
Influence of Anatomical Parameters on the Dimensions of the Subantral Space and Sinus Mucosa Thickening after Sinus Floor Elevation. A Retrospective Cone Beam Computed Tomography Study

 and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Surgical Procedures
2.3. Biomaterials Used
2.4. CBCT Imaging Analyses
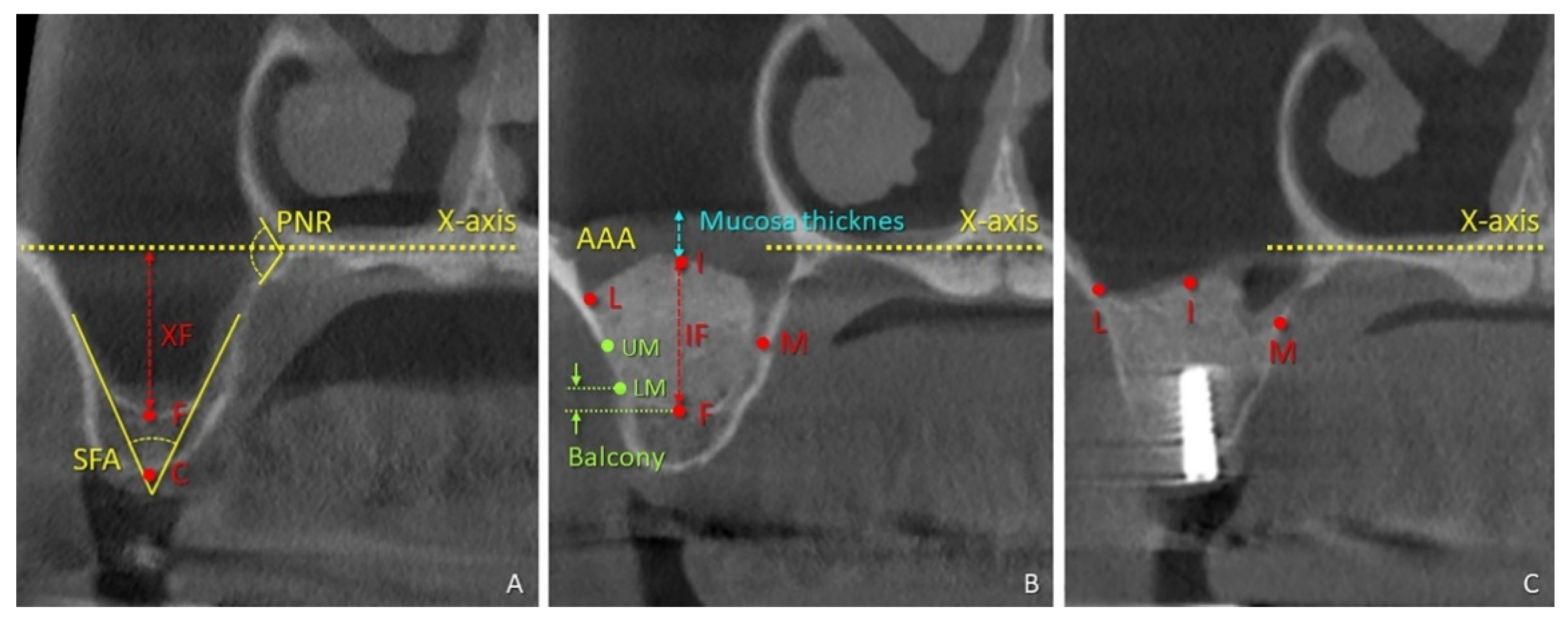
2.5. Radiographic Evaluations
- (i)
- at time 0 (t-0), the floor of the nose (X-axis), the center of the bony crest (C), the base of the sinus floor (F), the alveolar-antral artery (AAA), and the palatal nasal recess (PNR).
- (ii)
- at time 1 week (t-1w), the upper (UM) and lower margin (LM) of the antrostomy, the uppermost extension of the hard tissue within the elevated space at the medial, intermediate, and lateral aspects.
- (iii)
- at time 9 months (t-9m), the uppermost extension of the hard tissue within the elevated space at the medial (M), intermediate (I), and lateral (L) aspects.
