
Effective Demand Forecasting in Health Supply Chains: Emerging Trend, Enablers, and Blockers

Research Department, Pamela Steele Associates, Oxford OX2 7HT, UK
Logistics 2021, 5(1), 12; https://0-doi-org.brum.beds.ac.uk/10.3390/logistics5010012
Submission received: 18 December 2020
/
Revised: 10 February 2021
/
Accepted: 24 February 2021
/
Published: 28 February 2021
(This article belongs to the Special Issue Gaming Simulations in Health Care Logistics)
Abstract
:Health supply chains aim to improve access to healthcare, and this can be attained only when health commodities appropriate to the health needs of the global population are developed, manufactured, and made available when and where needed. The weak links in the health supply chains are hindering the access of essential healthcare resulting in inefficient use of scarce resources and loss of lives. A chain is only as strong as its weakest link, and demand forecasting is one of the weakest links of health supply chains. Also, many of the existing bottlenecks in supply chains and health systems impede the accurate forecasting of demand, and without the ability to forecast demand with certainty, the stakeholders cannot plan and make commitments for the future. Forecasts are an important feeder for budgeting and logistics planning. Under this backdrop, the study examines how improved forecasting can lead to better short-term and long-term access to health commodities and outlines market-related risks. It explores further how incentives are misaligned creating an uneven distribution of risks, leading to the inability to match demand and supply. For this purpose, a systematic literature review was performed, analyzing 71 articles from a descriptive and content approach. Findings indicate the emerging trends in global health and the consequences of inaccurate demand forecasting for health supply chains. The content analysis identifies key factors that can pose a varying degree of risks for the health supply chain stakeholders. The study highlights how the key factors emerge as enablers and blockers, depending on the impact on the overall health supply chains. The study also provides recommendations for actions for reducing these risks. Consequently, limitations of this work are presented, and opportunities are identified for future lines of research. Finally, the conclusion confirms that by adopting a combination of approaches, stakeholders can ensure better information sharing, identify avenues of diversifying risks, and understand the implications.
1. Introduction
Global health programs will accomplish their objectives only if the accessibility of health commodities improves, especially in low- and-middle-income countries (LMICs). Achieving this requires channelizing development aid and public finance for more and better health commodities to prevent and reduce the disease burden. A good health system will necessitate a supply chain that can deliver and guarantee affordable health commodities at the appropriate quality. Health supply chains not only deliver health commodities but also return information on demand, consumption, and shortages to the health planners. Supply chain management is a well-developed scientific discipline but has not been fully used in improving health supply chains in LMICs. As a result, supply chains that serve patients in LMICs remain weak and ineffective, putting treatment programs at risk, and weakening the overall health system’s ability to respond to the healthcare needs of the population [1,2,3]. Weaker links in global health supply chains including fragile last-mile delivery, human resource challenges, fewer opportunities for research and development, etc. are constraining the access to health commodities. These weak links in the health supply chains result in supply shortages, inefficient use of scarce resources, reluctance in understanding the needs of LMICs and unfortunately loss of lives in many cases.
One of the weakest links in global health supply chains is demand forecasting of health commodities. Many of the health supply chain bottlenecks impede accurate demand forecasting, and without the accuracy to forecast demand market viability, production capacity, and financial commitments become challenging. National governments and the international donor community rely on forecasts for budgeting while implementing partners and health programs depend on the forecasts to plan their health supply chain logistics. In a constantly evolving world, forecasting new health commodities become important, but extremely difficult due to lack of data and the uncertainty of how breakthrough healthcare technologies and products will be accepted by consumers [4]. The right information can prove vital to providing the proper care, products, and services; and health supply chains should aim to move beyond mere prediction to forecasting. As a critical element of the planning and implementation process forecasting, identify future events and thus can support supply chain functions
In decision-making process, forecasts could be considered the cornerstones to effective strategies, since data gathered can either enhance or thwart the organization’s survival. There are multiple models of forecasting, and the various stakeholder must seriously consider which approach will provide the best information and the right guidance towards implementing that information successfully. Also, the quality of forecasting tools impacts the ability to gather adequate data about the future demands and trends. The healthcare sector is continually evolving, which presents both opportunities and threats. It is difficult to standardize forecasting tools since health demands often differ due to factors such as patient experiences, resource allocation, disease burden, leadership, etc. Appropriate forecasting tools will determine projections based on identified business drivers, influencing factors, and business constraints [5].
The ongoing pandemic and the global health crisis have burdened health supply chains with significant disruptions, both in the upstream and downstream activities. Acute shortages, logistic challenges, and travel restrictions have added fuel to fire. Due to these disruptions, accurate short-term forecasts have become an important managerial tool for decision-making, and mid-term to long-term forecasting is critical for supply chain planning. Recent experiences suggest that immediate healthcare needs and patient buying behavior change with the progression of the pandemic. The bullwhip effect is evident which exacerbates the health supply chain bottlenecks [6]. Under this backdrop, the study examines how improved forecasting can lead to better short-term and long-term access to health commodities and outlines market-related risks. It also highlights how incentives are misaligned and provides recommendations for actions for reducing these risks and correct the misalignments.
2. Review of Literature
2.1. Early Literature on Forecasting
One of the earliest works in forecasting analyzed models to establish selection criteria for the most suitable model according to company needs [7]. Later, Mahajan and Wind (1988), suggested six areas to improve research and implementation of forecasting models [8]. Another relevant survey by Hardie, Fader, and Wisniewsky (1998) provided a comprehensive investigation of several leading published models in consumer-packaged goods [9]. Evidence also suggests that forecasting techniques can change depending on the level of technology used. Higher use of technology mainly used internal data for forecasting, while lower use of technology relied more on quantitative techniques such as customer surveys [10]. Ozer (1999) critically reviewed forecasting in respect to objectives, applicability to different products, data requirements, suitable environments, and time frames, and diagnosis [11]. Kahn (2002) presented exploratory research to describe the new forecasting effort, techniques, and accuracy [12]. Lawrence et al. (2006) explores judgmental forecasting, while Meade and Islam (2006) provided a progress review of forecasting of the diffusion of innovations [13,14].
Forecasting should be an important tool supporting the prediction of future events. Since the prediction needs vary, there is seldom one superior method that works for all organizations and systems. The impact of external factors can differ, and these factors that cannot be predicted or controlled often impact the forecast [15]. It is recommended that healthcare stakeholders endeavor to distinguish as many degrees of doubts as to the problem permits. This will yield a better understanding of which information is relevant and useful. Forecasting has its own sets of benefits and pitfalls, which require dedicated involvement from planners to maximize the benefits of forecasting.
2.2. Health Supply Chains
The supply chain is a critical component of health systems. The performance of the supply chain determines the ability of the health systems to provide affordable and high-quality healthcare services at all delivery points. This highlights the need to invest in robust and well-functioning supply chains. Numerous countries are focusing on improving health supply chain performance through supply chain transformation and allocating more resources to the health system [16]. The concept of supply chain management has also gained momentum in the field of healthcare as a tool for increasing productivity and improving quality [17]. In particular, public healthcare organizations, which represent a significant part of the healthcare delivery system, have been involved in a series of innovative projects that address the supply chain of purchasing and logistics. This has especially received increased attention due to the pressure to improve the performance of public services [18]. Early evidence from the literature suggests possible cost-saving opportunities when supply chain practices are embedded in healthcare. For example, outsourcing of inventory management creates cost savings without deviating from quality standards, the applicability of JIT (just-in-time) models in healthcare settings, etc. [19,20].
The application of supply chain management concepts is even more relevant in an LMIC context, since unlike the advanced nations, where health supply chains are supported by private sectors, in LMICs the public and private sectors coexist creating interconnected flows [21]. The most common mode of managing health supply chains in LMICs is through the Central Medical Stores, although donors have also created vertical supply chains to handle the distribution of essential medicine and related services. These independent supply chains, which are either program-specific or disease-specific often run in parallel with the national distribution system as seen in many LMICs. The complexity of LMIC health supply chains creates inefficiencies and makes them vulnerable to many challenges. The various challenges can include stock-outs, corruption, product diversion, poor last-mile delivery, etc. leading to reduced health outcomes. This is exacerbated by the lack of accountability and fragmented leadership, making it easier to pass on the blame and create strong incentives for corruption [22].
In global health, supply chain management can be a daunting task involving forecasting, price negotiations, last-mile distribution, and maintain trained healthcare logistic staff. The wide array of relationships, stakeholders, products, and requirements make the health supply chain highly complex, intricate, and dynamic [23]. It supports the flow of three essential flows namely materials, information, and finances. Over time the concept of supply chain management in healthcare has emerged to incorporate a scope beyond traditional logistics functions and include requirements such as capacity building, customer service, etc. [24].
2.3. Forecasting in Health Supply Chains
Demand forecasting, in a health supply chain context, is defined as the continuing process of projecting which health commodity will be purchased, where, when, by whom, and in what quantities [25]. Forecast help understands the health commodity needs that have been met or will have a purchasing power resulting in actual orders [26]. Effective demand can act as an indicator for assessing the actual need for essential health commodities at the facility level and end-user level. After determining which diagnostics and drugs will be stocked, key stakeholders will have to have a clear understanding of the short-term and long-term needs. In this case, forecasting is used to estimate the quantities of each product that a program will dispense to users for a specific period in the future. In a global health context, forecasting is usually done on an annual or semi-annual basis to align with the program objectives and procurement needs.
Decision-makers rely on information about demand at every stage of the health supply chain. Aggregate forecasting takes into consideration the total demand for health commodities in a market after considering factors such as price, availability of funding, use rates, etc. Although this is one of the many complex steps in the supply chain, it is integral to support evidence-based decision-making for all the stakeholders to improve accessibility and availability of healthcare. For health commodities, demand forecasting begins when the product is conceived during the research and development stage and continues through the product life cycle and the value chain [27]. Hence, the information on demand is very crucial to shaping future markets, especially developing markets characterized by uncertainties. Accurate mid-term and long-term forecasts will enable support in the design of robust and proactive health supply chains and deliver health benefits to the population [28]. Demand forecasting serves the following critical function in the market for global healthcare commodities.
- Demand forecasting allows manufacturers to invest in manufacturing capacity, ensuring supply matches the demand and take advantage of economies of scale.
- Forecasting helps identify demand gaps in the healthcare market and informs manufacturers and researchers allowing them to allocate resources to develop solutions for the existing gaps. This will facilitate the response of the healthcare community to LMIC needs and accelerate the pace of product availability.
- Forecasting supports local pharmaceutical manufacturing in LMICs, thereby strengthening health systems’ response to reducing disease burden and improving the quality of life.
- Forecasts help donors and the international community to allocate funds efficiently by ensuring appropriate prices and adequate supplies of health commodities.
- Forecasting can identify and highlight the demand- and supply-side constraints to guide policy and advocacy efforts. This can contribute towards broadening access and shaping future healthcare portfolio, especially in LMICs.
The demand forecasting that begins with the conceptualization of a product is continually adjusted through the lifecycle, to facilitate a successful launch and usage [29]. Forecasts for the various products in the pipeline are made based on the early characteristics and efficacy to support a research and development investment case for suppliers and funders.
