
The Impact of Sport Training on Oral Health in Athletes


Department of Medical, Oral and Biotechnological Sciences, University “G. D’Annunzio” of Chieti-Pescara, Via dei Vestini 31, 66100 Chieti, Italy
*
Author to whom correspondence should be addressed.
Dent. J. 2021, 9(5), 51; https://0-doi-org.brum.beds.ac.uk/10.3390/dj9050051
Submission received: 15 March 2021
/
Revised: 16 April 2021
/
Accepted: 28 April 2021
/
Published: 3 May 2021
(This article belongs to the Special Issue Sport and Dental Traumatology)
{kind=link}
{kind=link}
{kind=link}
Abstract
:Athletes’ oral health appears to be poor in numerous sport activities and different diseases can limit athletic skills, both during training and during competitions. Sport activities can be considered a risk factor, among athletes from different sports, for the onset of oral diseases, such as caries with an incidence between 15% and 70%, dental trauma 14–70%, dental erosion 36%, pericoronitis 5–39% and periodontal disease up to 15%. The numerous diseases are related to the variations that involve the ecological factors of the oral cavity such as salivary pH, flow rate, buffering capability, total bacterial count, cariogenic bacterial load and values of secretory Immunoglobulin A. The decrease in the production of S-IgA and the association with an important intraoral growth of pathogenic bacteria leads us to consider the training an “open window” for exposure to oral cavity diseases. Sports dentistry focuses attention on the prevention and treatment of oral pathologies and injuries. Oral health promotion strategies are needed in the sports environment. To prevent the onset of oral diseases, the sports dentist can recommend the use of a custom-made mouthguard, an oral device with a triple function that improves the health and performance of athletes. During training, the sports dentist must monitor the athletes and the sports examination protocol must be implemented with the inclusion of the clinical examination, quantitative and qualitative analysis of saliva and instructions on the use, cleansing and storage of the mouthguard.
1. Introduction
The growing diffusion of sports activities is focusing attention on the development of diseases correlated with the sporting performance, in addition to the health benefits.
The athlete should know the risks associated with carrying out sporting activities and direct more attention to the health status of his oral cavity since the alterations of the oral cavity contribute in a negative way to the health, well-being and physical performance of the athlete [1].
The main disorders of the oral cavity, correlated with the performance of various sports that have a significant impact on the quality of life of athletes, are represented by trauma, joint disorders, alterations and/or oral pathologies, such as caries, erosions, dental discolorations and periodontal disease. Moreover, the intense physical exercise at the start of competitions and throughout training time involves a reduction in salivary flow rate and in secretory IgA (S-IgA) load, resulting in a decrease in the host organism’s defenses and, therefore, an increase in susceptibility to particular pathologies, such as upper respiratory tract infections (URTI) and, specifically, pathologies of the oral cavity [2,3,4,5].
Therefore, during sport activities, the athletes must be monitored by sport dentists for changes affecting their oral cavity and the sports examination protocol must be implemented with the inclusion of clinical examination, quantitative and qualitative analyses of saliva and the instructions on the use, cleansing and storage of the mouthguard, which is a dental device used by athletes who need to wear oral protection during sports activities [6].
The first purpose of the present review is to describe the main diseases affecting the athletes’ oral cavity and the changes that occur in their oral ecosystem during sport training with and/or without use of mouthguard. The second objective is to delineate a program of prophylaxis and/or treatment for the diseases and oral changes reported.
2. The Oral Ecosystem and the Saliva Diagnostic Function
The oral ecosystem is a moist environment that includes the various anatomical microniches of the oral cavity and the oral microbiome. Two important physiological fluids, saliva and gingival crevicular fluid, wet the oral ecosystems and provide water, nutrients, adherence and antimicrobial factors [7].
Different physiochemical factors characterize the habitat of the oral cavity, thus supporting the development and growth of different microbial communities.
The oral microbiome includes a complex range of microorganisms, either present in saliva as organisms in the planktonic phase or, in the sessile phase, adhering to the oral surfaces as a dental plaque biofilm, namely 2000 taxa of bacteria, archaea and protozoa, fungi and viruses [7,8,9].
They are organized through a mechanism of mutual exchange of resources that give life to an ecosystem and, in most cases, they live in balance with each other and they bring significant benefits to the host organism. The major oral diseases, such as tooth decay and periodontal disease, arise from imbalance or dysbiosis within the plaque biofilm [7,8,9].
The gingival fluid is an exudate from plasma; it contains proteins, albumin, leukocytes, immunoglobulins and complement and is characterized by slow diffusion through the healthy gingiva which increases during inflammation [8].
Human saliva is a body fluid secreted by the salivary glands, whose function is to maintain the integrity of the hard and soft tissues of the oral cavity and to wet the mucous membranes of the mouth, throat and larynx in order to maintain the homeostasis of the oral ecosystem [10,11]. Normally, the daily salivary flow is estimated to be between 0.5 and 2 L [10]; the temperature of the saliva is more or less 35–36° and the pH is 7 ± 0.25, being saturated with calcium phosphates [11]. The buffer systems present in the saliva allow the maintenance of proper acid–base balance, swinging the pH values between 5.7 and 6.2 in the rest condition, to values of stimulated saliva of 8, depending on the habits of oral hygiene, food and the buffering action of saliva [12,13].