2.6. Data Analysis
3. Results
3.1. Anatomical Parameters and Dimensional Changes Overtime in the Subantral Space
3.2. Correlations with the Height Gain
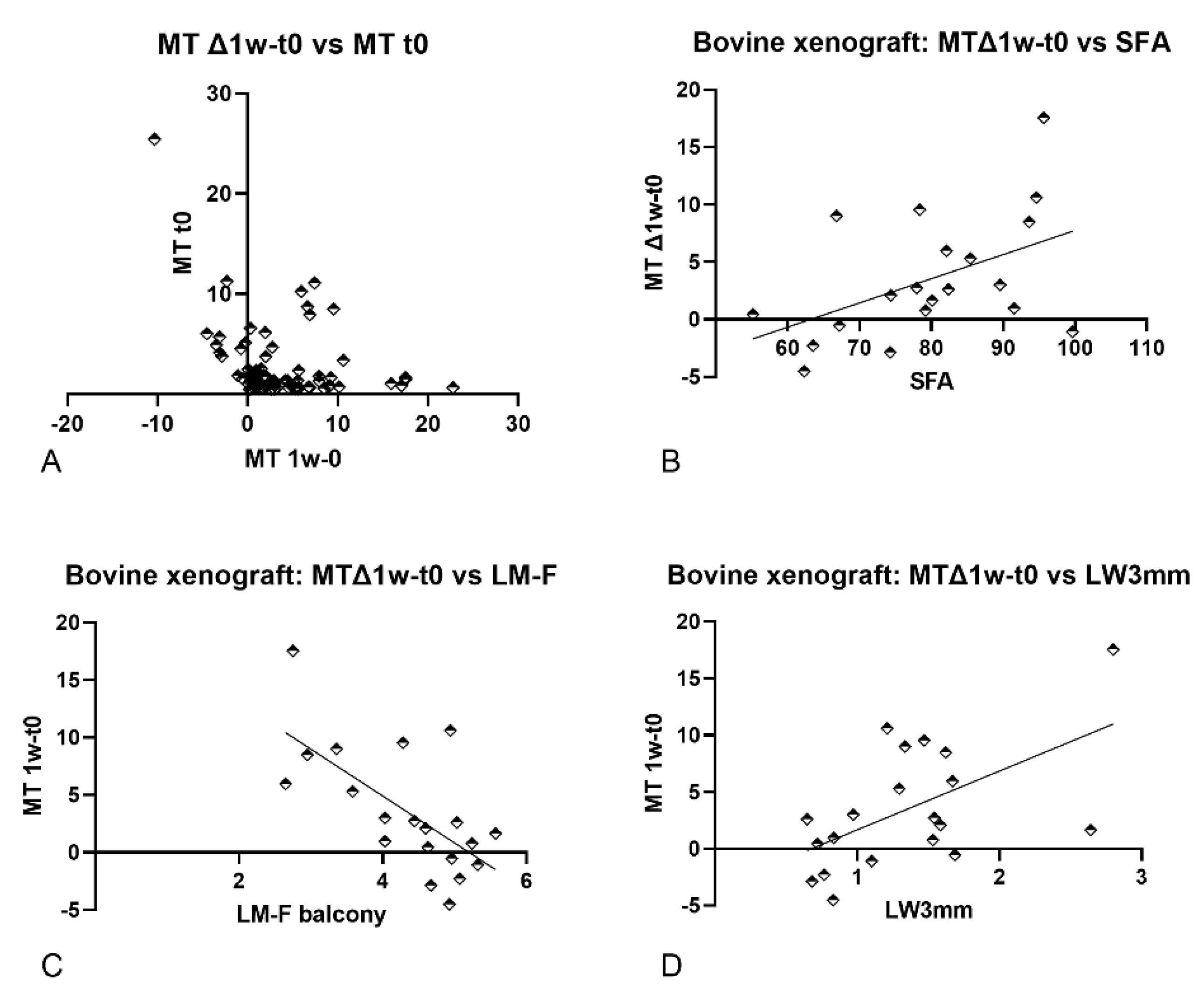
3.3. Correlations with the Mucosa Thickness after One Week of Healing (MT)
4. Discussion
4.1. Anatomical Parameters and Dimensional Changes Overtime in the Subantral Space
4.2. Correlations with the Height Gain
4.3. Correlations with the Mucosa Thickness Changes after One Week of Healing (MT Δ1w–t0)
4.4. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Del Fabbro, M.; Wallace, S.S.; Testori, T. Long-Term Implant Survival in the Grafted Maxillary Sinus: A Systematic Review. Int. J. Periodontics Restor. Dent. 2013, 33, 773–783. [Google Scholar] [CrossRef] [PubMed]
- Kawakami, S.; Botticelli, D.; Nakajima, Y.; Sakuma, S.; Baba, S. Anatomical analyses for maxillary sinus floor augmentation with a lateral approach: A cone beam computed tomography study. Ann. Anat. Anat. Anz. 2019, 226, 29–34. [Google Scholar] [CrossRef]
- Lozano-Carrascal, N.; Salomó-Coll, O.; Gehrke, S.A.; Guirado, J.L.C.; Hernández-Alfaro, F.; Gargallo-Albiol, J. Radiological evaluation of maxillary sinus anatomy: A cross-sectional study of 300 patients. Ann. Anat. Anat. Anz. 2017, 214, 1–8. [Google Scholar] [CrossRef]
- Kawai, T.; Tanaka, R.; Yeung, A.W.K.; Von Arx, T.; Bornstein, M.M. Frequency and type of incidentally detected radiodensities in the maxillary sinus: A retrospective analysis using cone beam computed tomography (CBCT). Clin. Oral Investig. 2018, 23, 1091–1099. [Google Scholar] [CrossRef] [PubMed]
- Yeung, A.W.K.; Tanaka, R.; Khong, P.L.; von Arx, T.; Bornstein, M.M. Frequency, location, and association with dental pathol-ogy of mucous retention cysts in the maxillary sinus. A radiographic study using cone beam computed tomography (CBCT). Clin. Oral Investig. 2018, 22, 1175–1183. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Seiffert, C.; Maestre-Ferrín, L.; Fodich, I.; Jacobs, R.; Buser, D.; Von Arx, T. An Analysis of Frequency, Morphology, and Locations of Maxillary Sinus Septa Using Cone Beam Computed Tomography. Int. J. Oral Maxillofac. Implant. 2016, 31, 280–287. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maestre-Ferrin, L.; Galan-Gil, S.; Rubio-Serrano, M.; Penarrocha-Diago, M.; Penarrocha-Oltra, D. Maxillary sinus septa: A systematic review. Med. Oral Patol. Oral Cir. Bucal 2010, 15, e383–e386. [Google Scholar] [CrossRef] [Green Version]
- Dandekeri, S.S.; Hegde, C.; Kavassery, P.; Sowmya, M.; Shetty, B. CBCT study of morphologic variations of maxillary sinus septa in relevance to sinus augmentation procedures. Ann. Maxillofac. Surg. 2020, 10, 51–56. [Google Scholar] [CrossRef]
- Wagner, F.; Dvorak, G.; Nemec, S.; Pietschmann, P.; Traxler, H.; Schicho, K.; Seemann, R. Morphometric analysis of sinus depth in the posterior maxilla and proposal of a novel classification. Sci. Rep. 2017, 7, srep45397. [Google Scholar] [CrossRef]
- Kawakami, S.; Lang, N.P.; Iida, T.; Ferri, M.; Alccayhuaman, K.A.A.; Botticelli, D. Influence of the position of the antrostomy in sinus floor elevation assessed with cone-beam computed tomography: A randomized clinical trial. J. Investig. Clin. Dent. 2018, 9, e12362. [Google Scholar] [CrossRef]
- Kawakami, S.; Lang, N.; Ferri, M.; Alccayhuaman, K.; Botticelli, D. Influence of the Height of the Antrostomy in Sinus Floor Elevation Assessed by Cone Beam Computed Tomography: A Randomized Clinical Trial. Int. J. Oral Maxillofac. Implant. 2019, 34, 223–232. [Google Scholar] [CrossRef]