Forecasting for healthcare commodities is unique since they are made in a dynamic environment, many years in advance of when a commodity might become available for use. At this stage, forecasts represent demand scenarios based on several assumptions. For health commodities such as vaccines, which have a particularly long development cycle, the uncertainty can be greater which will have direct consequences on the forecasts [30]. Strategic forecasts are in the process of continuous refinement through the lifecycle, with iterative feedback loops, reflecting the changes. Forecasts evolve with product maturity and market maturity. Forecasts are useful at all levels of the health system and are used by local facilities, regional hubs, central ministry, private sector, international donors, procurement agents, delivery agents, etc. Supply chain forecasts depend heavily on the accuracy of country and local buyer forecasting activities. Given the importance of forecasting for robust health supply chains, it is surprising that it is still a problem in global health. A primary reason could be the sudden improvement in funding and availability of an array of health products and services, without the corresponding improvement in forecasting techniques. Also, the risk allocation in the global health market is distributed unequally across key stakeholders, leading to a misalignment towards the health outcomes [31].
Although demand forecasting is not a new challenge, the need for better forecasting has become imperative in the context of the current efforts to increase access to health commodities under the backdrop of the pandemic. Crucial decisions on which vaccine, medicine, and diagnostics to produce and to buy depend on the realistic projections of the future [32]. Ambiguous forecasts can impact outcomes leading to limited funds and shortages across the health supply chains. However, the most important consequences are on health, endangering lives, and adding to the threat of drug resistance [33].
The economic costs for poor demand forecasting are also high. The business case for manufacturer’s participation in LMICs can be weakened, having an impact on the access to health commodities, which has been cited as a critical factor affecting pharmaceutical companies’ role in serving the global health needs [34]. In short, better demand forecasting is at the heart of the global health agenda, and hence merits attention from all stakeholders involved in planning, budgeting, and engaging in logistic activities across the health supply chains. Traditionally, demand forecasting for health commodities was a relatively isolated function in LMICs, which was limited to only the firms with business interest, using some basic health information and health system coverage [35]. LMICs also suffer from poor forecasting skills of health supply chain professionals which require better allocation of resources for capacity building and development [36]. Poor demand forecasting is a key driver of stock-outs and raises the risk that substandard medicines entering the health system [37]. Because substandard medications may not be strong enough to effectively treat patients or protect them from illness, their use increases the risk of mortality and drug resistance.
More recently, with the increased attempts to align economic growth with sustainable development, there has been a greater emphasis on channelizing funds and resources to improve access to health commodities and design robust health supply chains. There has been a considerable increase in the funding and aid for improving health systems, especially in LMICs across the health supply chains. The World Health Organisation (WHO) has taken the responsibility for developing the demand forecasts for some health commodities and likewise, there has been good progress in the public–private partnerships as well [38]. However, little has been done to overcome challenges in health supply chain data management and institutional incentives that constrain robust decision-making [39].
2.4. Risks Associated with Forecasting
The forecasting challenges can be understood only by looking at the nature and extent of risks faced by various stakeholders of the health supply chains [40]. The risks are shaped by emerging features such as shifting disease burdens, complex international markets, dynamic patient needs, new products, and advanced health technologies, etc. The asymmetry of these risks can create missed opportunities for health supply chain stakeholders and hamper access to healthcare [41].
The relationship between demand forecasting and risks is multi-dimensional. Accurate forecasting for health commodities becomes difficult because of the inherent risks in health commodities and the associated supply chain activities. Also, inaccurate forecasts can aggravate the risks for those buying and selling health commodities in the market, and for those planning to enter and invest in the same market. This will have direct and indirect consequences on the patient’s health and ongoing interventions [42].
The supply-side risks are associated with the development and manufacturing of the health commodity. First, the scientific pathway to developing and launching a health commodity can be fraught with uncertainty. Public–private partnerships can support reducing this risk through diversification [43]. However, this is difficult to achieve and the manufacturers often bear the risks alone. Second, production batches may fail tests for efficacy and safety due to failure in components, systems, or human error. This can affect demand forecasting in the healthcare market and the risk is borne by the manufacturer. Third, inelasticity of supply of inputs dependent on agriculture, weather, and other market risks can influence demand forecasting of health commodities [44].
The demand-side factors are related to the use of healthcare commodities and the likelihood that a commodity will be attractive to those who need it. First, health commodities developed to solve specific health needs often face little competition and enjoy a period of exclusivity [45]. However, where alternatives are available, it will impact the demand for health commodities which need to be considered while forecasting demand. Awareness about the size and characteristics of the potential market could overcome this risk. Second, changing preferences, shifting disease burdens, and inherent characteristics can render health commodities obsolete [46]. This is a particular problem if manufacturing assets are specific to a product facing the risk of obsolescence.
Thirdly, demand forecasting of healthcare commodities depends on exogenous factors such as the availability of data on disease burden, cultural and demographic influences, etc. Fourthly, weak budgets and budgetary constraints can impact contractual obligations, especially in a resource-constrained set-up. This vulnerability will impact the demand forecasting thereby creating gaps in the scientific and financial pipeline. The uncertainty in grant approval, complexity of the disbursal cycles, and the sustainability of funding health commodities are unique risks embodying health supply chains [47]. Funders commit to a particular funding stream, under transparent rules, over a multi-year period. Fifthly, price fluctuations will force healthcare commodities’ prices to behave differently than expected. Also, prices are governed by the purchasing power and negotiating skills of key stakeholders.
Cross-cutting factors such as regulatory frameworks, weak enforcement, and supply chain disruptions convey significant risks, especially in an LMIC environment. Regulatory agencies may be poorly defined and unpredictable. This can cause inadequate enforcement and make the health system susceptible to fake and poor-quality health commodities and crowding out good quality products and services. Supply chain disruptions such as delivery bottlenecks, poor inventory management resulting in shortages or surplus, and the shortfall in complementary resources such as human resources, infrastructure, etc. at the required time and location can hinder forecasting and supply chain planning. Aiming to achieve more transparent regulations and well-organized investments in strengthening health supply chains can support overwhelm these cross-cutting challenges.
From reviewing the literature, the research gap is apparent. The following main research contributions are presented to close some of these gaps in the study of demand forecasting in health supply chains. The presented paper contributes to investigating the enablers and blockers to forecasting in health supply chains. Furthermore, the paper also highlights how incentives are misaligned and recommends strategies for correcting these misalignments and reducing the risks. Table 1 illustrates the novelty of the research. The listed studies aimed to verify if the concept of forecasting risks and misalignment of incentives in health supply chains have been investigated earlier. The table highlights that although we have had different combinations of studies, there is no evidence to suggest that the objectives of the current study have been examined earlier.
3. Methodology
In this section, the research methodology is defined, and the steps taken are described in the following subsections.
3.1. Sources of Information, and Inclusion and Exclusion Criteria
To support the purpose of the study, a systematic literature review was chosen to be conducted, since it reduces bias in the research process, by precisely defining inclusion and exclusion criteria for the selection of articles [59]. The systematic literature review process began by choosing the databases for research. The databases that were chosen are ScienceDirect, Elsevier, Google Scholar, Wiley, Springer, and Centre for Global Development, which provides excellent peer-reviewed journals. Additional sources such as book chapters, conference proceedings, and industrial reports were also considered. Secondly, the period for analysis was determined. Since, the area of research included the broad areas of health, supply chain management, and forecasting the study included evidence from 1974 to 2020. The study includes documents written in English only.
3.2. Keyword Definition and Search
To find the associated articles focusing on forecasting in the health supply chain, the databases search began by article title containing the combination of words: “Health supply chain”, “Pharmaceutical supply chain”, “Demand forecasting”, and “Global health”. An asterisk sign was included at the end of the to address any sets of combinations. As a result, 486 articles were found. The next validation step was to examine the 486 articles’ title, abstract, and keywords section, for specific words related to developing countries, which included a variety of associated and combined keywords. Filters were employed to remove duplicate papers and papers that were not relevant to demand forecasting in the health supply chains. This helped in refining the final selection of papers resulting in 94 literature articles.
3.3. Articles Review and Selection
Subsequently, the search was restricted to carefully read and review each of the 94 articles: Title, keywords, abstract, and entire article content, focusing on the combination of forecasting, risks, and incentives in the health supply chains, following the inclusion and exclusion criteria, and considering the relevance of each paper to the purpose of this article, to guarantee pertinence of the study. As a result, a total of 71 papers were identified for this literature review. It is important to highlight that the main characteristics of the 23 papers taken out on this last step included: lack of focus on health supply chains, papers not related to the critical subject of forecasting and associated risks, and documents not meeting the inclusion or exclusion criteria. Therefore, out of 486 papers found, 71 articles are related to demand forecasting in the health supply chain, contributing to 15% of the total papers.
3.4. Articles and Results
In this step, the 71 chosen articles were analyzed and classified according to different categories based on their characteristics and content. First, the descriptive analysis included: Year of publication, the primary area of focus, and research methodologies being used. Second, the content analysis included the emerging themes in public health and the consequences of inaccurate demand forecasting for health supply chains. Therefore, the results of the descriptive and content analysis provide the basis for the following research steps—the identification of factors that act as key enablers and blockers for health supply chain forecasting.
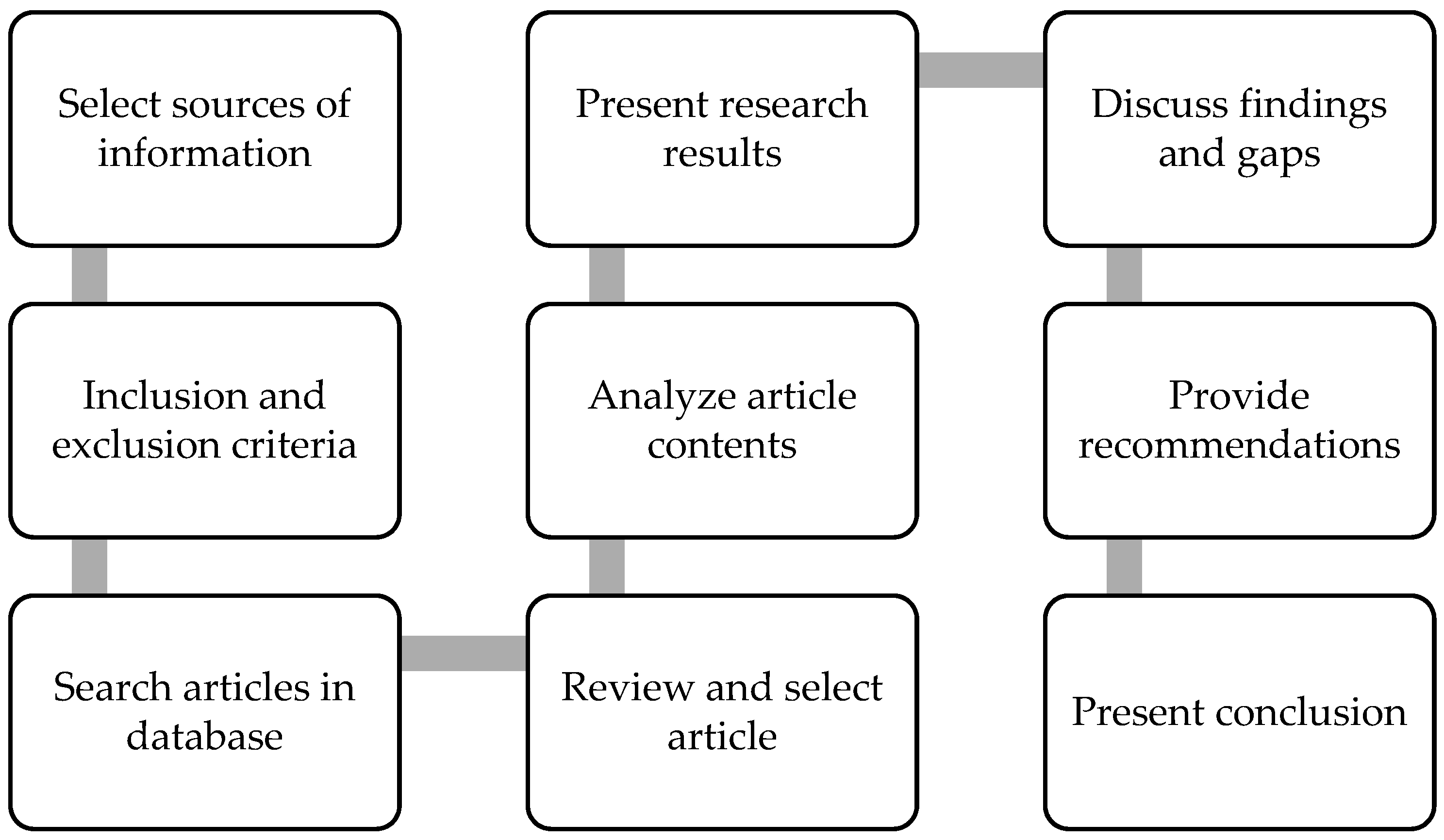
The closing part of the methodology consists of presenting the discussion on the research findings, gaps, and limitations, as well as future research recommendations followed by the conclusion. Figure 1 shows the sequence of steps taken for this research methodology.