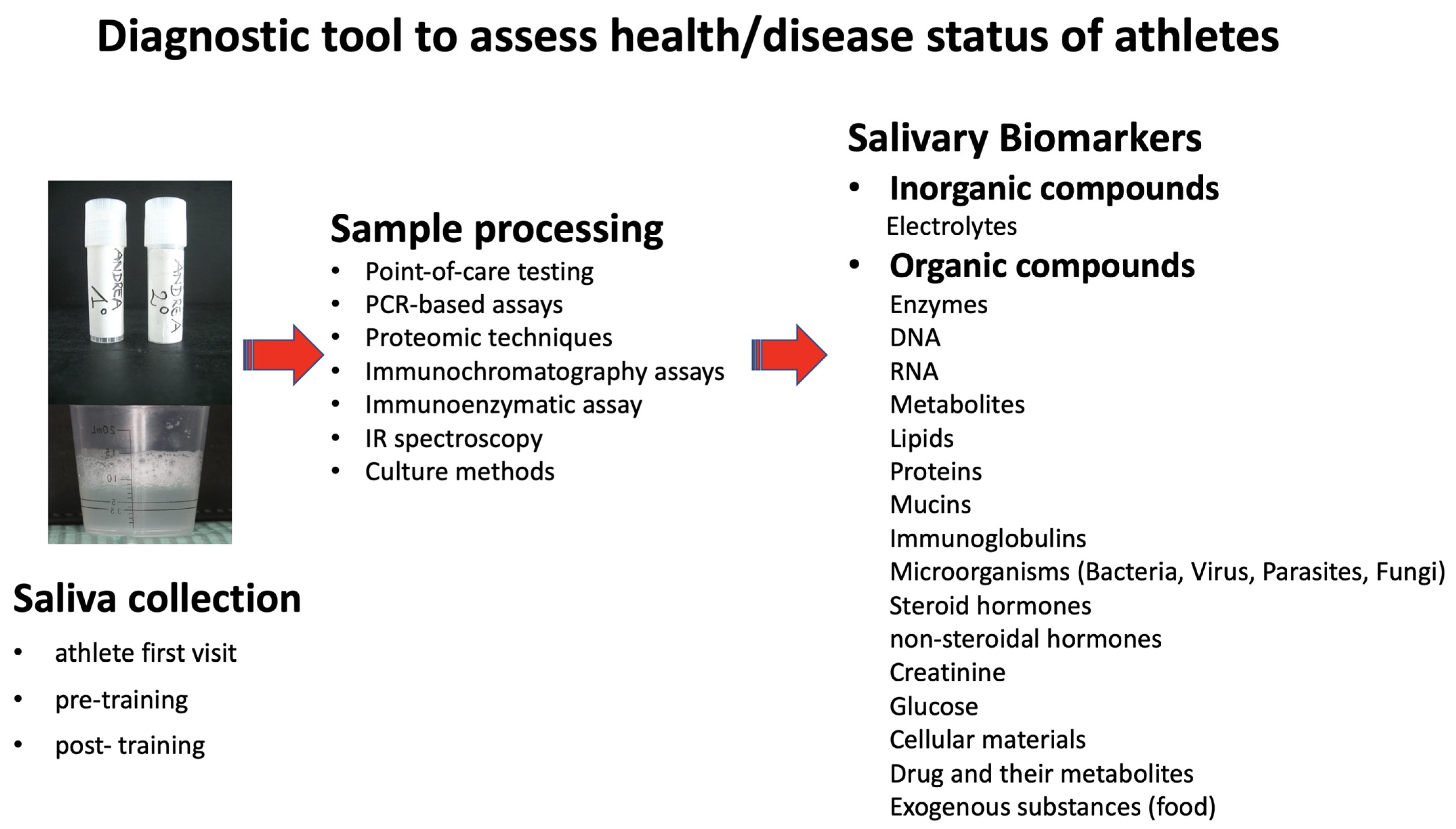
Saliva hosts a broad spectrum of proteins/peptides, nucleic acids, electrolytes, heavy metals, microorganisms, hormones, drugs and neurotransmitters that come from multiple local and systemic sources. Indeed, human saliva can be defined as a “body mirror” because it can reflect the physiological and pathological conditions of the whole body, including the oral cavity [13,14,15]. Therefore, it can represent an important diagnostic and monitoring tool in many fields such as dentistry, allowing healthcare providers to assess athletes, health or disease status [16] (Figure 1).
Differences between individuals in the microbiological composition of saliva can also be reflected in variations in the biochemical composition. However, several authors agree that changes in the oral microbiota accompany a number of dental diseases, given the complex composition of saliva and its importance for oral homeostasis. Moreover, considering that the methods of collection and the degree of stimulation of salivary flow can influence the salivary composition, it is necessary to develop standard operating procedures for the collection of the sample itself and for the storage conditions [17].
Numerous valid reasons lead us to use saliva as a diagnostic fluid to monitor the state of health and disease. Human saliva offers several advantages over other biological fluids, such as serum, as it is readily available; quick and easy to collect, store and ship; low cost in sufficient quantities for the analysis; is not susceptible to transformations; and is easy to handle for diagnostic procedures. The sampling is cost-efficient and stress-free [15,16,18,19]. Saliva collection is less invasive and safer than venous sampling, which could expose patients and health care providers to infectious diseases such as HIV or hepatitis virus [20].
The use of saliva can be performed in the field of sports medicine and exercise to examine exercise-related endocrinological, immunological and microbiological status as well as to assess training loads and subsequently the risk of developing diseases [19].
For example, determining cortisol concentrations in sequentially collected saliva samples in response to circadian rhythms to assess exercise stress can diagnose and prevent overtraining syndrome (OTS) in athletes. Overtraining syndrome is an accumulation of training and/or non-training stress that causes a decrease in long-term performance capacity with or without signs and symptoms related to physiological and psychological maladjustment, in which the restoration of performance capacity requires several weeks or months [21]. Moreover, an evaluation of salivary immunoglobulins (S-IgA) and antimicrobial proteins (α-amylase, lysozyme, lactoferrin) allows one to determine the effects of exercise on mucosal immunity. Decreases in S-IgA and antimicrobial protein concentration and/or secretion rate have been described in athletes during a training season, thus making the athlete more susceptible to upper respiratory tract infections [19]. Sport activities allow athletes to have a more “health-associated” intestinal microbiota. It is characterized by a greater presence of bacterial species that promote health, greater microbial diversity, functional metabolic capacity and metabolites associated with microbes, which can modulate mucosal immunity and improve gastrointestinal barrier function [22].
Finamore et al. demonstrated a link between saliva and intestinal profiles in patients with inflammatory bowel diseases (IBD), and this result suggests that, even in athletes, saliva sampling can also be used as a biomarker for gut disease in the oral–gut axis [23].
By analyzing the saliva, in particular the pH values, buffer capacity, flow rate and growth of cariogenic bacteria, it is possible to assess caries risk [24,25,26]. Further possibilities for diagnosing specific oral and systemic diseases can also be obtained by saliva tests, such as the assessment of periodontal diseases and atherosclerosis by checking salivary inflammatory cytokines including IL-1β, IL-6, TNF-α and prostaglandin E2; acute myocardial infarction by evaluating the concentration of C reactive protein (CRP); and pancreatic cancer by searching for the presence of Neisseria elongate and Streptococcus mitis [25,26,27].
At the same time, as a diagnostic tool, saliva has some disadvantages. Among the limits to the wide use of saliva, the great variability of its normal composition, attributable to diurnal/circadian variations of some biomolecules contained therein, must be regarded. Based on these variations, particular attention should be paid to the sampling procedure and the fixing of the reference limits for the concentrations of the individual components. At the same time, the high variability in the composition of saliva can be exploited for the monitoring of various biorhythms (seasonal, close to 24 h, circadian, etc.) in order to study the physiological characteristics of the human body during sport activities [15,19,28].
Research based on the use of infrared spectroscopy technique, applied to detect circadian changes in the content of biological fluids, including saliva, has shown that gender- and age-dependent differences have been reported for some physicochemical characteristics of human saliva [29].
Currently, all doctors, dentists and laboratories should favor the use of saliva following the example of the American National Institute of Dental and Craniofacial Research (ANIDCR) that, in 2002, removed all obstacles and approved these body fluids as a diagnostic tool for assessing health and disease status [25,26].
