
Effects of Different Application Times of Silver Diamine Fluoride on Mineral Precipitation in Demineralized Dentin

 ,
, 
Abstract
:
1. Introduction
2. Material and Methods
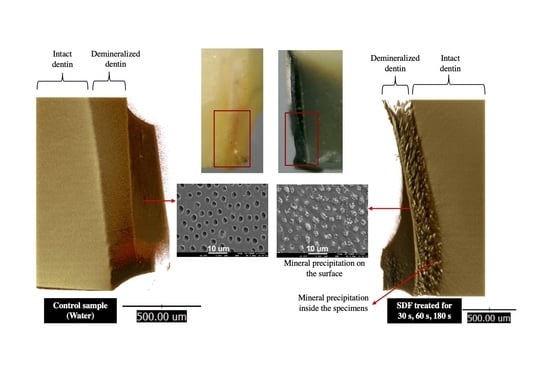
2.1. Specimen Preparation
- Group 1 (control): 25 μL of deionized water was applied;
- Group 2 (30 s): 25 μL of SDF was applied and left for 30 s;
- Group 3 (60 s): 25 μL of SDF was applied and left for 60 s;
- Group 4 (180 s): 25 μL of SDF was applied and left for 180 s.
2.2. Assessment of Mineral Apatite Precipitation Using FTIR-ATR
2.3. Assessment of Surface Mineral Precipitation Using SEM-EDX
2.4. Assessment of the Degree of Mineral Precipitation (Mineral Density) Using Synchrotron Radiation X-ray Tomographic Microscopy (SRXTM)
2.5. Statistical Analysis
3. Results
3.1. Assessment of Mineral Precipitation Using FTIR-ATR
3.2. Assessment of Surface Mineral Precipitation Using SEM-EDX
3.3. Assessment of the Degree of Mineral Precipitation (Mineral Density) Using Synchrotron Radiation X-ray Tomographic Microscopy (SRXTM)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD Oral Disorders Collaborators. Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J. Dent. Res. 2020, 99, 362–373. [Google Scholar] [CrossRef] [PubMed]
- Schwendicke, F. Less Is More? The Long-Term Health and Cost Consequences Resulting from Minimal Invasive Caries Management. Dent. Clin. N. Am. 2019, 63, 737–749. [Google Scholar] [CrossRef]
- Fontana, M. Nonrestorative Management of Cavitated and Noncavitated Caries Lesions. Dent. Clin. N. Am. 2019, 63, 695–703. [Google Scholar] [CrossRef]
- Urquhart, O.; Tampi, M.P.; Pilcher, L.; Slayton, R.L.; Araujo, M.W.B.; Fontana, M.; Guzman-Armstrong, S.; Nascimento, M.M.; Novy, B.B.; Tinanoff, N.; et al. Nonrestorative Treatments for Caries: Systematic Review and Network Meta-analysis. J. Dent. Res. 2019, 98, 14–26. [Google Scholar] [CrossRef]
- Horst, J.A.; Heima, M. Prevention of Dental Caries by Silver Diamine Fluoride. Compend. Contin. Educ. Dent. 2019, 40, 158–163, quiz 164. [Google Scholar]
- Chibinski, A.C.; Wambier, L.M.; Feltrin, J.; Loguercio, A.D.; Wambier, D.S.; Reis, A. Silver Diamine Fluoride Has Efficacy in Controlling Caries Progression in Primary Teeth: A Systematic Review and Meta-Analysis. Caries Res. 2017, 51, 527–541. [Google Scholar] [CrossRef]
- Zhao, I.S.; Gao, S.S.; Hiraishi, N.; Burrow, M.F.; Duangthip, D.; Mei, M.L.; Lo, E.C.; Chu, C.H. Mechanisms of silver diamine fluoride on arresting caries: A literature review. Int. Dent. J. 2018, 68, 67–76. [Google Scholar] [CrossRef] [Green Version]
- Mei, M.L.; Ito, L.; Cao, Y.; Li, Q.L.; Lo, E.C.; Chu, C.H. Inhibitory effect of silver diamine fluoride on dentine demineralisation and collagen degradation. J. Dent. 2013, 41, 809–817. [Google Scholar] [CrossRef]
- Mei, M.L.; Lo, E.C.M.; Chu, C.H. Arresting Dentine Caries with Silver Diamine Fluoride: What’s Behind It? J. Dent. Res. 2018, 97, 751–758. [Google Scholar] [CrossRef]
- Sayed, M.; Matsui, N.; Hiraishi, N.; Inoue, G.; Nikaido, T.; Burrow, M.F.; Tagami, J. Evaluation of discoloration of sound/demineralized root dentin with silver diamine fluoride: In-vitro study. Dent. Mater. J. 2019, 38, 143–149. [Google Scholar] [CrossRef] [Green Version]
- Mei, M.L.; Nudelman, F.; Marzec, B.; Walker, J.M.; Lo, E.C.M.; Walls, A.W.; Chu, C.H. Formation of fluorohydroxyapatite with silver diamine fluoride. J. Dent. Res. 2017, 96, 1122–1128. [Google Scholar] [CrossRef] [Green Version]
