
Quantitative Risk Assessment of Exposure to Mycobacterium avium subsp. paratuberculosis (MAP) via Different Types of Milk for the Slovenian Consumer

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
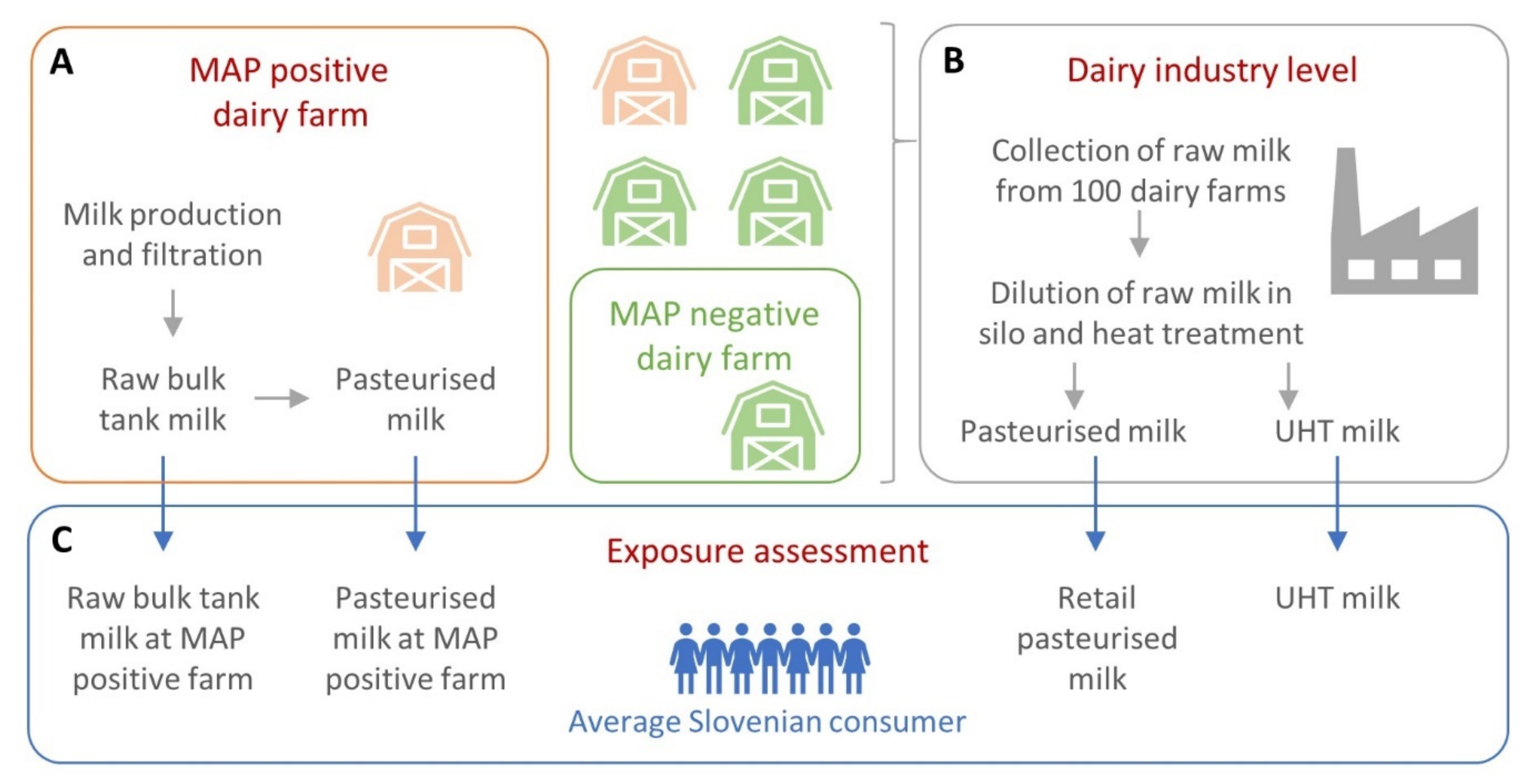
2.1. Model Structure and Parameters
2.2. Model Simulation and Validation
2.3. Risk Characterisation
3. Results
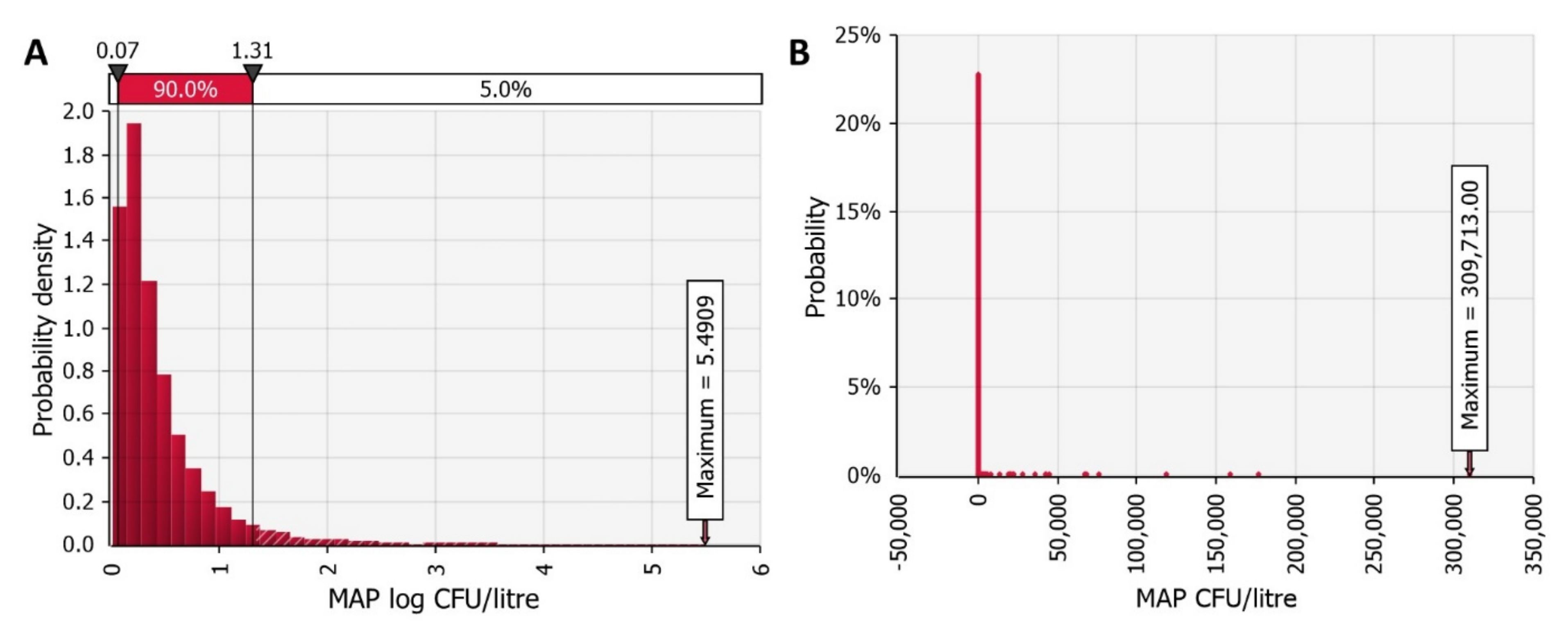
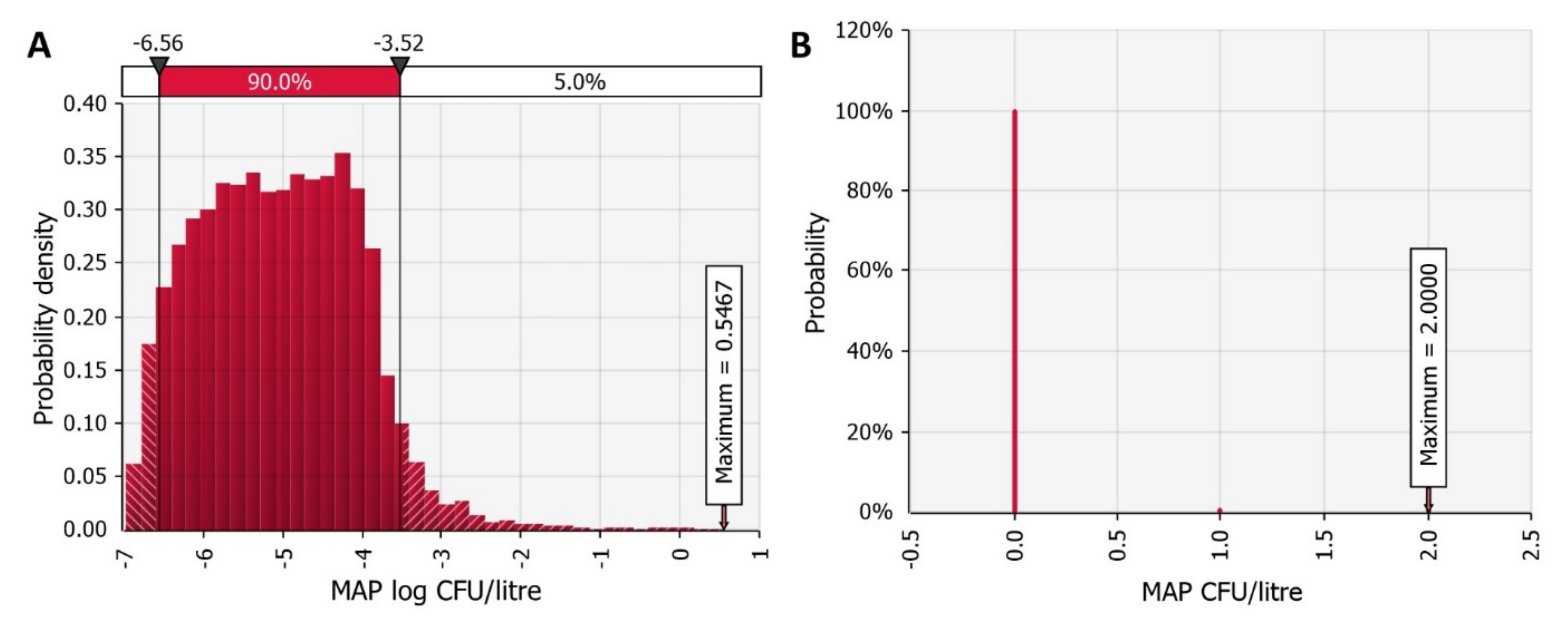
3.1. MAP Contamination of Raw and Pasteurised Milk in a MAP Positive Farm
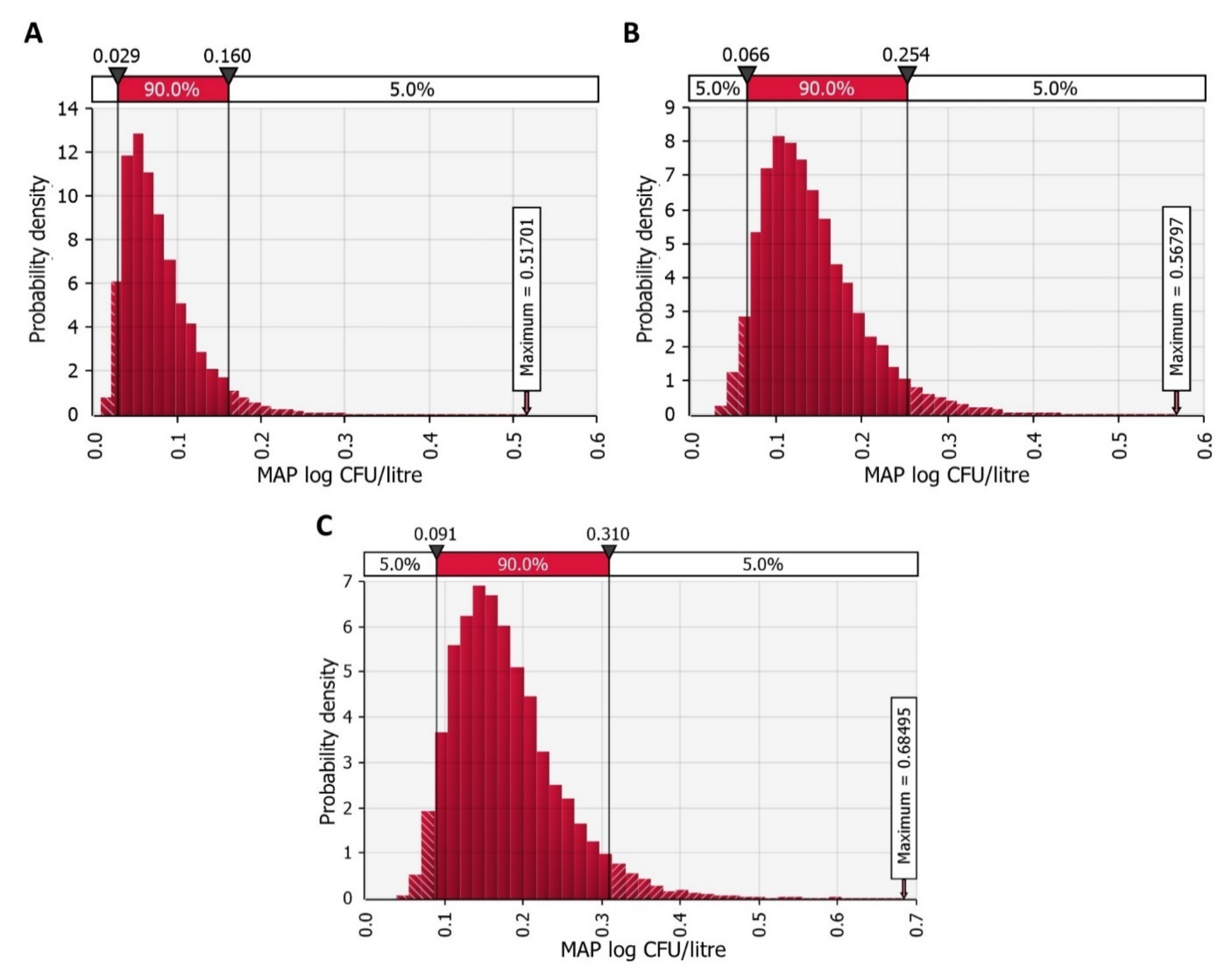
3.2. MAP Contamination of Pasteurised and UHT Milk at the Industry Level
3.3. Risk of Exposure to MAP via Milk for the Average Consumer
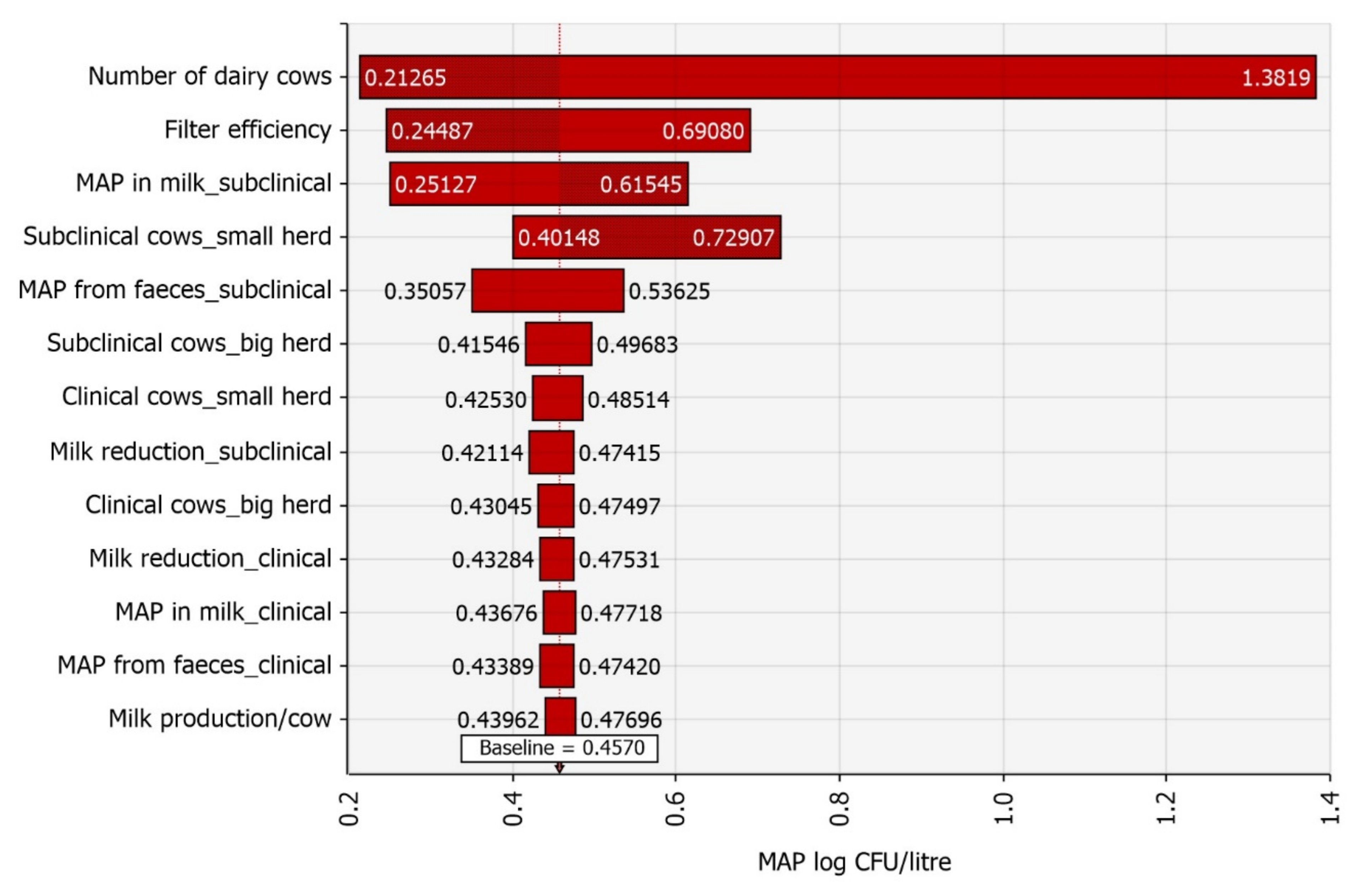
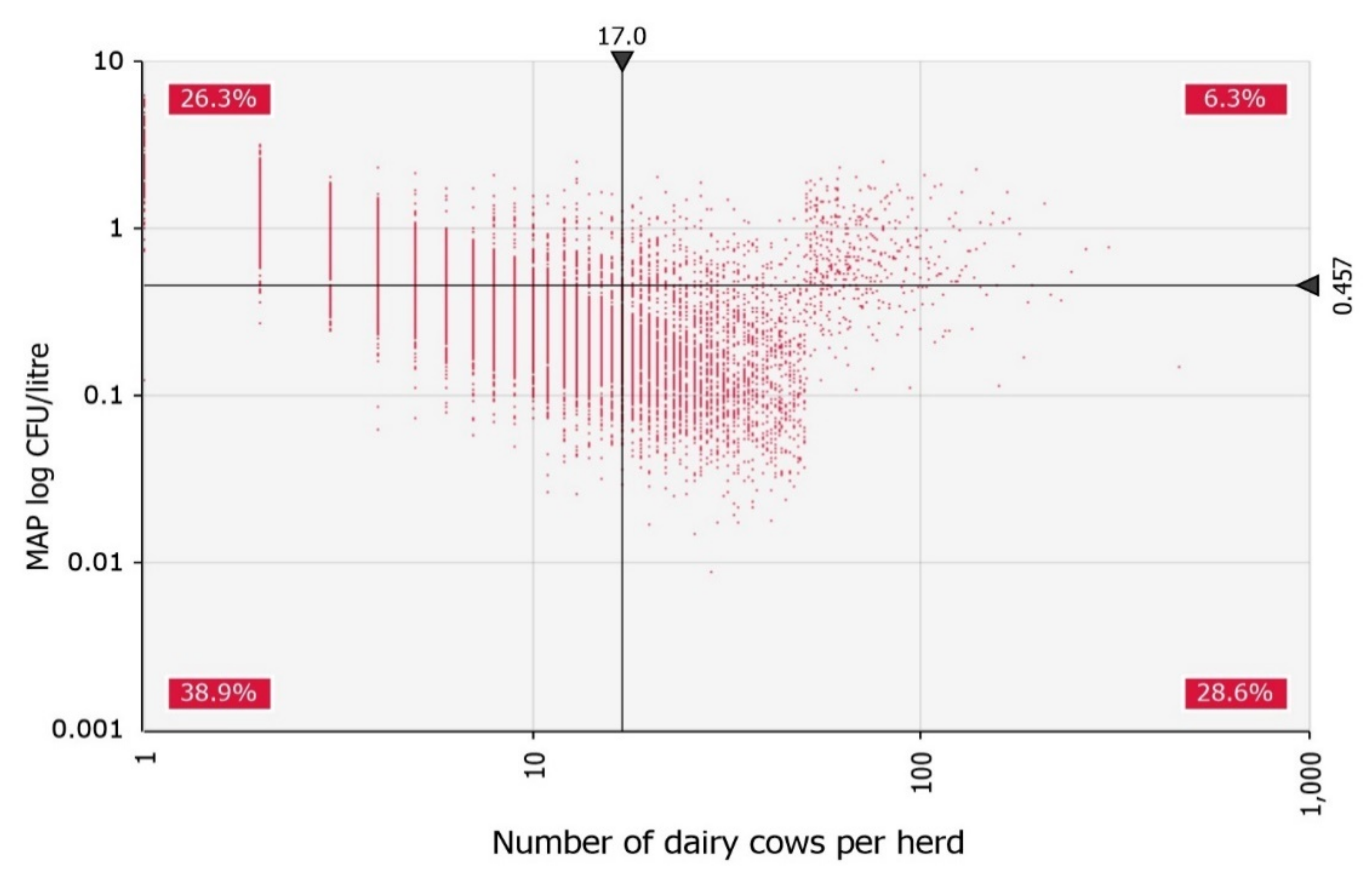
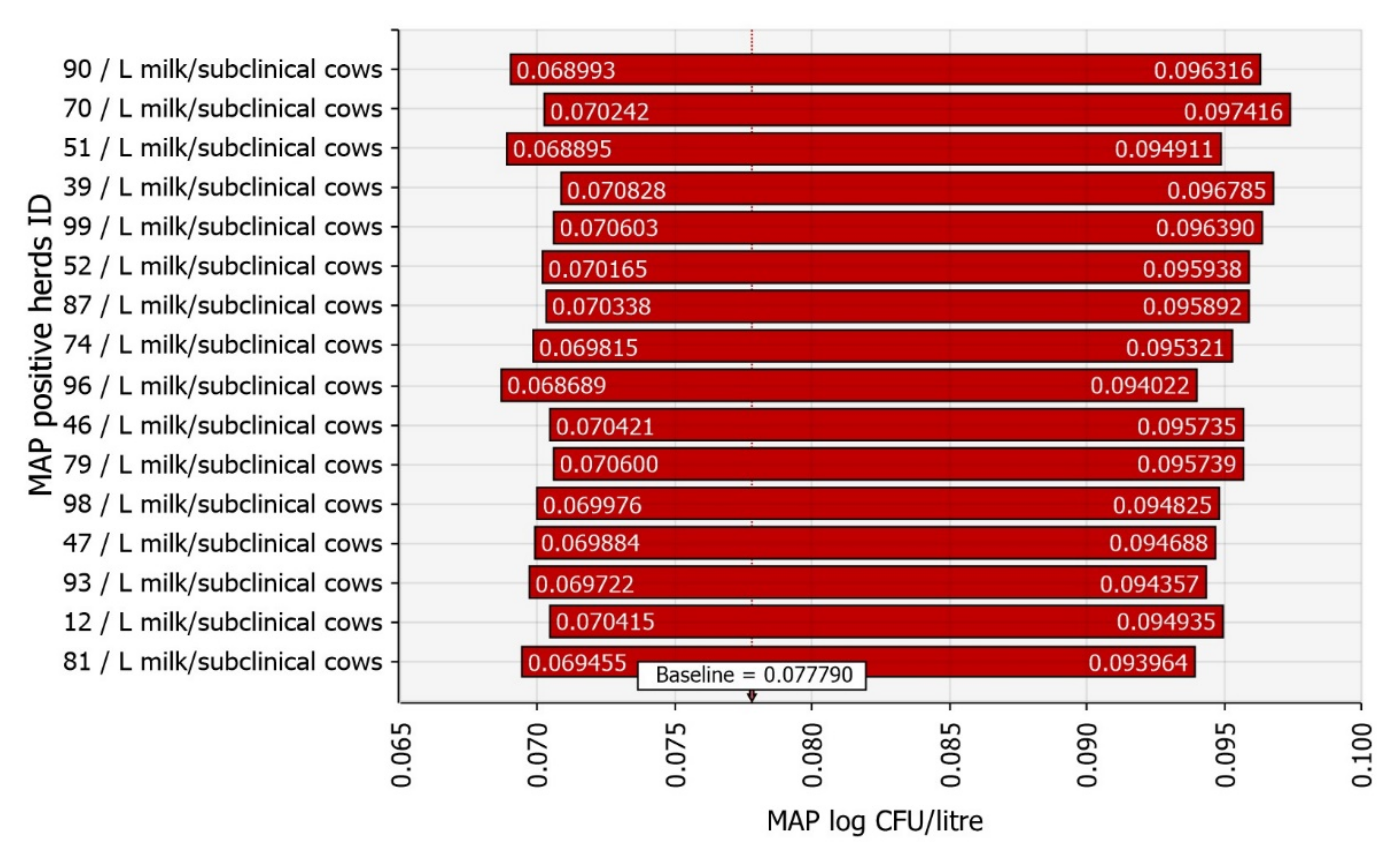
3.4. Sensitivity Analysis
3.5. Risk Characterisation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feller, M.; Huwiler, K.; Stephan, R.; Altpeter, E.; Shang, A.; Furrer, H.; Pfyffer, G.E.; Jemmi, T.; Baumgartner, A.; Egger, M. Mycobacterium avium subspecies paratuberculosis and Crohn’s disease: A systematic review and meta-analysis. Lancet. Infect. Dis. 2007, 7, 607–613. [Google Scholar] [CrossRef]
- Ekundayo, T.C.; Falade, A.O.; Igere, B.E.; Iwu, C.D.; Adewoyin, M.A.; Olasehinde, T.A.; Ijabadeniyi, O.A. Systematic and meta-analysis of Mycobacterium avium subsp. paratuberculosis related type 1 and type 2 diabetes mellitus. Sci. Rep. 2022, 12, 4608. [Google Scholar] [CrossRef] [PubMed]
- Ozana, V.; Hruska, K.; Sechi, L.A. Neglected Facts on Mycobacterium Avium Subspecies Paratuberculosis and Type 1 Diabetes. Int. J. Mol. Sci. 2022, 23, 3657. [Google Scholar] [CrossRef] [PubMed]
- Masala, S.; Cossu, D.; Palermo, M.; Sechi, L.A. Recognition of Zinc Transporter 8 and MAP3865c Homologous Epitopes by Hashimoto’s Thyroiditis Subjects from Sardinia: A Common Target with Type 1 Diabetes? PLoS ONE 2014, 9, e97621. [Google Scholar] [CrossRef] [Green Version]
- Ekundayo, T.C.; Olasehinde, T.A.; Falade, A.O.; Adewoyin, M.A.; Iwu, C.D.; Igere, B.E.; Ijabadeniyi, O.A. Systematic Review and Meta-Analysis of Mycobacterium avium subsp. paratuberculosis as Environmental Trigger of Multiple Sclerosis. Mult. Scler. Relat. Disord. 2022, 59, 103671. [Google Scholar] [CrossRef]