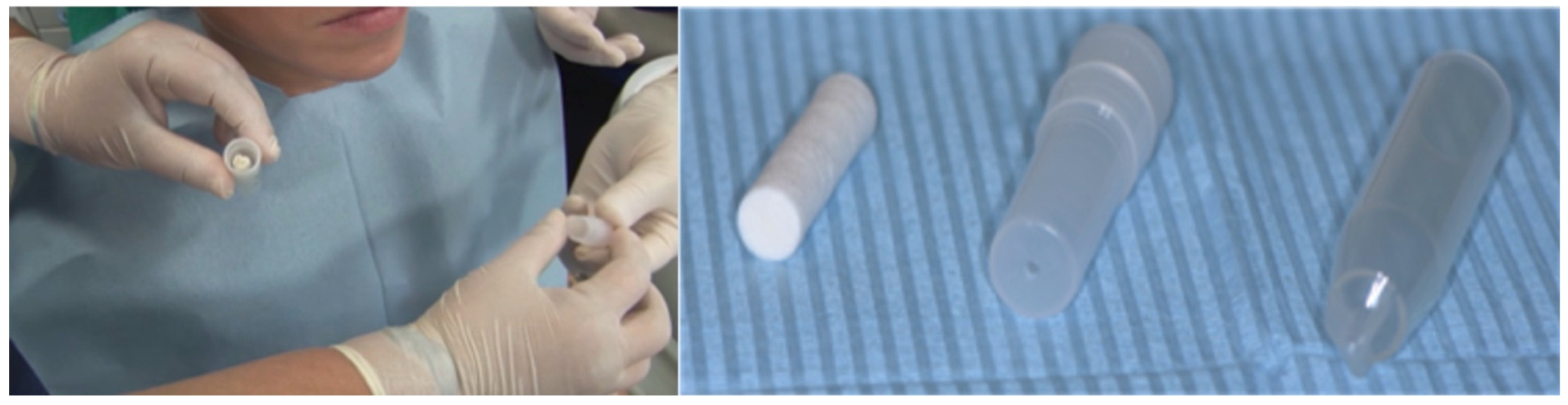
Thus, during the first visit of the athletes, salivary tests must be performed. The stimulated saliva can be collected with salivettes (Sarstedt AG & Co, Nümbrecht, Germany), with the athletes chewing the cotton roll present in the salivette for 1 min (Figure 2). The collected saliva can be subjected to chairside or laboratory analysis, in order to obtain information on microbiological, immunological and other ecological factors [30].
Moreover, the dentist must motivate the patient and can improve his compliance by determining the status of oral health through the saliva analysis. The checks must be continued during training, and must include new salivary tests for control of the variations in the oral ecological factors caused by sports activities and by use of the mouthguard.
Such attention to the starting situation and the changes that occur in the athletes’ oral cavity is justified by the need to resort to all available forms of prevention in order to preserve the oral health of athletes, usually adolescents.
3. Sports and Oral Health
The environment of the oral cavity is influenced by lifestyle, hygiene and eating habits, the possible intake of drugs and the performance of sports activities. Thanks to numerous researches carried out by sports dentists over the years, knowledge about the factors that regulate the oral ecology, such as salivary pH and flow, microbial load and S-IgA levels has been enlarged.
Firstly, diet, weekly frequency and training hours, climatic conditions and psychophysical stress conditions can produce significant variations in the oral ecosystem [1].
A review of the correlation between physical activity and oral health shows that the second seems to be low in a wide range of sports, and it is interesting to note how this condition is common in all competitive athletes. The sport can be considered one of the causes for bad oral health appearing in athletes [31,32].
The main diseases described frequently in the athletes’ oral cavity are caries, erosions and periodontal disease and several authors have analyzed the oral changes correlated to sports training. Needleman et al. (2015), examining young professional athletes, found that sport activities can be considered a risk factor among athletes from different sports for the onset of oral diseases, such as caries with an incidence between 15% and 70%; dental trauma 14–70%, dental erosion 36%, pericoronitis 5–39% and periodontal disease up to 15% [31,33,34,35].
Poor oral hygiene and all the physiological changes that occur during sport activities are fundamental factors in the development of oral and systemic diseases. The role played by oral bacteria is well known in cardiovascular diseases (atheromatous lesions, coronary disease), in esophageal cancer, colorectal and pancreatic cancer, as well as in rheumatoid arthritis [36].
Between several sport activities, football and swimming are the sports categories more at risk.
Gay Escoda et al., in a study on FC Barcelona players, reported values of the decayed, missing and filled teeth index (DMFT) that were used to evaluate caries prevalence of 5.7 and plaque index (PI), to evaluate oral hygiene according to Quigley and Hein, of 2.3 [37].
D’Ercole et al. demonstrated that young footballers had a salivary microbial load, relative to cariogenic microorganisms (such as S. mutans, Lactobacillus spp.), statistically higher than in boys who did not practice any sport, both before and at the end of sports training. A statistically significant decrease in S-IgA concentration also occurred after the training time [38].
These microbiological and immunological alterations expose young footballers to an increased risk in developing oral disease than sedentary subjects. In fact, the football players demonstrated a higher PI, an increase in dental discolorations, a higher frequency of bad habits (atypical swallowing, onychophagy) and a lower frequency of daily brushing in contrast to individuals who do not practice any kind of sports activity [38].
The training time is characterized by greater salivary function and intense physiological response. The decrease in the production of S-IgA and the association with an important intraoral growth of pathogenic bacteria leads us to consider the training period an open window for exposure to oral cavity diseases [39].
During exercise, intense physical activity produces lactic acid, which leads to a lowering of blood pH. A decrease in pH was also reported in the salivary level, before and after training. Changes in salivary pH are related to the level of CO2 in the blood: the levels of CO2 in the blood increase with the sport performance and, consequently, a high concentration of CO2 is transferred from the blood to saliva, with a consequent decrease in salivary pH [40].
Regarding the swimmers, the most common diseases reported are dental stains, caused by disinfectants of the pool water and by the time spent within the swimming pools. Although more than 6 h of training are required to develop them, they represent an esthetic problem with psychological repercussions; therefore, their onset must be considered as a health problem [32]. In addition, swimmers and water polo players are exposed to the onset of erosive tooth wear (ETW), a chemical-mechanical process characterized by a cumulative loss of hard dental tissue of a non-bacterial nature. This is a painful, irreversible condition and it is linked to the low pH values of the pool water (range 2.8–4.5), in contrast to normal values, equal to 7.2–8.0, or to an inadequate chlorination of the pool water [41,42].
Dental erosion is a common pathology among athletes and it can be correlated to the high consumption of food and drink in young people and sportspeople.
The widespread use, during sports activities, of sugary drinks with a very low pH, often lower than 3, depends on the spread of the internet and social media, that promotes the use of energy drinks, based on electrolytes and carbohydrates, in order to compensate hypoglycemia, dehydration, depletion of mineral salts and muscle glycogen that occur in athletes during physical activity. Indeed, the use of nutritional supplements is not supported by valid scientific literature and a healthy diet does not need mineral supplements [43,44,45].
The multifactorial nature of the pathogenesis of erosion in regards to both the use/abuse of energy drinks, takes into account the variables between the different drinks, the frequency with which they are introduced, the buffering power of saliva at the time of intake, the type of diet, the level of hydration and the degree of oral hygiene of the athletes [40,46,47,48,49,50].
Performing sports such as swimming in a well-controlled way and with adequate training can, on the contrary, induce benefits to the athlete.
D’Ercole et al., in competitive swimmers, showed a statistically significant decrease in S-IgA values, but their mean values were significantly higher than in non-competitive swimmers. Moreover, the cariogenic bacteria were present in the saliva of competitive swimmers with lower frequency than the “protective” microorganisms such as S. sanguinis, thus exposing athletes to a lesser risk of attracting caries, as confirmed clinically by lower values of active caries [2].
4. Sport Mouthguard: Effects on the Oral Ecosystem
Competitive athletes follow challenging training regimes to obtain optimum performance. Although sports activities have beneficial effects to general health, they also expose the athlete to an onset of oral diseases, including dental trauma; regardless of their origin (school, work, play, violence or accidental), they reflect on patient’s quality of life and require immediate treatment and a program of prevention of any future consequences.
