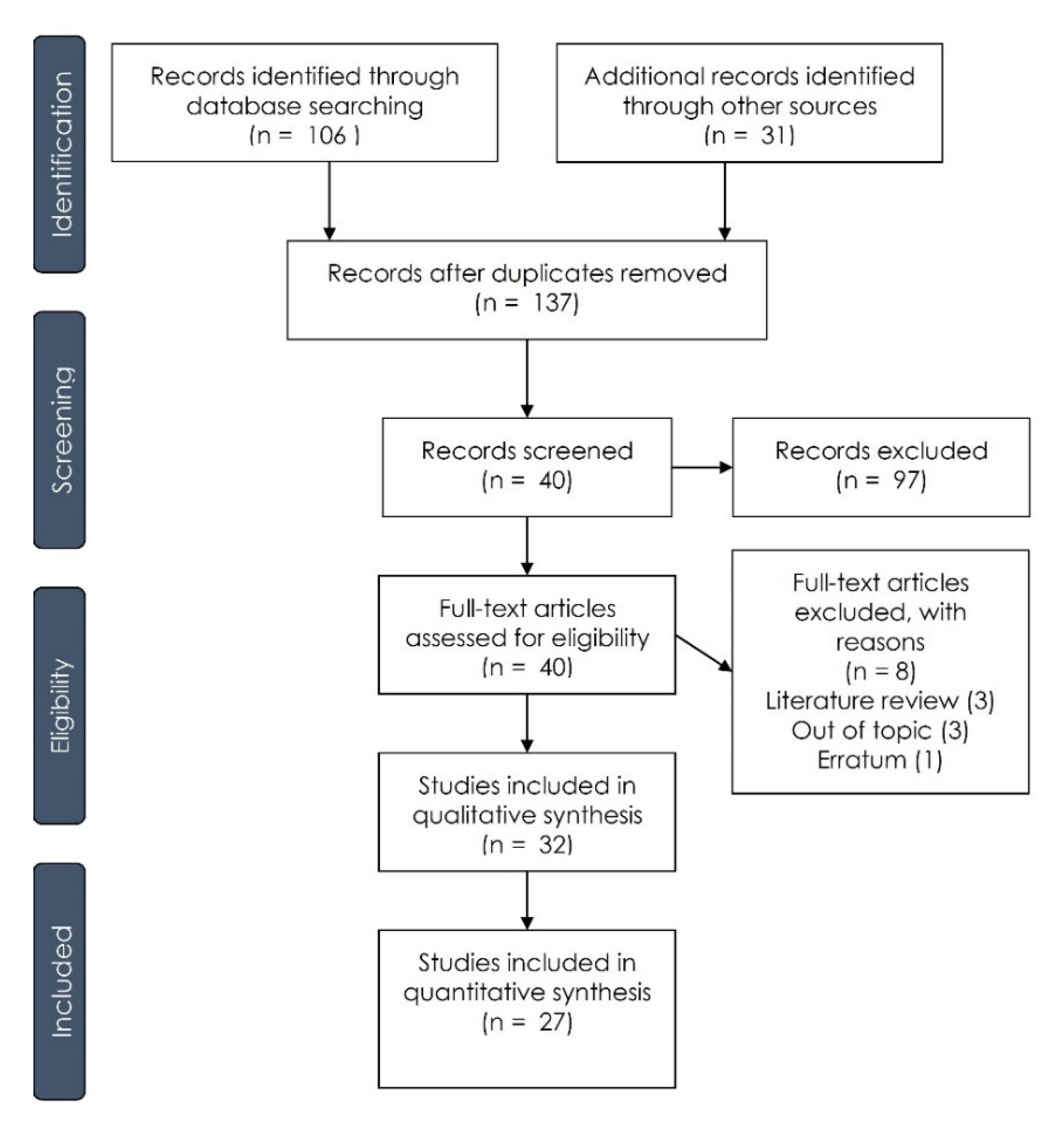
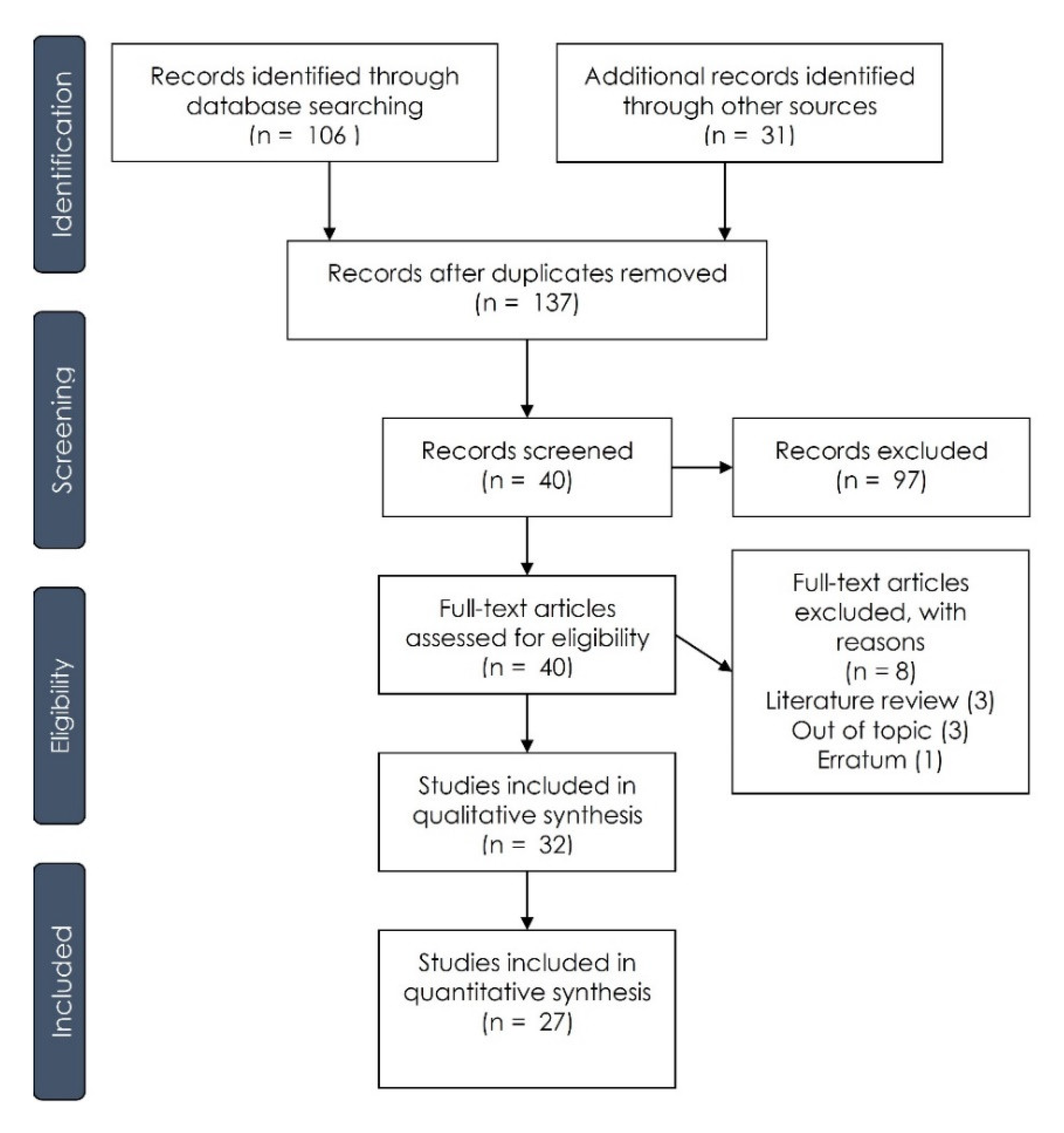
3.1. Paper Selection Process
3.2. General Property of the Studies Included
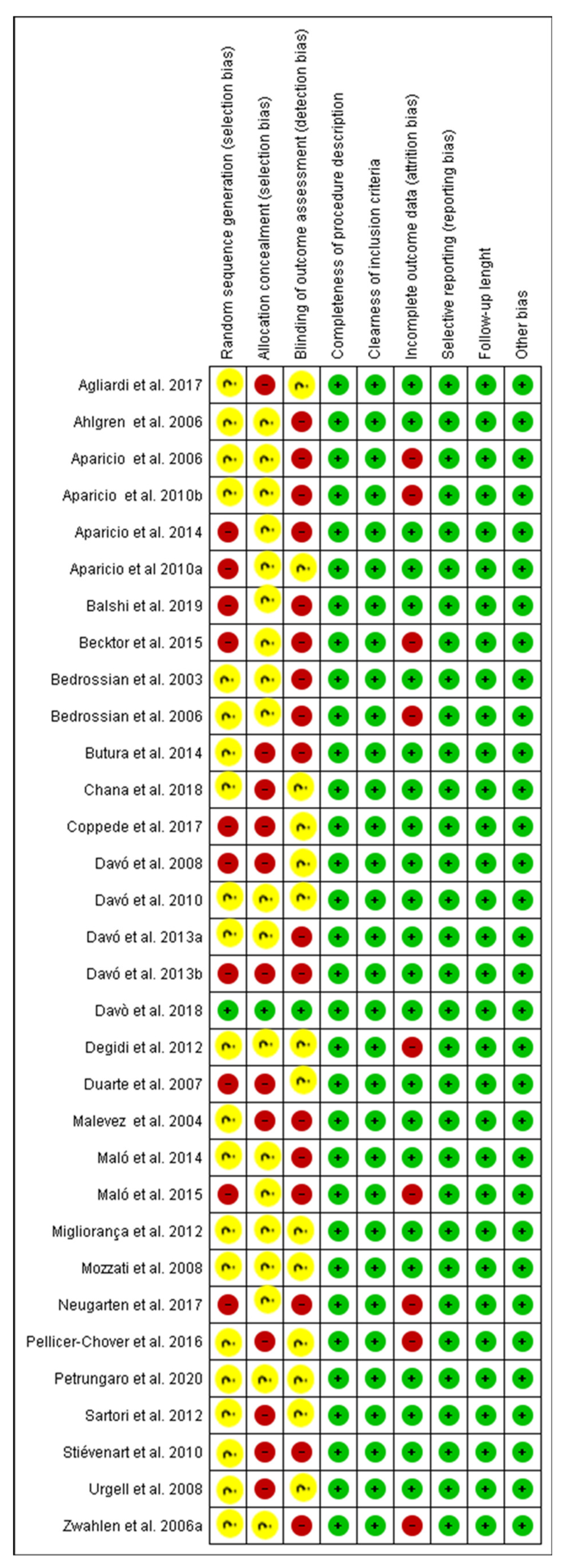
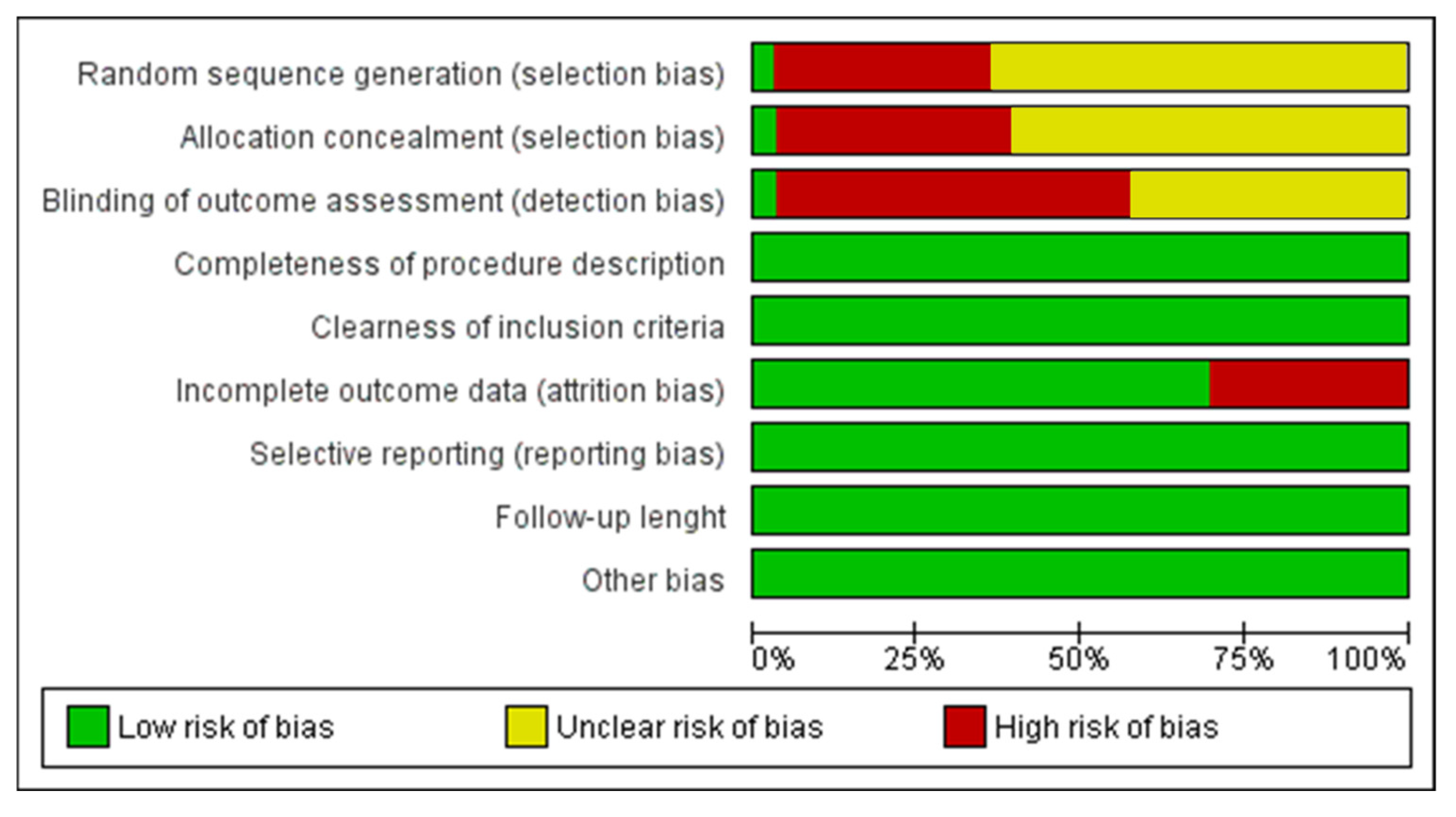
3.3. Study Characteristics and Risk of Bias Assessment
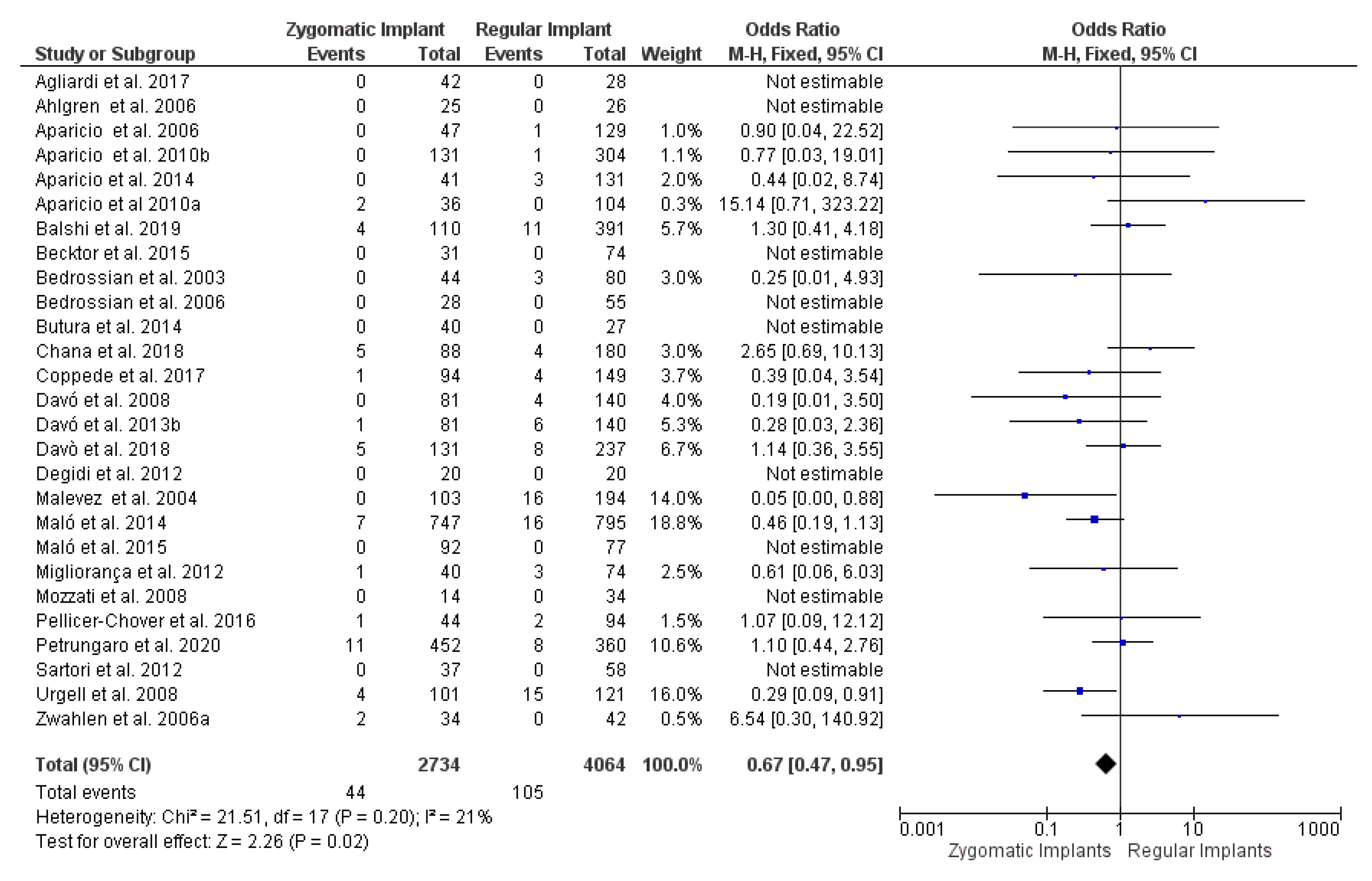
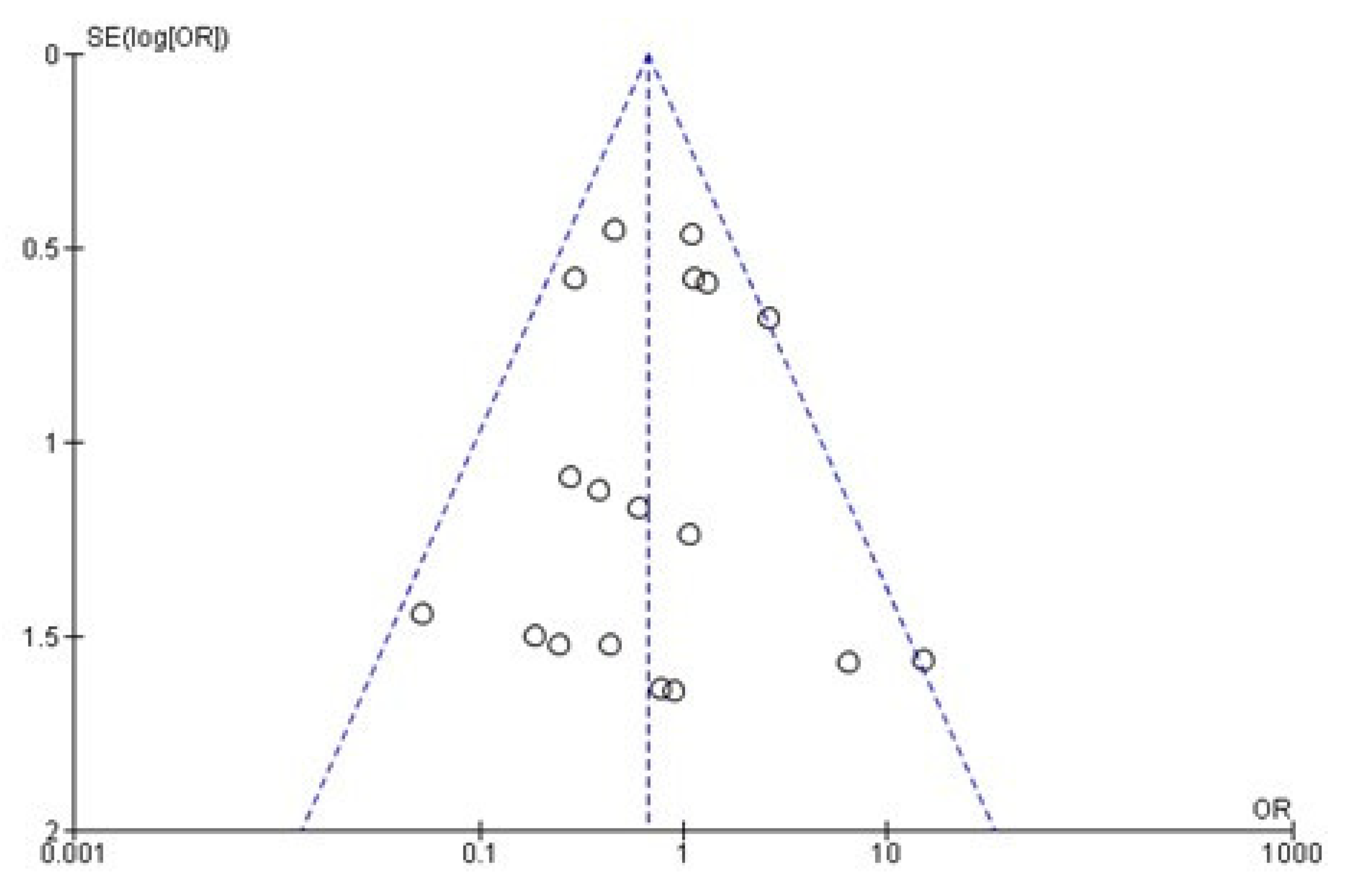
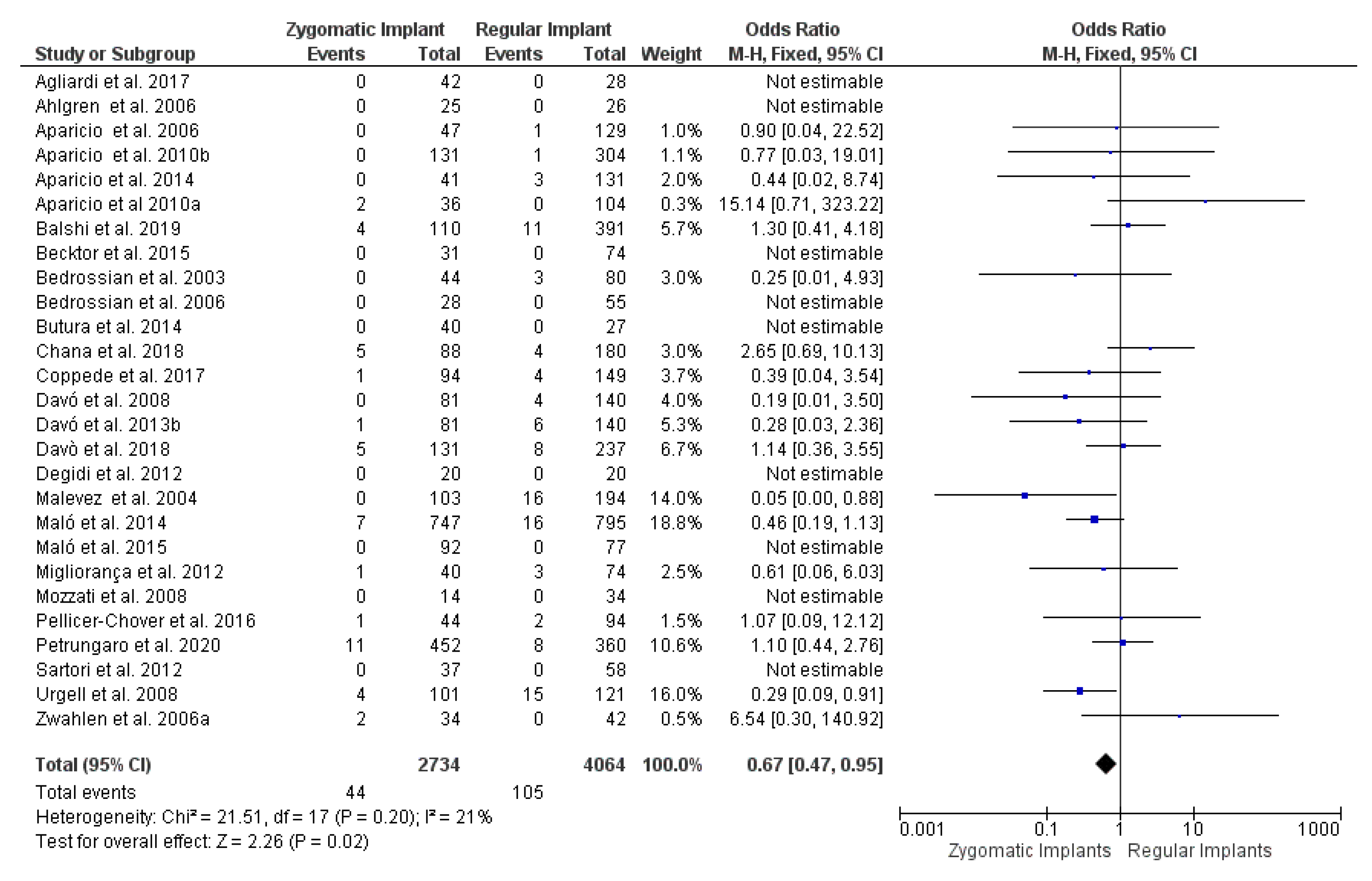
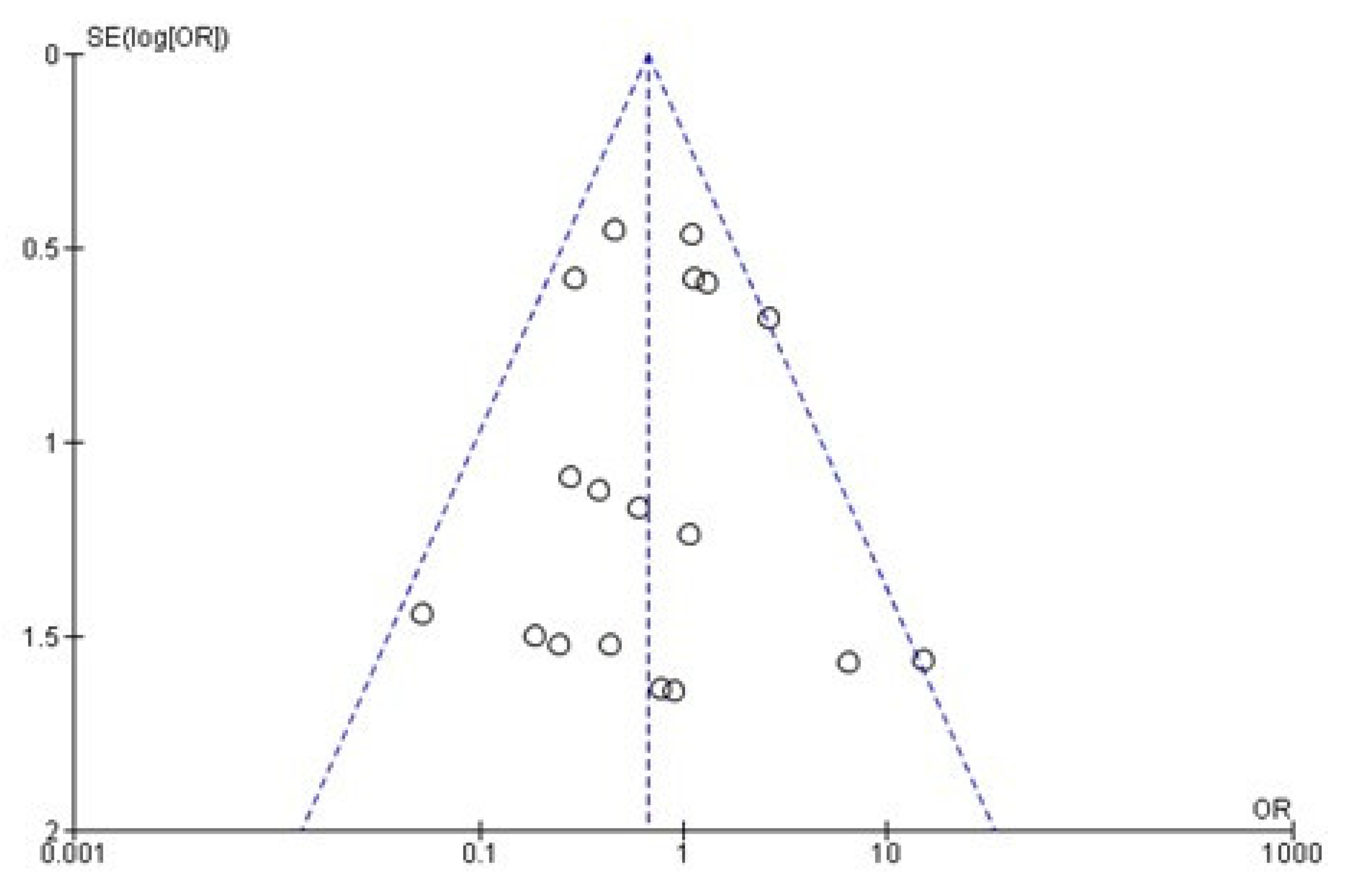
3.4. Meta-Analysis Evaluation
4. Discussion
Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wagner, F.; Dvorak, G.; Nemec, S.; Pietschmann, P.; Figl, M.; Seemann, R. A principal components analysis: How pneumatization and edentulism contribute to maxillary atrophy. Oral Dis. 2016, 23, 55–61. [Google Scholar] [CrossRef] [Green Version]
- Cawood, J.; Howell, R. A classification of the edentulous jaws. Int. J. Oral Maxillofac. Surg. 1988, 17, 232–236. [Google Scholar] [CrossRef]
- Unger, J.W.; Ellinger, C.W.; Gunsolley, J.C. An analysis of the effect of mandibular length on residual ridge loss in the edentulous patient. J. Prosthet. Dent. 1992, 67, 827–830. [Google Scholar] [CrossRef]
- Al-Thobity, A.; Wolfinger, G.; Balshi, S.; Flinton, R.; Balshi, T. Zygomatic implants as a rehabilitation approach for a severely deficient maxilla. Int. J. Oral Maxillofac. Implant. 2014, 29, 283–289. [Google Scholar] [CrossRef] [Green Version]
- Hernández-Alfaro, F.; Ragucci, G.M.M.; Méndez-Manjón, I.; Giralt-Hernando, M.; Guijarro-Martínez, R.; Sicilia-Blanco, P.; Ventura-Martínez, N.; Valls-Ontañón, A. Rehabilitation of the severely atrophic maxilla using LeFort I maxillary advancement and simultaneous zygoma implant placement: Proof of concept. Int. J. Oral Implantol. 2019, 12, 359–372. [Google Scholar]
- Comuzzi, L.; Tumedei, M.; Piattelli, A.; Iezzi, G. Short vs. standard length cone morse connection implants: An in vitro pilot study in low density polyurethane foam. Symmetry 2019, 11, 1349. [Google Scholar] [CrossRef] [Green Version]
- Comuzzi, L.; Tumedei, M.; Pontes, A.E.; Piattelli, A.; Iezzi, G. Primary stability of dental implants in low-density (10 and 20 pcf) polyurethane foam blocks: Conical vs cylindrical implants. Int. J. Environ. Res. Public Health 2020, 17, 2617. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tumedei, M.; Piattelli, A.; Degidi, M.; Mangano, C.; Iezzi, G. A Narrative review of the histological and histomorphometrical evaluation of the peri-implant bone in loaded and unloaded dental implants. a 30-year experience (1988–2018). Int. J. Environ. Res. Public Health 2020, 17, 2088. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanali, S.; Tumedei, M.; Pignatelli, P.; Inchingolo, F.; Pennacchietti, P.; Pace, G.; Piattelli, A. Implant primary stability with an osteocondensation drilling protocol in different density polyurethane blocks. Comput. Methods Biomech. Biomed. Eng. 2020, 1–7. [Google Scholar] [CrossRef]
- Fujiwara, S.; Kato, S.; Bengazi, F.; Velez, J.U.; Tumedei, M.; Kotsu, M.; Botticelli, D. Healing at implants installed in osteotomies prepared either with a piezoelectric device or drills: An experimental study in dogs. Oral Maxillofac. Surg. 2021, 25, 65–73. [Google Scholar] [CrossRef]
- Kotsu, M.; Urbizo Velez, J.; Bengazi, F.; Tumedei, M.; Fujiwara, S.; Kato, S.; Botticelli, D. Healing at implants installed from ~70- to <10-Ncm insertion torques: An experimental study in dogs. Oral Maxillofac. Surg. 2021, 25, 55–64. [Google Scholar] [CrossRef]
- De Moraes, P.; Olate, S.; Nóbilo, M.D.A.; Asprino, L.; De Moraes, M.; Barbosa, J.D.A. Maxillary “All-On-Four” treatment using zygomatic implants. A mechanical analysis. Rev. Stomatol. Chir. Maxillofac. Chir. Orale 2016, 117, 67–71. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, E.J.; Kuabara, M.R.; Gulinelli, J.L. “All-on-four” concept and immediate loading for simultaneous rehabilitation of the atrophic maxilla and mandible with conventional and zygomatic implants. Br. J. Oral Maxillofac. Surg. 2010, 48, 218–220. [Google Scholar] [CrossRef]