- Arru, G.; Caggiu, E.; Paulus, K.; Sechi, G.P.; Mameli, G.; Sechi, L.A. Is there a role for Mycobacterium avium subspecies paratuberculosis in Parkinson’s disease? J. Neuroimmunol. 2016, 293, 86–90. [Google Scholar] [CrossRef]
- Dow, C.T. Warm, Sweetened Milk at the Twilight of Immunity—Alzheimer’s Disease—Inflammaging, Insulin Resistance, M. paratuberculosis and Immunosenescence. Front. Immunol. 2021, 12, 714179. [Google Scholar] [CrossRef]
- Richter, E.; Wessling, J.; Lugering, N.; Domschke, W.; Rusch-Gerdes, S. Mycobacterium avium subsp. paratuberculosis infection in a patient with HIV, Germany. Emerg. Infect. Dis. 2002, 8, 729–731. [Google Scholar] [CrossRef]
- Niegowska, M.; Rapini, N.; Piccinini, S.; Mameli, G.; Caggiu, E.; Manca Bitti, M.L.; Sechi, L.A. Type 1 Diabetes at-risk children highly recognize Mycobacterium avium subspecies paratuberculosis epitopes homologous to human Znt8 and Proinsulin. Sci. Rep. 2016, 6, 22266. [Google Scholar] [CrossRef] [Green Version]
- Garvey, M. Mycobacterium avium subspecies paratuberculosis: A causative agent in human morbidity and risk to public health safety. Open Vet. J. 2018, 8, 172–181. [Google Scholar] [CrossRef] [Green Version]
- Barkema, H.W.; Hesselink, J.W.; McKenna, S.L.B.; Benedictus, G.; Groenendaal, H. Global Prevalence and Economics of Infection with Mycobacterium avium subsp. paratuberculosis in Ruminants. In Paratuberculosis: Organism, Disease, Control; Behr, M.A., Collins, D.M., Eds.; CAB International: Oxfordshire, UK, 2010; pp. 10–21. [Google Scholar]
- EFSA Panel on Animal Health and Welfare (AHAW); More, S.; Bøtner, A.; Butterworth, A.; Calistri, P.; Depner, K.; Edwards, S.; Garin-Bastuji, B.; Good, M.; Gortázar Schmidt, C.; et al. Assessment of Listing and Categorisation of Animal Diseases within the Framework of the Animal Health Law (Regulation (EU) No 2016/429): Paratuberculosis. EFSA J. 2017, 15, e04960. [Google Scholar] [CrossRef]
- Crohn, B.B.; Ginzburg, L.; Oppenheimer, G.D. Regional Ileitis: A Pathologic and Clinical Entity. J. Am. Med. Assoc. 1932, 99, 1323–1329. [Google Scholar] [CrossRef]
- Garvey, M. Mycobacterium Avium Paratuberculosis: A Disease Burden on the Dairy Industry. Animals 2020, 10, 1773. [Google Scholar] [CrossRef] [PubMed]