The mouthguard is an oral device that, when inserted in the mouth, covers the palate and all occlusal surfaces of the teeth, to reduce oral–maxillofacial trauma and to protect the oral hard and soft tissues from fractures and lacerations and the maxillaries from fractures and dislocations [51,52].
The American Standards for Testing Materials classifies mouthguards into three categories: stock, boil and bite and custom-made [52].
Ethylene vinyl acetate (EVA) is the most suitable material for the mouthguard. It is a polymeric plastic of ethylene and vinyl acetate, characterized by flexibility, elasticity and certified biocompatibility [52,53].
The primary function of the mouthguard is trauma prevention; however, this device can be utilized for other functions, for example, as a reservoir of materials designed to prevent oral diseases, such as chlorhexidine, fluorine, casein. Moreover, it can be a valid aid in the athlete’s performance, as it provides a psychological and a physical advantage.
Chiavaroli et al. showed an inhibition of 8-iso-prostaglandin2α, a marker of antioxidant deficiency and lipid peroxidation, in salivary release in athletes who used the mouthguard during the game. In contrast, the authors described a significant increase in the salivary isoprostane level in athletes who did not use the mouthguard [54].
Recent studies showed that the use of the mouthguard improved physical performance by increasing, in both aerobic and anaerobic activities, the respiratory capacity of athletes [55]. In subjects with reduced respiratory capacity, as in patients with cystic fibrosis, 8-iso-PGF2α concentration was significantly higher than in healthy controls [56]. Based on results obtained, Chiavaroli et al. hypothesized that the use of the mouthguard increases aerobic performance and leads to a further decrease in 8-iso-PGF2α release with a reduction in oxidative stress [54].
Considering numerous advantages, custom-made mouthguards, conceived and realized by specialized dentists and dental technicians to guarantee the characteristics of protection, stability, individuality and comfort, must be adopted in all sports activities.
Despite the obvious benefits of using the mouthguard, including the possibility of overcoming communication, hydration and nutrition difficulties, the clinician should not overlook other problems that may arise from its use, especially in professional sportsmen who undergo several hours of training every day.
In fact, inadequately designed, worn and jagged-edged mouthguards can result in injuries to the oral mucosa, such as hyperkeratosis, erythema and ulceration, as described in the mouths of athletes who had worn boil and bite mouthguards for an entire competitive season. Several authors reported that the wounds caused by damaged mouthguards, at the oral level, can favor the entry of microorganisms present on the surface of the mouthguard into the bloodstream, with consequent opportunistic systemic infections (eg., endocarditis, pericarditis, pneumonia, etc.) [57,58].
As described by Glass et al., the boil and bite mouthguards can be contaminated by several microorganisms and therefore can become a microbial reservoir from which can be generated oral and systemic diseases [59].
“Boil and bite” mouthguards, worn by hockey and football players, harbored many pathogenic and opportunistic bacteria, yeasts and molds. The main bacterial species found on mouthguard surfaces were: Staphylococcus spp., Micrococcus spp., Brevibacterium spp. and Cellulomonas spp. The most common species of yeasts were Candida parapsilosis and Rhodotorula mucilaginosa, while the most common species of mold were Bipolaris/Cochliobolus spp. and Penicillium chrysogenum [58,60].
Batoni et al. reported that the use of oral removable devices creates new retention niches that favor S. mutans biofilm colonization [61].
Glass et al., with the aid of SEM, hypothesize that the pathogenic change of the microorganisms on the surface of the mouthguard may depend on the material wear and tear and on the difficulty in preserving it [58,59].
D’Ercole et al., in a study performed to monitor changes in the oral cavity by determining clinical, salivary and bacterial markers, before, during and after sports treatment with custom-made mouthguard, confirm that the use of these dental devices is among the factors that can affect oral homeostasis [53].
They reported that the prolonged use of the device elevates full mouth plaque score (FMPS) and full mouth blood score (FMBS) and decreases the buffering capacity and salivary pH, thus inhibiting the saliva protective effect [53]. In this study, Saliva-Check Mutans GC® test demonstrated that the microbial load of Streptococcus mutans remained unvaried during the observation period, according to Sanpei et al. and Lara-Carrillo et al. In addition, one year of therapy leads to a worsening of the patient’s clinical indexes, because they lose the motivation to maintain good oral hygiene [62,63].
5. Sport Mouthguard in the Prevention of Oral Diseases
Competitive players can achieve high performance only in the presence of a state of health.
Boil and bite mouthguards are the most used by athletes for their low cost and easy access but at the same time they have numerous disadvantages.
Instead, it is important to emphasize that custom-made mouthguards have many advantages over stock and ready-made: they show optimum comfort and a good fit and they reveal no negative effects on faction satisfaction of elite Taekwondo athletes. Moreover, they offer protection against orofacial injuries and allow stable muscular activity during the training of Karate-Dō athletes [52,64].
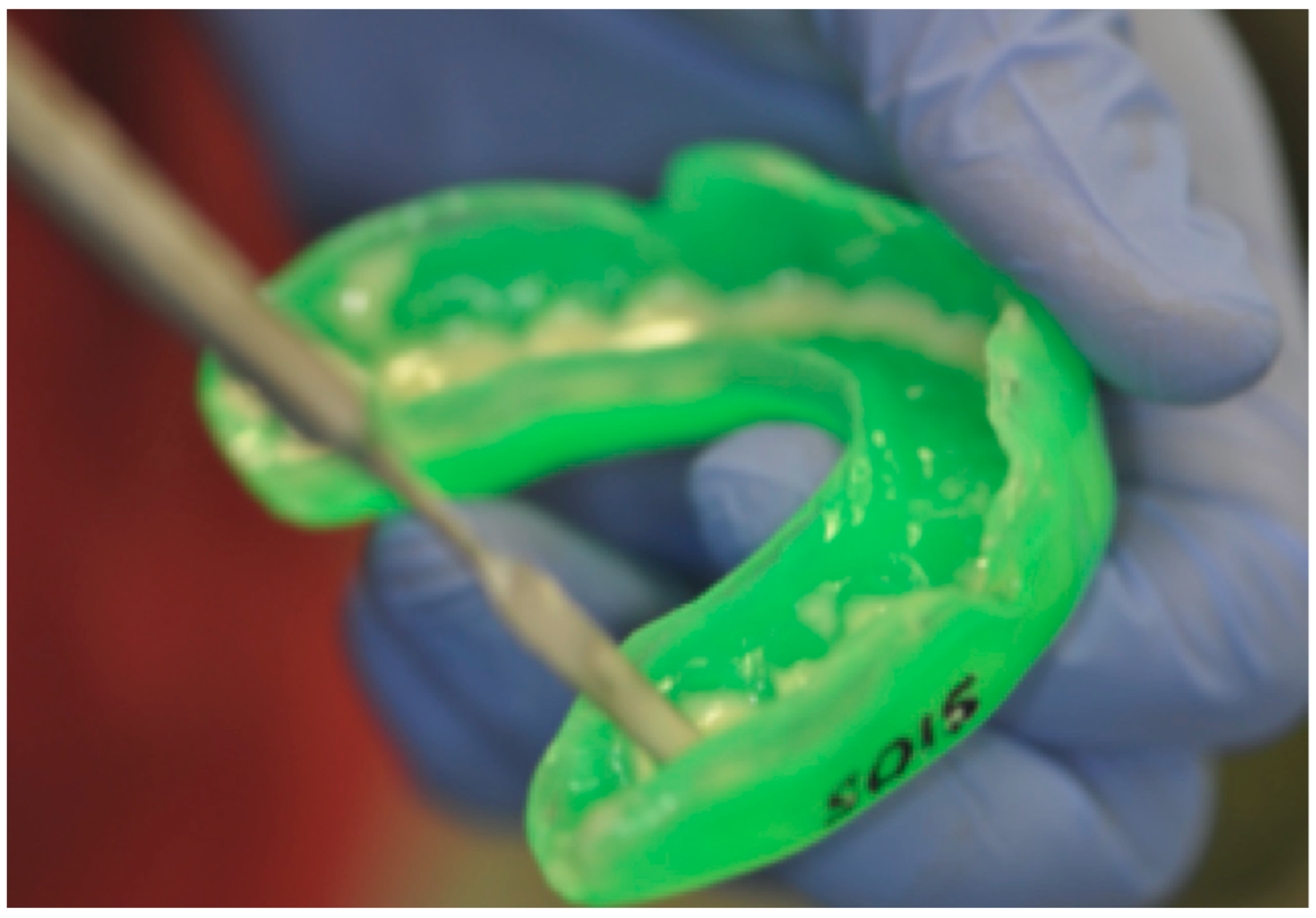
To prevent oral damage caused by the prolonged use of mouthguard and the adhering pathogenic microorganisms, some strategies can be used, such as addition of protective substances inside the device (Figure 3). The chlorhexidine can be used as an active ingredient for preventing and reducing the colonization, development and pathogenicity of dental plaque [65].
