
Adjuvant Effect of Titanium Brushes in Peri-Implant Surgical Treatment: A Systematic Review

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Protocol and Registration
2.2. Search Strategy and Eligibility Criteria
2.3. Information Sources and Keywords
2.4. Study Selection
Study Data
2.5. Quality Assessment (Risk of Bias)
3. Results
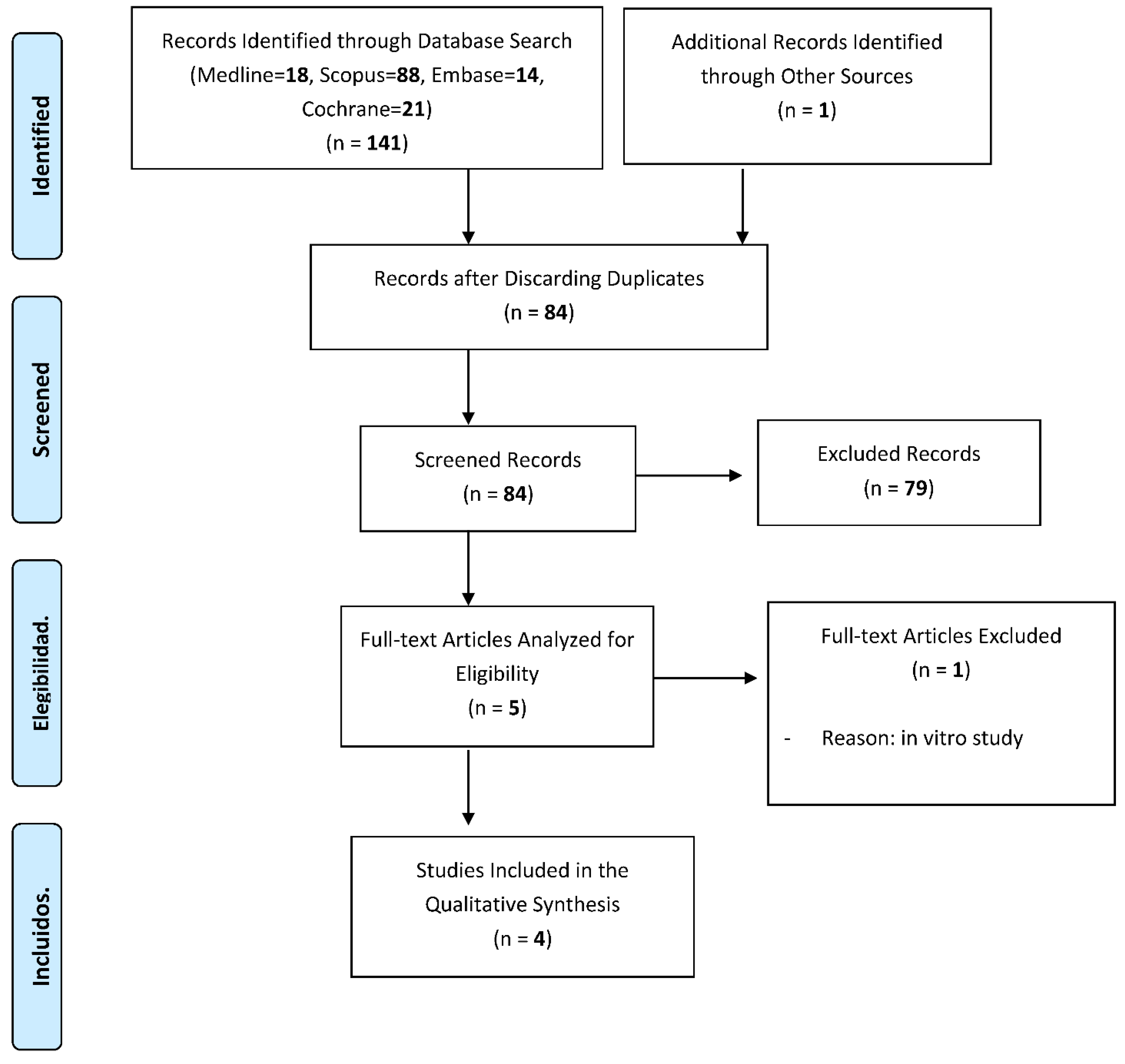
3.1. Study Selection and Flowchart
3.2. Characteristics of the Included Studies
3.3. Qualitative Synthesis of the Included Studies
3.4. Risk of Bias Tool Assessment
4. Discussion
5. Recommendations for Further Research
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Charalampakis, G.; Leonhardt, A.; Rabe, P.; Dahlén, G. Clinical and microbiological characteristics of peri-implantitis cases: A retrospective multicentre study. Clin. Oral Implant. Res. 2011, 23, 1045–1054. [Google Scholar] [CrossRef]
- Smeets, R.; Henningsen, A.; Jung, O.; Heiland, M.; Hammächer, C.; Stein, J.M. Definition, etiology, prevention and treatment of peri-implantitis—A review. Head Face Med. 2014, 10, 34. [Google Scholar] [CrossRef] [Green Version]
- Tonetti, M.S.; Chapple, I.L.C.; Jepsen, S.; Sanz, M. Primary and secondary prevention of periodontal and peri-implant diseases. J. Clin. Periodontol. 2015, 42, S1–S4. [Google Scholar] [CrossRef]
- Romandini, M.; Lima, C.; Pedrinaci, I.; Araoz, A.; Soldini, M.C.; Sanz, M. Clinical signs, symptoms, perceptions, and impact on quality of life in patients suffering from peri-implant diseases: A university-representative cross-sectional study. Clin. Oral Implant. Res. 2021, 32, 100–111. [Google Scholar] [CrossRef]
- Norowski, P.A., Jr.; Bumgardner, J.D. Review Biomaterial and Antibiotic Strategies for Peri-implantitis. J. Biomed. Mater. Res. B Appl. Biomater. 2009, 88, 530–543. [Google Scholar] [CrossRef]
- Figuero, E.; Graziani, F.; Sanz, I.; Herrera, D.; Sanz, M. Management of peri-implant mucositis and peri-implantitis. Periodontology 2000 2014, 66, 255–273. [Google Scholar] [CrossRef]
- Romandini, M.; Lima, C.; Pedrinaci, I.; Araoz, A.; Soldini, M.C.; Sanz, M. Prevalence and risk/protective indicators of peri-implant diseases: A university-representative cross-sectional study. Clin. Oral Implant. Res. 2021, 32, 112–122. [Google Scholar] [CrossRef]
- Quirynen, M.; de Soete, M.; van Steenberghe, D. Infectious risks for oral implants: A review of the literature. Clin. Oral Implant. Res. 2002, 13, 1–19. [Google Scholar] [CrossRef]