- Harris, N.B.; Barletta, R.G. Mycobacterium avium subsp. paratuberculosis in Veterinary Medicine. Clin. Microbiol. Rev. 2001, 14, 489–512. [Google Scholar] [CrossRef] [Green Version]
- Nigsch, A.; Robbe-Austerman, S.; Stuber, T.P.; Bitar, P.D.P.; Gröhn, Y.T.; Schukken, Y.H. Who infects whom?—Reconstructing infection chains of Mycobacterium avium ssp. paratuberculosis in an endemically infected dairy herd by use of genomic data. PLoS ONE 2021, 16, e0246983. [Google Scholar] [CrossRef] [PubMed]
- Whittington, R.; Donat, K.; Weber, M.F.; Kelton, D.; Nielsen, S.S.; Eisenberg, S.; Arrigoni, N.; Juste, R.; Sáez, J.L.; Dhand, N.; et al. Control of Paratuberculosis: Who, Why and How. A Review of 48 Countries. BMC Vet. Res. 2019, 4, 198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuenstner, J.T.; Naser, S.; Chamberlin, W.; Borody, T.; Graham, D.Y.; McNees, A.; Hermon-Taylor, J.; Hermon-Taylor, A.; Dow, C.T.; Thayer, W.; et al. The Consensus from the Mycobacterium avium ssp. paratuberculosis (MAP) Conference 2017. Front. Public Health 2017, 5, 208. [Google Scholar] [CrossRef]
- Timms, V.J.; Daskalopoulos, G.; Mitchell, H.M.; Neilan, B.A. The association of Mycobacterium avium subsp paratuberculosis with inflammatory bowel disease. PLoS ONE 2016, 11, e0148731. [Google Scholar] [CrossRef] [Green Version]
- Kuenstner, J.T.; Potula, R.; Bull, T.J.; Grant, I.R.; Foddai, A.; Naser, S.A.; Bach, H.; Zhang, P.; Yu, D.; Lu, X.; et al. Presence of Infection by Mycobacterium avium subsp. paratuberculosis in the Blood of Patients with Crohn’s Disease and Control Subjects Shown by Multiple Laboratory Culture and Antibody Methods. Microorganisms 2020, 8, 2054. [Google Scholar] [CrossRef]
- Qasem, A.; Elkamel, E.; Naser, S.A. Anti-MAP Triple Therapy Supports Immunomodulatory Therapeutic Response in Crohn’s Disease through Downregulation of NF-κB Activation in the Absence of MAP Detection. Biomedicines 2020, 8, 513. [Google Scholar] [CrossRef]