- Monje, A.; Urban, I.A.; Miron, R.J.; Caballe-Serrano, J.; Buser, D.; Wang, H.-L. Morphologic Patterns of the Atrophic Posterior Maxilla and Clinical Implications for Bone Regenerative Therapy. Int. J. Periodontics Restor. Dent. 2017, 37, e279–e289. [Google Scholar] [CrossRef] [Green Version]
- Imai, H.; Lang, N.; Ferri, M.; Hirota, A.; Alccayhuaman, K. Tomographic Assessment on the Influence of the Use of a Collagen Membrane on Dimensional Variations to Protect the Antrostomy After Maxillary Sinus Floor Augmentation: A Randomized Clinical Trial. Int. J. Oral Maxillofac. Implant. 2020, 35, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Hirota, A.; Lang, N.P.; Ferri, M.; Mesa, N.F.; Alccayhuaman, K.A.A.; Botticelli, D. Tomographic evaluation of the influence of the placement of a collagen membrane subjacent to the sinus mucosa during maxillary sinus floor augmentation: A randomized clinical trial. Int. J. Implant. Dent. 2019, 5, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.-H.; Han, W.-J.; Park, J.-T. Three-dimensional CBCT based evaluation of the inferior part of the maxillary sinus: Retrospective Study. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef]
- Baldini, N.; D’Elia, C.; Bianco, A.; Goracci, C.; Sanctis, M.; Ferrari, M. Lateral approach for sinus floor elevation: Large versus small bone window—A split-mouth randomized clinical trial. Clin. Oral Implant. Res. 2016, 28, 974–981. [Google Scholar] [CrossRef]
- Lu, W.; Xu, J.; Wang, H.-M.; He, F.-M.; Nishimoto, M.; Kan, J.K.; Rungcharassaeng, K.; Roe, P.; Lozada, J.L. Influence of Lateral Windows with Decreased Vertical Height Following Maxillary Sinus Floor Augmentation: A 1-year Clinical and Radiographic Study. Int. J. Oral Maxillofac. Implant. 2018, 33, 661–670. [Google Scholar] [CrossRef] [Green Version]
- Mardinger, O.; Abba, M.; Hirshberg, A.; Schwartz-Arad, D. Prevalence, diameter and course of the maxillary intraosseous vascular canal with relation to sinus augmentation procedure: A radiographic study. Int. J. Oral Maxillofac. Surg. 2007, 36, 735–738. [Google Scholar] [CrossRef]
- Kiliç, S.; Güngörmüş, M. Cone Beam Computed Tomography Assessment of Maxillary Sinus Floor Augmentation Using Beta-Tricalcium Phosphate Alone or in Combination with Platelet-Rich Plasma: A Randomized Clinical Trial. Int. J. Oral Maxillofac. Implant. 2016, 31, 1367–1375. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nosaka, Y.; Nosaka, H.; Arai, Y. Complications of postoperative swelling of the maxillary sinus membrane after sinus floor augmentation. J. Oral Sci. Rehabil. 2015, 1, 26–33. [Google Scholar]
- Temmerman, A.; Van Dessel, J.; Cortellini, S.; Jacobs, R.; Teughels, W.; Quirynen, M. Volumetric changes of grafted volumes and the Schneiderian membrane after transcrestal and lateral sinus floor elevation procedures: A clinical, pilot study. J. Clin. Periodontol. 2017, 44, 660–671. [Google Scholar] [CrossRef] [PubMed]
- Makary, C.; Rebaudi, A.; Menhall, A.; Naaman, N. Changes in Sinus Membrane Thickness After Lateral Sinus Floor Elevation: A Radiographic Study. Int. J. Oral Maxillofac. Implant. 2016, 31, 331–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, H.-L.; Monje, A.; Suarez, F.; Benavides, E.; Wang, H.-L. Palatonasal Recess on Medial Wall of the Maxillary Sinus and Clinical Implications for Sinus Augmentation via Lateral Window Approach. J. Periodontol. 2013, 84, 1087–1093. [Google Scholar] [CrossRef] [Green Version]
