
Compound Odontoma Removed by Endoscopic Intraoral Approach: Case Report
by
 , and
, and
Masakazu Hamada
1, 
Rena Okawa
2,*,
Kyoko Nishiyama
1,
Ryota Nomura
2,
Narikazu Uzawa
1 and
Kazuhiko Nakano
2 1
Department of Oral and Maxillofacial Surgery II, Osaka University Graduate School of Dentistry, Osaka 565-0871, Japan
2
Department of Pediatric Dentistry, Osaka University Graduate School of Dentistry, Osaka 565-0871, Japan
*
Author to whom correspondence should be addressed.
Dent. J. 2021, 9(7), 81; https://0-doi-org.brum.beds.ac.uk/10.3390/dj9070081
Submission received: 9 June 2021
/
Revised: 29 June 2021
/
Accepted: 5 July 2021
/
Published: 7 July 2021
Abstract
:A 12-year-old Japanese boy was referred to our hospital for evaluation of a radiopaque area on the left side of the mandible. Radiographic and computed tomographic examinations revealed a radiopaque lesion located on the lingual side, along with permanent tooth eruption. Several small tooth-like structures were noted within the lesion and the mandibular left second premolar was inclined in a mesial direction. An odontoma was clinically diagnosed and surgical removal by an endoscopic intraoral approach under general anesthesia was planned. Reports of oral surgery using an endoscopic approach have been presented, though none for an odontoma. With the expectation that removal of the odontoma would improve dentition in this case, we planned future management. A minimally invasive surgical removal procedure by an endoscopic intraoral approach from the lingual side was performed and good early recovery was noted. The resected tumor consisted of several small tooth-like structures. Histopathological diagnosis was a compound odontoma. One-year follow-up findings showed that the post-surgical course was good.
1. Introduction