- Agrawal, G.; Hamblin, H.; Clancy, A.; Borody, T. Anti-Mycobacterial Antibiotic Therapy Induces Remission in Active Paediatric Crohn’s Disease. Microorganisms 2020, 8, 1112. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, I.A.; Pietralonga, P.A.G.; Schwarz, D.G.G.; Faria, A.C.S.; Moreira, M.A.S. Short Communication: Recovery of Viable Mycobacterium avium subspecies paratuberculosis from Retail Pasteurized Whole Milk in Brazil. J. Dairy Sci. 2012, 95, 6946–6948. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robertson, R.E.; Cerf, O.; Condron, R.J.; Donaghy, J.A.; Heggum, C.; Jordan, K. Review of the Controversy over Whether or Not Mycobacterium avium subsp. paratuberculosis Poses a Food Safety Risk with Pasteurised Dairy Products. Int. Dairy J. 2017, 73, 10–18. [Google Scholar] [CrossRef]
- Honap, S.; Johnston, E.; Agrawal, G.; Al-Hakim, B.; Hermon-Taylor, J.; Sanderson, J. Anti-Mycobacterium paratuberculosis (MAP) therapy for Crohn’s disease: An overview and update. Frontline Gastroenterol. 2020, 12, 397–403. [Google Scholar] [CrossRef]
- Agrawal, G.; Aitken, J.; Hamblin, H.; Collins, M.; Borody, T.J. Putting Crohn’s on the MAP: Five Common Questions on the Contribution of Mycobacterium avium subspecies paratuberculosis to the Pathophysiology of Crohn’s Disease. Dig. Dis. Sci. 2021, 66, 348–358. [Google Scholar] [CrossRef] [PubMed]
- Eslami, M.; Shafiei, M.; Ghasemian, A.; Valizadeh, S.; Al-Marzoqi, A.H.; Shokouhi Mostafavi, S.K.; Nojoomi, F.; Mirforughi, S.A. Mycobacterium avium paratuberculosis and Mycobacterium avium complex and related subspecies as causative agents of zoonotic and occupational diseases. J. Cell. Physiol. 2019, 234, 12415–12421. [Google Scholar] [CrossRef]
- Kuenstner, L.; Kuenstner, J.T. Mycobacterium avium ssp. paratuberculosis in the Food Supply: A Public Health Issue. Front. Public Health 2021, 9, 647448. [Google Scholar] [CrossRef]
- Zupančič, K.; Skok, K.; Repnik, K.; Weersma, R.K.; Potočnik, U.; Skok, P. Multi-locus genetic risk score predicts risk for Crohn’s disease in Slovenian population. World J. Gastroenterol. 2016, 22, 3777–3784. [Google Scholar] [CrossRef]
- Urlep, D.; Blagus, R.; Orel, R. Incidence Trends and Geographical Variability of Pediatric Inflammatory Bowel Disease in Slovenia: A Nationwide Study. Biomed. Res. Int. 2015, 2015, 921730. [Google Scholar] [CrossRef] [Green Version]