- Cho, S.C.; Wallace, S.S.; Froum, S.J.; Tarnow, D.P. Influence of anatomy on Schneiderian membrane perforations during sinus elevation surgery: Three-dimensional analysis. Pract. Proced. Aesthetic Dent. PPAD 2001, 13, 160–163. [Google Scholar]
- Testori, T.; Yu, S.-H.; Tavelli, L.; Wang, H.-L. Perforation Risk Assessment in Maxillary Sinus Augmentation with Lateral Wall Technique. Int. J. Periodontics Restor. Dent. 2020, 40, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Pizzini, A.; Basma, H.S.; Li, P.; Geurs, N.C.; Abou-Arraj, R.V. The impact of anatomic, patient and surgical factors on membrane perforation during lateral wall sinus floor elevation. Clin. Oral Implant. Res. 2021, 32, 274–284. [Google Scholar] [CrossRef]
- Basma, H.; Saleh, I.; Abou-Arraj, R.; Li, P.; Benavides, E.; Wang, H.-L.; Chang, H.-L. Association between lateral wall thickness and sinus membrane perforation during lateral sinus elevation: A retrospective study. Int. J. Oral Implant. 2021, 14, 77–85. [Google Scholar]
- Sakuma, S.; Ferri, M.; Imai, H.; Mesa, N.F.; Victorio, D.J.B.; Alccayhuaman, K.A.A.; Botticelli, D. Involvement of the maxillary sinus ostium (MSO) in the edematous processes after sinus floor augmentation: A cone-beam computed tomographic study. Int. J. Implant. Dent. 2020, 6, 1–9. [Google Scholar] [CrossRef]
- Guo, Z.Z.; Liu, Y.; Qin, L.; Song, Y.L.; Xie, C.; Li, D.H. Longitudinal response of membrane thickness and ostium patency follow-ing sinus floor elevation: A prospective cohort study. Clin. Oral Implant. Res. 2016, 27, 724–729. [Google Scholar] [CrossRef]
- Danesh-Sani, S.A.; Engebretson, S.P.; Janal, M.N. Histomorphometric results of different grafting materials and effect of healing time on bone maturation after sinus floor augmentation: A systematic review and meta-analysis. J. Periodontal Res. 2016, 52, 301–312. [Google Scholar] [CrossRef]
- Barone, A.; Ricci, M.; Grassi, R.F.; Nannmark, U.; Quaranta, A.; Covani, U.; Grassi, F.R. A 6-month histological analysis on maxillary sinus augmentation with and without use of collagen membranes over the osteotomy window: Randomized clinical trial. Clin. Oral Implant. Res. 2011, 24, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Dancey, C.P.; Reidy, J. Statistics without Maths for Psychology; Pearson/Prentice Hall: Harlow, UK, 2007. [Google Scholar]
- Akoglu, H. User’s guide to correlation coefficients. Turk. J. Emerg. Medicine 2018, 18, 91–93. [Google Scholar] [CrossRef]
- Geminiani, A.; Papadimitriou, D.E.V.; Ercoli, C. Maxillary sinus augmentation with a sonic handpiece for the osteotomy of the lateral window: A clinical report. J. Prosthet. Dent. 2011, 106, 279–283. [Google Scholar] [CrossRef]
- Geminiani, A.; Weitz, D.S.; Ercoli, C.; Feng, C.; Caton, J.G.; Papadimitriou, D.E. A comparative study of the incidence of Schnei-derian membrane perforations during maxillary sinus augmentation with a sonic oscillating handpiece versus a conven-tional turbine handpiece. Clin. Implant Dent. Relat. Res. 2015, 17, 327–334. [Google Scholar] [CrossRef] [PubMed]
- Agabiti, I.; Botticelli, D. Two-Stage Ridge Split at Narrow Alveolar Mandibular Bone Ridges. J. Oral Maxillofac. Surg. 2017, 75, 2115.e1–2115.e12. [Google Scholar] [CrossRef]
- Agabiti, I.; Botticelli, D. Transcrestal sinus floor elevation performed twice with collagen sponges and using a sonic instrument. J. Oral Sci. Rehabil. 2016, 2, 40–47. [Google Scholar]