Odontomas are one of the most common benign odontogenic tumors that occur in the jaw and are composed of enamel, dentin, cementum, and pulp tissue [1,2]. The 4th edition of the World Health Organization’s Classification (WHO classification) of odontogenic tumors published in January of 2017 divides these tumors into complex and compound odontoma [3], which are usually asymptomatic lesions found incidentally during routine radiography [4]. Analyses of odontoma cases in Japan have shown that about half of the patients are between the ages of 10 and 19, with the detection rate for those under the age of 10 reported to be about 10% [5,6]. If no effect on the dentition is observed, treatment may be difficult depending on the site of occurrence. In recent years, endoscopes have come to be used in a variety of areas [7,8]. It has also been used in the field of oral surgery [9,10,11,12,13]. However, there are no reports of its use for odontomas. Here, we report a case of compound odontoma that developed in the mandible of a child and was removed from the lingual side by use of an endoscopic intraoral approach.
2. Case Report
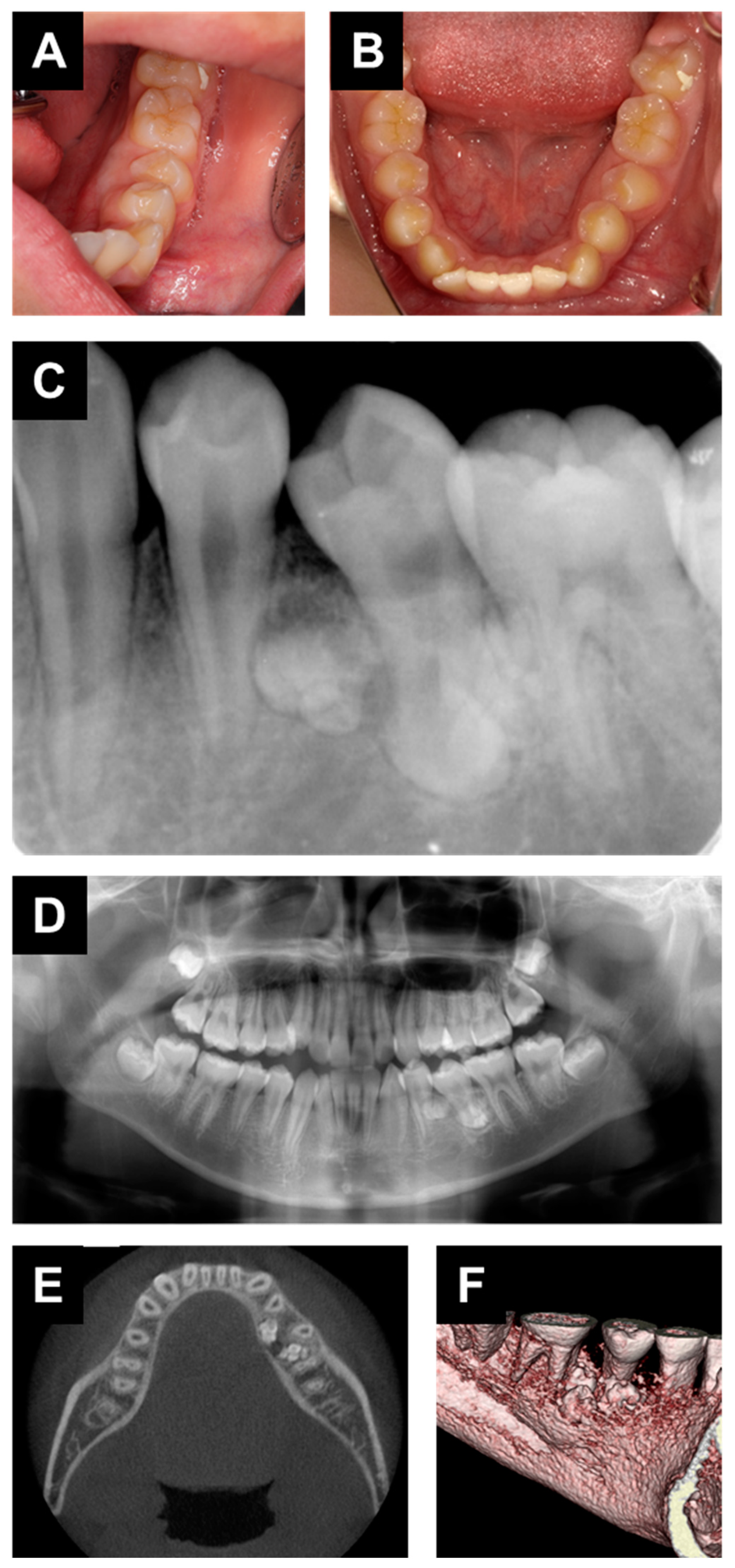
A 12-year-old boy was referred to the Department of Oral and Maxillofacial Surgery at Osaka University Dental Hospital for evaluation of a radiopaque area on the left side of the mandible. There was no special mention of systemic history and the patient reported no symptoms in the affected area. An intraoral examination revealed no obvious gingival swelling around the left mandibular region (Figure 1A), though the mandibular left second premolar was inclined in a mesial direction (Figure 1B). Panoramic and periapical radiography findings showed a radiopaque area around the root apices of the left mandibular first premolar, left mandibular second premolar, and left mandibular first premolar (Figure 1C,D). Computed tomography (CT) results showed several small tooth-like structures within the lesion located on the lingual side (Figure 1E,F), and an odontoma was clinically diagnosed.