- Jensen, O.T.; Adams, M.W.; Butura, C.; Galindo, D.F. Maxillary V-4: Four implant treatment for maxillary atrophy with dental implants fixed apically at the vomer-nasal crest, lateral pyriform rim, and zygoma for immediate function. Report on 44 patients followed from 1 to 3 years. J. Prosthet. Dent. 2015, 114, 810–817. [Google Scholar] [CrossRef] [PubMed]
- Malo, P.; de Araújo Nobre, M.; Lopes, A.; Moss, S.M.; Molina, G.J. A longitudinal study of the survival of All-on-4 implants in the mandible with up to 10 years of follow-up. J. Am. Dent. Assoc. 2011, 142, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Bavetta, G.; Bavetta, G.; Randazzo, V.; Cavataio, A.; Paderni, C.; Grassia, V.; Dipalma, G.; Isacco, C.G.; Scarano, A.; De Vito, D.; et al. A retrospective study on insertion torque and Implant Stability Quotient (ISQ) as stability parameters for immediate loading of implants in fresh extraction sockets. BioMed. Res. Int. 2019, 2019, 9720419. [Google Scholar] [CrossRef] [Green Version]
- Balan, I.; Di Girolamo, M.; Lauritano, D.; Carinci, F. Treatment of severe atrophic maxilla with zygomatic implants: A case series. Oral Implantol. 2017, 10, 317–324. [Google Scholar] [CrossRef]
- Scarano, A.; Conte, R.; Murmura, G.; Lorusso, F.; Harrath, A.H. Satisfaction grade assessment of patients treated with zygomatic implants with self-tapping apex and machined body. J. Biol. Regul. Homeost. Agents 2019, 33, 1651–1656. [Google Scholar]
- Scarano, A.; Lorusso, F.; Arcangelo, M.; D’Arcangelo, C.; Celletti, R.; De Oliveira, P.S. Lateral sinus floor elevation performed with trapezoidal and modified triangular flap designs: A randomized pilot study of post-operative pain using thermal infrared imaging. Int. J. Environ. Res. Public Health 2018, 15, 1277. [Google Scholar] [CrossRef] [Green Version]
- Scarano, A.; Murmura, G.; Mastrangelo, F.; Lorusso, F.; Greco Lucchina, A.; Carinci, F. A novel technique to prevent sinus membrane collapse during maxillary sinus floor augmentation without bone graft: Technical note. J. Biol. Regul. Homeost. Agents 2018, 32, 1589–1592. [Google Scholar]
- Ito, Z.; Matsuyama, Y.; Sakai, Y.; Imagama, S.; Wakao, N.; Ando, K.; Hirano, K.; Tauchi, R.; Muramoto, A.; Matsui, H.; et al. Bone union rate with autologous iliac bone versus local bone graft in posterior lumbar interbody fusion. Spine 2010, 35, E1101–E1105. [Google Scholar] [CrossRef]
- De Carvalho, F.A.; Ponzoni, D.; Vedovatto, E.; de Carvalho, P.S.P. Remodeling of calvarial graft in increased atrophic maxillary thickness. A prospective clinical study. Clin. Implant Dent. Relat. Res. 2020, 22, 84–90. [Google Scholar] [CrossRef]
- Aghaloo, T.L.; Tencati, E.; Hadaya, D. Biomimetic enhancement of bone graft reconstruction. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 193–205. [Google Scholar] [CrossRef] [PubMed]
- Bertolai, R.; Aversa, A.; Catelani, C.; Rossi, A.; Giannini, D. Treatment of extreme maxillary atrophy with Zygoma implants. Minerva Stomatol. 2015, 64, 253–264. [Google Scholar] [PubMed]
- Karlan, M.S.; Cassisi, N.J. Fractures of the zygoma: A geometric, biomechanical, and surgical analysis. Arch. Otolaryngol. Head Neck Surg. 1979, 105, 320–327. [Google Scholar] [CrossRef] [PubMed]
- Uchida, Y.; Goto, M.; Katsuki, T.; Akiyoshi, T. Measurement of the maxilla and zygoma as an aid in installing zygomatic implants. J. Oral Maxillofac. Surg. 2001, 59, 1193–1198. [Google Scholar] [CrossRef] [Green Version]
- Nkenke, E.; Hahn, M.; Lell, M.; Wiltfang, J.; Schultze-Mosgau, S.; Stech, B.; Radespiel-Tröger, M.; Neukam, F.W. Anatomic site evaluation of the zygomatic bone for dental implant placement: Zygomatic bone for dental implants. Clin. Oral Implant. Res. 2003, 14, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Romeed, S.A.; Malik, R.; Dunne, S.M. Zygomatic implants: The impact of zygoma bone support on biomechanics. J. Oral Implant. 2014, 40, 231–237. [Google Scholar] [CrossRef]