- Agabiti, I.; Alccayhuaman, K.A.A.; Nakajima, Y.; Botticelli, D. An enigmatic soft tissue creeping phenomenon: The spontaneous peri-implant mucosa margin and papilla growth. A retrospective clinical study. Clin. Exp. Dent. Res. 2020. [Google Scholar] [CrossRef]
- Masuda, K.; Silva, E.; Botticelli, D.; Alccayhuaman, K.; Xavier, S. Antrostomy Preparation for Maxillary Sinus Floor Augmentation Using Drills or a Sonic Instrument: A Microcomputed Tomography and Histomorphometric Study in Rabbits. Int. J. Oral Maxillofac. Implant. 2019, 34, 819–827. [Google Scholar] [CrossRef]
- Ferri, M.; Lang, N.P.; Alfonso, E.E.A.; Quintero, I.D.B.; Burgos, E.M.; Botticelli, D. Use of sonic instruments for implant biopsy retrieval. Clin. Oral Implant. Res. 2014, 26, 1237–1243. [Google Scholar] [CrossRef]
- Cesaretti, G.; Lang, N.P.; Salata, L.A.; Schweikert, M.T.; Hernandez, M.E.G.; Botticelli, D. Sub-crestal positioning of implants results in higher bony crest resorption: An experimental study in dogs. Clin. Oral Implant. Res. 2015, 26, 1355–1360. [Google Scholar] [CrossRef] [PubMed]
- Viganò, P.; Botticelli, D.; Salata, L.A.; Schweikert, M.T.; Velez, J.U.; Lang, N.P. Healing at implant sites prepared conventionally or by means of Sonosurgery®. An experimental study in dogs. Clin. Oral Implant. Res. 2014, 26, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Pommer, B.; Dvorak, G.; Jesch, P.; Palmer, R.M.; Watzek, G.; Gahleitner, A. Effect of Maxillary Sinus Floor Augmentation on Sinus Membrane Thickness in Computed Tomography. J. Periodontol. 2012, 83, 551–556. [Google Scholar] [CrossRef]
- Scala, A.; Botticelli, D.; Faeda, R.S.; Rangel, I.G.; De Oliveira, J.A.; Lang, N.P. Lack of influence of the Schneiderian membrane in forming new bone apical to implants simultaneously installed with sinus floor elevation: An experimental study in monkeys. Clin. Oral Implant. Res. 2011, 23, 175–181. [Google Scholar] [CrossRef]
- Scala, A.; Botticelli, D.; Rangel, I.G.; De Oliveira, J.A.; Okamoto, R.; Lang, N.P. Early healing after elevation of the maxillary sinus floor applying a lateral access: A histological study in monkeys. Clin. Oral Implant. Res. 2010, 21, 1320–1326. [Google Scholar] [CrossRef] [PubMed]
- Scala, A.; Lang, N.P.; Velez, J.U.; Favero, R.; Bengazi, F.; Botticelli, D. Effects of a collagen membrane positioned between augmentation material and the sinus mucosa in the elevation of the maxillary sinus floor. An experimental study in sheep. Clin. Oral Implant. Res. 2016, 27, 1454–1461. [Google Scholar] [CrossRef]
- Iida, T.; Neto, E.C.M.; Botticelli, D.; Alccayhuaman, K.A.A.; Lang, N.P.; Xavier, S.P. Influence of a collagen membrane positioned subjacent the sinus mucosa following the elevation of the maxillary sinus. A histomorphometric study in rabbits. Clin. Oral Implant. Res. 2017, 28, 1567–1576. [Google Scholar] [CrossRef]
- Favero, V.; Lang, N.P.; Canullo, L.; Velez, J.U.; Bengazi, F.; Botticelli, D. Sinus floor elevation outcomes following perforation of the Schneiderian membrane. An experimental study in sheep. Clin. Oral Implant. Res. 2015, 27, 233–240. [Google Scholar] [CrossRef] [PubMed]
- Caneva, M.; Lang, N.P.; Rangel, I.J.G.; Ferreira, S.; Caneva, M.; De Santis, E.; Botticelli, D. Sinus mucosa elevation using Bio-Oss® or Gingistat® collagen sponge: An experimental study in rabbits. Clin. Oral Implant. Res. 2016, 28, e21–e30. [Google Scholar] [CrossRef] [PubMed]