- Zhao, M.; Gönczi, L.; Lakatos, P.L.; Burisch, J. The Burden of Inflammatory Bowel Disease in Europe in 2020. J. Crohn’s Colitis 2021, 15, 1573–1587. [Google Scholar] [CrossRef]
- Mihajlovic, B.; Klassen, M.; Springthorpe, S.; Couture, H.; Farber, J. Assessment of Sources of Exposure for Mycobacterium avium subsp. paratuberculosis in Food and Water. Int. Food Risk Anal. J. 2011, 1, 1–22. [Google Scholar] [CrossRef] [Green Version]
- Waddell, L.; Rajić, A.; Stärk, K.; Mcewen, S.A. Mycobacterium avium ssp. paratuberculosis Detection in Animals, Food, Water and Other Sources or Vehicles of Human Exposure: A Scoping Review of the Existing Evidence. Prev. Vet. Med. 2016, 132, 32–48. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitchell, R.M.; Medley, G.F.; Collins, M.T.; Schukken, Y.H. A meta-analysis of the effect of dose and age at exposure on shedding of Mycobacterium avium subspecies paratuberculosis (MAP) in experimentally infected calves and cows. Epidemiol. Infect. 2012, 140, 231–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kravitz, A.; Pelzer, K.; Nammalwar, S. The Paratuberculosis Paradigm Examined: A Review of Host Genetic Resistance and Innate Immune Fitness in Mycobacterium Avium Subsp. Paratuberculosis Infection. Front. Vet. Sci. 2021, 8, 721706. [Google Scholar] [CrossRef] [PubMed]
- Fecteau, M.E. Paratuberculosis in cattle. Vet. Clin. N. Am. Food Anim. Pract. 2018, 34, 209–222. [Google Scholar] [CrossRef] [PubMed]
- Begg, D.J.; Whittington, R.J. Experimental animal infection models for Johne’s disease, an infectious enteropathy caused by Mycobacterium avium subsp. Paratuberculosis. Vet. J. 2008, 176, 129–145. [Google Scholar] [CrossRef]
- Van Roermund, H.J.W.; de Koeijer, A.A.; Velthuis, A.G.J.; Weber, M.F.; Saatkamp, H.W.; de Jong, M.C.M. Quality Assurance Program for Paratuberculosis; Reports of the Animal Sciences Group; Animal Sciences Group: Lelystad, The Netherlands, 2004. [Google Scholar]
- Barkema, H.W.; Orsel, K.; Nielsen, S.S.; Koets, A.P.; Rutten, V.P.M.G.; Bannantine, J.P.; Keefe, G.P.; Kelton, D.F.; Wells, S.J.; Whittington, R.J.; et al. Knowledge gaps that hamper prevention and control of Mycobacterium avium subspecies paratuberculosis infection. Transbound. Emerg. Dis. 2017, 65, 125–148. [Google Scholar] [CrossRef] [Green Version]