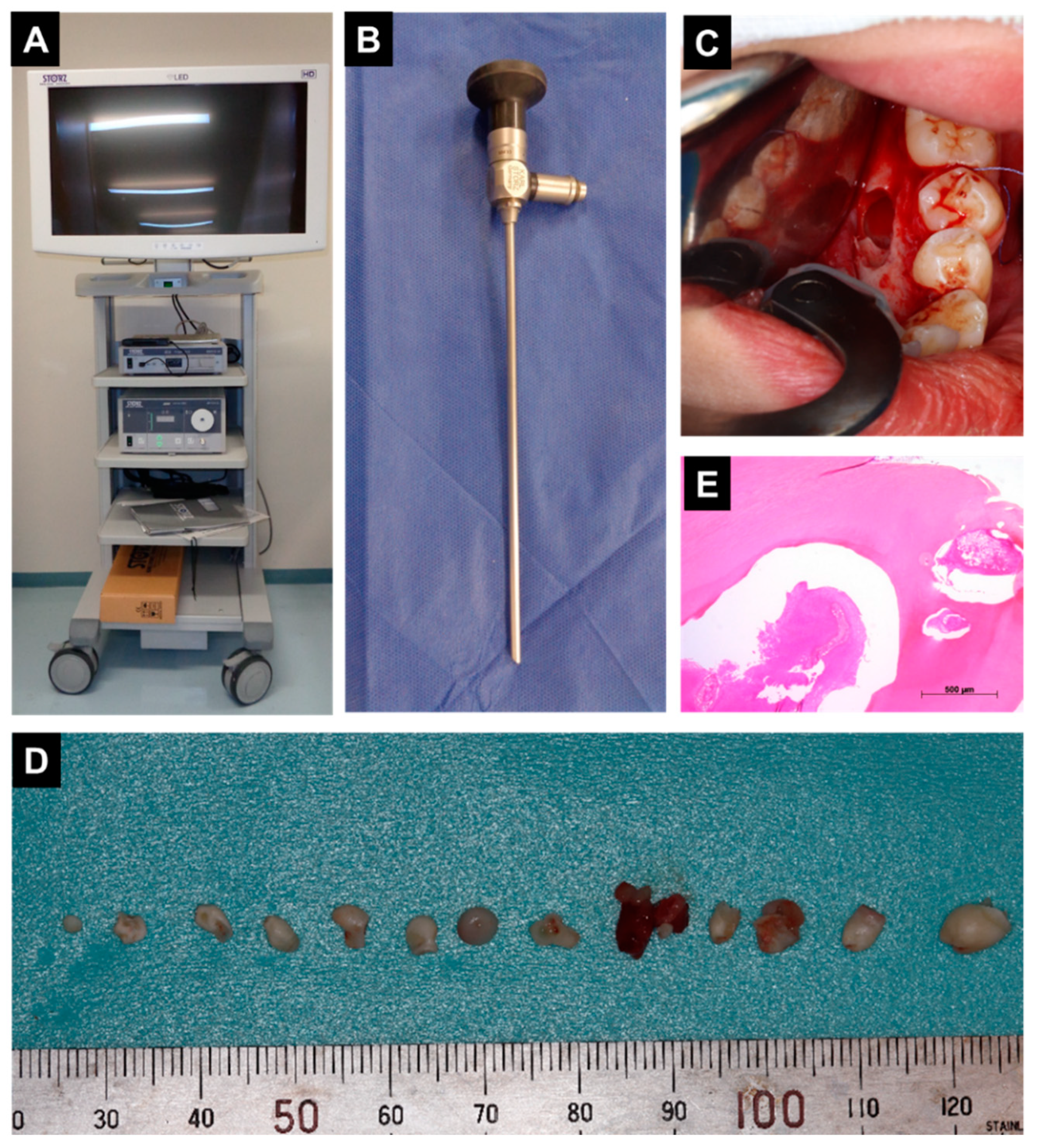
Under general anesthesia, minimally invasive surgical removal with an endoscopic intraoral approach from the lingual side was performed (Figure 2A–C). Since it was difficult to see the lesion directly or with a dental mirror from the lingual side, we decided to use an endoscope for this surgery. We used the KARL STORZ Endoskope (KARL STORZ, Tuttlingen, Germany). The endoscope was used to ensure that the lesion was removed. The resected tumor was found to consist of several small tooth-like structures (Figure 2D). In histopathological analysis findings, hematoxylin and eosin staining of the tooth-like structures showed them to be composed of dentin and cementum with centrally located loose fibrous tissue, considered to be pulp tissue (Figure 2E). Histopathological diagnosis was a compound odontoma.
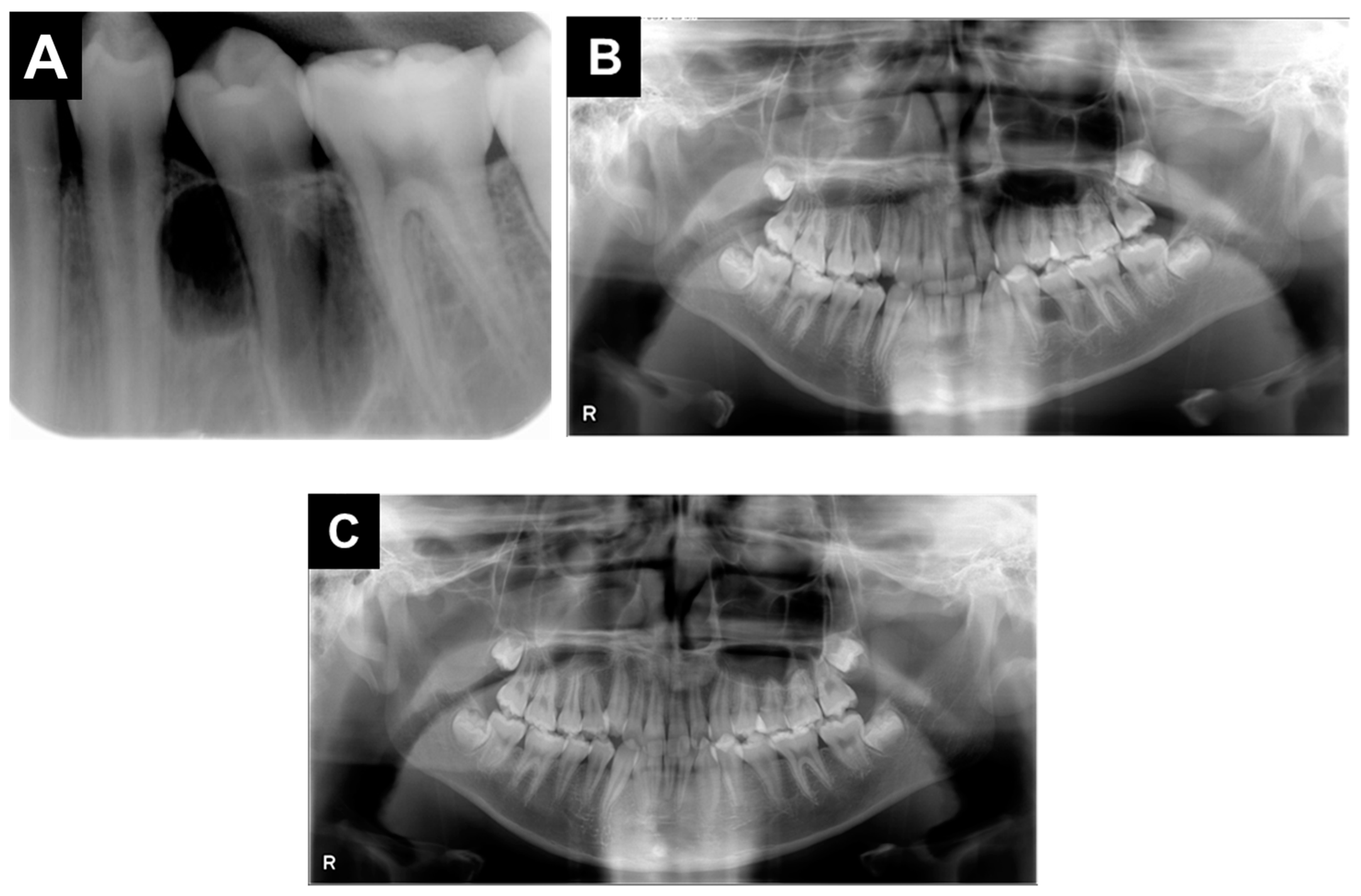
Adjacent tooth roots showed no problems (Figure 3A,B). One year after removal of the odontoma, no recurrence was seen and though dentition improvement was expected, that was not noted (Figure 3C). Furthermore, devitalization of premolars, such as root resorption, tooth discoloration, or mobility, was not observed. The parents and patient did not wish to continue treatment for dentition or occlusion from that time.
3. Discussion
Odontomas are one of the most common benign odontogenic tumors that occur in the jaw, and can be divided into complex and compound type [1,2,3]. Among odontogenic tumors, the frequency of ameloblastomas has been reported to be highest at 45.2%, followed by odontomas at 24.9%, with the incidence rate of complex odontoma 9.7% and that of complex odontoma 15.3% [1]. These tumors are usually asymptomatic lesions found incidentally during a routine radiography examination, and standard treatment of an odontoma associated with soft tissue is complete removal so as to avoid recurrence [2,4]. In the present case, complete removal was the first choice.
Complications associated with an odontoma include eruption disturbance and tooth malposition, while these tumors have also been linked to root resorption of adjacent teeth [14,15]. In the present patient, the odontoma did not cause any eruption problems, and was noticed incidentally in panoramic radiography and periapical radiograph results. Although there was no problem with tooth eruption, the lesion was located on the lingual rather than buccal side, thus it was necessary to consider an approach that would not damage adjacent teeth during extraction. Because of the location between the mandibular left first premolar and mandibular left second premolar, the mandibular left second premolar showed a partial curvature and centrifugal inclination of the root, which caused its tooth crown to be slanted in a proximal direction.
Teeth that erupt in a low position may have increased risk of dental caries or periodontal problems due to difficulties with oral hygiene status, and can also cause various other problems. Such a condition can be prevented by early detection and extraction for avoiding abnormalities in the direction of tooth eruption. Diagnosis based on panoramic radiography results is important when malalignment is observed. However, extraction of an odontoma located between adjacent roots of teeth under formation is risky. Therefore, it is important to detect such a lesion early and consider the timing of extraction while observing the eruption of permanent teeth. In the present case, we planned dentition management with the expectation that removal of the odontoma would improve the condition.