- Omori, Y.; Silva, E.R.; Botticelli, D.; Alccayhuaman, K.A.A.; Lang, N.P.; Xavier, S.P. Reposition of the bone plate over the antrostomy in maxillary sinus augmentation: A histomorphometric study in rabbits. Clin. Oral Implant. Res. 2018, 29, 821–834. [Google Scholar] [CrossRef] [PubMed]
- Imai, H.; Iezzi, G.; Piattelli, A.; Ferri, M.; Alccayhuaman, K.A.A.; Botticelli, D. Influence of the Dimensions of the Antrostomy on Osseointegration of Mini-implants Placed in the Grafted Region After Sinus Floor Elevation: A Randomized Clinical Trial. Int. J. Oral Maxillofac. Implant. 2020, 35, 591–598. [Google Scholar] [CrossRef] [PubMed]
- Scala, A.; Viña-Almunia, J.; Carda, C.; De Llano, J.J.M.; Soto-Peñaloza, D.; Peñarrocha-Diago, M.; Peñarrocha-Diago, M.; Botticelli, D. Sequential healing of the elevated sinus floor with different size of antrostomy: A histomorphometric study in rabbits. Oral Maxillofac. Surg. 2020, 24, 403–410. [Google Scholar] [CrossRef]
- Dellavia, C.; Speroni, S.; Pellegrini, G.; Gatto, A.; Maiorana, C. A New Method to Evaluate Volumetric Changes in Sinus Augmentation Procedure. Clin. Implant. Dent. Relat. Res. 2013, 16, 684–690. [Google Scholar] [CrossRef] [PubMed]
- Kivovics, M.; Szabó, B.T.; Németh, O.; Iványi, D.; Trimmel, B.; Szmirnova, I.; Orhan, K.; Mijiritsky, E.; Szabó, G.; Dobó-Nagy, C. Comparison between micro-computed tomography and cone-beam computed tomography in the as-sessment of bone quality and a long-term volumetric study of the augmented sinus grafted with an albumin impregnated allograft. J. Clin. Med. 2020, 9, 303. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kato, S.; Botticelli, D.; De Santis, E.; Kanayama, M.; Ferreira, S.; Rangel-Garcia, I., Jr. Sinus mucosa thinning and perforation after sinus augmentation. A histological study in rabbits. Oral Maxillofac. Surg. 2021, 1–9. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| t0 | t1w | t9m | t1w–t0 | t9m–t1w | t9m–t0 | ||
|---|---|---|---|---|---|---|---|
| MT | Sinus mucosa thickness | 2.7 ± 3.7 | 6.4 ± 5.5 | 1.7 ± 2.1 | 3.7 ± 5.3 | −4.7 ± 5.8 | −1.0 ± 4.2 |
| CF | Bone crest height | 3.2 ± 1.3 | |||||
| XF | Distance from x-axis and sinus floor (height of interest) | 9.5 ± 2.7 | |||||
| MF | Height gain from F at the medial aspect | 7.1 ± 2.7 | 6.7 ± 2.4 | −0.4 ± 1.6 | |||
| IF | Height gain from F at the intermediate aspect | 11.1 ± 2.8 | 9.4 ± 3.0 | −1.7 ± 2.0 | |||
| LF | Height gain from F at the lateral aspect | 8.3 ± 2.6 | 7.8 ± 2.3 | −0.5 ± 1.4 | |||
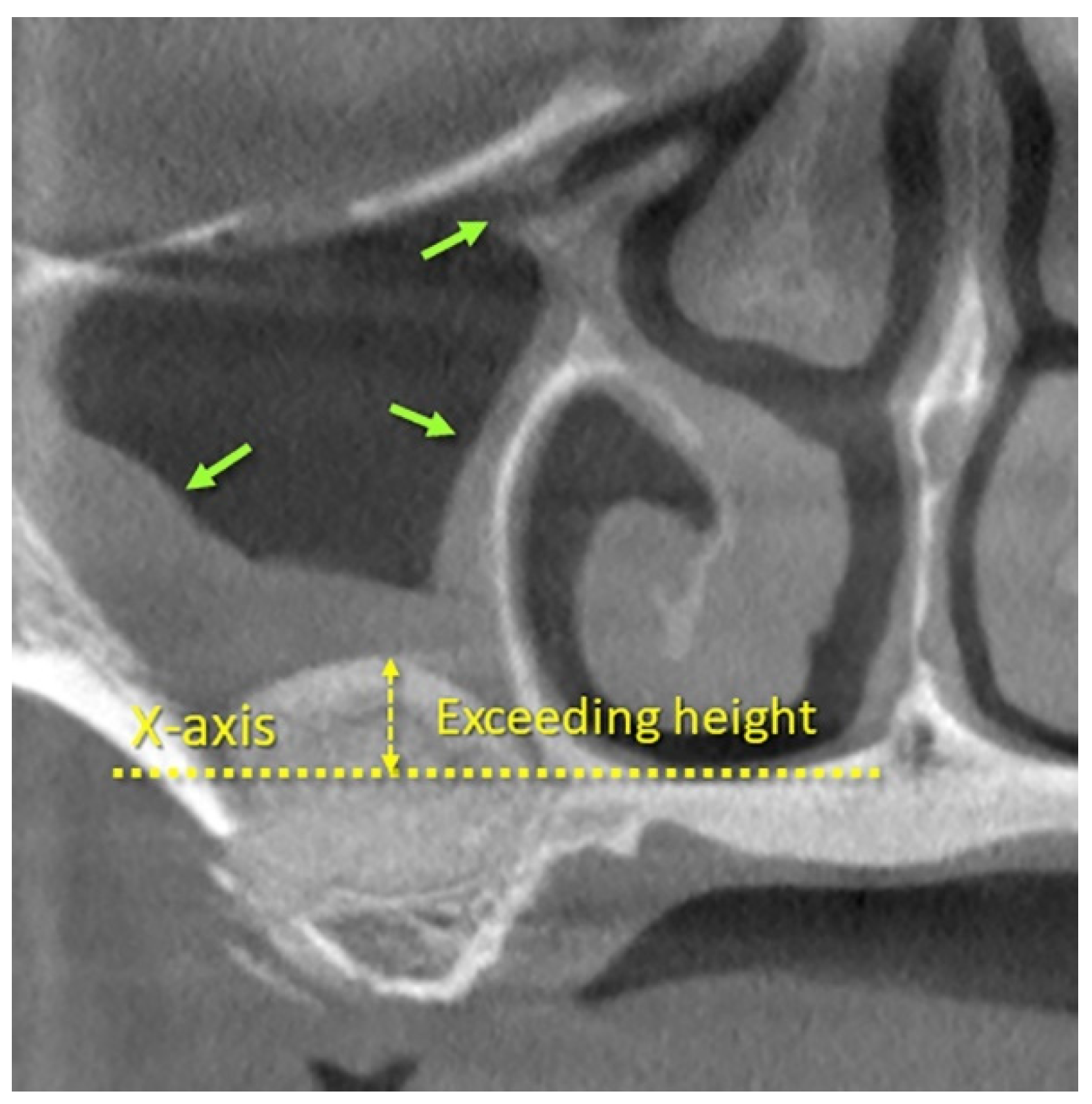
| EH | Exceeding height at X-axis | 1.6 ± 3.5 | −0.1 ± 3.3 | 1.7 ± 2.0 | |||
| X-area | Area enclosed by the sinus bone walls and the X-axis (area of interest) | 99.3 ± 41.6 | |||||
| Area | Area of the elevated space | 100.7 ± 32.0 | 80.6 ± 33.2 | −20.1 ± 21.5 | |||
| XW | Distance between the medial and lateral sinus bone walls on the X-axis | ||||||
| PNR * | Palato-nasal recess angle | 129.1 ± 22.9 | |||||
| SFA * | Sinus floor angle | 80.6 ± 13.3 | |||||
| LW3 | Lateral bone wall thickness at 3 mm from F | 1.3 ± 0.6 | |||||
| LW9 | Lateral bone wall thickness at 9 mm from F | 1.2 ± 0.5 | |||||
| LM-F | Balcony; distance between the lower margin of the antrostomy (LM) and the sinus floor (F) | 3.6 ± 1.3 | |||||
| LM-UM | Antrostomy height | 5.7 ± 1.1 | |||||
| UM-F | Distance between the upper margin of the antrostomy (UM) and the sinus floor (F) | 9.3 ± 1.6 | |||||
| AAA | Alveolar-antral artery distance from C | 16.9 ± 3.1 | |||||
| CF + IF | Available height for implant insertion | 14.3 ± 3.0 | 12.6 ± 3.0 | −1.7 ± 2.0 |