- Gill, C.O.; Saucier, L.; Meadus, W.J. Mycobacterium avium subsp. paratuberculosis in Dairy Products, Meat, and Drinking Water. J. Food Prot. 2011, 74, 480–499. [Google Scholar] [CrossRef]
- Gerrard, Z.E.; Swift, B.M.C.; Botsaris, G.; Davidson, R.S.; Hutchings, M.R.; Huxley, J.N.; Rees, C.E.D. Survival of Mycobacterium avium subspecies paratuberculosis in retail pasteurised milk. Food Microbiol. 2018, 74, 57–63. [Google Scholar] [CrossRef]
- Paolicchi, F.; Cirone, K.; Morsella, C.; Gioffré, A. First Isolation of Mycobacterium avium subsp paratuberculosis from Commercial Pasteurized Milk in Argentina. Braz. J. Microbiol. 2012, 43, 1034–1037. [Google Scholar] [CrossRef] [Green Version]
- Botsaris, G.; Swift, B.M.C.; Slana, I.; Liapi, M.; Christodoulou, M.; Hatzitofi, M.; Christodoulou, V.; Rees, C.E.D. Detection of Viable Mycobacterium avium subspecies paratuberculosis in Powdered Infant Formula by Phage-PCR and Confirmed by Culture. Int. J. Food Microbiol. 2016, 216, 91–94. [Google Scholar] [CrossRef] [PubMed]
- Liandris, E.; Gazouli, M.; Taka, S.; Andreadou, M.; Vaiopoulou, A.; Tzimotoudis, N.; Kasampalidis, I.; Mpaseas, D.; Fyliousis, G.; Poltrionieri, P.; et al. Evaluation of the Microbial Safety of Child Food of Animal Origin in Greece. J. Food Sci. 2014, 79, M362–M368. [Google Scholar] [CrossRef] [PubMed]
- Boulais, C.; Wacker, R.; Augustin, J.C.; Ben Cheikh, M.H.; Peladan, F. Modeling the Occurrence of Mycobacterium avium subsp. paratuberculosis in Bulk Raw Milk and the Impact of Management Options for Exposure Mitigation. J. Food Prot. 2011, 74, 1126–1136. [Google Scholar] [CrossRef] [PubMed]
- Stabel, J.R.; Lambertz, A. Efficacy of Pasteurization Conditions for the Inactivation of Mycobacterium avium subsp. paratuberculosis in Milk. J. Food Prot. 2004, 67, 2719–2726. [Google Scholar] [CrossRef] [PubMed]
- ACMSF. ACM/486: Heat Resistance of Mycobacterium avium subsp. paratuberculosis (MAP) in Milk at Pasteurisation Temperatures. In Proceedings of the Advisory Committee on the Microbiological Safety of Food 38th Meeting, London, UK, 19 September 2000; pp. 1–7. Available online: https://acmsf.food.gov.uk/sites/default/files/mnt/drupal_data/sources/files/multimedia/pdfs/ACM486.PDF (accessed on 16 June 2019).