4. Results
The results integrate the descriptive and content analysis of the 71 articles. The descriptive analysis consists of identifying and classifying the articles by publication year, the primary area of focus, and research methodologies. The content analysis focuses on the emerging themes in public health, and the consequences of inaccurate demand forecasting for health supply chains.
4.1. Descriptive Analysis
This subsection presents the descriptive analysis, statistics, and insights on the 71 articles of the study. The information is analyzed by the year of publication, the primary area of focus, and research methodologies.
4.1.1. Analysis of Articles by Year of Publication
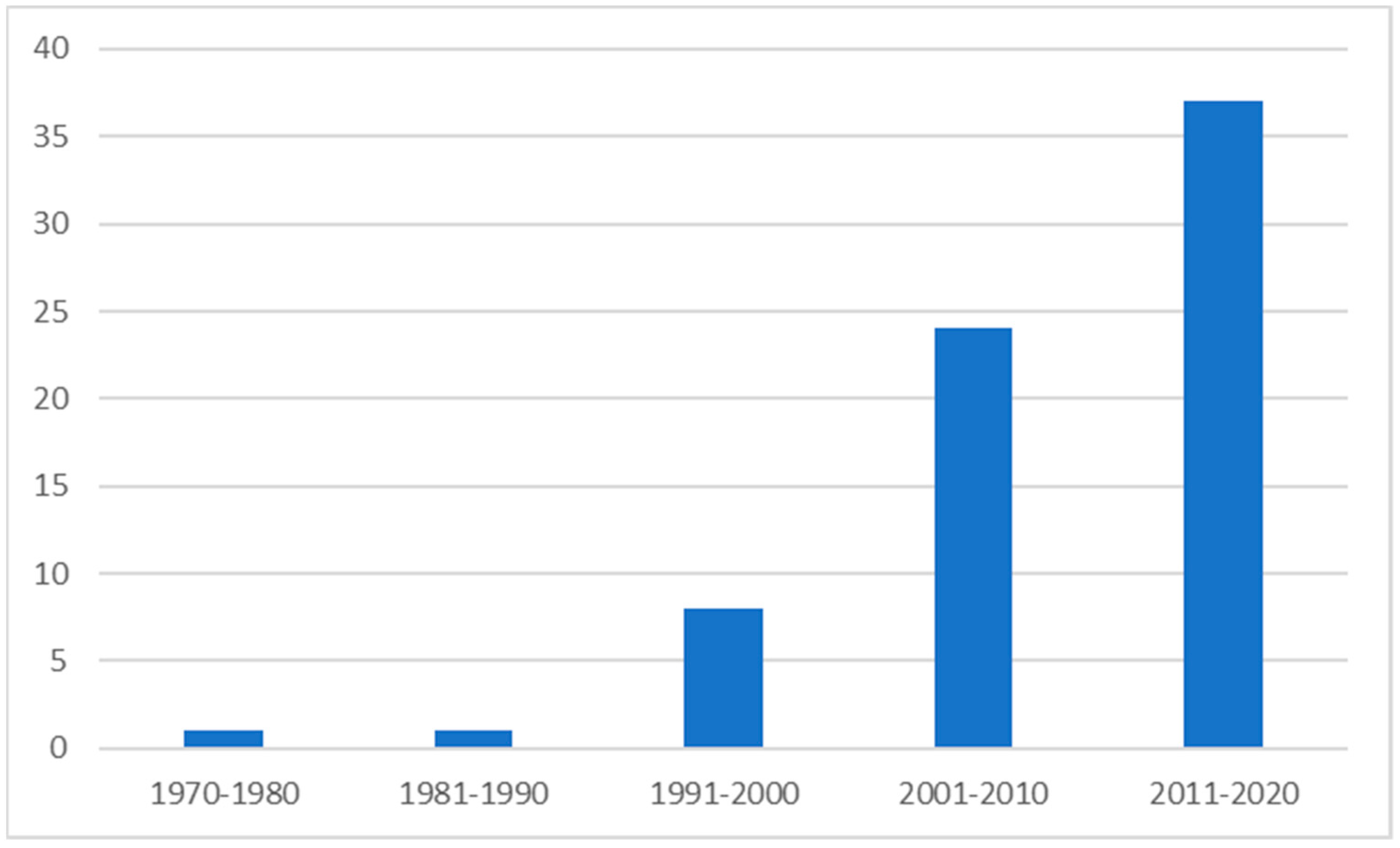
Figure 2 illustrates the distribution of the 71 articles. As shown, there is an increase in the publications related to health supply chain forecasting and associated risks in the period of investigation, indicating a growing interest in the area. The earliest evidence is seen in the 1970s and 1980s each representing initial literature on forecasting and its various applications in social sciences. In the following decade (1990–2000), there has been an increase in research focusing on forecasting techniques in supply chain management. This emphasized various aspects such as the use of forecasting for improved information sharing, enhancing new product trials, and managing supply chain pitfalls [1,9,60]. The analysis further reveals an increase in the area of research centering forecasting in healthcare and supply chain management. These sources highlighted the importance of forecasting for stakeholder collaboration, strategic procurement, strengthening healthcare logistics, and supporting innovation and its scale-up [14,18,20,48,61]. Some authors also explore forecasting in context to international aid, access to essential health commodities, and embracing supply chain practices in healthcare management [19,49,62]. Emphasis was also given to understanding the importance of forecasting in 9global health and there was an early foray into understanding the risks associated with forecasting in the global health context [25,27,42]. Only one paper by Yadav et. al., (2007) investigated the stakeholder incentives in the supply chain Artemisinin Combination Therapy (ACT) Treatments [50]. 52% of the articles reviewed were published between 2011 and 2020 indicating an exponential growth in the research in health supply chain forecasting and associated risks. The sources included understanding the role of forecasting in supply chain collaboration for transparency; supply risks and asymmetric cost information; and stakeholders role in improving access to medicine through robust forecasting [51,52,53,54]. Hermes, et. al, (2020) and Wolfgang, et.al., (2017) studied the role of the digital transformation of the healthcare industry, while Jbaily et.al., (2020) explored mathematical modelling for designing efficient drug supply chains [16,40,41]. There was also an increased interest in applying forecasting techniques during a pandemic and vaccine development [28,30]. However, none of the papers delved deeper into the misalignment of incentives for the various stakeholders.
4.1.2. Analysis of Articles by Primary Area of Focus
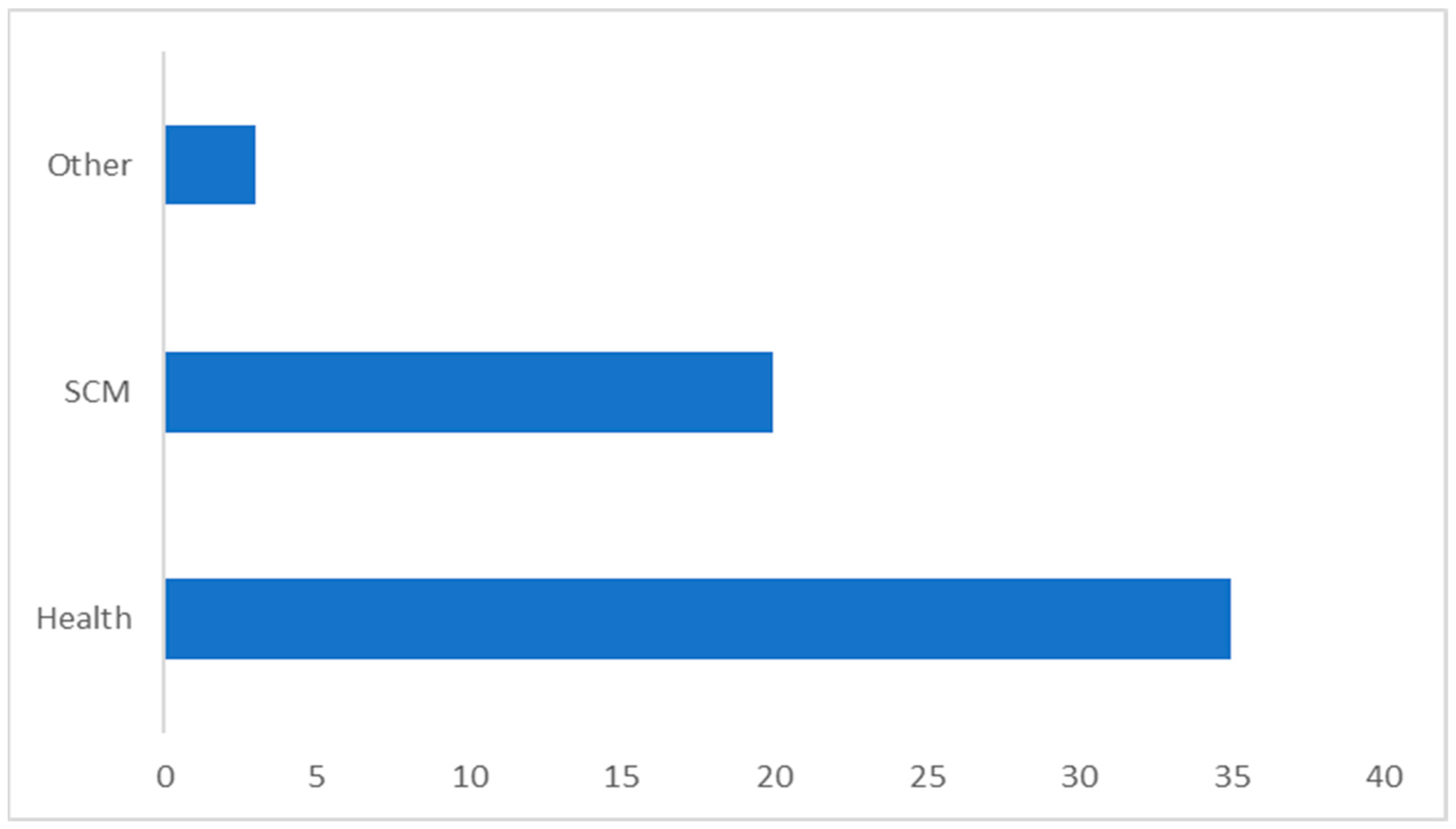
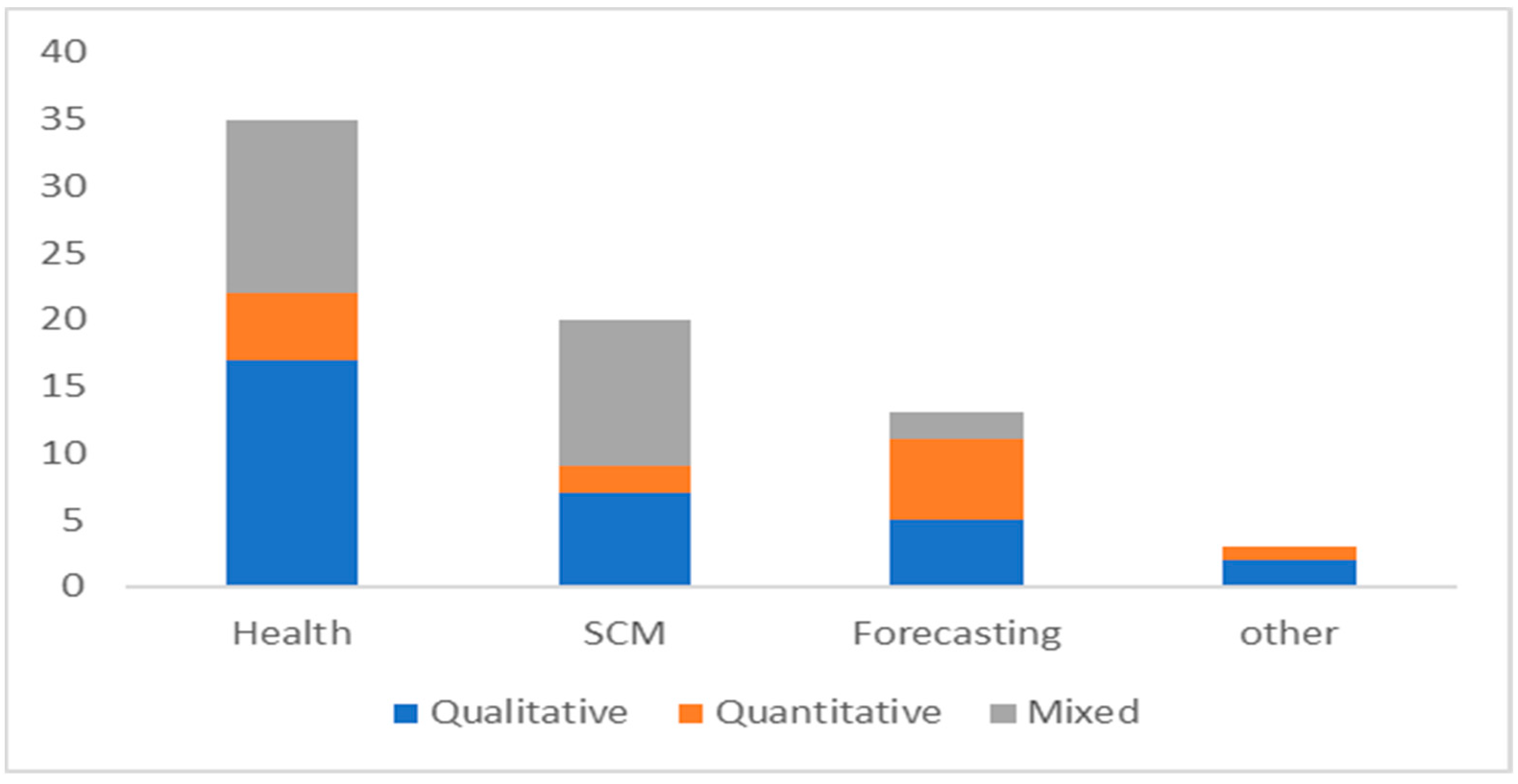
Figure 3 shows the distribution of the articles reviewed by the primary area of focus. As observed, out of the 71 articles, 35 articles (49%) are focused on global health, followed by 20 articles (28%) on supply chain management; 13 articles (18%) on forecasting; and the remaining of the papers 3 (4%) include diverse focus areas including technology and international aid.
The papers on health highlighted divergent themes including socioeconomic disparities in health; risk and uncertainty, healthcare logistics, and demand for global health products [20,31,38,42]. Interestingly, access to vaccine technologies in developing countries was explored by Milstien, et.al., (2007) and Mackintosh et.al., (2018) studied health sector procurement as developmental linkages in a resource-constrained set-up [34,62]. Nuances of healthcare forecasting were probed by Stark, et.al., (2008), which was further analyzed in context to medicine stock-outs by Sued, et.al., (2011) [3,5]. Other areas of global health that emerged in the review include the rise of public–private partnership in drug development and related areas of the healthcare landscape, mapping WHO’s building blocks and supply chain functions, and the role of local manufacturing in designing robust health supply chains [36,43,45,63].
The literature on supply chain management mainly focused on examining ways to overcome supply chain challenges, understanding the appropriate supply chain design, dynamics of the supplier–retailer channels, and healthcare logistics [1,17,55,64]. Wang and Disney (2016) prodded the bullwhip effect and Seidman and Atun (2017) tried to answer if changes to supply chains and procurement processes yield cost savings and improve the availability of pharmaceuticals, vaccines, or health products [6,56]. Shen, et.al., (2019) reviewed supply chain contracting with information considerations, and Chen, et.al., (2020) examined contract types under correlated supply risks and asymmetric cost information [52,65]. The earliest papers on forecasting discussed the forecasting techniques applied for new product development and provided a new direction for research and implementation [7,8]. Matthews (2005) deliberated the significance of forecasting on public procurement and Meade and Islam (2006) evaluated how forecasting supported the diffusion of innovation [14,18]. Kasapoglu (2016) delved into the selection of forecasting models in healthcare and Nikolopoulos et.al., (2020) discussed forecasting and planning during a pandemic [15,28].
4.1.3. Analysis of Articles by Research Methodology
Figure 4 shows the distribution of research articles by the research methodologies used to analyze forecasting in health supply chains. 31 articles (44%) used qualitative tools to conduct research, of which 17 articles (55%) had a primary focus on health, 5 articles (23%) had a focus on supply chain management, and 13 articles (16%) focused on forecasting. The qualitative tools included observations, use of a variety of interviews, focus groups, etc. to understand stakeholder engagement, access to medicine, risks in health partnerships, health supply chain challenges, and trends of health spending in LMICs [3,48,50,66,67]. In the supply chain management context, qualitative tools helped explore healthcare logistics, public–private partnerships, and diagnosis of the root causes of underperformance of health supply chains [17,22,68].