- Hu, S.; Meyer, B.; Duggal, M. A silver renaissance in dentistry. Eur. Arch. Paediatr. Dent. 2018, 19, 221–227. [Google Scholar] [CrossRef]
- Firouzmandi, M.; Vasei, F.; Giti, R.; Sadeghi, H. Effect of silver diamine fluoride and proanthocyanidin on resistance of carious dentin to acid challenges. PLoS ONE 2020, 15, e0238590. [Google Scholar] [CrossRef]
- American Academy of Pediatric Dentistry. Guideline on Management of Dental Patients with Special Health Care Needs. Pediatr Dent. 2016, 38, 171–176. [Google Scholar]
- Crystal, Y.O.; Niederman, R. Silver Diamine Fluoride Treatment Considerations in Children’s Caries Management. Pediatr Dent. 2016, 38, 466–471. [Google Scholar]
- Horst, J.A.; Ellenikiotis, H.; Milgrom, P.L. UCSF Protocol for Caries Arrest Using Silver Diamine Fluoride: Rationale, Indications and Consent. J. Calif Dent. Assoc. 2016, 44, 16–28. [Google Scholar]
- Seifo, N.; Robertson, M.; MacLean, J.; Blain, K.; Grosse, S.; Milne, R.; Seeballuck, C.; Innes, N. The use of silver diamine fluoride (SDF) in dental practice. Br. Dent. J. 2020, 228, 75–81. [Google Scholar] [CrossRef]
- Chen, Z.; Cao, S.; Wang, H.; Li, Y.; Kishen, A.; Deng, X.; Yang, X.; Wang, Y.; Cong, C.; Wang, H.; et al. Biomimetic remineralization of demineralized dentine using scaffold of CMC/ACP nanocomplexes in an in vitro tooth model of deep caries. PLoS ONE 2015, 10, e0116553. [Google Scholar] [CrossRef] [PubMed]
- British Standard. BS ISO 23317:2014. Implants for Surgery. In Vitro Evaluation for Apatite-Forming Ability of Implant Materials; BSI: British, UK, 2014. [Google Scholar]
- Kokubo, T.; Yamaguchi, S. Simulated body fluid and the novel bioactive materials derived from it. J. Biomed. Mater. Res. A 2019, 107, 968–977. [Google Scholar] [CrossRef]
- Liu, Y.; Yao, X.; Liu, Y.W.; Wang, Y. A Fourier transform infrared spectroscopy analysis of carious dentin from transparent zone to normal zone. Caries Res. 2014, 48, 320–329. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Wang, Z.; Jiang, T.; Wang, Y. Biomimetic regulation of dentine remineralization by amino acid in vitro. Dent. Mater. 2019, 35, 298–309. [Google Scholar] [CrossRef]
- Lopes, C.d.C.A.; Limirio, P.H.J.O.; Novais, V.R.; Dechichi, P. Fourier transform infrared spectroscopy (FTIR) application chemical characterization of enamel, dentin and bone. Appl. Spectrosc. Rev. 2018, 53, 747–769. [Google Scholar] [CrossRef]
- Yin, I.X.; Yu, O.Y.; Zhao, I.S.; Mei, M.L.; Li, Q.L.; Tang, J.; Lo, E.C.M.; Chu, C.H. Inhibition of dentine caries using fluoride solution with silver nanoparticles: An in vitro study. J. Dent. 2020, 103, 103512. [Google Scholar] [CrossRef] [PubMed]
- Berzina-Cimdina, L.; Borodajenko, N. Research of Calcium Phosphates Using Fourier Transform Infrared Spectroscopy. In Infrared Spectroscopy—Materials Science, Engineering and Technology; InTech: Rijeka, Croatian, 2012; pp. 123–148. [Google Scholar]
- Vidal Bde, C.; Mello, M.L. Collagen type I amide I band infrared spectroscopy. Micron 2011, 42, 283–289. [Google Scholar] [CrossRef]
- Ghimire, H.; Venkataramani, M.; Bian, Z.; Liu, Y.; Perera, A.G.U. ATR-FTIR spectral discrimination between normal and tumorous mouse models of lymphoma and melanoma from serum samples. Sci. Rep. 2017, 7, 16993. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riaz, T.; Zeeshan, R.; Zarif, F.; Ilyas, K.; Muhammad, N.; Safi, S.Z.; Rahim, A.; Rizvi, S.A.A.; Rehman, I.U. FTIR analysis of natural and synthetic collagen. Appl. Spectrosc. Rev. 2018, 53, 703–746. [Google Scholar] [CrossRef]