| MF 1w | IF 1w | LF 1w | MF 9m | IF 9m | LF 9m | ||
|---|---|---|---|---|---|---|---|
| XF; Distance from x-axis and sinus floor (height of interest) | r | 0.28 | 0.17 | 0.19 | 0.34 | 0.31 | 0.37 |
| p-value | 0.015 | 0.144 | 0.095 | 0.003 | 0.006 | 0.0008 | |
| 95% CI | 0.049 to 0.47 | −0.06 to 0.38 | −0.04 to 0.40 | 0.12 to 0.52 | 0.09 to 0.50 | 0.16 to 0.56 | |
| XW; Distance between medial and lateral sinus bone walls on X-axis (width of interest) | r | 0.02 | −0.02 | −0.10 | 0.05 | 0.09 | 0.08 |
| p-value | 0.845 | 0.829 | 0.368 | 0.661 | 0.437 | 0.486 | |
| 95% CI | −0.21 to 0.25 | −0.25 to 0.21 | −0.33 to 0.13 | −0.18 to 0.28 | −0.14 to 0.31 | −0.15 to 0.30 | |
| PNR angle; Palato-nasal recess angle | r | −0.19 | −0.11 | 0.0003 | −0.20 | −0.20 | −0.05 |
| p-value | 0.105 | 0.35 | 0.998 | 0.082 | 0.076 | 0.684 | |
| 95% CI | −0.40 to 0.05 | −0.33 to 0.13 | −0.23 to 0.23 | −0.41 to 0.03 | −0.41 to 0.03 | −0.27 to 0.18 | |
| SFA; Sinus floor angle | r | −0.18 | −0.33 | −0.28 | −0.29 | −0.39 | −0.34 |
| p-value | 0.123 | 0.004 | 0.012 | 0.01 | 0.0004 | 0.002 | |
| 95% CI | −0.39 to 0.055 | −0.52 to −0.10 | −0.48 to −0.06 | −0.49 to −0.07 | −0.57 to −0.18 | −0.53 to −0.12 | |
| LM-F: balcony | r | 0.15 | 0.26 | 0.23 | 0.11 | 0.27 | 0.18 |
| p-value | 0.194 | 0.023 | 0.044 | 0.335 | 0.018 | 0.118 | |
| 95% CI | −0.08 to 0.37 | 0.03 to 0.46 | 0.0002 to 0.44 | −0.12 to 0.33 | 0.04 to 0.47 | −0.05 to 0.39 | |
| LM-UM; height of the antrostomy | r | −0.23 | −0.08 | −0.09 | −0.22 | −0.20 | 0.044 |
| p-value | 0.044 | 0.5 | 0.411 | 0.059 | 0.079 | 0.7 | |
| 95% CI | −0.44 to 0.0003 | −0.30 to 0.15 | −0.32 to 0.14 | −0.42 to 0.01 | −0.41 to 0.03 | −0.19 to 0.27 | |
| Both Biomaterials (n = 78) | Porcine Xenograft (n = 58) | Bovine Xenograft (n = 20) | ||
|---|---|---|---|---|
| XF; Distance from x-axis and sinus floor (height of interest) | r | 0.25 | 0.25 | 0.04 |
| p-value | 0.03 | 0.061 | 0.869 | |
| 95% CI | 0.02 to 0.45 | −0.02 to 0.48 | −0.42 to 0.48 | |
| XW; Distance between medial and lateral sinus bone walls on the X-axis (width of interest) | r | 0.23 | 0.21 | 0.17 |
| p-value | 0.045 | 0.109 | 0.484 | |
| 95% CI | −0.0008 to 0.43 | −0.06 to 0.45 | −0.31 to 0.58 | |
| PNR angle; Palato-nasal recess angle | r | −0.19 | −0.096 | −0.18 |
| p-value | 0.094 | 0.4737 | 0.448 | |
| 95% CI | −0.40 to 0.04 | −0.35 to 0.17 | −0.59 to 0.30 | |
| SFA; Sinus floor angle | r | −0.04 | −0.06 | −0.05 |
| p-value | 0.702 | 0.676 | 0.823 | |
| 95% CI | −0.27 to 0.19 | −0.32 to 0.21 | −0.50 to 0.41 | |
| LM-UM; height of the antrostomy | r | −0.12 | −0.12 | 0.19 |
| p-value | 0.278 | 0.369 | 0.411 | |
| 95% CI | −0.34 to 0.11 | −0.37 to 0.15 | −0.28 to 0.60 |
| Both Biomaterials (n = 78) | Porcine Xenograft (n = 58) | Bovine Xenograft (n = 20) | ||
|---|---|---|---|---|
| IF 1w; Height gain in the intermediate region after 1 week | r | 0.19 | 0.05 | 0.2 |
| p-value | 0.092 | 0.711 | 0.396 | |
| 95% CI | −0.04 to 0.40 | −0.22 to 0.31 | −0.28 to 0.60 | |
| IF 9m; Height gain in the intermediate region after 9 months | r | 0.16 | −0.17 | 0.19 |
| p-value | 0.163 | 0.205 | 0.432 | |
| 95% CI | −0.07 to 0.37 | −0.42 to 0.10 | −0.29 to 0.59 | |
| IF Δ9m−1w; Height changes between 9 months and 1 week | r | −0.02 | −0.26 | 0.18 |
| p-value | 0.847 | 0.0498 | 0.446 | |
| 95% CI | −0.25 to 0.21 | −0.49 to 0.007 | −0.30 to 0.59 |
| Both Biomaterials (n = 78) | Porcine Xenograft (n = 58) | Bovine Xenograft (n = 20) | ||