The use of chlorhexidine in the mouthguard was encouraged by the effects obtained from D’Ercole et al. in an in vivo study. From this study emerged the observation that the addition of chlorhexidine, during the training time, inhibits microbial proliferation on the support itself and reduces the salivary concentration of Streptococcus mutans, Candida spp. and molds. Moreover, the contemporary use increases the value of the salivary pH and buffering capacity [66,67].
According to the different needs of the patient, other materials such as fluoride and casein can be used.
Fluoride is indicated for patients who need a fluoroprophylaxis protocol, which involves the use of fluoride (toothpaste and/or gel) to strengthen dental enamel and to make it less susceptible to bacterial attack and to the formation of caries [1].
Research on casein showed that its application in custom-made EVA mouthguards is able to directly counteract the adhesion of plaque on the surface of the teeth and to increase pH values, salivary flow, amount of stimulated saliva and buffer capacity, improving the oral health of the athletes [68].
The positive effects on the white spot lesions, the increase of salivary flow, buffering capacity and pH values, are referred to by Hegde and Thakkar, through the use of casein-chewing gums [69].
Nagai et al. propose to insert a bioactive filler into the structure of the EVA material. This new material proved to be bacteriostatic against Streptococcus mutans and Porphyromonas gingivalis and it has no cytotoxic effect on human gingival cells [70]. Yoshida et al. showed that silver nanoparticles, embedded in the EVA matrix, exhibited effective antibacterial properties against Streptococcus sobrinus, Porphyromonas gingivalis and Escherichia coli, thus suggesting the use of this material for the construction of mouthguards [71].
Sadly, bacteria, saliva and food debris tend to accumulate on the mouthguard, giving it an unpleasant smell and taste, thereby requiring constant cleaning of the device [59].
Following the basic rules of oral hygiene before exercise and cleaning the device after each use can prevent damage to the oral cavity. Unfortunately, athletes tend to easily neglect the rules of conservation and cleaning of the mouthguard. Namba et al., in an interview given by 22 rugby players, showed that only two of them were properly guided by a sports dentist on ways to sanitize their mouthguard [72].
There are still no precise and well-coded rules for the maintenance of mouthguards and few authors have described them. Barton recommended daily disinfection by immersion in a commercially available antimicrobial denture-cleansing solution [73]. Ogawa achieved efficient hygienic storage of EVA dental devices by washing them with sterilized water and storing them in a ventilated environment [74].
D’Ercole et al., testing different disinfectants, demonstrated that there is no ideal method. The solutions such as hydrogen peroxide, 0.5% sodium hypochlorite and Oral Care Foam™ resulted in a significant reduction of microorganisms adhering to the surface and achieved optimal mouthguard disinfection. SEM observation confirmed that the different substances, indicated above, reduce the development of microbial communities on the EVA surface [67].
In general, the athlete must still be advised to carry out daily hygiene of the mouthguard with appropriate antimicrobial solutions; not to leave the device soaking in the detergent solution for a long time, to prevent it from taking on a bitter taste and acquiring a viscous surface film; not to immerse it in mouthwashes or solutions containing alcohol, to avoid deterioration of the material; and, finally, to rinse the mouthguard dipped in the cleaning solution before inserting it into the mouth [66,73,74].
As for storage, many athletes do not care about the possible contamination of the mouthguard and deposit it everywhere. The most suitable method for storage remains the use of perforated containers that allow ventilation, after drying the mouthguard with a napkin to remove liquid residues.
Moreover, it is necessary to specify that mouthguards are made with a highly deformable plastic material when exposed to high temperatures [75].
For this reason, it is recommended not to dry it with a hairdryer, not to use boiling water and to avoid exposure to direct sunlight for long periods of time.
6. Conclusions
Studies carried out on effects of sports activities on the oral cavity are different and concern several aspects of this issue. Although sport is an absolutely healthy and positive habit in the life of the young or adult people, it can be considered a lifestyle at risk for development of various pathologies.
These risks can be avoided by using a custom-made mouthguard due to its triple function: protection against sports-related injuries; reservoir of substances protective for the oral ecology; improvement of athletic performance.
Moreover, monitoring the athletes with oral health screening, clinical examination, salivary analysis and implementing oral health promotion programs may provide an assessment of sport athletes’ risk status for developing several diseases.
The study of microbial markers, immune status and habits of sports subjects is essential to establish the management of the training load, with the aim of reducing physical stress, the risk of oral infection and a worsening of the quality of life (oral diseases affect self-esteem, nutrition and health, as they cause pain, anxiety and social discomfort).
Since the disease can stop exercise and performance, further research, to clarify how the sports training affects immunity and health status, is needed.
In the future, analysis of saliva could be applied in a personalized way to choose the best diet and training program for the individual to achieve the best possible performance and to prevent athletes’ injuries.