- Davó, R.; David, L. Quad zygoma: Technique and realities. Oral Maxillofac. Surg. Clin. N. Am. 2019, 31, 285–297. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Abreu, M.H.N.G. Survival and complications of zygomatic implants: A systematic review. Oral Maxillofac. Surg. 2012, 17, 81–93. [Google Scholar] [CrossRef]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Survival and complications of zygomatic implants: An updated systematic review. J. Oral Maxillofac. Surg. 2016, 74, 1949–1964. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Agliardi, E.; Romeo, D.; Panigatti, S.; de Araújo Nobre, M.; Maló, P. Immediate full-arch rehabilitation of the severely atrophic maxilla supported by zygomatic implants: A prospective clinical study with minimum follow-up of 6 years. Int. J. Oral Maxillofac. Surg. 2017, 46, 1592–1599. [Google Scholar] [CrossRef]
- Ahlgren, F.; Størksen, K.; Tornes, K. A study of 25 zygomatic dental implants with 11 to 49 months’ follow-up after loading. Int. J. Oral Maxillofac. Implant. 2006, 21, 421–425. [Google Scholar]
- Aparicio, C.; Ouazzani, W.; Aparicio, A.; Fortes, V.; Muela, R.; Pascual, A.; Codesal, M.; Barluenga, N.; Franch, M. Immediate/early loading of zygomatic implants: Clinical experiences after 2 to 5 years of follow-up. Clin. Implant Dent. Relat. Res. 2010, 12 (Suppl. 1), e77–e82. [Google Scholar] [CrossRef]
- Aparicio, C.; Ouazzani, W.; Aparicio, A.; Fortes, V.; Muela, R.; Pascual, A.; Codesal, M.; Barluenga, N.; Manresa, C.; Franch, M. Extrasinus zygomatic implants: Three year experience from a new surgical approach for patients with pronounced buccal concavities in the edentulous maxilla. Clin. Implant Dent. Relat. Res. 2010, 12, 55–61. [Google Scholar] [CrossRef]
- Aparicio, C.; Ouazzani, W.; Garcia, R.; Arevalo, X.; Muela, R.; Fortes, V. A prospective clinical study on titanium implants in the zygomatic arch for prosthetic rehabilitation of the atrophic edentulous maxilla with a follow-up of 6 months to 5 years. Clin. Implant Dent. Relat. Res. 2006, 8, 114–122. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Manresa, C.; Francisco, K.; Ouazzani, W.; Claros, P.; Potau, J.M.; Aparicio, A. The long-term use of zygomatic implants: A 10-year clinical and radiographic report. Clin. Implant Dent. Relat. Res. 2014, 16, 447–459. [Google Scholar] [CrossRef] [PubMed]
- Balshi, S.F.; Wolfinger, G.J.; Balshi, T.J. A retrospective analysis of 110 zygomatic implants in a single-stage immediate loading protocol. Int. J. Oral Maxillofac. Implant. 2009, 24, 335–341. [Google Scholar]
- Becktor, J.P.; Isaksson, S.; Abrahamsson, P.; Sennerby, L. Evaluation of 31 zygomatic implants and 74 regular dental implants used in 16 patients for prosthetic reconstruction of the atrophic maxilla with cross-arch fixed bridges. Clin. Implant Dent. Relat. Res. 2005, 7, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Bedrossian, E.; Stumpel, L.; Beckely, M.L.; Indresano, T.; Indersano, T. The zygomatic implant: Preliminary data on treatment of severely resorbed maxillae. A clinical report. Int. J. Oral Maxillofac. Implant. 2002, 17, 861–865. [Google Scholar]
- Bedrossian, E.; Rangert, B.; Stumpel, L.; Indresano, T. Immediate function with the zygomatic implant: A graftless solution for the patient with mild to advanced atrophy of the maxilla. Int. J. Oral Maxillofac. Implant. 2006, 21, 937–942. [Google Scholar]
- Butura, C.C.; Galindo, D.F. Combined immediate loading of zygomatic and mandibular implants: A preliminary 2-year report of 19 patients. Int. J. Oral Maxillofac. Implant. 2014, 29, e22–e29. [Google Scholar] [CrossRef] [Green Version]