|---|---|---|---|---|
| IF 1w; Height gain in the intermediate region after 1 week | r | −0.15 | −0.26 | 0.21 |
| p-value | 0.202 | 0.0504 | 0.367 | |
| 95% CI | −0.36 to 0.09 | −0.49 to 0.008 | −0.27 to 0.61 | |
| IF 9m; Height gain in the intermediate region after 9 months | r | −0.16 | −0.18 | 0.1 |
| p-value | 0.17 | 0.1712 | 0.663 | |
| 95% CI | −0.37 to 0.08 | −0.43 to 0.09 | −0.37 to 0.53 | |
| IF 9m−1w; Height gain changes between 9 months and 1 week | r | −0.008 | 0.14 | −0.44 |
| p-value | 0.944 | 0.289 | 0.053 | |
| 95% CI | −0.24 to 0.22 | −0.13 to 0.39 | −0.74 to 0.02 |
| Both Biomaterials (n = 78) | Gen-Os (n = 58) | Cerabone (n = 20) | ||
|---|---|---|---|---|
| XF; Distance from x-axis and sinus floor (height of interest) | r | 0.09 | 0.18 | −0.16 |
| p-value | 0.448 | 0.168 | 0.489 | |
| 95% CI | −0.14 to 0.31 | −0.09 to 0.43 | −0.58 to 0.31 | |
| XW; Distance between medial and lateral sinus bone walls on the X-axis (width of interest) | r | 0.21 | 0.22 | 0.12 |
| p-value | 0.063 | 0.099 | 0.627 | |
| 95% CI | −0.02 to 0.42 | −0.05 to 0.46 | −0.36 to 0.54 | |
| PNR angle; Palato-nasal recess angle | r | −0.02 | −0.10 | 0.18 |
| p-value | 0.891 | 0.472 | 0.447 | |
| 95% CI | −0.24 to 0.21 | −0.35 to 0.17 | −0.30 to 0.59 | |
| SFA; Sinus floor angle | r | 0.20 | 0.11 | 0.50 |
| p-value | 0.076 | 0.416 | 0.026 | |
| 95% CI | −0.03 to 0.41 | −0.16 to 0.36 | 0.056 to 0.78 | |
| LM-F: balcony | r | −0.18 | 0.02 | −0.64 |
| p-value | 0.120 | 0.884 | 0.003 | |
| 95% CI | −0.39 to 0.05 | −0.25 to 0.28 | −0.85 to −0.26 | |
| LM-UM; height of the antrostomy | r | 0.22 | 0.23 | 0.28 |
| p-value | 0.058 | 0.076 | 0.225 | |
| 95% CI | −0.014 to 0.42 | −0.03 to 0.47 | −0.19 to 0.65 | |
| MT t0; mucosa width at t0 | r | −0.25 | −0.25 | −0.23 |
| p-value | 0.025 | 0.055 | 0.339 | |
| 95% CI | −0.46 to −0.026 | −0.49 to 0.01 | −0.62 to 0.25 | |
| LW3mm; lateral wall thickness at 3 mm from sinus floor F | r | 0.18 | 0.07 | 0.47 |
| p-value | 0.106 | 0.595 | 0.038 | |
| 95% CI | −0.05 to 0.40 | −0.20 to 0.33 | 0.02 to 0.76 | |
| LW9mm; lateral wall thickness at 9 mm from sinus floor F | r | −0.06 | −0.07 | −0.03 |
| p-value | 0.577 | 0.590 | 0.9072 | |
| 95% CI | −0.29 to 0.17 | −0.33 to 0.20 | −0.48 to 0.43 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Omori, Y.; Nakajima, Y.; Imai, H.; Yonezawa, D.; Ferri, M.; Apaza Alccayhuaman, K.A.; Botticelli, D. Influence of Anatomical Parameters on the Dimensions of the Subantral Space and Sinus Mucosa Thickening after Sinus Floor Elevation. A Retrospective Cone Beam Computed Tomography Study. Dent. J. 2021, 9, 76. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9070076
Omori Y, Nakajima Y, Imai H, Yonezawa D, Ferri M, Apaza Alccayhuaman KA, Botticelli D. Influence of Anatomical Parameters on the Dimensions of the Subantral Space and Sinus Mucosa Thickening after Sinus Floor Elevation. A Retrospective Cone Beam Computed Tomography Study. Dentistry Journal. 2021; 9(7):76. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9070076
Chicago/Turabian StyleOmori, Yuki, Yasushi Nakajima, Hideki Imai, Daichi Yonezawa, Mauro Ferri, Karol Alí Apaza Alccayhuaman, and Daniele Botticelli. 2021. "Influence of Anatomical Parameters on the Dimensions of the Subantral Space and Sinus Mucosa Thickening after Sinus Floor Elevation. A Retrospective Cone Beam Computed Tomography Study" Dentistry Journal 9, no. 7: 76. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9070076