A minimally invasive surgical approach is important for function preservation, as well as patient satisfaction and early recovery. In the present case, careful removal of the tumor in a manner to spare bone not damage the premolars under root formation was considered important. Endoscopic technology, typically employed for a minimally invasive procedure, is widely used with various surgical techniques to reduce tissue invasion during surgery and minimize bleeding [7,8]. In the field of oral surgery, it has been used for cases with fractures of the condylar neck, extraction of deep impacted teeth, and molar apicoectomy procedures [9,10,11,12,13]. On the other hand, there are no known reports regarding use of an endoscopic approach for removal of an odontoma. By using an endoscope, cases typically requiring an extraoral approach can be treated with an intraoral approach, as the technique is designed to reduce the possibility of skin scarring and facial nerve damage as much as possible. Benefits of endoscopically guided surgery in the dental field include minimal invasiveness, avoidance of facial incisions, and reduced amounts of bone loss, bleeding, and nerve and soft tissue damage (Table 1).
In the present case, CT results showed several small tooth-like structures within the lesion and their location on the lingual side. A method performed under direct vision is usually selected for removal of an odontoma, though limitations include difficulty with visualizing the lingual side or near the tooth root, which subsequently increases operative time and risk of iatrogenic damage, such as damage to neurovascular structures or excessive bone removal. Since it was difficult to see the lesion directly from the lingual side or with a dental mirror, we decided to use an endoscope for this procedure. With development of intraoral endoscopy techniques, more conservative bone removal has become possible, and we were able to avoid the risk of root damage in the adjacent tooth and confirm that the lesion had been definitely removed.
Author Contributions
Conceptualization, M.H. and R.O.; methodology, R.O.; validation, M.H., R.O. and K.N. (Kyoko Nishiyama); formal analysis, R.N.; investigation, R.N.; resources, R.O.; data curation, K.N. (Kyoko Nishiyama); writing—original draft preparation, M.H.; writing—review and editing, K.N. (Kazuhiko Nakano); visualization, K.N. (Kazuhiko Nakano); supervision, N.U.; project administration, K.N. (Kazuhiko Nakano). All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki.
Informed Consent Statement
Written informed consent was obtained from the parent of this patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors hereby confirm that there are no known conflict of interest associated with this publication and that there has been no significant financial support for this work that could have influenced the findings presented.
References
- Fernandes, A.M.; Duarte, E.C.B.; Pimenta, F.J.G.S.; Souza, L.N.; Santos, V.R.; Mesquita, R.A.; De Aguiar, M.C.F. Odontogenic tumors: A study of 340 cases in a Brazilian population. J. Oral Pathol. Med. 2005, 34, 583–587. [Google Scholar] [CrossRef] [PubMed]
- Nelson, B.L.; Thompson, L.D.R. Compound Odontoma. Head Neck Pathol. 2010, 4, 290–291. [Google Scholar] [CrossRef] [PubMed]
- Wright, J.M.; Vered, M. Update from the 4th Edition of the World Health Organization Classification of Head and Neck Tumours: Odontogenic and Maxillofacial Bone Tumors. Head Neck Pathol. 2017, 11, 68–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bordini, J.; Contar, C.M.; Sarot, J.R.; Fernandes, Â.; Machado, M.A.N. Multiple Compound Odontomas in the Jaw: Case Report and Analysis of the Literature. J. Oral Maxillofac. Surg. 2008, 66, 2617–2620. [Google Scholar] [CrossRef] [PubMed]
- Hisatomi, M.; Asaumi, J.-I.; Konouchi, H.; Honda, Y.; Wakasa, T.; Kishi, K. A case of complex odontoma associated with an impacted lower deciduous second molar and analysis of the 107 odontomas. Oral Dis. 2002, 8, 100–105. [Google Scholar] [CrossRef] [PubMed]
- Kamakura, N.; Nakano, K.; Okawa, R.; Nomura, R.; Matsumoto, M.; Fukuda, Y.; Ooshima, T. Impacted primary second molar with odontoma identified in the adjacent tissue. Pediatr. Dent. J. 2009, 19, 117–122. [Google Scholar] [CrossRef] [Green Version]