- Chana, H.; Smith, G.; Bansal, H.; Zahra, D. A retrospective cohort study of the survival rate of 88 zygomatic implants placed over an 18-year period. Int. J. Oral Maxillofac. Implant. 2019, 34, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Coppedê, A.; De Mayo, T.; de Sá Zamperlini, M.; Amorin, R.; De Pádua, A.P.A.T.; Shibli, J.A. Three-year clinical prospective follow-up of extrasinus zygomatic implants for the rehabilitation of the atrophic maxilla. Clin. Implant Dent. Relat. Res. 2017, 19, 926–934. [Google Scholar] [CrossRef] [PubMed]
- Davó, R.; Felice, P.; Pistilli, R.; Barausse, C.; Marti-Pages, C.; Ferrer-Fuertes, A.; Ippolito, D.R.; Esposito, M. Immediately loaded zygomatic implants vs conventional dental implants in augmented atrophic maxillae: 1-year post-loading results from a multicentre randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 145–161. [Google Scholar] [PubMed]
- Davó, R.; Malevez, C.; Pons, O. Immediately loaded zygomatic implants: A 5-year prospective study. Eur. J. Oral Implantol. 2013, 6, 39–47. [Google Scholar]
- Davó, R.; Pons, O. Prostheses supported by four immediately loaded zygomatic implants: A 3-year prospective study. Eur. J. Oral Implantol. 2013, 6, 263–269. [Google Scholar]
- Davo, R.; Pons, O.; Rojas, J.; Carpio, E. Immediate function of four zygomatic implants: A 1-year report of a prospective study. Eur. J. Oral Implantol. 2010, 3, 323–334. [Google Scholar]
- Davó, R.; Malevez, C.; Rojas, J.; Rodríguez, J.; Regolf, J. Clinical outcome of 42 patients treated with 81 immediately loaded zygomatic implants: A 12- to 42-month retrospective study. Eur. J. Oral Implantol. 2008, 1, 141–150. [Google Scholar]
- Degidi, M.; Nardi, D.; Piattelli, A.; Malevez, C. Immediate loading of zygomatic implants using the intraoral welding technique: A 12-month case series. Int. J. Periodontics Restor. Dent. 2012, 32, 154–161. [Google Scholar]
- Duarte, L.R.; Filho, H.N.; Francischone, C.E.; Peredo, L.G.; Brånemark, P.-I. The establishment of a protocol for the total rehabilitation of atrophic maxillae employing four zygomatic fixtures in an immediate loading system—A 30-month clinical and radiographic follow-Up. Clin. Implant Dent. Relat. Res. 2007, 9, 186–196. [Google Scholar] [CrossRef]
- Malevez, C.; Abarca, M.M.; Durdu, F.F.; Daelemans, P. Clinical outcome of 103 consecutive zygomatic implants: A 6–48 months follow-up study. Clin. Oral Implant. Res. 2004, 15, 18–22. [Google Scholar] [CrossRef]
- Maló, P.; Nobre, M.D.A.; Lopes, A.; Ferro, A.; Moss, S. Five-year outcome of a retrospective cohort study on the rehabilitation of completely edentulous atrophic maxillae with immediately loaded zygomatic implants placed extra-maxillary. Eur. J. Oral Implantol. 2014, 7, 267–281. [Google Scholar] [PubMed]
- Maló, P.; de Araújo Nobre, M.; Lopes, A.; Ferro, A.; Moss, S. Extramaxillary surgical technique: Clinical outcome of 352 patients rehabilitated with 747 zygomatic implants with a follow-up between 6 months and 7 years. Clin. Implant Dent. Relat. Res. 2015, 17 (Suppl. 1), e153–e162. [Google Scholar] [CrossRef] [PubMed]
- Migliorança, R.M.; Sotto-Maior, B.S.; Senna, P.M.; Francischone, C.E.; Del Bel Cury, A.A. Immediate occlusal loading of extrasinus zygomatic implants: A prospective cohort study with a follow-up period of 8 years. Int. J. Oral Maxillofac. Surg. 2012, 41, 1072–1076. [Google Scholar] [CrossRef] [PubMed]
- Mozzati, M.; Monfrin, S.B.; Pedretti, G.; Schierano, G.; Bassi, F. Immediate loading of maxillary fixed prostheses retained by zygomatic and conventional implants: 24-month preliminary data for a series of clinical case reports. Int. J. Oral Maxillofac. Implant. 2008, 23, 308–314. [Google Scholar]
- Neugarten, J.; Tuminelli, F.; Walter, L. Two bilateral zygomatic implants placed and immediately loaded: A retrospective chart review with up-to-54-month follow-up. Int. J. Oral Maxillofac. Implant. 2017, 32, 1399–1403. [Google Scholar] [CrossRef] [Green Version]