- Muthukuru, M.; Zainvi, A.; Esplugues, E.O.; Flemmig, T.F. Non-surgical therapy for the management of peri-implantitis: A sys-tematic review. Clin. Oral Implant. Res. 2012, 23, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Berglundh, T.; Armitage, G.; Araujo, M.G.; Avila-Ortiz, G.; Blanco, J.; Camargo, P.M.; Chen, S.; Cochran, D.; Derks, J.; Figuero, E.; et al. Peri-implant diseases and conditions: Consensus report of workgroup 4 of the 2017 world workshop on the classification of periodontal and Peri-Implant diseases and conditions. J. Clin. Periodontol. 2018, 45, S286–S291. [Google Scholar] [CrossRef] [Green Version]
- Ramanauskaite, A.; Daugela, P.; Juodzbalys, G. Treatment of peri-implantitis: Meta-analysis of findings in a systematic literature review and novel protocol proposal. Quintessence Int. 2016, 47, 379. [Google Scholar] [PubMed]
- Schwarz, F.; Sahm, N.; Iglhaut, G.; Becker, J. Impact of the method of surface debridement and decontamination on the clinical outcome following combined surgical therapy of peri-implantitis: A randomized controlled clinical study. J. Clin. Periodontol. 2011, 38, 276–284. [Google Scholar] [CrossRef]
- Rösing, C.K.; Fiorini, T.; Haas, A.N.; Muniz, F.; Oppermann, R.V.; Susin, C. The impact of maintenance on peri-implant health. Braz. Oral Res. 2019, 33, e074. [Google Scholar] [CrossRef] [Green Version]
- Mancini, L.; Romandini, M.; Fratini, A.; Americo, L.M.; Panda, S.; Marchetti, E. Biomaterials for Periodontal and Peri-Implant Re-generation. Materials 2021, 14, 3319. [Google Scholar] [CrossRef]
- Buitrago Vera, P.J.; de Rojas, F.J. Diagnóstico, tratamiento y prevención de la mucositis periimplntaria y la periimplan-titis. JIRD 2002, 7, 37. [Google Scholar]
- Claffey, N.; Clarke, E.; Polyzois, I.; Renvert, S. Surgical treatment of peri-implantitis. J. Clin. Periodontal. 2008, 35, 316–332. [Google Scholar] [CrossRef]
- De Tapia, B.; Valles, C.; Ribeiro-Amaral, T.; Mor, C.; Herrera, D.; Sanz, M.; Nart, J. The adjunctive effect of a titanium brush in implant surface decontamination at peri-implantitis surgical regenerative interventions: A randomized controlled clinical trial. J. Clin. Periodontal. 2019, 46, 586–596. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Green, S. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0; The Cochrane Collaboration: London, UK, 2011; Available online: www.cochrane-handbook.org (accessed on 1 March 2020).
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alotaibi, M.; Moran, G.; Grufferty, B.; Renvert, S.; Polyzois, I. The effect of a decontamination protocol on contaminated titanium dental implant surfaces with different surface topography in edentulous patients. Acta Odontol. Scand. 2018, 77, 66–75. [Google Scholar] [CrossRef]
- Toma, S.; Brecx, M.C.; Lasserre, J.F. Clinical Evaluation of Three Surgical Modalities in the Treatment of Peri-Implantitis: A Randomized Controlled Clinical Trial. J. Clin. Med. 2019, 8, 966. [Google Scholar] [CrossRef] [Green Version]