14 articles (20%) used quantitative tools to conduct research, of which 5 articles (36%) had a primary focus on health, 2 articles (14%) had a focus on supply chain management, and 6 articles (43%) focused on forecasting. The quantitative tools used in the studies helped analyze numerical data to find patterns and averages, make predictions, test causal relationships, and generalize results to wider populations. In health the tools were employed to support scale-up of healthcare innovations, forecast healthcare needs, modelling of drug supply chains, and understand the impact of long development cycle on forecasts [5,16,30,61]. Quantitative tools also aided understanding buyback contracts, forecasting incentives, and how inelasticity of supply of inputs can influence demand forecasting of health commodities [44,64].
26 articles (37%) used mixed methodologies to conduct research, of which 13 articles (50%) had a primary focus on health, 11 articles (42%) had a focus on supply chain management, and 2 articles (8%) focused on forecasting. It is worth mentioning, most of the articles performed a literature review, which was used as a basis for research. There is a wide range of approaches by which to analyze the forecasting of health supply chains.
4.2. Content Analysis
The following subsubsections analyze the forecasting in health supply chains in context to the emerging trends, and associated risks being researched in the 71 articles.
4.2.1. Emerging Trends Influencing Global Health
Although demand forecasting for many health commodities is challenging, it is even more difficult when the healthcare landscape is inundated with new commodities, technologies, and sources of funds. This is more critical for LMICs since emerging trends in the global healthcare landscape can expose vulnerabilities of existing health systems and can have the greatest impact on health.
New Sources of Funds
The main sources of finance for health commodities in LMICs are private, out-of-pocket expenses, and public funds channelized through the Ministry of Health and parastatal agencies [61]. Although these sources have been increasing gradually, the expansion of the international donor funds has resulted in the discontinuation of these sources [57]. Hence, donor funding has become an important market-shaping factor in global healthcare. Donor funding has substantially increased for HIV/AIDS, tuberculosis, malaria, and vaccines. These new funds are being channelized through new mechanisms and new approaches are being launched.
The increase in funds and funders has had a significant impact on the demand forecasting of health supply chains. Donor funding is unpredictable and is driven by the motives of the funding agencies. Hence, this tends to be more fluctuating than the national health financing systems of LMICs [49]. Commitments are not aligned with disbursements and the funding can be stopped at any time if there are governance challenges. Hence, when health supply chains become more reliant on donor funding, which has been an emerging trend in global health, demand forecasting can become difficult. Moreover, the increase in demand due to an increase in indoor funding also needs huge investments to boost national and regional capacity. This necessitates a more robust national procurement, warehousing, and logistic infrastructure. These supply chain activities also need accurate forecasts to plan and justify investments.
An Array of New Health Commodities
The increase in the sources of funds for global health and the willingness to invest in research and development has paved way for new health commodities being developed and made available, even in the LMICs. The array of new products has many payoffs for health. However, this can create challenges for funders, intermediaries, and consumers who are used to having fewer health commodities at their disposal with well-established supply and procurement links [66]. The global community is hopeful of successful clinical trials of vaccines to defeat the COVID-19. It is a race against time to make vaccines available and accessible to all countries to overcome the challenges of the ongoing pandemic. This would mean that over the next few years, vaccines with significant value to global health are expected to be prequalified by WHO and enter health supply chains, which are already struggling the cope with the menace of the pandemic. In short, these are important milestones for the global health community. However, major logistic challenges, especially in a resource-constrained set-up needs to be addressed as well. Beyond this, the advancement of technology has resulted in new health commodities to be significantly different from the older generation versions. These differences have established the need for good demand forecasting across the health supply chains for all key stakeholders for a few reasons.
First, many of the health commodities are still on patent and their prices reflect the manufacturer’s need to recover the research and development costs. Consequently, the unit prices are higher, and advanced technology makes it difficult to produce low-cost generics [62]. Secondly, some of the health commodities have a lower shelf life and longer manufacturing cycles. At times, the active ingredients might also be dependent on agricultural processes. These factors can make demand forecasting critical and challenging at the same time.
Thirdly, stock-outs can interrupt patient treatment or lead to drug resistance in the community. Fourthly, many of the new commodities entering the healthcare market are now being funded for specific global health problems. Hence, manufacturers do not have access to lucrative markets and are unable to follow tiered pricing in multiple markets to recoup profits [58]. They are reliant on developing markets and hence forecasting will be essential to understand the pipeline of the fund flow. Lastly, many manufacturers especially in LMICs might find it difficult and/or impossible to apply for approvals through a regulatory authority [63]. However, WHO has set up a new prequalification system for the approval of drugs in LMICs.