- Pellicer-Chover, H.; Cervera-Ballester, J.; Penarrocha-Oltra, D.; Bagan, L.; Penarrocha-Diago, M. Influence of the prosthetic arm length (palatal position) of zygomatic implants upon patient satisfaction. Med. Oral Patol. Oral Cir. Bucal 2016, 21, e380–e384. [Google Scholar] [CrossRef]
- Petrungaro, P.S.; Gonzales, S.; Villegas, C.; Yousef, J.; Arango, A. A Retrospective study of a multi-center case series of 452 zygomatic implants placed over 5 years for treatment of severe maxillary atrophy. Compend. Contin. Educ. Dent. 2020, 41, 232–241. [Google Scholar]
- Sartori, E.M.; Padovan, L.E.M.; de Mattias Sartori, I.A.; Ribeiro, P.D.; Carvalho, A.C.G.D.S.; Goiato, M.C. Evaluation of satisfaction of patients rehabilitated with zygomatic fixtures. J. Oral Maxillofac. Surg. 2012, 70, 314–319. [Google Scholar] [CrossRef] [PubMed]
- Stiévenart, M.; Malevez, C. Rehabilitation of totally atrophied maxilla by means of four zygomatic implants and fixed prosthesis: A 6–40-month follow-up. Int. J. Oral Maxillofac. Surg. 2010, 39, 358–363. [Google Scholar] [CrossRef]
- Urgell, J.P.; Gutiérrez, V.R.; Escoda, C.G.G. Rehabilitation of atrophic maxilla: A review of 101 zygomatic implants. Med. Oral Patol. Oral Cir. Bucal 2008, 13, 363–370. [Google Scholar]
- Zwahlen, R.A.; Grätz, K.W.; Oechslin, C.K.; Studer, S.P. Survival rate of zygomatic implants in atrophic or partially resected maxillae prior to functional loading: A retrospective clinical report. Int. J. Oral Maxillofac. Implant. 2006, 21, 413–420. [Google Scholar]
- Gehrke, S.A.; Mazón, P.; Del Fabbro, M.; Tumedei, M.; Aramburú Júnior, J.; Pérez-Díaz, L.; De Aza, P.N. Histological and Histomorphometric Analyses of Two Bovine Bone Blocks Implanted in Rabbit Calvaria. Symmetry 2019, 11, 641. [Google Scholar] [CrossRef] [Green Version]
- Javed, F.; Romanos, G.E. The role of primary stability for successful immediate loading of dental implants. A literature review. J. Dent. 2010, 38, 612–620. [Google Scholar] [CrossRef] [PubMed]
- Scarano, A.; De Oliveira, P.S.; Traini, T.; Lorusso, F. Sinus Membrane Elevation with Heterologous Cortical Lamina: A Randomized Study of a New Surgical Technique for Maxillary Sinus Floor Augmentation without Bone Graft. Materials 2018, 11, 1457. [Google Scholar] [CrossRef] [Green Version]
- Scarano, A.; Inchingolo, F.; Murmura, G.; Traini, T.; Piattelli, A.; Lorusso, F. Three-Dimensional Architecture and Mechanical Properties of Bovine Bone Mixed with Autologous Platelet Liquid, Blood, or Physiological Water: An In Vitro Study. Int. J. Mol. Sci. 2018, 19, 1230. [Google Scholar] [CrossRef] [Green Version]
- Veltri, M.; González-Martín, O.; Belser, U.C. Influence of simulated bone-implant contact and implant diameter on secondary stability: A resonance frequency in vitro study. Clin. Oral Implant. Res. 2014, 25, 899–904. [Google Scholar] [CrossRef]
- Hsu, J.-T.; Shen, Y.-W.; Kuo, C.-W.; Wang, R.-T.; Fuh, L.-J.; Huang, H.-L. Impacts of 3D bone-to- implant contact and implant diameter on primary stability of dental implant. J. Formos. Med. Assoc. 2017, 116, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Chappuis, V.; Rahman, L.; Buser, R.; Janner, S.; Belser, U.; Buser, D. Effectiveness of contour augmentation with guided bone regeneration: 10-year results. J. Dent. Res. 2017, 97, 266–274. [Google Scholar] [CrossRef]
- González-Martín, O.; Lee, E.; Weisgold, A.; Veltri, M.; Su, H. Contour management of implant restorations for optimal emergence profiles: Guidelines for immediate and delayed provisional restorations. Int. J. Periodontics Restor. Dent. 2020, 40, 61–70. [Google Scholar] [CrossRef]