- Jepsen, K.; Jepsen, S.; Laine, M.L.; Anssari Moin, D.; Pilloni, A.; Zeza, B.; Sanz, M.; Ortiz-Vigon, A.; Roos-Jansåker, A.M.; Renvert, S. Reconstruction of Peri-implant Osseous Defects: A Multicenter Randomized Trial. J. Dent. Res. 2016, 95, 58–66. [Google Scholar] [CrossRef]
- Guler, B.; Uraz, A.; Yalım, M.; Bozkaya, S. The Comparison of Porous Titanium Granule and Xenograft in the Surgical Treat-ment of Peri-Implantitis: A Prospective Clinical Study. Clin. Implant Dent. Relat. Res. 2017, 19, 316–327. [Google Scholar] [CrossRef]
- John, G.; Becker, J.; Schwarz, F. Rotating titanium brush for plaque removal from rough titanium surfaces—An in vitro study. Clin. Oral Implants Res. 2014, 25, 838–842. [Google Scholar] [CrossRef]
- Gustumhaugen, E.; Lönn-Stensrud, J.; Scheie, A.A.; Lyngstadaas, S.P.; Ekfeldt, A.; Taxt-Lamolle, S. Effect of chemical and mechanical debridement techniques on bacterial re-growth on rough titanium surfaces: An in vitro study. Clin. Oral Implant. Res. 2013, 25, 707–713. [Google Scholar] [CrossRef] [PubMed]
- Sanz-Martín, I.; Paeng, K.; Park, H.; Cha, J.-K.; Jung, U.-W.; Sanz, M. Significance of implant design on the efficacy of different peri-implantitis decontamination protocols. Clin. Oral Investig. 2021, 25, 3589–3597. [Google Scholar] [CrossRef]
- Ronay, V.; Merlini, A.; Attin, T.; Schmidlin, P.R.; Sahrmann, P. In vitro cleaning potential of three implant debridement methods. Simulation of the non-surgical approach. Clin. Oral Implants Res. 2017, 28, 151–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sahrmann, P.; Ronay, V.; Hofer, D.; Attin, T.; Jung, R.E.; Schmidlin, P.R. In vitro cleaning potential of three different implant debridement methods. Clin. Oral Implants Res. 2015, 26, 314–319. [Google Scholar] [CrossRef]
- Sahrmann, P.; Ronay, V.; Sener, B.; Jung, R.E.; Attin, T.; Schmidlin, P.R. Cleaning potential of glycine air-flow application in an in vitro peri-implantitis model. Clin. Oral Implants Res. 2013, 24, 666–670. [Google Scholar] [CrossRef] [PubMed]
- Park, J.B.; Jeon, Y.; Ko, Y. Effects of titanium brush on machined and sandblasted/acid-etched titanium disc using confocal mi-croscopy and contact profilometry. Clin. Oral Implants Res. 2015, 26, 130–136. [Google Scholar] [CrossRef]
- Al-Hashedi, A.A.; Laurenti, M.; Abdallah, M.N.; Albuquerque, R.F.; Tamimi, F. Electrochemical Treatment of Contaminated Tita-nium Surfaces in Vitro: An Approach for Implant Surface Decontamination. ACS Biomater. Sci. Eng. 2016, 2, 1504–1518. [Google Scholar] [CrossRef]