New Customers
Additional and new sources of funds have introduced new buyers into the healthcare supply chain landscape. This has consequences for demand forecasting in terms of volumes and timing of purchases. This was seen in the grants provided by the Global Fund. The approach decentralized purchasing power to numerous national buyers including the public sector, non-governmental organizations, and faith-based organizations. The idea was to promote country ownership and strengthen national supply chains through capacity development. However, this approach created parallel supply chains a fragmented market of inexperienced buyers who had limited experience to influence and negotiate. Their decision-making, competing priorities, and governance issues are also not well understood by other stakeholders along the health supply chains. This makes demand forecasting difficult and establishing relationships of trust and transparency is impeded. This can also result in wide price differences of essential medicine across geographical locations. In contrast, GAVI’s approach aimed at establishing long-term procurement arrangements. Although this approach has clear benefits, it should also be supported by accurate medium-term to long-term demand forecasting.
Innovative Business Models
The healthcare markets are also being characterized by innovative business models as new suppliers enter the market. This necessarily does not ensure improved access to essential health commodities, as numerous regulatory bottlenecks and logistics challenges have made LMICs vulnerable to supplier’s production and delivery problems. An expansion of suppliers in LMICs can also have consequences for the security of supplies [56]. As with new buyers, new suppliers often lack expertise in demand forecasting and procurement approaches. Their motivations and challenges are not well understood and documented, which can weaken national health supply chains. In addition, the risks can be greater for the new suppliers, as they might not have deep pockets unlike international agencies to sustain the costs of poor demand forecasting. Poor demand forecasting can also impede the willingness of traditional mature suppliers to invest in production capabilities in developing markets. Also, the cost of doing business in LMICs tend to be higher due to supply chain complexities, country-specific requirement, and uncertainty of funding [22]. LMICs also suffer from parallel supply chains which have inundated the healthcare markets with counterfeits and poor-quality health commodities.
More Intermediaries
In addition to new buyers, suppliers, commodities, and funds, health supply chains have also seen the increased participation from new intermediaries—each playing a different role—although not in proper synchronization always. Health supply chains have now witnessed numerous private–public partnerships, to encourage more innovation and improved health outcomes [68]. These partnerships have been contributing to new product development which can demand forecasting both important and difficult.
4.2.2. Consequences of Inaccurate Demand Forecasting for Health Supply Chains
This section highlights the financial and human risks which accrue due to poor forecasting of health commodities. First, inaccurate demand forecasting can cause excess demand leading to a rise in prices (if not fixed), and the shortage will be felt across the various channels of the supply chain. This can have negative financial implications and have serious health ramifications in the form of untreated patients and vulnerable population. Also, the supplier may suffer from reputational damages, and interrupting treatment can also increase the disease burden. Secondly, erroneous forecasts can create an excess inventory which can block capital and create idle production capacity. Thirdly, if a supplier makes wrong demand predictions, the supplier is left with overcapacity in the long run which may result in costly contractual obligations and hidden costs. It will likewise impact prices and the willingness to participate in the market. Factors such as the willingness of the national programs, exiting interventions, approval of novel technologies, etc. This can force many manufacturers, especially in LMICs go out of business and make others anxious about future investments [48].
Fourthly, though suppliers aim to main lower prices for health commodities supplied to LMICs guided by corporate social responsibility, higher risks can force suppliers to increase the price of healthcare in LMICs. This often has deadly consequences for access to medicine and out-of-pocket expenditure. A successful strategy in this regard has been adopted by the Clinton Foundation HIV program, whereby better demand forecasts and longer-term purchasing agreements facilitate reducing risks and negotiations for lowering prices [69]. Fifthly, lower risks will encourage more participation and investments in scientific research and development. If pharmaceutical companies face uncertainties around demand in developing markets, their interest to develop products for these complex markets will be very low. There will less mobilization of funds and ill-functioning health supply chains will make access to healthcare more difficult. Lastly, the most serious public health impact is the loss of lives due to poor access to essential healthcare commodities, especially in rural and remote areas.
5. Findings and Discussion
Under the current arrangements, the consequences of risks are primarily faced by the manufacturers including the risk of shortages, overcapacity, and reputational damage. Although the patients and communities in LMICs face the risk of higher prices, inferior quality of health products, and long-term impact on physical and mental well-being. Consequences are only felt partially by funders and other intermediaries, who could reduce the different kinds of risks. These risks are also prevalent in developed markets.
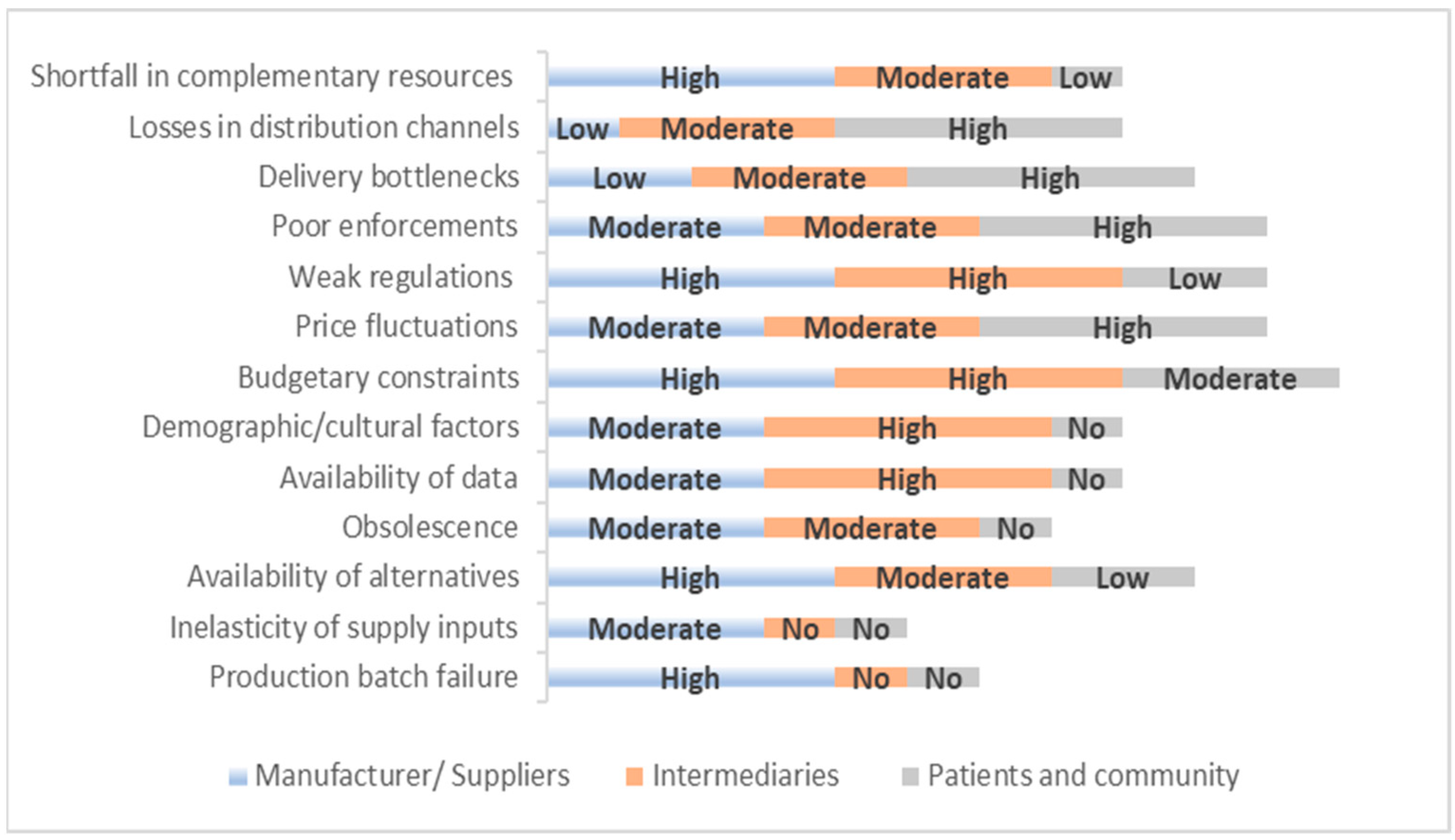
The content analysis has helped identify key factors that can pose a varying degree of risks for the health supply chain stakeholders. To provide a simpler understanding of the varying degree of risk, each factor is categorized into a level of risk (no risk to high risk) for the various stakeholders. After this, the level of risks is coded as follows—no risk is coded 1, low risk is coded 2, moderate risk is coded 3, and high risk is coded 4. The coding methodology helps in quantifying the degree of risk across the supply chain for the various stakeholders and provides a risk allocation map as shown in Figure 5.
The share of risks is not uniform for the key stakeholders across the health supply chains. The risk of production batch failure, availability of alternatives, budgetary constraints, weak regulations, etc. is a major risk impacting the manufacturers. The intermediaries constitute a network of various stakeholders and it is interesting to recognize the varying impact of the risks. The intermediaries are influenced highly by weak regulations (quality regulators, national buyers, funding agencies), budgets (funding agencies and national buyers), demography (procurement agents and logistic providers), and unavailability of data (procurement agents and logistic providers). Availability of alternatives and obsolescence creates moderate risks for procurement agents, logistic providers, and national buyers. Although the patients are negatively impacted by the risks of price fluctuations, poor regulatory enforcement, delivery bottlenecks, and losses in the distribution channels.
Figure 5 shows significant scope for risk-sharing between the various supply chain stakeholders in the healthcare landscape. If the manufacturers are expected to provide health commodities at lower prices to improve the accessibility of healthcare, it important that the other intermediaries also share the burden. If this approach is not adopted, then in the long run the stakeholders bearing risks disproportionately will either leave the market or engage in activities that could endanger the functioning of the health supply chains. This will have a trickle-down impact and can have significant consequences for the patients and the community at large [50].
However, higher levels of health spending and matured health supply chains have allowed stakeholders to safeguard against market fluctuations. A consistent flow of information with feedback loops has created a system of information sharing, wherein the various stakeholders have established collaborative arrangements and developed markets are characterized by risk-sharing [55]. However, in an LMIC context, unreliable data and limited resources cause fragmentation which can make demand forecasting difficult and more uncertain for various supply chain stakeholders to participate.