- Jensen, O.T.; Adams, M.W.; Smith, E. Paranasal bone: The prime factor affecting the decision to use transsinus vs zygomatic implants for biomechanical support for immediate function in maxillary dental implant reconstruction. Int. J. Oral Maxillofac. Implant. 2014, 29, e130–e138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gümrükçü, Z. Biomechanical evaluation of zygomatic implant use in patients with different buccal maxillary defect levels. Int. J. Oral Maxillofac. Implant. 2019, 34, e115–e122. [Google Scholar] [CrossRef]
- Al-Nawas, B.; Wegener, J.; Bender, C.; Wagner, W. Critical soft tissue parameters of the zygomatic implant. J. Clin. Periodontol. 2004, 31, 497–500. [Google Scholar] [CrossRef]
- Peñarrocha-Diago, M.; Bernabeu-Mira, J.C.; Fernández-Ruíz, A.; Aparicio, C.; Peñarrocha-Oltra, D. Bone regeneration and soft tissue enhancement around zygomatic implants: Retrospective case series. Materials 2020, 13, 1577. [Google Scholar] [CrossRef] [Green Version]
- Brånemark, P.; Gröndahl, K.; Öhrnell, L.; Nilsson, P.; Petruson, B.; Svensson, B.; Engstrand, P.; Nannmark, U. Zygoma fixture in the management of advanced atrophy of the maxilla: Technique and long-term results. Scand. J. Plast. Reconstr. Surg. Hand Surg. 2004, 38, 70–85. [Google Scholar] [CrossRef]
- Albrektsson, T.; Wennerberg, A. On osseointegration in relation to implant surfaces. Clin. Implant Dent. Relat. Res. 2019, 21 (Suppl. 1), 4–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarano, A.; Piattelli, A.; Quaranta, A.; Lorusso, F. Bone response to two dental implants with different sandblasted/acid-etched implant surfaces: A histological and histomorphometrical study in rabbits. BioMed Res. Int. 2017, 2017, 8724951. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Population\Patients | Intervention | Comparison | Outcomes |
|---|---|---|---|
| Patient group of interest? | What is the main intervention you wish to consider? | Is there an alternative intervention to compare? | What is the clinical outcome? |
| Subjects that need oral rehabilitation with zygomatic implant surgery in maxillary severe atrophies. | Zygomatic implant positioning for fixed maxillary rehabilitation. | Zygomatic implant vs. regular maxillary implant survival rate. | Can zygomatic implants provide a valuable survival rate for fixed rehabilitation in maxillary severe atrophies? |
| Search Strategies | |
|---|---|
| Keywords: | Advanced keyword search: (zygomatic dental implant AND oral rehabilitation) AND (retrospective study OR prospective study OR controlled study) |
| Databases | PubMed/Medline, EMBASE |
| Authors | Year | Journal | Zygomatic Implant Configuration | Prosthesis | Follow up | Zygomatic-Regular Implant Survival Rate | Complications | Zygomatic Implant Failure |
|---|---|---|---|---|---|---|---|---|
| Agliardi et al. | 2017 | Int J Oral Maxillofac Surg | Double (9) Quad (6) | Full-arch (15)-Partial (0) | 79 m to 97 m | 100%-/ | - | - |
| Ahlgren et al. | 2006 | Int J Oral Maxillofac Implants | Double (13) | Full-arch (13)-Partial (0) | 11–49 m | 100–100% | - | - |
| Aparicio et al. | 2010 | Clin Implant Dent Relat Res | Single (4) Double (17) | Full-arch (20)-Partial (0) | 36–48 m | 100–100% | - | - |
| Aparicio et al. | 2006 | Clin Implant Dent Relat Res | Single (7) Double (62) | Full-arch (69)-Partial (0) | 60 m | 100–99% | Sinusitis | - |
| Aparicio et al. | 2010 | Clin Implant Dent Relat Res | - | Full-arch (23)-Partial (2) | 24 m to 60 m | 100–99.2% | Regular implant failure (1), Abutment screw fracture (5) | 1 implant |
| Aparicio et al. | 2014 | Clin Implant Dent Relat Res | Single (3) Double (41) | Full-arch (22)-Partial (0) | 120 m | 95.12–97.71% | 2 implants | |
| Balshi et al. | 2009 | Int J Oral Maxillofac Implants | - | Full-arch (56)-Partial (0) | 9–70 m | 96.37–97.2% | Osseointegration failure | 4 implants |
| Becktor et al. | 2005 | Clin Implant Dent Relat Res | Single (1) Double (15) | Full-arch (16)-Partial (0) | 9–69 m | 100% | Sinusitis | - |
| Bedrossian et al. | 2006 | Int J Oral Maxillofac Implants | Double (14) | Full-arch (14)-Partial (0) | 6 m | 100–100% | - | - |