Author Contributions
Conceptualization, S.D.; methodology, D.T. and A.C.; investigation, D.F.; resources, D.T.; data curation, S.D.; writing—original draft preparation, S.D. and A.C.; writing—review and editing, D.T. and D.F. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Gallagher, J.; Ashley, P.; Needlman, I. Implementation of a behavioural change intervention to enhance oral health behaviours in elite athletes: A feasibility study. BMJ Open Sport Exerc. Med. 2020. [Google Scholar] [CrossRef]
- D’Ercole, S.; Tieri, M.; Martinelli, D.; Tripodi, D. The effect of swimming on oral health status: Competitive versus non-competitive athletes. J. Appl. Oral Sci. 2016, 24, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Spinas, E.; Mameli, A.; Giannetti, L. Traumatic dental injuries resulting from sports activities; immediate treatment and five years follow-up: An observational study. Open Dent. J. 2018, 12, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Giuca, M.R.; Pasini, M.; Tecco, S. Levels of salivary immunoglobulins and periodontal evaluation in smoking patients. BMC Immunol. 2014, 15. [Google Scholar] [CrossRef] [Green Version]
- Nieman, D.C.; Henson, D.A.; Fagoaga, O.R. Change in salivary IgA following a competitive marathon race. Int. J. Sports Med. 2002, 69–75. [Google Scholar] [CrossRef]
- Knapik, J.J.; Marshall, S.W.; Lee, R.B.; Darakjy, S.S.; Jones, S.B.; Mitchener, T.A.; Dela Cruz, G.; Jones, B.H. Mouthguards in sport activities: History, physical properties and injury prevention effectiveness. Sports Med. 2007, 37, 117–144. [Google Scholar] [CrossRef]
- Samaranayake, L.; Matsubara, V.H. Normal oral flora and the oral ecosystem. Dent. Clin. N. Am. 2017, 61, 199–215. [Google Scholar] [CrossRef]
- Marsh, P.D. In sickness and in health-what does the oral microbiome mean to us? An ecological perspective. Adv. Dent. Res. 2018, 29, 60–65. [Google Scholar] [CrossRef]
- Marcotte, H.; Lavoie, M.C. Oral microbial ecology and the role of salivary immunoglobulin A. Microbiol. Mol. Biol. Rev. 1998, 62, 71–109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaufman, E.; Lamster, I.B. The diagnostic applications of saliva—A review. Crit. Rev. Oral Biol. Med. 2002, 13, 197–212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Amerongen, A.V.; Veerman, E.C. Saliva--the defender of the oral cavity. Oral Dis. 2002, 8, 12–22. [Google Scholar] [CrossRef] [Green Version]
- Mese, H.; Matsuo, R.J. Salivary secretion, taste and hyposalivation. Oral Rehabil. 2007, 34, 711–723. [Google Scholar] [CrossRef] [PubMed]
- Pfaffe, T.; Cooper-White, J.; Beyerlei, P.; Kostner, K.; Punyadeera, C. Diagnostic potential of saliva: Current state and future applictions. Clin. Chem. 2012, 36, 126–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- García-Godoy, F.; Hicks, M.J. Maintaining the integrity of the enamel surface: The role of dental biofilm, saliva and preventive agents in enamel demineralization and remineralization. J. Am. Dent. Assoc. 2008, 139, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Segal, A.; Wong, D.T. Salivary diagnostics: Enhancing disease detection and making medicine better. Eur. J. Dent. Educ. 2008, 12, 22–29. [Google Scholar] [CrossRef]
- Wong, D.T. Salivary diagnostics: Scientific and clinical frontiers. Adv. Dent. Res. 2011, 23, 350–352. [Google Scholar] [CrossRef]
- Ilea, A.; Andrei, V.; Feurdean, C.N.; Băbțan, A.M.; Petrescu, N.B.; Câmpian, R.S.; Boșca, A.B.; Ciui, B.; Tertiș, M.; Săndulescu, R.; et al. Saliva, a magic biofluid available for multilevel assessment and a mirror of general health-a systematic review. Biosensors (Basel) 2019, 9, 27. [Google Scholar] [CrossRef] [Green Version]
- Mandel, I.D. Salivary diagnosis: More than a lick and a promise. J. Am. Dent. Assoc. 1993, 124, 85–87. [Google Scholar] [CrossRef]
- Papacosta, E.; Nassis, G.P. Saliva as a tool for monitoring steroid, peptide and immune markers in sport and exercise science. J. Sci. Med. Sport 2011, 5, 424–434. [Google Scholar] [CrossRef]
- Wang, A.; Wang, C.; Tu Wong, D.T. Oral biofluid biomarker research: Current status and emerging frontiers. Diagnostics (Basel) 2016, 6, 45. [Google Scholar] [CrossRef]
- Ushiki, K.; Tsunekawa, K.; Shoho, Y.; Martha, L.; Ishigaki, H.; Matsumoto, R.; Yanagawa, Y.; Nakazawa, A.; Yoshida, A.; Nakajima, K.; et al. Assessment of exercise-induced stress by automated measurement of salivary cortisol concentrations within the circadian rhythm in Japanese female long-distance runners. Sports Med. Open 2020, 6, 38. [Google Scholar] [CrossRef] [PubMed]
- Mohr, A.E.; Jäger, R.; Carpenter, K.C.; Kerksick, C.M.; Purpura, M.; Townsend, J.R.; West, N.P.; Black, K.; Gleeson, M.; Pyne, D.B.; et al. The athletic gut microbiota. J. Int. Soc. Sports Nutr. 2020, 17, 24. [Google Scholar] [CrossRef] [PubMed]
- Finamore, A.; Peluso, I.; Cauli, O. Salivary stress/immunological markers in crohn’s disease and ulcerative colitis. Int. J. Mol. Sci. 2020, 13, 8562. [Google Scholar] [CrossRef]
- Hegde, M.N.; Attavar, S.H.; Shetty, N.; Hegde, N.D.; Hegde, N.N. Saliva as a biomarker for dental caries: A systematic review. J. Conserv. Dent. 2019, 22, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Mummolo, S.; Marchetti, E.; Giuca, M.R. In-office bacteria test for a microbial monitoring during the conventional and self-ligating orthodontic treatment. Head Face Med. 2013, 9. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubala, E.; Strzelecka, P.; Grzegocka, M.; Lietz-Kijak, D.; Gronwald, H.; Piotr, S.; Kijak, E. A review of selected studies that determine the physical and chemical properties of saliva in the field of dental treatment. Biomed Res. Int. 2018, 13. [Google Scholar] [CrossRef] [PubMed]
- Hemadi, A.S.; Huang, R.; Zhou, Y.; Zou, J. Salivary proteins and microbiota as biomarkers for early childhood caries risk assessment. Int. J. Oral Sci. 2017, 9, e1. [Google Scholar] [CrossRef] [Green Version]