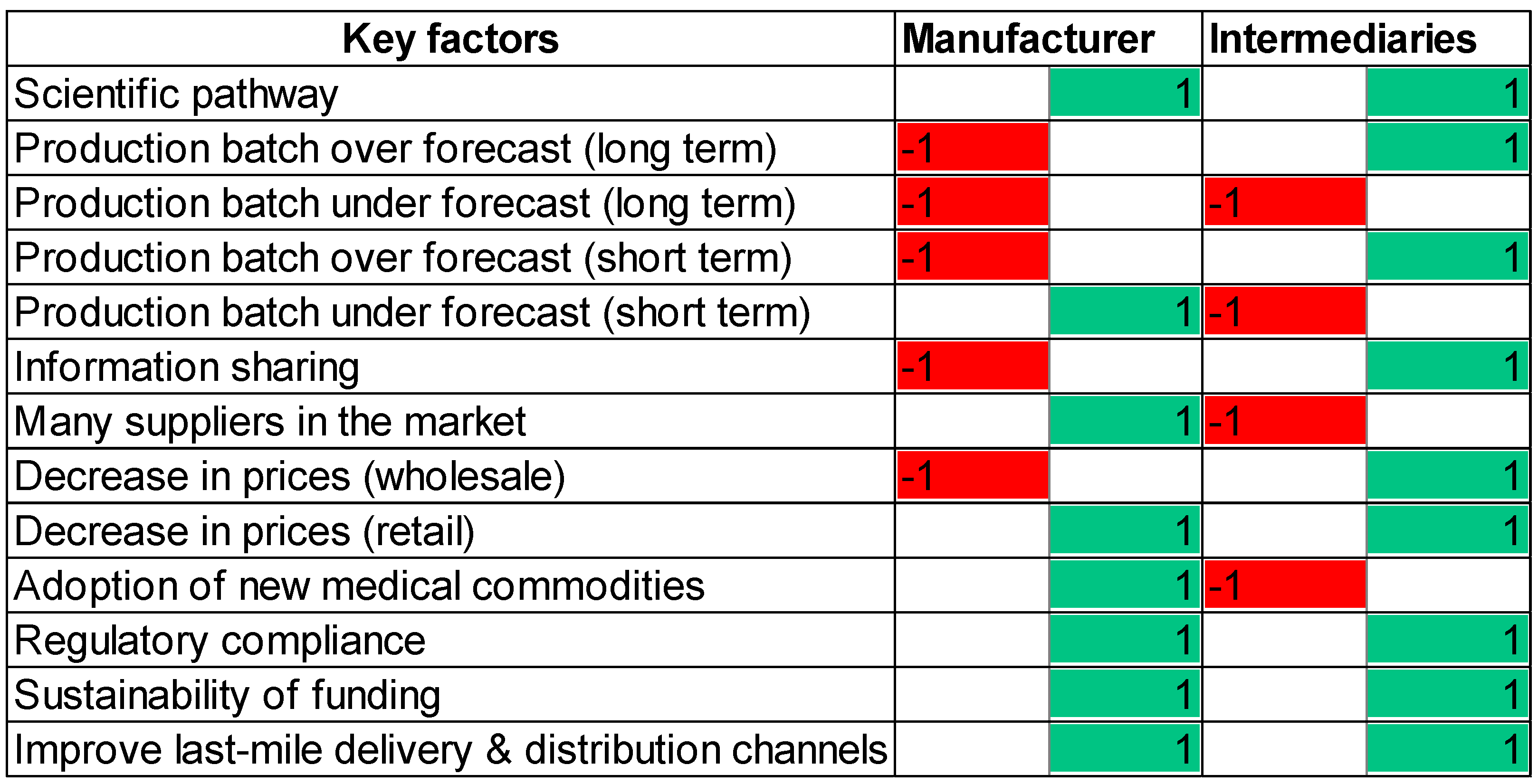
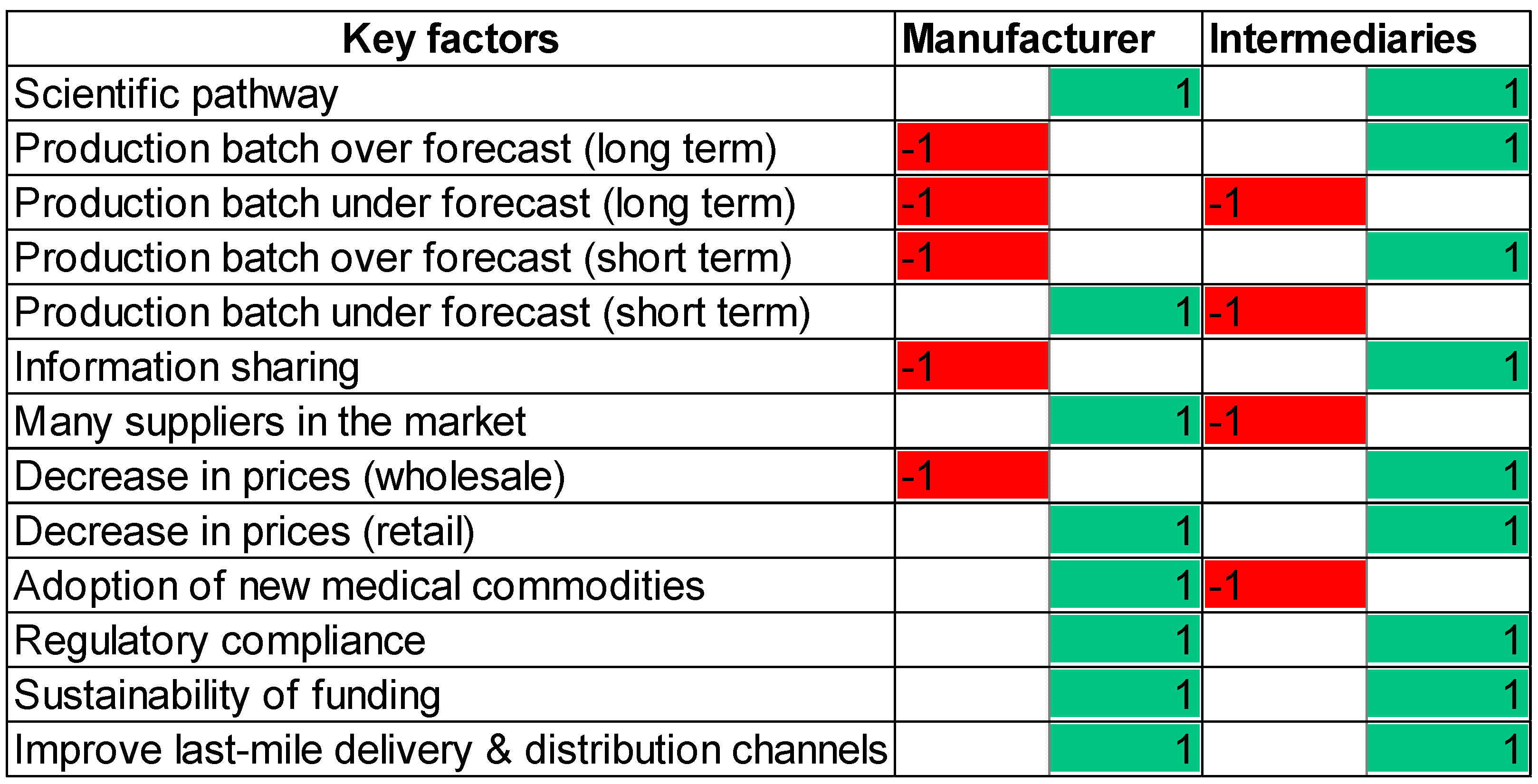
It is important for all health supply chain stakeholders to explore and understand the key factors, as identified by the content analysis. The factors present opportunities for improvement and challenges to overcome as well. Although the main goal of health supply chain forecasts is to improve access to essential healthcare commodities, the risks associated with it have led to several blockers and few enablers for the various stakeholders [53]. To add to the complexity, the various blockers experience a skewed distribution, which can act as a discouragement for a group of stakeholders vis-à-vis the other participants [54]. This asymmetry can create an unfavorable ecosystem for a group of stakeholders which could result in their reduced participation and/or exit from the market. Figure 6, a heat map, depicts how the key factors can either emerge as an enabler or a blocker for the key stakeholders. It is to be borne in mind that an enabler is not necessarily an inducement and a blocker a necessary deterrent. It depends on how these factors impact the overall health supply chains and their ability to enhance the availability of essential health commodities. To construct the heat map, the key factors were given either a value of 1 or −1 depending on it acting as an enabler or blocker.
A robust scientific pathway is an enabler for manufacturers and intermediaries. It creates a pipeline of health commodities and introduces more products into the health supply chains. The long-term over-forecast of the production batch is a blocker for the manufacturers due to the cost of overcapacity while it is an enabler for the intermediaries guaranteeing capacity from the supplier. On the other hand, the long-term under-forecast of the production batch is a blocker for all stakeholders. It creates the cost of shortfalls for the manufacturers and results in poor accessibility for intermediaries impacting health outcomes. The short-term over-forecast of the production batch is a blocker for manufacturers resulting in the opportunity cost of blocked resources, while the same is an enabler for intermediaries ensuring access to healthcare commodities and technologies. The short-term under-forecast of the production batch is an enabler for manufacturers creating capacity cost-saving opportunities, while the same can create shortfall costs for intermediaries.
Information sharing can make manufacturers vulnerable to competitors or antitrust legislation, whereas the same can make the intermediaries more aware of where health commodities can be obtained the shortest lead time. The presence of many suppliers in the market enables manufacturers with greater negotiating power, while it can be costly and time-consuming for intermediaries to build relationships, create information interfaces, and evaluate contracts. A decrease in the wholesale prices is a blocker for the manufacturer if no assurance lowering wholesale price will lead to a higher return. However, a decrease in the wholesale price is helpful for intermediaries as it lowers the costs of logistics and distribution. Nevertheless, a decrease in retail prices supports health supply chain stakeholders as it improves the demand for health commodities for manufacturers and facilitates better uptake of medical products initially.
Adoption of new medical commodities expands resource allocation for manufacturers while it can generate high switching costs for the intermediaries. Regulatory compliance supports better safety and expedites approvals for manufacturers, whereas it ensures efficacy and reduced wastage for the intermediaries. Sustainability of funding supports resources for research and expansion of capacity for the manufacturers, while assuring a continual flow of healthcare commodities. In addition, improving the last-mile delivery and distribution channels enable accurate demand planning for all the key stakeholders.
The heat map highlights how various scenarios can differing impacts and risks on the stakeholders of health supply chains. This maldistribution of risks and returns can make it difficult for small firms to survive in the market, especially in LMICs. It adds further uncertainties to short-term and long-term demand forecasts of the future, making it less attractive for new participants to enter the market.
6. Recommendations
The discussion so far has highlighted the various risks with demand forecasting, and how these risks are not equally distributed along with the health supply chain stakeholders. It is important the risks are reduced, nullified, and diversified to ensure the smooth functioning of health supply chains. Understanding the broader canvas of risks is critical to ensuring systematic elimination of the same and exploring opportunities to minimize the impacts. For instance, the risk of batch failures can be minimized through improved production systems, supply chain issues can be circumvented through contractual agreements, and transparent regulations can ensure better enforcement and compliance in the system [40]. Likewise, demand pooling and a culture of information sharing will make aid and budgeting more predictable, reducing monopsony, and guaranteeing purchase commitment will support negotiations, and commodity portfolio diversification can prevent obsolescence risks [67]. To add to these, sustained investment in advocacy and communication, and improved mobilization of resources can help reduce the risks in demand forecasting. We discuss some of these strategies in depth.
- To build the forecasting capacity, a clear understanding of demand forecasting must be embedded across all health supply chain systems, especially in a resource-constrained set-up. All agencies involved in health supply chain forecasting should adhere to standard principles to support decisions made based on the forecasts. This will support understanding the market dynamics and mitigate risks.
- It is universally accepted across the global health supply chain communities that better data, its management, and information sharing will yield accurate forecasts. The advantages of these accrue from two source-diversity of information provides a better idea of the supply chain constraints and preferences to the various stakeholders, and it can lead to confirmation effect [51]. One of the main reasons in global health supply chains for not embracing information sharing is the skewed distribution of incentives. As explored in the literature and examined in this study, risks across different stakeholders are not aligned to match the demand and supply of health commodities [60,64]. Information culture and politics act as the main hurdles prohibiting the exchange of information [70]. The establishment of an information intermediary can be an important step towards solving these issues. The intermediary will act as the central custodian of all forecasting activities. It will lead the data collection and analyzing phase, supported by market research and transparent baselines at the country and regional levels. This will ensure a continual practice of collecting and updating forecasting information.