- Mei, M.L.; Ito, L.; Cao, Y.; Lo, E.C.; Li, Q.L.; Chu, C.H. An ex vivo study of arrested primary teeth caries with silver diamine fluoride therapy. J. Dent. 2014, 42, 395–402. [Google Scholar] [CrossRef] [Green Version]
- Vlassenbroeck, J.; Masschaele, B.; Cnudde, V.; Dierick, M.; Pieters, K.; Van Hoorebeke, L.; Jacobs, P. Octopus 8: A High Performance Tomographic Reconstruction Package for X-ray Tube and Synchrotron micro-CT. In Advances in X-ray Tomography for Geomaterials; John Wiley & Sons: Hoboken, NJ, USA, 2006; pp. 167–173. [Google Scholar]
- Limaye, A. Drishti: A volume exploration and presentation tool. In Developments in X-Ray Tomography VIII; International Society for Optics and Photonics: San Diego, CA, USA, 2012; p. 85060X. [Google Scholar] [CrossRef] [Green Version]
- Panpisut, P.; Suppapatpong, T.; Rattanapan, A.; Wongwarawut, P. Monomer conversion, biaxial flexural strength, apatite forming ability of experimental dual-cured and self-adhesive dental composites containing calcium phosphate and nisin. Dent. Mater. J. 2021, 40, 399–406. [Google Scholar] [CrossRef]
- Kokubo, T.; Takadama, H. How useful is SBF in predicting in vivo bone bioactivity? Biomaterials 2006, 27, 2907–2915. [Google Scholar] [CrossRef] [PubMed]
- Chu, C.H.; Mei, L.; Seneviratne, C.J.; Lo, E.C. Effects of silver diamine fluoride on dentine carious lesions induced by Streptococcus mutans and Actinomyces naeslundii biofilms. Int. J. Paediatr. Dent. 2012, 22, 2–10. [Google Scholar] [CrossRef]
- Mei, M.L.; Li, Q.L.; Chu, C.H.; Yiu, C.K.; Lo, E.C. The inhibitory effects of silver diamine fluoride at different concentrations on matrix metalloproteinases. Dent. Mater. 2012, 28, 903–908. [Google Scholar] [CrossRef]
- Aoba, T. Solubility properties of human tooth mineral and pathogenesis of dental caries. Oral Dis. 2004, 10, 249–257. [Google Scholar] [CrossRef] [PubMed]
- Cai, J.; Burrow, M.F.; Manton, D.J.; Tsuda, Y.; Sobh, E.G.; Palamara, J.E.A. Effects of silver diamine fluoride/potassium iodide on artificial root caries lesions with adjunctive application of proanthocyanidin. Acta Biomater. 2019, 88, 491–502. [Google Scholar] [CrossRef]
- Li, Y.; Liu, Y.; Psoter, W.J.; Nguyen, O.M.; Bromage, T.G.; Walters, M.A.; Hu, B.; Rabieh, S.; Kumararaja, F.C. Assessment of the Silver Penetration and Distribution in Carious Lesions of Deciduous Teeth Treated with Silver Diamine Fluoride. Caries Res. 2019, 53, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Sayed, M.; Matsui, N.; Uo, M.; Nikaido, T.; Oikawa, M.; Burrow, M.F.; Tagami, J. Morphological and elemental analysis of silver penetration into sound/demineralized dentin after SDF application. Dent. Mater. 2019, 35, 1718–1727. [Google Scholar] [CrossRef] [PubMed]
- Vogel, G.L. Oral fluoride reservoirs and the prevention of dental caries. Monogr. Oral Sci. 2011, 22, 146–157. [Google Scholar] [CrossRef]
- Lou, Y.L.; Botelho, M.G.; Darvell, B.W. Reaction of silver diamine [corrected] fluoride with hydroxyapatite and protein. J. Dent. 2011, 39, 612–618. [Google Scholar] [CrossRef]