- Bel’skaya, L.V.; Kosenok, V.K.; Sarf, E.A. Chronophysiological features of the normal mineral composition of human saliva. Arch. Oral Biol. 2017, 82, 286–292. [Google Scholar] [CrossRef]
- Bel’skaya, L.V.; Sarf, E.A.; Solomatin, D.V. Age and gender characteristics of the infrared spectra of normal human saliva. Appl. Spectrosc. 2020, 74, 536–543. [Google Scholar] [CrossRef]
- Mummolo, S.; Tieri, M.; Tecco, S. Clinical evaluation of salivary indices and levels of Streptococcus mutans and Lactobacillus in patients treated with Occlus-o-Guide. Eur. J. Paediatr. Dent. 2014, 15, 367–370. [Google Scholar] [CrossRef] [PubMed]
- Needleman, I. Oral health and elite sport performance. Br. J. Sports Med. 2015, 49, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Escartin, J.L.; Arnedo, A.; Pinto, V.; Vela, M.J. A study of dental staining among competitive swimmers. Community Dent. Oral Epidemiol. 2000, 28, 10–17. [Google Scholar] [CrossRef]
- Ashley, P.; Di Iorio, A.; Cole, E. Oral health of elite athletes and association with performance: A systematic review. Br. J. Sports Med. 2015, 49, 14–19. [Google Scholar] [CrossRef] [PubMed]
- Petersen, P.E.; Bourgeois, D.; Ogawa, H.; Estupinan-Day, S.; Ndiaye, C. The global burden of oral diseases and risks to oral health. Bull. World Health Organ. 2005, 83, 661–669. [Google Scholar] [PubMed]
- Spinas, E.; Giannetti, L.; Mameli, A.; Re, D. Dental injuries in young athletes, a five-year follow-up study. Eur. J. Paediatr. Dent. 2018, 19, 187–193. [Google Scholar]
- Bourgeois, D.; Inquimbert, C.; Ottolenghi, L.; Carrouell, F. Periodontal pathogens as risk factors of cardiovascular diseases, diabetes, rheumatoid arthritis, cancer, and chronic obstructive pulmonary disease-is there cause for consideration? Microorganisms 2019, 7, 424. [Google Scholar] [CrossRef] [Green Version]
- Gay-Escoda, C.; Vieira-Duarte-Pereira, D.M.; Ardèvol, J.; Pruna, R.; Fernandez, J.; Valmaseda-Castellòn, E. Study of the effect of oral health on physical condition of professional soccer players of the Football Club Barcelona. Med. Oral Patol. Oral Cir. Bucal 2011, 16, 436–439. [Google Scholar] [CrossRef] [Green Version]
- D’Ercole, S.; Tripodi, D.; Ristoldo, F.; Quaranta, F.; Amaddeo, P. Analysis of oral health status and of salivary factors in young soccer players: A pilot study. Med. Dello Sport 2013, 66, 71–80. [Google Scholar]
- D’Ercole, S.; Tripodi, D. The effect of swimming on oral ecological factors. J. Biol. Regul. Homeost. Agents 2013, 2, 551–558. [Google Scholar]
- Tanabe-Ikegawa, M.; Takahashi, T.; Churei, H.; Mitsuyama, A.; Ueno, T. Interactive effect of rehydration with diluted sports drink and water gargling on salivary flow, pH, and buffering capacity during ergometer exercise in young adult volunteers. J. Oral Sci. 2018, 60, 269–277. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bretz, W.A.; Carrilho, M.R. Salivary parameters of competitive swimmers at gas-chlorinated swimming-pools. J. Sports Sci. Med. 2013, 12, 207–208. [Google Scholar]
- Lussi, A.; Schlueter, N.; Rakhmatullina, E.; Ganss, C. Dental erosion: An overview with emphasis on chemical and histopathological aspects. Caries Res. 2011. [Google Scholar] [CrossRef]
- Anttonen, V.; Kemppainen, A.; Niinimaa, A.; Pesonen, P.; Tjaderhane, L.; Jaana, L. Dietary and oral hygiene habits of active athletes and adolescents attending ordinary junior high schools. Int. J. Paediatr. Dent. 2014, 24, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Committee on Nutrition and the Council on Sport Medicine and Fitness. Sports drinks and energy drinks for children and adolescents: Are they appropriate? Pediatrics 2011, 127, 1182–1189. [Google Scholar] [CrossRef] [Green Version]
- Kaczmarek, W. The status of mineralized dental tissues in young competitive swimmers. Acad. Med. Stetin. 2010, 56, 81–86. [Google Scholar]
- Grippo, J.O.; Simring, M.; Coleman, T.A. Abfraction, abrasion, biocorrosion, and the enigma of noncarious cervical lesions: A 20-year perspective. J. Esthet. Restor. Dent. 2012, 24, 10–23. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Zou, Y.; Ding, G. Correction: Dietary factors associated with dental erosion: A meta-analysis. PLoS ONE 2016, 11, e0161518. [Google Scholar] [CrossRef]
- Chrysanthakopoulos, N.A. Prevalence of tooth erosion and associated factors in 13-16-year old adolescents in Greece. J. Clin. Exp. Dent. 2012, 4, 160–166. [Google Scholar] [CrossRef]
- Sheiham, A.; James, W.P. Diet and dental caries: The pivotal role of free sugars reemphasized. J. Dent. Res. 2015, 94, 1341–1347. [Google Scholar] [CrossRef]
- Bellomo, R.G.; Tripodi, D.; Bosna, C.; D’Ercole, S.; Barassi, G.; Porreca, A.; Veraldi, R.; Prosperi, L.; Barbato, C. Mediterranean diet and physical activity improve posture, fat mass and salivary pH. J. Biol. Regul. Homeost. Agents 2018, 32, 1317–1321. [Google Scholar] [PubMed]
- Kaur, G.; Mangat, S.S. Attitude toward mouthguard utilization among North Indian school children. J. Int. Soc. Prev. Community Dent. 2016, 6, 69–74. [Google Scholar] [CrossRef] [Green Version]
- Spinas, E.; Aresu, M.; Giannetti, L. Use of mouth guard in basketball: Observational study of a group of teenagers with and without motivational reinforcement. Eur. J. Paediatr. Dent. 2014, 15, 392–396. [Google Scholar]
- D’Ercole, S.; Martinelli, D.; Tripodi, D. Influence of sport mouthguard on the ecological factor of the children oral cavity. BMC Oral Health 2014, 14, 97. [Google Scholar] [CrossRef] [Green Version]
- Chiavaroli, A.; D’Ercole, S.; Fulco, D.; Ferrante, C.; Orlando, G.; Recinella, L.; Tripodi, D. The use of customized mouthguards during the training produced protective effects on salivary factors of young athletes. EJPD 2021, (in press). [Google Scholar]
- Schultz Martins, R.; Girouard, P.; Elliott, E.; Mekary, S. Physiological responses of a jaw-repositioning custom-made mouthguard on airway and their effects on athletic performance. J. Strength Cond. Res. 2018. [Google Scholar] [CrossRef]