- Risk allocation across the health supply chains can be achieved through effecting contracting practices. This can include a minimum purchase agreement, buyback contracts, revenue sharing models, and flexible quantity contracts [52,65]. It to be borne in mind that a single contracting type might not be suitable for all situations. A combination approach should be explored for better risk allocation and improved demand forecasting of health commodities.
- Private sector participation is becoming crucial for the successful implementation of health interventions and makes health commodities more accessible. Thus, the policy interventions in the public sector might not impact the private sector, until the major bottlenecks are removed.
Limitation and Future Scope
This paper presents limitations. The restriction of database access availability has limited the research and thus articles from other sources of primary importance could have been excluded from processing. The keywords used may not be all-inclusive; expanding search could provide a more comprehensive review of the topic. The review was carried out on 71 articles; therefore, the exploration of more articles could broaden the conceptualization and knowledge of empirical research, and issues currently addressed.
Research on forecasting in health supply chains is limited and current studies focus mainly on the challenges of designing robust health supply chains. Hence, there is a need to investigate deeper to identify the challenges of forecasting, since many of the major challenges in health supply chains are linked to unreliable forecasts.
Current research shows a gradual improvement in forecasting in health supply chains, but information on how risks are allocated, and incentives are aligned is limited.
Even though research on healthcare supply chain forecasting is available, perspectives of key stakeholders are needed, especially regarding the distribution of risk and rewards [71]. This includes components and raw materials suppliers, and logistics service provides, and end users. Therese are areas of research opportunity that may offer new avenues for future exploration.
7. Conclusions
The global health supply chain community’s ability to forecast demand for health commodities has not been at par with the desire of improving access to essential healthcare for those who need it the most. This is mainly due to the unequal distribution of risks across the participants of health supply chains, and these risks have direct consequences on the demand and supply of healthcare. Hence, not all participants have incentives aligned towards better forecasts for critical products and services. This has resulted in higher costs, frequent shortages, and the viability of investing in scientific research and development. This can be corrected by embedding demand forecasting as a crucial component of health supply chains and removing hurdles in the pathway of information sharing. Effective contracting methods would enhance stakeholder collaboration facilitating diversification of risks and improvements in the access to quality health commodities. The recommendation, when implemented will be able to save lives by improving demand forecasts at the global level and strengthening national health systems.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lee, H.L.; Billington, C. Managing supply chain inventory: Pitfalls and opportunities. Sloan Manag. Rev. Spring 1992, 33, 65–73. [Google Scholar]
- Kraiselburd, S.; Yadav, P. Supply chains and global health: An imperative for bringing operations management scholarship into action. Prod. Oper. Manag. 2013, 22, 377–381. [Google Scholar] [CrossRef]
- Sued, O.; Schreiber, C.; Giron, N.; Ghidinelli, M. HIV drug and supply stock-outs in Latin America. Lancet Infect. Dis. 2011, 11, 810–811. [Google Scholar] [CrossRef]
- Assmus, G. New Product Forecasting. J. Forecast. 1984, 3, 121–138. [Google Scholar] [CrossRef]
- Stark, D.; Mould, D.; Schweikert, A. 5 steps to creating a forecast. Healthc. Financ. Manag. 2008, 62, 100–105. [Google Scholar] [PubMed]
- Wang, X.; Disney, S.M. The bullwhip effect: Progress, trends and directions. Eur. J. Oper. Res. 2016, 250, 691–701. [Google Scholar] [CrossRef] [Green Version]
- Wind, Y. A Note on the Classification and Evaluation of New Product Forecasting Models. In Proceedings of the American Marketing Association Conference, April 1974; Available online: https://www.researchgate.net/publication/261323275_A_Note_on_the_Classification_and_Evaluation_of_New_Product_Forecasting_Models (accessed on 24 February 2021).
- Mahajan, V.; Wind, Y. New product forecasting models. Directions for research and implementation. Int. J. Forecast. 1988, 4, 341–358. [Google Scholar] [CrossRef]
- Hardie, B.G.; Fader, P.S.; Wisniewsky, M. An Empirical Comparison of New Product Trial Forecasting Models. J. Forecast. 1998, 17, 209–229. [Google Scholar] [CrossRef]
- Lynn, G.S.; Schnaars, S.P.; Skov, R.B. A Survey of New Product Forecasting Practices in Industrial High Technology and Low Technology Businesses—Traditional versus Multi-Attribute Approaches. Ind. Mark. Manag. 1999, 28, 565–571. [Google Scholar] [CrossRef]
- Ozer, M. A survey of New Product Evaluation Models. J. Prod. Innov. Manag. 1999, 16, 77–94. [Google Scholar] [CrossRef]
- Kahn, K.B. An exploratory Investigation of new product forecasting practices. J. Prod. Innov. Manag. 2002, 19, 133–143. [Google Scholar] [CrossRef]
- Lawrence, M.; Goodwin, P.; O’connor, M.; Önkal, D. Judgmental Forecasting: A Review of Progress Over the Last 25 Years. Int. J. Forecast. 2006, 22, 493–518. [Google Scholar] [CrossRef] [Green Version]
- Meade, N.; Islam, T. Modelling and Forecasting the Diffusion of Innovation—A 25-Year Review. Int. J. Forecast. 2006, 22, 519–545. [Google Scholar] [CrossRef]
- Kasapoglu, O.A. Selection of the Forecasting Model in Health Care. J. Hosp. Med Manag. 2016, 2, 2. [Google Scholar]
- Jbaily, A.; Feldhaus, I.; Bigelow, B.; Kamareddine, L.; Tolla, M.T.; Bouvier, M.; Kiros, M.; Verguet, S. Toward health system strengthening in low- and middle-income countries: Insights from mathematical modeling of drug supply chains. BMC Health Serv. Res. 2020, 20, 776. [Google Scholar] [CrossRef]
- Doerner, K.F.; Reiman, M. Logistics of health care management. Comput. Oper. Res. 2007, 34, 621–623. [Google Scholar] [CrossRef]
- Matthews, D. Strategic procurement in the public sector: A mask for financial and administrative policy. J. Public Procure. 2005, 5, 388–399. [Google Scholar] [CrossRef] [Green Version]
- Moschuri, S.J.; Kondylis, M.N. Outsourcing in public hospitals: A Greek perspective. J. Health Organ. Manag. 2006, 20, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Jarrett, P.G. An analysis of international health care logistics: The benefits and implications of implementing just-in-time systems in the health care industry. Leadersh. Health Serv. 2006, 19, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Yadav, P.; Tata, H.L.; Magali, B. The World Medicines Situation 2011: Storage and Supply Chain Management; World Health Organization: Geneva, Switzerland, 2011. [Google Scholar]
- Yadav, P. Health Product Supply Chains in Developing Countries: Diagnosis of the Root Causes of Underperformance and an Agenda for Reform. Health Syst. Reform 2015, 1, 142–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, D.; Souteyran, Y.; Banda, M.A.; Kaufman, J.; Perriëns, J.H. Investment in HIV/AIDS programs: Does it help strengthen health systems in developing countries? Glob. Health 2008, 4, 8. [Google Scholar] [CrossRef] [Green Version]
- Sullivan, E.; Goentzel, J.; Weintraub, R. Concept Note: The Global Health Supply Chain; Harvard Business Publishing: Boston, MA, USA, 2012. [Google Scholar]
- Sekhri, N.; Levine, R.; Pickett, J. A Risky Business Saving Money and Improving Global Health through Better Demand Forecasts; Center for Global Development: Washington, DC, USA, 2007. [Google Scholar]
- USAID|DELIVER PROJECT, Task Order 1. Quantification of Health Commodities: A Guide to Forecasting and Supply Planning for Procurement; USAID|DELIVER PROJECT, Task Order 1: Arlington, VA, USA, 2008. [Google Scholar]
- Sekhri, N.; Chisholm, R.; Longhi, A.; Evans, P.; Rilling, M.; Wilson, E. Principles for Forecasting Demand for Global Health Products; Centre for Global Development: Washington, DC, USA, 2006. [Google Scholar]
- Nikolopoulos, K.; Punia, S.; Schäfers, A.; Tsinopoulos, C.; Vasilakis, C. Forecasting and planning during a pandemic: COVID-19 growth rates, supply chain disruptions, and governmental decisions. Eur. J. Oper. Res. 2021, 290, 99–115. [Google Scholar] [CrossRef]
- Mas-Machuca, M.; Sainz, M.; Martinez-Costa, C. A review of forecasting models for new products. Intang. Cap. 2014, 10. [Google Scholar] [CrossRef] [Green Version]
- Schaefer, G.O.; Tam, G.C.; Savulescu, J.; Voo, T.C. COVID-19 vaccine development: Time to consider SARS-CoV-2 challenge studies? Vaccine 2020, 38, 5085–5088. [Google Scholar] [CrossRef]
- Adler, N.E.; Newman, K. Socioeconomic Disparities in Health: Pathways and Policies. Health Aff. 2002, 21, 60–76. [Google Scholar] [CrossRef] [PubMed]
- Hodgson, S.H.; Mansatta, K.; Mallett, G.; Harris, V.; Emary, K.R.W.; Pollard, A.J. What defines an efficacious COVID-19 vaccine? A review of the challenges assessing the clinical efficacy of vaccines against SARS-CoV-2. Lancet Infect. Dis. 2020, 21, e26–e35. [Google Scholar] [CrossRef]
- Ventola, C.L. The antibiotic resistance crisis: Part 1: Causes and threats. Pharm. Ther. 2015, 40, 277–283. [Google Scholar]
- Mackintosh, M.; Tibandebage, P.; Njeru, M.K.; Kungu, J.K.; Israel, C.; Mujinja, P.G.M. Rethinking health sector procurement as developmental linkages in East Africa. Soc. Sci. Med. 2018, 200, 182–189. [Google Scholar] [CrossRef] [PubMed]
- Soyiri, I.N.; Reidpath, D.D. An overview of health forecasting. Environ. Health Prev. Med. 2013, 18. [Google Scholar] [CrossRef] [Green Version]
- Steele, P.; Subramanian, L.; Tolani, F. Interventions to Improve Access to Medicine in Developing Countries: Mapping WHO’s Building Blocks and Supply Chain Functions. Acta Sci. Pharm. Sci. 2019, 3, 111–120. [Google Scholar] [CrossRef]
- Webb, S. A bitter pill to swallow: The problem of, and solutions to, Sub-Saharan Africa’s counterfeit pharmaceutical trade. The Columbia J. Glob. Health 2014, 4, 19–25. [Google Scholar] [CrossRef]
- Yadav, P.; Curtis, K.; Sekhri, N. Mapping and Realigning Incentives in the Supply Chain for Global Health Products; Center for Global Development: Washington, DC, USA, 2006. [Google Scholar]
- Dixon-Woods, M.; McNicol, S.; Martin, G. Ten challenges in improving quality in healthcare: Lessons from the Health Foundation’s programme evaluations and relevant literature. BMJ Qual. Saf. 2012, 21, 876–884. [Google Scholar] [CrossRef] [Green Version]
- Wolfgang, K.; Thorsten, B.; Christian, R.M. Digitalization in Supply Chain Management and Logistics: Smart and Digital Solutions for an Industry 4.0 Environment. In Proceedings of the Hamburg International Conference of Logistics (HICL), Hamburg, Germany, 12–13 October 2017; ISBN 978-3-7450-4328-0. [Google Scholar]
- Hermes, S.; Riasanow, T.; Clemons, E.K.; Bohm, M.; Krcmar, H. The digital transformation of the healthcare industry: Exploring the rise of emerging platform ecosystems and their influence on the role of patients. Bus. Res. 2020, 13, 1033–1069. [Google Scholar] [CrossRef]
- Barder, O.; Levine, R. An Introduction to Risk and Uncertainty. In Global Health Forecasting Working Group Background Paper; Center for Global Development: Washington, DC, USA, 2006. [Google Scholar]
- Thadani, K.B. Public Private Partnership in the Health Sector: Boon or Bane. Procedia Soc. Behav. Sci. 2014, 157, 307–316. [Google Scholar] [CrossRef]
- Kalkuhl, M.; von Braun, J.; Torero, M. (Eds.) Food Price Volatility and Its Implications for Food Security and Policy; Springer: Cham, Switzerland, 2016. [Google Scholar] [CrossRef] [Green Version]
- Taylor, D. The Pharmaceutical Industry and the Future of Drug Development. Pharm. Environ. 2015. [Google Scholar] [CrossRef]
- Bollyky, T.J.; Templin, T.; Cohen, M.; Dieleman, J.L. Lower-Income Countries that Face the Most Rapid Shift in Noncommunicable Disease Burden Are Also the Least Prepared. Health Aff. 2017, 36, 1866–1875. [Google Scholar] [CrossRef]
- Grépin, K.A.; Pinkstaff, C.B.; Shroff, Z.C.; Ghaffar, A. Donor funding health policy and systems research in low- and middle-income countries: How much, from where and to whom. Health Res. Policy Syst. 2017, 15, 68. [Google Scholar] [CrossRef]
- Grace, C. Global Health Partnership Impact on Commodity Pricing and Security; DFID Health Resource Centre: London, UK, 2014. [Google Scholar]
- Bulíř, A.; Hamann, A.J. Volatility of Development Aid: From the Frying Pan into the Fire? World Dev. 2008, 36, 2048–2066. [Google Scholar]
- Yadav, P.; Sekhri, N.; Curtis, K.A. Barriers to Access: An Assessment of Stakeholder Risks and Incentives in the Value Chain for Artemisinin Combination Therapy (ACT) Treatments. Available online: https://ssrn.com/abstract=1008307 (accessed on 30 November 2020).