- Ye, Y.J.; Wang, S. Minimally invasive surgery for gastrointestinal stromal tumors--pursuing the trivial, or striving for perfection. Zhonghua Wei Chang Wai Ke Za Zhi 2019, 22, 820–825. [Google Scholar] [PubMed]
- Fukushima, T.; Miyazaki, S.; Takusagawa, Y.; Reichman, M. Unilateral Interhemispheric Keyhole Approach for Anterior Cerebral Artery Aneurysms. Neurosurg. Med. Ethics 1991, 53, 42–47. [Google Scholar]
- Leonhardt, H.; Franke, A.; Nowak, A.; McLeod, N.; Lauer, G. Clinical experience and results with a Rhombic Plate for transoral endoscopically-assisted osteosynthesis of fractures of the condylar neck. Br. J. Oral Maxillofac. Surg. 2019, 57, 1063–1067. [Google Scholar] [CrossRef] [PubMed]
- Liau, I.; Han, J.; Cheng, A.; Duke, P.; Sambrook, P.J.; Goss, A. Endoscopically Assisted Intraoral Removal of an Ectopic Third Molar in the Mandibular Subcondylar Region. J. Craniofacial Surg. 2017, 28, 970–972. [Google Scholar] [CrossRef] [PubMed]
- Gadre, K.; Waknis, P. Intra-oral removal of ectopic third molar in the mandibular condyle. Int. J. Oral Maxillofac. Surg. 2010, 39, 294–296. [Google Scholar] [CrossRef] [PubMed]
- Von Arx, T.; Steiner, R.G.; Tay, F.R. Apical surgery: Endoscopic findings at the resection level of 168 consecutively treated roots. Int. Endod. J. 2011, 44, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Akiyama, K.; Nakai, Y.; Samukawa, Y.; Miyake, M.; Hoshikawa, H. Assessment of Simultaneous Surgery for Odontogenic Sinusitis: Endoscopic Sinus Surgery With Endoscopic Apicoectomy. J. Craniofacial Surg. 2019, 30, 239–243. [Google Scholar] [CrossRef] [PubMed]
- Preoteasa, C.T.; Preoteasa, E. Compound odontoma-morphology, clinical findings and treatment. Case report. Rom. J. Morphol. Embryol. 2018, 59, 997–1000. [Google Scholar] [PubMed]
- Kämmerer, P.W.; Schneider, D.; Schiegnitz, E.; Schneider, S.; Walter, C.; Frerich, B.; Kunkel, M. Clinical parameter of odontoma with special emphasis on treatment of impacted teeth-a retrospective multicentre study and literature review. Clin. Oral Investig. 2016, 20, 1827–1835. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
(A,B) Intraoral photographs taken at the initial visit. (C) Panoramic radiography, (D) periapical radiography, and (E) computed tomography images. (F) Three-dimensional construction of affected region.
Figure 1.
(A,B) Intraoral photographs taken at the initial visit. (C) Panoramic radiography, (D) periapical radiography, and (E) computed tomography images. (F) Three-dimensional construction of affected region.

Figure 2.
(A,B) The endoscope used in the surgery, (C) Intraoperative appearance after removal of tumor. (D) Excised surgical specimen showing tumor mass. (E) A histological examination of the specimen showed irregularly sized vascular spaces surrounded by dense connective tissue (H and E staining).
Figure 2.
(A,B) The endoscope used in the surgery, (C) Intraoperative appearance after removal of tumor. (D) Excised surgical specimen showing tumor mass. (E) A histological examination of the specimen showed irregularly sized vascular spaces surrounded by dense connective tissue (H and E staining).

Figure 3.
(A) Periapical and (B) panoramic radiography images after surgery obtained at follow-up examination. (C) Panoramic radiography image at 1-year follow-up.
Figure 3.
(A) Periapical and (B) panoramic radiography images after surgery obtained at follow-up examination. (C) Panoramic radiography image at 1-year follow-up.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Advantages of endoscopic intraoral approach.
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Hamada, M.; Okawa, R.; Nishiyama, K.; Nomura, R.; Uzawa, N.; Nakano, K. Compound Odontoma Removed by Endoscopic Intraoral Approach: Case Report. Dent. J. 2021, 9, 81. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9070081
AMA Style
Hamada M, Okawa R, Nishiyama K, Nomura R, Uzawa N, Nakano K. Compound Odontoma Removed by Endoscopic Intraoral Approach: Case Report. Dentistry Journal. 2021; 9(7):81. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9070081
Chicago/Turabian StyleHamada, Masakazu, Rena Okawa, Kyoko Nishiyama, Ryota Nomura, Narikazu Uzawa, and Kazuhiko Nakano. 2021. "Compound Odontoma Removed by Endoscopic Intraoral Approach: Case Report" Dentistry Journal 9, no. 7: 81. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9070081
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.