| Bedrossian et al. | 2003 | Int J Oral Maxillofac Implants | Double (22) | Full-arch (22)-Partial (0) | 34 m | 100–91.25% | - | - |
| Butura et al. | 2014 | Int J Oral Maxillofac Implants | Single (1) Double (12), Triple (1), Quad (1) | Full-arch (15)-Partial (0) | 24 m | 100–100% | - | - |
| Chana et al. | 2018 | Int J Oral Maxillofac Implants | - | - | 216 m | 94.32% | Sinusitis, implant mobility, pain | 5 implants |
| Coppede et al. | 2017 | Clin Implant Dent Relat Res | Single (6) Double (27), Triple (3), Quad (6) | Full-arch (42)-Partial (0) | 36 m | 98.9–97.7% | Osseointegration failure | 1 implant |
| Davò et al. | 2018 | Eur J Oral Implantol | Double (6) Quad (29) | Full-arch (35)-Partial (0) | 12 m | 96.1–91.6% | Sinus membrane perforation (4), major swelling (1), sinusitis (4), implant mucositis (2), Peri-orbital infection and swelling (2) | 5 implants/3 patients |
| Davó et al. | 2013 | Eur J Oral Implantol | - | Full-arch (37)-Partial (5) | 60 m | 98.5–94.9% | Osseointegration failure, peri-implant mucositis | 1 implant |
| Davó et al. | 2010 | Eur J Oral Implantol | Quad (17) | Full-arch (17)-Partial (0) | 12 m | 100–100% | Eye orbit drill penetration, fistula | - |
| Davó et al. | 2008 | Eur J Oral Implantol | Single (5) Double (35) Quad (2) | Full-arch (37)-Partial (5) | 12-42 m | 100–97% | Implant mobility | - |
| Davó et al. | 2013 | Eur J Oral Implantol | Quad (17) | Full-arch (17)-Partial (0) | 36 months | 100%-/ | Eye orbit drill penetration, fistula, sinusitis, fistula | - |
| Degidi et al. | 2012 | Int J Periodontics Restorative Dent | Double (10) | Full-arch (10)-Partial (0) | 12 m | 100–100% | - | - |
| Duarte et al. | 2007 | Clin Implant Dent Relat Res | Quad (12) | Full-arch (12)-Partial (0) | 30 m | 97.91% | Osseointegration failure, sinusitis, implant mobility, pain | 1 implant |
| Malevez et al. | 2004 | Clin Oral Implants Res | Double (55) | Full-arch (55)-Partial (0) | 6-48 m | 100–91.75% | Sinusitis | - |
| Maló et al. | 2014 | Eur J Oral Implantol | Single (73) Double (214), Triple (14) Quad (51) | Full-arch (352)-Partial (0) | 6–84 m | 98.2–97-9 | Sinusitis, implant mobility | 14 implants |
| Maló et al. | 2015 | Clin Implant Dent Relat Res | Single (8) Double (18) Triple (5) Quad (8) | Full-arch (39)-Partial (0) | 36 m | 100–100% | Sinusitis, implant mobility, fistula | - |
| Migliorança et al. | 2012 | Int J Oral Maxillofac Surg | Full-arch (21)-Partial (0) | 96 m | 97.50% | Implant mobility | 1 implant | |
| Mozzati et al. | 2008 | Int J Oral Maxillofac Implants | Double (7) | Full-arch (7)-Partial (0) | 24 m | 100–100% | - | - |
| Neugarten et al. | 2017 | Int J Oral Maxillofac Implants | Quad (28) | Full-arch (28)-Partial (0) | 54 m | 96%-/ | Osseointegration failure | 4 implants |
| Pellicer-Chover et al. | 2016 | Med Oral Patol Oral Cir Bucal | Double (22) | Full-arch (22)-Partial (0) | 12 m | 97.7–97.8% | - | - |
| Petrungaro et al. | 2020 | Compend Contin Educ Dent | Single (134) Double (79) Quad (40) | Full-arch (234)-Partial (15) | 60 m | 97.6–97.7% | - | 11 implants |
| Sartori et al. | 2012 | J Oral Maxillofac Surg | Double (16) Quad (3) | Full-arch (16)-Partial (0) | 48 m | 100–100% | ||
| Stiévenart et al. | 2010 | Int J Oral Maxillofac Surg | Quad (20) | Full-arch (20)-Partial (0) | 6-40 m | 96% | Osseointegration failure, sinusitis, implant mobility, pain | 3 implants |
| Urgell et al. | 2008 | Med Oral Patol Oral Cir Bucal | Single (7) Double (47) | Full-arch (54)-Partial (0) | 48 months | 96.04–93.22% | Osseointegration failure, sinusitis, implant mobility, pain | 4 implants |
| Zwahlen et al. | 2006 | Int J Oral Maxillofac Implants | Single (2) Double (15) | Full-arch (18)-Partial (0) | 8 m | 94.1%-/ | Sinusitis, implant mobility, pain, fistula | 2 implants |
| Authors | Year | Journal | Study | Patients | Zygomatic Implants | Regular Implants | Delayed Loading Zygomatic Implants | Immediate Loading Zygomatic Implants |