- Carral, C.; Muñoz, F.; Permuy, M.; Liñares, A.; Dard, M.; Blanco, J. Mechanical and chemical implant decontamination in surgical peri-implantitis treatment. Preclinical “in vivo” study. J. Clin. Periodontol. 2016, 43, 694–701. [Google Scholar] [CrossRef]
- Viganò, P.; Alccayhuaman, K.A.A.; Sakuma, S.; Amari, Y.; Bengazi, F.; Botticelli, D. Use of TiBrush for surface decontamination at peri-implantitis sites in dogs: Radiographic and histological outcomes. J. Investig. Clin. Dent. 2018, 10, e12378. [Google Scholar] [CrossRef]


{kind=link}
| Database | Search Strategy | Results |
|---|---|---|
| Medline | #1 (periimplantitis) OR (peri-implantitis) | 2.038 |
| #2 (implant surface decontamination) | 172 | |
| #3 (titanium brush) | 80 | |
| #1 AND #2 AND #3 | 18 | |
| Scopus | #1 (periimplantitis) OR (peri-implantitis) | 8.762 |
| #2 (implant surface decontamination) | 2.057 | |
| #3 (titanium brush) | 10.239 | |
| #1 AND #2 AND #3 | 88 | |
| Cochrane | #1 (periimplantitis) OR (peri-implantitis) | 21 |
| #2 (implant surface decontamination) | 6 | |
| #3 (titanium brush) | 3 | |
| #1 AND #2 AND #3 | 21 | |
| Embase | #1 (periimplantitis) OR (peri-implantitis) | 3.014 |
| #2 (implant surface decontamination) | 226 | |
| #3 (titanium brush) | 105 | |
| #1 AND #2 AND #3 | 14 |
| Author and Year | Type of Study | Sample | Decontamination Method | Type of Surgery | Follow-Up Time | Findings |
|---|---|---|---|---|---|---|
| Tapia et al., (2018) [17] | RCT | Control group: n = 15 Experimental group: n = 15 | Control group: points of US and H2O2 at 3%. Experimental group: = control group + titanium brushes | Regenerative | 12 months | PD in the experimental group: p = 0.007 Rest of variables: p > 0.05 |
| Toma et al., (2019) [22] | RCT | Plastic curettes group: n = 15 Abrasive air group: n = 16 Titanium brushes group: n = 16 | Plastic curettes group (Gracey): with irrigation with NaCl. Abrasive air group (Perio-Flow®): glycine amino acid powder application + irrigation with NaCl. Titanium brushes group (Ti-Brush®): with irrigation with NaCl. | Resective | 6 months | PI and PD in the titanium brushes group: p < 0.001) BL in the titanium brushes group with respect to the plastic curettes: p < 0.001) |
| Jepsen et al., (2016) [23] | RCT | Case group: n = 33 Control group: n = 30 | Both groups with decontamination with titanium brushes + H2O2 al 3%. | Case group: regenerative | 12 months | Increased bone gain in the case group: p < 0.0001 |
| Control group: resective. | ||||||
| Guler et al., (2016) [24] | Prospective Clinical Study | Group 1: n = 18 Group 2: n = 6 | Group 1: titanium curettes + titanium brushes Group 2: titanium curettes. | Group 1: regenerative | 6 months | Increased bone gain in group 1: p < 0.05 |