- Spicuzza, L.; Parisi, G.F.; Tardino, L.; Ciancio, N.; Nenna, R.; Midulla, F.; Leonardi, S. Exhaled markers of antioxidant activity and oxidative stress in stable cystic fibrosis patients with moderate lung disease. J. Breath Res. 2018, 12, 026010. [Google Scholar] [CrossRef] [PubMed]
- Glass, R.T.; Conrad, R.S.; Wood, C.R. Protective athletic mouthguards: Do they cause harm? Sports Health 2009, 1, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Glass, R.T.; Wood, C.R.; Bullard, J.W.; Conrad, R.S. Possible disease transmission by contaminated mouthguards in two young football players. Gen. Dent. 2007, 55, 436–440. [Google Scholar] [PubMed]
- Glass, R.T.; Conrad, R.S.; Kohler, G.A.; Warren, A.J.; Bullard, J.W. Microbiota found in protective athletic mouthguards. Sports Health 2011, 3, 244–248. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glass, R.T.; Bullard, J.W.; Conrad, R.S. The contamination of protective mouthguards: A characterization of the microbiota found in football players’ protective mouthguards as compared to the oral microbiota found in first-year medical students. J. Amer. Dent. Inst. Cont. Educ. 2006, 93, 23–38. [Google Scholar]
- Batoni, G.; Pardini, M.; Giannotti, A.; Ota, F.; Giuca, M.R.; Gabriele, M.; Campa, M.; Senesi, S. Effect of removable orthodontic appliances on oral colonisation by mutans streptococci in children. Eur. J. Oral Sci. 2001, 109, 388–392. [Google Scholar] [CrossRef]
- Sanpei, S.; Endo, T.; Shimooka, S. Caries risk factors in children under treatment with sectional brackets. Angle Orthod. 2010, 80, 509–514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lara-Carrillo, E.; Montiel-Bastida, N.M.; Sanchez-Perez, L.; Alais-Tavira, J. Effect of orthodontic treatment on saliva, plaque and the levels of Streptococcus mutans and Lactobacillus. Med. Oral Patol. Oral Cir. Bucal 2010, 15, 924–929. [Google Scholar] [CrossRef] [Green Version]
- Raquel, G.; Namba, E.L.; Bonotto, D.; Ribeiro Rosa, E.A.; Trevilatto, P.C.; Naval Machado, M.Â.; Vianna-Lara, M.S.; Azevedo-Alanis, L.R. The use of a custom-made mouthguard stabilizes the electromyographic activity of the masticatory muscles among Karate-Dō athletes. J. Bodyw. Mov. Ther. 2016, 21, 109–116. [Google Scholar] [CrossRef]
- Mummolo, S.; D’Ercole, S.; Marchetti, E.; Campanella, V.; Martinelli, D.; Marzo, G.; Tripodi, D. Oral antiseptic and periodontitis: A clinical and microbiological study. Oral Health Dent. Manag. 2014, 13, 698–702. [Google Scholar] [PubMed]
- D’Ercole, S.; Tieri, M.; Fulco, D.; Martinelli, D.; Tripodi, D. The use of chlorhexidine in mouthguards. J. Biol. Regul. Homeost. Agents 2017, 31, 487–493. [Google Scholar] [PubMed]
- D’Ercole, S.; Tieri, M.; Martinelli, D.; Ciaravino, C.; Fulco, D.; Tripodi, D. Microbial contamination and disinfection of sport mouthguard: In vitro study. Curr. Microbiol. 2020, 77, 246–253. [Google Scholar] [CrossRef]
- Tripodi, D.; Martinelli, D.; Ciaravino, C.; Fulco, D.; Tieri, M.; D’Ercole, S. The use of casein in sport mouthguards: Microbiological and ecological variations in oral cavity. J. Biol. Regul. Homeost. Agents 2018, 32, 1045–1049. [Google Scholar]
- Hegde, R.J.; Thakkar, J.B. Comparative evaluation of the effects of casein phosphopeptide-amorphous calcium phosphate (CPP-ACP) and xylitol-containing chewing gum on salivary flow rate, pH and buffering capacity in children: An in vivo study. J. Indian Soc. Pedod. Prev. Dent. 2017, 35, 332–337. [Google Scholar] [CrossRef]
- Nagai, K.; Domon, H.; Oda, M.; Shirai, T.; Ohsumi, T.; Terao, Y.; Arai, Y. Antimicrobial activity of ethylene-vinyl acetate containing bioactive filler against oral bacteria. Dent. Mater. J. 2017, 36, 784–790. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, Y.; Churei, H.; Takeuchi, Y.; Wada, T.; Uo, M.; Izumi, Y.; Ueno, T. Novel antibacterial mouthguard material manufactured using silver-nanoparticle-embedded ethylene-vinyl acetate copolymer masterbatch. Dent. Mater. J. 2018, 37, 437–444. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Namba, E.; Strapasson, A.; Jarzynski, J.; Baratto, S.P.; Tomazinho, P.H. Sanitization of sports mouthguards. RSBO 2013, 10, 72–75. [Google Scholar]
- Barton, L. Mouthguards: Daily Sanitizing between Uses Urged. 2016. Available online: https://www.momsteam.com/health-safety/mouth-guards-daily-sanitizing-between-uses-urged (accessed on 1 April 2021).
- Ogawa, T.; Yamasaki, S.; Honda, M.; Terao, Y.; Kawabata, S.; Maeda, Y. Long-term survival of salivary streptococci on dental devices made of ethylene vinyl acetate. Int. J. Oral Sci. 2012, 4, 14–18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gould, T.E.; Piland, S.G.; Shin, J.; Hoyle, C.E.; Nazarenko, S. Characterization of mouthguard materials: Physical and mechanical properties of commercialized products. Dent. Mater. 2009, 25, 771–780. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Human saliva collected from an athlete for the research of the main biomarkers.

Figure 2.
The collection of stimulated saliva with salivettes.
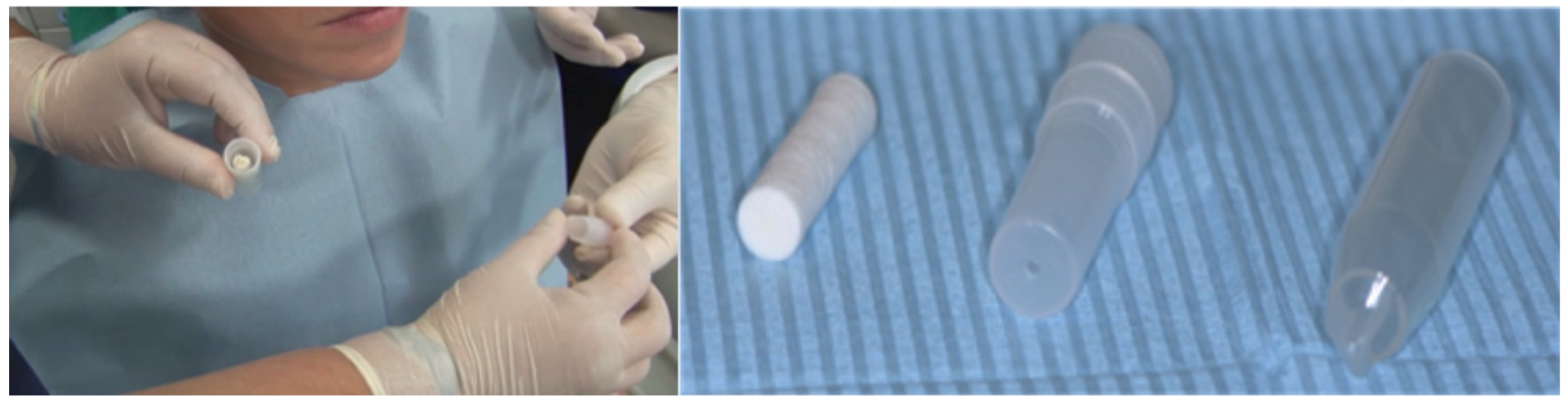
Figure 3.
Addition of protective substances inside the device to prevent oral damage caused by the mouthguard.
Figure 3.
Addition of protective substances inside the device to prevent oral damage caused by the mouthguard.

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Tripodi, D.; Cosi, A.; Fulco, D.; D’Ercole, S. The Impact of Sport Training on Oral Health in Athletes. Dent. J. 2021, 9, 51. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9050051
AMA Style
Tripodi D, Cosi A, Fulco D, D’Ercole S. The Impact of Sport Training on Oral Health in Athletes. Dentistry Journal. 2021; 9(5):51. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9050051
Chicago/Turabian StyleTripodi, Domenico, Alessia Cosi, Domenico Fulco, and Simonetta D’Ercole. 2021. "The Impact of Sport Training on Oral Health in Athletes" Dentistry Journal 9, no. 5: 51. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9050051
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.