- Punyanirun, K.; Yospiboonwong, T.; Kunapinun, T.; Thanyasrisung, P.; Trairatvorakul, C. Silver diamine fluoride remineralized artificial incipient caries in permanent teeth after bacterial pH-cycling in-vitro. J. Dent. 2018, 69, 55–59. [Google Scholar] [CrossRef]
- Zhao, I.S.; Mei, M.L.; Li, Q.L.; Lo, E.C.M.; Chu, C.H. Arresting simulated dentine caries with adjunctive application of silver nitrate solution and sodium fluoride varnish: An in vitro study. Int. Dent. J. 2017, 67, 206–214. [Google Scholar] [CrossRef] [Green Version]
- Zhao, I.S.; Mei, M.L.; Burrow, M.F.; Lo, E.C.; Chu, C.H. Effect of silver diamine fluoride and potassium iodide treatment on secondary caries prevention and tooth discolouration in cervical glass ionomer cement restoration. Int. J. Mol. Sci. 2017, 18, 340. [Google Scholar] [CrossRef] [Green Version]
- Romero, M.; Lippert, F. Indirect caries-preventive effect of silver diamine fluoride on adjacent dental substrate: A single-section demineralization study. Eur. J. Oral Sci. 2021, 129, e12751. [Google Scholar] [CrossRef]
- Kim, S.; Nassar, M.; Tamura, Y.; Hiraishi, N.; Jamleh, A.; Nikaido, T.; Tagami, J. The effect of reduced glutathione on the toxicity of silver diamine fluoride in rat pulpal cells. J. Appl. Oral Sci. 2021, 29, e20200859. [Google Scholar] [CrossRef]
- Marrelli, M.; Codispoti, B.; Shelton, R.M.; Scheven, B.A.; Cooper, P.R.; Tatullo, M.; Paduano, F. Dental Pulp Stem Cell Mechanoresponsiveness: Effects of Mechanical Stimuli on Dental Pulp Stem Cell Behavior. Front. Physiol. 2018, 9, 1685. [Google Scholar] [CrossRef]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Groups/ Time | 0 h Median (Min,Max) | 24 h Median (Min,Max) | 1 Week Median (Min,Max) | 2 Weeks Median (Min,Max) | Friedman Statistics | p Values |
|---|---|---|---|---|---|---|
| Control (Water) | 0.134 (0.070,0.453) | 0.133 (0.07,0.35) A | 0.123 (0.07,0.38) B,C | 0.117 (0.07,0.38) D,E | 11.34 | >0.05 |
| SDF 30 s | 0.282 (0.080,0.722) | 0.244 (0.093,0.928) A | 0.318 (0.101,0.949) B | 0.308 (0.104,0.935) D | 5.215 | >0.05 |
| SDF 60 s | 0.116 a (0.068,0.613) | 0.173 (0.040,0.593) | 0.148 (0.084,0.804) | 0.206 a (0.088,0.957) | 0.48 | a 0.0143 |
| SDF 180 s | 0.180 a,b (0.048,0.421) | 0.202 c,d (0.061,0.701) | 0.316 a,c (0.093,0.832) C | 0.250 b,d (0.126,0.895) E | 20.54 | a 0.0029 b 0.0085 c 0.0085 d 0.0234 |
| Kruskal–Wallis statistics | 2.667 | 8.021 | 12.80 | 16.12 | ||
| p values | >0.05 | A 0.0461 | B 0.168 C 0.0083 | D 0.0023 E 0.0046 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Srisomboon, S.; Kettratad, M.; Pakawanit, P.; Rojviriya, C.; Phantumvanit, P.; Panpisut, P. Effects of Different Application Times of Silver Diamine Fluoride on Mineral Precipitation in Demineralized Dentin. Dent. J. 2021, 9, 70. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9060070
Srisomboon S, Kettratad M, Pakawanit P, Rojviriya C, Phantumvanit P, Panpisut P. Effects of Different Application Times of Silver Diamine Fluoride on Mineral Precipitation in Demineralized Dentin. Dentistry Journal. 2021; 9(6):70. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9060070
Chicago/Turabian StyleSrisomboon, Surapong, Matana Kettratad, Phakkhananan Pakawanit, Catleya Rojviriya, Prathip Phantumvanit, and Piyaphong Panpisut. 2021. "Effects of Different Application Times of Silver Diamine Fluoride on Mineral Precipitation in Demineralized Dentin" Dentistry Journal 9, no. 6: 70. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9060070