|---|---|---|---|---|---|---|---|---|
| Agliardi et al. | 2017 | Int J Oral Maxillofac Surg | P | 15 | 42 | 18 | - | 47 |
| Ahlgren et al. | 2006 | Int J Oral Maxillofac Implants | R | 13 | 25 | 26 | 25 | - |
| Aparicio et al. | 2010 | Clin Implant Dent Relat Res | P | 20 | 36 | 104 | 36 | - |
| Aparicio et al. | 2006 | Clin Implant Dent Relat Res | P | 69 | 131 | 304 | 131 | - |
| Aparicio et al. | 2010 | Clin Implant Dent Relat Res | R | 25 | 47 | 129 | - | 47 |
| Aparicio et al. | 2014 | Clin Implant Dent Relat Res | R | 22 | 41 | 131 | 41 | - |
| Balshi et al. | 2009 | Int J Oral Maxillofac Implants | R | 56 | 110 | 391 | - | 110 |
| Becktor et al. | 2005 | Clin Implant Dent Relat Res | P | 16 | 31 | 74 | 31 | - |
| Bedrossian et al. | 2006 | Int J Oral Maxillofac Implants | P | 14 | 28 | 55 | - | 28 |
| Bedrossian et al. | 2003 | Int J Oral Maxillofac Implants | R | 22 | 44 | 80 | 44 | - |
| Butura et al. | 2014 | Int J Oral Maxillofac Implants | R | 15 | 40 | 27 | - | 40 |
| Chana et al. | 2018 | Int J Oral Maxillofac Implants | R | 45 | 88 | 180 | 88 | - |
| Coppede et al. | 2017 | Clin Implant Dent Relat Res | P | 42 | 94 | 179 | 16 | 78 |
| Davò et al. | 2018 | Eur J Oral Implantol | P | 35 | 131 | 237 | - | 131 |
| Davó et al. | 2013 | Eur J Oral Implantol | P | 42 | 81 | 140 | - | 81 |
| Davó et al. | 2010 | Eur J Oral Implantol | P | 17 | 68 | - | - | 68 |
| Davó et al. | 2008 | Eur J Oral Implantol | P | 42 | 81 | 140 | - | 81 |
| Davó et al. | 2013 | Eur J Oral Implantol | P | 17 | 68 | - | - | 68 |
| Degidi et al. | 2012 | Int J Periodontics Restorative Dent | P | 10 | 20 | 20 | - | 20 |
| Duarte et al. | 2007 | Clin Implant Dent Relat Res | P | 12 | 48 | - | - | 48 |
| Malevez et al. | 2004 | Clin Oral Implants Res | R | 55 | 103 | 194 | 103 | - |
| Maló et al. | 2014 | Eur J Oral Implantol | R | 352 | 747 | 795 | - | 747 |
| Maló et al. | 2015 | Clin Implant Dent Relat Res | R | 39 | 92 | 77 | - | 92 |
| Migliorança et al. | 2012 | Int J Oral Maxillofac Surg | P | 21 | 40 | 74 | - | 40 |
| Mozzati et al. | 2008 | Int J Oral Maxillofac Implants | P | 7 | 14 | 34 | - | 14 |
| Neugarten et al. | 2017 | Int J Oral Maxillofac Implants | R | 28 | 105 | - | - | 105 |
| Pellicer-Chover et al. | 2016 | Med Oral Patol Oral Cir Bucal | R | 22 | 44 | 94 | 44 | - |
| Petrungaro et al. | 2020 | Compend Contin Educ Dent | P | 249 | 452 | 360 | 249 | - |
| Sartori et al. | 2012 | J Oral Maxillofac Surg | R | 16 | 37 | 58 | 16 | - |
| Stiévenart et al. | 2010 | Int J Oral Maxillofac Surg | P | 20 | 80 | - | 40 | 40 |
| Urgell et al. | 2008 | Med Oral Patol Oral Cir Bucal | R | 54 | 101 | 221 | 101 | - |
| Zwahlen et al. | 2006 | Int J Oral Maxillofac Implants | R | 18 | 34 | 42 | - | 34 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lorusso, F.; Conte, R.; Inchingolo, F.; Festa, F.; Scarano, A. Survival Rate of Zygomatic Implants for Fixed Oral Maxillary Rehabilitations: A Systematic Review and Meta-Analysis Comparing Outcomes between Zygomatic and Regular Implants. Dent. J. 2021, 9, 38. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9040038
Lorusso F, Conte R, Inchingolo F, Festa F, Scarano A. Survival Rate of Zygomatic Implants for Fixed Oral Maxillary Rehabilitations: A Systematic Review and Meta-Analysis Comparing Outcomes between Zygomatic and Regular Implants. Dentistry Journal. 2021; 9(4):38. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9040038
Chicago/Turabian StyleLorusso, Felice, Roberto Conte, Francesco Inchingolo, Felice Festa, and Antonio Scarano. 2021. "Survival Rate of Zygomatic Implants for Fixed Oral Maxillary Rehabilitations: A Systematic Review and Meta-Analysis Comparing Outcomes between Zygomatic and Regular Implants" Dentistry Journal 9, no. 4: 38. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9040038