- Fechner, K.; Dreymann, N.; Schimkowiak, S.; Czerny, C.P.; Teitzel, J. Efficacy of dairy on-farm high-temperature, short-time pasteurization of milk on the viability of Mycobacterium avium ssp. paratuberculosis. J. Dairy Sci. 2019, 102, 11280–11290. [Google Scholar] [CrossRef]
- Garcia, A.B.; Shalloo, L. Invited Review: The Economic Impact and Control of Paratuberculosis in Cattle. J. Dairy Sci. 2015, 98, 5019–5039. [Google Scholar] [CrossRef] [Green Version]
- Bedrač, M.; Bele, S.; Kožar, M.; Moljk, B.; Brečko, J.; Pintar, M.; Zagorc, B. Poročilo o Stanju Kmetijstva, Živilstva, Gozdarstva in Ribištva v Letu 2017 [Report on the State of Slovenian Agriculture, Food, Forestry and Fisheries in Year 2017]; Pintar, M., Ed.; Agricultural Institute of Slovenia, Ministry of Agriculture, Forestry and Food: Ljubljana, Slovenia, 2018; pp. 18–43. Available online: https://www.kis.si/f/docs/Porocila_o_stanju_v_kmetijstvu_OEK/ZP_2017_splosno__priloge_za_net_2.pdf (accessed on 27 March 2020).
- Kušar, D.; Ocepek, M.; Logar, K.; Pate, M.; Krt, B. Seroprevalence of Cattle Paratuberculosis in Slovenia in 2008 and a Comparison of Data from Current and Previous Studies. Slov. Vet. Res. 2011, 48, 39–44. [Google Scholar]
- Knific, T.; Kirbiš, A.; Gethmann, J.M.; Prezelj, J.; Krt, B.; Ocepek, M. Modelling Paratuberculosis Transmission in a Small Dairy Herd Typical of Slovenia Suggests That Different Models Should Be Used to Study Disease Spread in Herds of Different Sizes. Animals 2022, 12, 1150. [Google Scholar] [CrossRef]
- Knific, T.; Ocepek, M.; Kirbiš, A.; Lentz, H.H.K. Implications of Cattle Trade for the Spread and Control of Infectious Diseases in Slovenia. Front. Vet. Sci. 2020, 6, 454. [Google Scholar] [CrossRef] [Green Version]
- Palisade Corporation. @RISK: Software for Risk Analysis and Simulation; Palisade Corporation: Ithaca, NY, USA, 2019; Available online: https://www.palisade.com/ (accessed on 16 March 2020).
- Statistical Office of the Republic of Slovenia. Sistat Database. Available online: https://pxweb.stat.si/sistat/en/Podrocja/Index/85/agriculture-forestry-and-fishery (accessed on 6 June 2019).
- Agricultural Institute of Slovenia. Govedoreja v Sloveniji, GOVEDO.si. Available online: https://www.govedo.si/ (accessed on 10 June 2019).
- Palisade Corporation. User’s Guide @RISK Risk Analysis and Simulation; Palisade Corporation: Ithaca, NY, USA, 2016; Available online: https://www.palisade.com/downloads/documentation/75/EN/RISK7_EN.pdf (accessed on 16 March 2020).
- Rani, S.; Beaver, A.; Schukken, Y.H.; Pradhan, A.K. Modeling the Effects of Infection Status and Hygiene Practices on Mycobacterium avium subspecies paratuberculosis Contamination in Bulk Tank Milk. Food Control 2019, 104, 367–376. [Google Scholar] [CrossRef]
- Beaunée, G.; Vergu, E.; Ezanno, P. Modelling of Paratuberculosis Spread between Dairy Cattle Farms at a Regional Scale. Vet. Res. 2015, 46, 111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bates, A.; O’Brien, R.; Liggett, S.; Griffin, F. The Effect of Sub-Clinical Infection with Mycobacterium avium subsp. paratuberculosis on Milk Production in a New Zealand Dairy Herd. BMC Vet. Res. 2018, 14, 93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Kessel, J.S.; Karns, J.S.; Wolfgang, D.R.; Hovingh, E.; Jayarao, B.M.; Van Tassell, C.P.; Schukken, Y.H. Environmental Sampling to Predict Fecal Prevalence of Salmonella in an Intensively Monitored Dairy Herd. J. Food Prot. 2008, 71, 1967–1973. [Google Scholar] [CrossRef] [PubMed]
- Serraino, A.; Bonilauri, P.; Arrigoni, N.; Ostanello, F.; Ricchi, M.; Marchetti, G.; Bonfante, E.; Albonetti, S.; Giacometti, F. Quantitative Risk Assessment of Mycobacterium avium subsp. paratuberculosis Survival in Pasteurized Milk in Three Dairy Plants in Italy. Food Control 2014, 45, 120–126. [Google Scholar] [CrossRef]
- WHO/FAO. Risk Characterization of Microbiological Hazards in Food: Guidelines; World Health Organization: Geneva, Switzerland, 2009; Available online: https://apps.who.int/iris/handle/10665/44224 (accessed on 7 May 2018).