| Group 2: regenerative |
| Author and Year | PI (%) | PD (mm) | BoP (%) | BL (mm) | ||||
|---|---|---|---|---|---|---|---|---|
| Initial | Final | Initial | Final | Initial | Final | Initial | Final | |
| Tapia et al. (2018) [17] | 14.54 ± 6.12 | 16.56 ± 8.39 | 6.16 ± 1.27 | 3.32 ± 0.72 | 100 ± 0 | 20 ± 41 | 3.91 ± 0.93 | 1.2 ± 1.14 |
| Toma et al. (2019) [22] | 1.12 ± 0.44 | 0.3 ± 0.23 | 6.45 ± 1.87 | 3.98 ± 1.43 | 62 ± 4.7 | 16 ± 3.7 | 7.09 ± 1.23 | 5.88 ± 1.3 |
| Jepsen et al. (2016) [23] | 25.8 ± 36.8 | 21.0 ± 28.7 | 6.3 ± 1.3 | 3.5 ± 1.5 | 89.4 ± 20.7 | 33.3 ± 3.7 | M: 5.55 ± 2.3 D: 5.41 ± 2.72 | M: 1.98 ± 1.99 D: 1.96 ± 1.95 |
| 24.8 ± 36.3 | 10.33 ± 20.0 | 6.3 ± 1.6 | 3.5 ± 1.1 | 85.8 ± 23.9 | 40.4 ± 37.1 | M: 4.63 ± 4.45 D: 4.45 ± 2.23 | M: 3.63 ± 2.34 D: 3.63 ± 2.32 | |
| Guler et al. (2016) [24] | 0.73 ± 0.72 | 0.64 ± 0.52 | 5.28 ± 1.06 | 3.34 ± 0.82 | 50.17 ± 25.19 | 24.32 ± 11.22 | - | BG: 1.74 ± 0.65 |
| 0.98 ± 0.82 | 0.61 ± 0.66 | 4.72 ± 1.02 | 3.18 ± 0.54 | 63.51 ± 24.38 | 33.00 ± 15.51 | - | BG: 1.05 ± 0.54 | |
| Study | 1 | 2 | 3 | 4 | 5 | 6 | 7 | Final Assessment |
|---|---|---|---|---|---|---|---|---|
| Tapia et al., (2018) [17] |  |  |  |  |  |  |  |  |
| Toma et al., (2019) [22] |  |  |  |  |  |  |  |  |
| Jepsen et al., (2016) [23] |  |  |  |  |  |  |  |  |
| Author and Year | Confounding | Selection of Participants | Classification of Interventions | Deviations from Intended Deviations | Missing Data | Measurement of Outcomes | Selection of Reported Results | Overall |
|---|---|---|---|---|---|---|---|---|
| Guler et al., (2016) [19] | Low | Low | Low | Low | Moderate | Low | Moderate | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
González, F.J.; Requena, E.; Miralles, L.; Sanz, J.L.; Barberá, J.; Enciso, J.J.; Larrazábal, C.; Gómez, M.D. Adjuvant Effect of Titanium Brushes in Peri-Implant Surgical Treatment: A Systematic Review. Dent. J. 2021, 9, 84. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9080084
González FJ, Requena E, Miralles L, Sanz JL, Barberá J, Enciso JJ, Larrazábal C, Gómez MD. Adjuvant Effect of Titanium Brushes in Peri-Implant Surgical Treatment: A Systematic Review. Dentistry Journal. 2021; 9(8):84. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9080084
Chicago/Turabian StyleGonzález, Francisco Javier, Estefanía Requena, Lucía Miralles, José Luis Sanz, Javier Barberá, José Juan Enciso, Carolina Larrazábal, and María Dolores Gómez. 2021. "Adjuvant Effect of Titanium Brushes in Peri-Implant Surgical Treatment: A Systematic Review" Dentistry Journal 9, no. 8: 84. https://0-doi-org.brum.beds.ac.uk/10.3390/dj9080084