- EFSA Scientific Committee. Scientific Opinion on Risk Assessment Terminology. EFSA J. 2012, 10, 2664. [Google Scholar] [CrossRef] [Green Version]
- Okura, H.; Nielsen, S.S.; Toft, N. Modeling the Effect of Direct and Indirect Contamination of On-Farm Bulk Tank Milk with Mycobacterium avium subsp. paratuberculosis. Foodborne Pathog. Dis. 2013, 10, 270–277. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Symbol | Description | Probability Distribution | Source |
|---|---|---|---|
| Herd level prevalence (Si) | |||
| Herd level prevalence, best-case scenario (%) | [53] | ||
| Herd level prevalence, middle scenario (%) | [53] | ||
| Herd level prevalence, estimated scenario (%) | [53] | ||
| Within-herd level prevalence | |||
| Number of dairy cows per herd | [56] | ||
| Proportion of subclinically infected cows | [52,58]; expert opinion | ||
| Proportion of clinically infected cows | [52,58]; expert opinion | ||
| Milk production | |||
| Milk production per healthy cow (litres/day) | [56] | ||
| Proportion of milk produced per subclinical cow | [58,59]; expert opinion | ||
| Proportion of milk produced per subclinical cow | [60]; expert opinion | ||
| Milk contamination with MAP | |||
| MAP shedding in milk per subclinical cow (log CFU/litre) | [58,59]; expert opinion | ||
| MAP shedding in milk per clinical cow (log CFU/litre) | [58,59]; expert opinion | ||
| MAP from faeces per subclinical cow (log CFU/litre) | [59] | ||
| MAP from faeces per clinical cow (log CFU/litre) | [59] | ||
| Milk filter efficiency | [58,61]; expert opinion | ||
| MAP reduction with pasteurisation (log CFU) | [62] | ||
| Symbol | Description | Calculation |
|---|---|---|
| Herd status | ||
| Number of subclinically infected cows | ||
| Number of clinically infected cows | ||
| Number of healthy cows | ||
| Milk production | ||
| Milk per subclinically infected cow (litres/day) | ||
| Milk per clinically infected cow (litres/day) | ||
| Milk per herd (litres/day) | ||
| Milk contamination with MAP | ||
| Internal milk contamination (log CFU) | ||
| External milk contamination (log CFU) | ||
| Bulk tank raw milk contamination on farm level (log CFU) | ||
| Raw milk contamination on farm level (CFU/litre) | ||
| Pasteurised whole milk contamination on farm level (CFU/litre) | ||
| Silo milk contamination on dairy industry level (log CFU) | ||
| Pasteurised whole milk contamination on dairy industry level (CFU/litre) | ||
| the Threshold Value for the Number of Cows in a Small Herd | |||||
|---|---|---|---|---|---|
| 25 Cows | 36 Cows | Basic Mode l50 Cows | 75 Cows | 100 Cows | |
| Milk contamination | Mean (5th, 95th PC) | ||||
| (log CFU/L) | 0.53 (0.1, 1.45) | 0.48 (0.08, 1.37) | 0.46 (0.07, 1.31) | 0.43 (0.07, 1.28) | 0.43 (0.07, 1.28) |
| (CFU/L) | 175.28 (0, 28) | 166.55 (0, 24) | 164.75 (0, 22) | 132.12 (0, 20) | 136.53 (0, 20) |
| (CFU/L) | 0.001 (0, 0) | 0.001 (0, 0) | 0.001 (0, 0) | 0.0008 (0, 0) | 0.001 (0, 0) |
| scenario 1 (log CFU/L) | 0.11 (0.04, 0.21) | 0.09 (0.03, 0.18) | 0.08 (0.03, 0.16) | 0.07 (0.03, 0.14) | 0.06 (0.03, 0.12) |
| scenario 2 (log CFU/L) | 0.2 (0.1, 0.34) | 0.17 (0.08, 0.29) | 0.14 (0.07, 0.25) | 0.12 (0.06, 0.22) | 0.11 (0.06, 0.2) |
| scenario 3 (log CFU/L) | 0.26 (0.14, 0.42) | 0.21 (0.11, 0.36) | 0.18 (0.09, 0.31) | 0.15 (0.08, 0.27) | 0.14 (0.08, 0.24) |
| (CFU/L) | 0 (0, 0) | 0 (0, 0) | 0 (0, 0) | 0 (0, 0) | 0 (0, 0) |
| Human exposure | % | ||||
| Raw milk in a positive farm with >0 MAP CFU/L | 89.13 | 87.58 | 86.67 | 85.98 | 85.82 |
| Raw milk in a positive farm with >100 MAP CFU/L | 2.05 | 1.90 | 1.83 | 1.82 | 1.84 |
| Pasteurised milk in a positive farm with >0 MAP CFU/L | 0.09 | 0.09 | 0.08 | 0.06 | 0.06 |
| Pasteurised milk at the industry level with >0 MAP CFU/L | 0 | 0 | 0 | 0 | 0 |
| Likelihood of Exposure | Level of MAP CFU/L of Milk | Level of Risk | Level of Uncertainty | |
|---|---|---|---|---|
| Raw bulk tank milk in a MAP positive farm | Almost certain | High | High | Low to moderate |
| Pasteurised milk in a MAP positive farm | Unlikely | Low | Low | Low to moderate |
| Pasteurised milk at the dairy industry level (all three scenarios) | Rare | Insignificant | Negligible | Low to moderate |
| UHT milk at the dairy industry level | Insignificant | Insignificant | Negligible | Low |
| Exposure of the average Slovenian consumer | Possible | Low | Low | Moderate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Knific, T.; Ocepek, M.; Kirbiš, A.; Krt, B.; Prezelj, J.; Gethmann, J.M. Quantitative Risk Assessment of Exposure to Mycobacterium avium subsp. paratuberculosis (MAP) via Different Types of Milk for the Slovenian Consumer. Foods 2022, 11, 1472. https://0-doi-org.brum.beds.ac.uk/10.3390/foods11101472
Knific T, Ocepek M, Kirbiš A, Krt B, Prezelj J, Gethmann JM. Quantitative Risk Assessment of Exposure to Mycobacterium avium subsp. paratuberculosis (MAP) via Different Types of Milk for the Slovenian Consumer. Foods. 2022; 11(10):1472. https://0-doi-org.brum.beds.ac.uk/10.3390/foods11101472
Chicago/Turabian StyleKnific, Tanja, Matjaž Ocepek, Andrej Kirbiš, Branko Krt, Jasna Prezelj, and Jörn M. Gethmann. 2022. "Quantitative Risk Assessment of Exposure to Mycobacterium avium subsp. paratuberculosis (MAP) via Different Types of Milk for the Slovenian Consumer" Foods 11, no. 10: 1472. https://0-doi-org.brum.beds.ac.uk/10.3390/foods11101472