- Brun, A.; Karaosman, H.; Barresi, T. Supply Chain Collaboration for Transparency. Sustainability 2020, 12, 4429. [Google Scholar] [CrossRef]
- Chen, J.; Xu, H.; Zhou, P. Delegation vs. direct sourcing revisited: Contract types under correlated supply risks and asymmetric cost information. Int. J. Prod. Res. 2020, 58, 7005–7022. [Google Scholar] [CrossRef]
- Duong, M.H.; Moles, R.J.; Chaar, B.; Chen, T.F. Stakeholder roles in facilitating access to essential medicines. Res. Soc. Adm. Pharm. 2018, 15, 260–266. [Google Scholar] [CrossRef]
- Duong, M.H.; Moles, R.J.; Chaar, B.; Chen, T.F. Stakeholder perspectives on the challenges surrounding management and supply of essential medicines. Int. J. Clin. Pharm. 2019, 41, 1210–1219. [Google Scholar] [CrossRef] [PubMed]
- Fisher, M.L. What Is the Right Supply Chain for Your Product? Harv. Bus. Rev. 1997, 105–116. [Google Scholar]
- Seidman, G.; Atun, R. Do changes to supply chains and procurement processes yield cost savings and improve availability of pharmaceuticals, vaccines, or health products? A systematic review of evidence from low-income and middle-income countries. BMJ Glob. Health 2017, 2, e000243. [Google Scholar] [CrossRef]
- Ejughemre, U. Donor Support and the Impacts on Health System Strengthening in Sub-Saharan Africa: Assessing the Evidence through a Review of the Literature. Am. J. Public Health Res. 2013, 1, 146–151. [Google Scholar] [CrossRef] [Green Version]
- Chalkidou, K.; Claxton, K.; Silverman, R.; Yadav, P. Value-based tiered pricing for universal health coverage: An idea worth revisiting. Gates Open Res. 2020, 4, 16. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Camacho, C.A.; Montoya-Torres, J.R.; Jaegler, A.; Gondran, N. Sustainability metrics for real case applications of the supply chain network design problem: A systematic literature review. J. Clean Prod. 2019, 231, 600–618. [Google Scholar] [CrossRef]
- Lee, H.L.; Whang, S. Information Sharing in a Supply Chain; Graduate School of Business Stanford University, Department of Industrial Engineering and Engineering Management: Stanford, CA, USA, 1998; Research Paper No. 1549. [Google Scholar]
- Lane, C.; Glassman, A. Bigger and Better? Scaling Up and Innovation in Health Aid. Health Aff. 2007, 26, 935–948. [Google Scholar] [CrossRef] [Green Version]
- Milstien, J.B.; Gaulé, P.; Kaddar, M. Access to vaccine technologies in developing countries: Brazil and India. Vaccine 2007, 25, 7610–7619. [Google Scholar] [CrossRef] [PubMed]
- Tauqeer, F.; Myhr, K.; Gopinathan, U. Institutional barriers and enablers to implementing and complying with internationally accepted quality standards in the local pharmaceutical industry of Pakistan: A qualitative study. Health Policy Plan. 2019, 34, 440–449. [Google Scholar] [CrossRef]
- Yadav, P.; Schmidt, C.P. Buy-Back Contracts and Forecasting Incentives in a Supplier-Retailer Channel. Available online: https://ssrn.com/abstract=929713 (accessed on 30 November 2020).
- Shen, B.; Choi, T.; Minner, S. A review on supply chain contracting with information considerations: Information updating and information asymmetry. Int. J. Prod. Res. 2019, 57, 4898–4936. [Google Scholar] [CrossRef] [Green Version]
- Elias, C.J. Can we ensure health is within reach for everyone? Lancet 2006, 368, S40–S41. [Google Scholar] [CrossRef]
- Glassman, A.; Kenny, C. Health Spending, Middle-Income Countries Face a Priorities Ditch, not a Financing Ditch—But that Still Merits Aid; Center for Global Development: Washington, DC, USA, 2015. [Google Scholar]
- Roehrich, J.K.; Lewis, M.A.; George, G. Are public-private partnerships a healthy option? A systematic literature review. Soc. Sci. Med. 2014, 113, 110–119. [Google Scholar] [CrossRef] [Green Version]
- Soni, A.; Magaziner, I. Getting More for the Money: How Lower Prices Were Possible, Progress to Date & the Challenges Ahead; Global Health Council: Washington, DC, USA, 2005. [Google Scholar]
- Davenport, T.H.; Eccles, R.G.; Prusak, L. Information politics. Sloan Manag. Rev. 1992, 34, 53–65. [Google Scholar]
- Silva-Aravena, F.; Ceballos-Fuentealba, I.; Álvarez-Miranda, E. Inventory Management at a Chilean Hospital Pharmacy: Case Study of a Dynamic Decision-Aid Tool. Mathematics 2020, 8, 1962. [Google Scholar] [CrossRef]
Figure 1.
Steps taken for research methodology.
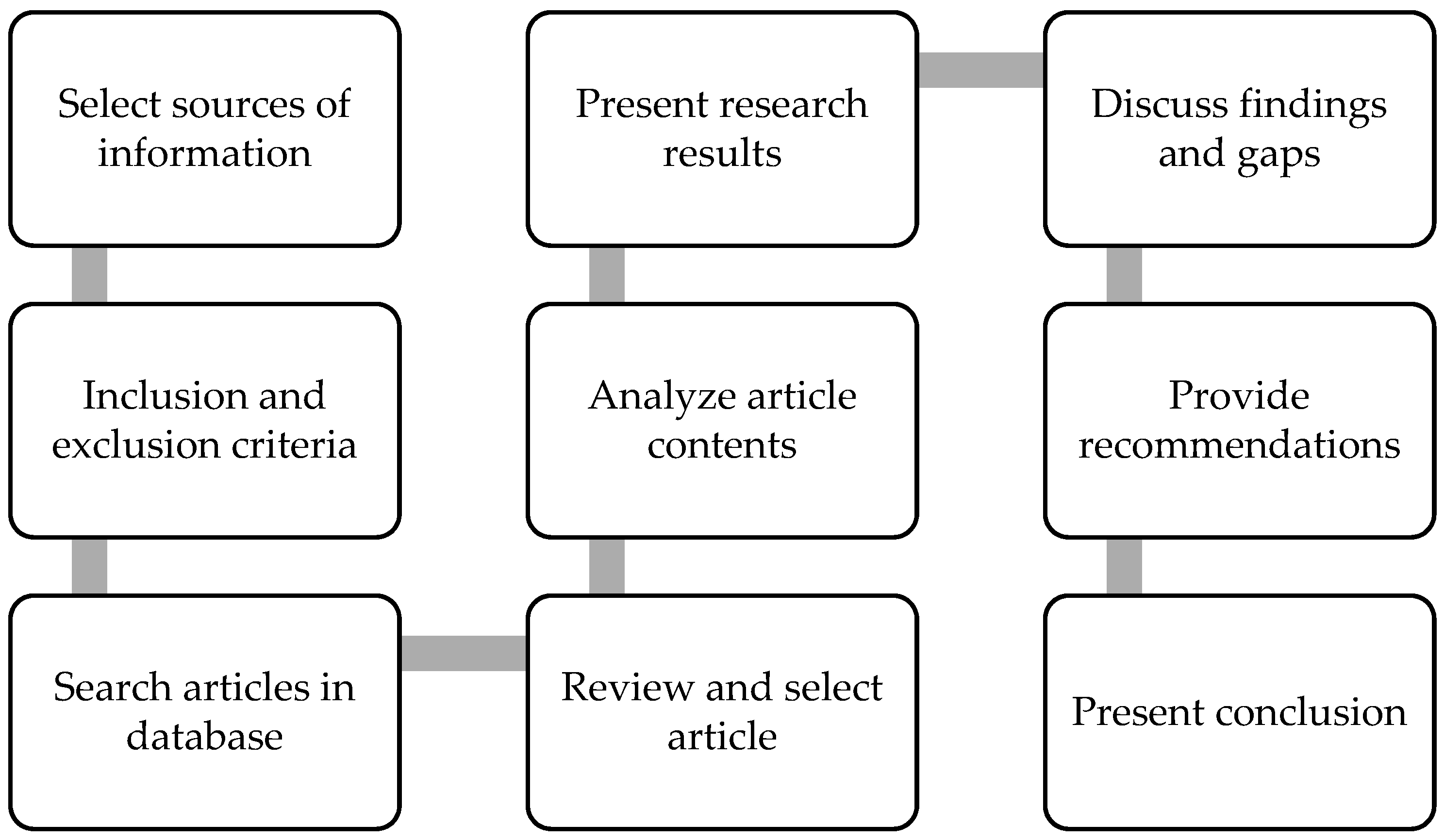
Figure 2.
Distribution of articles by year of publication.
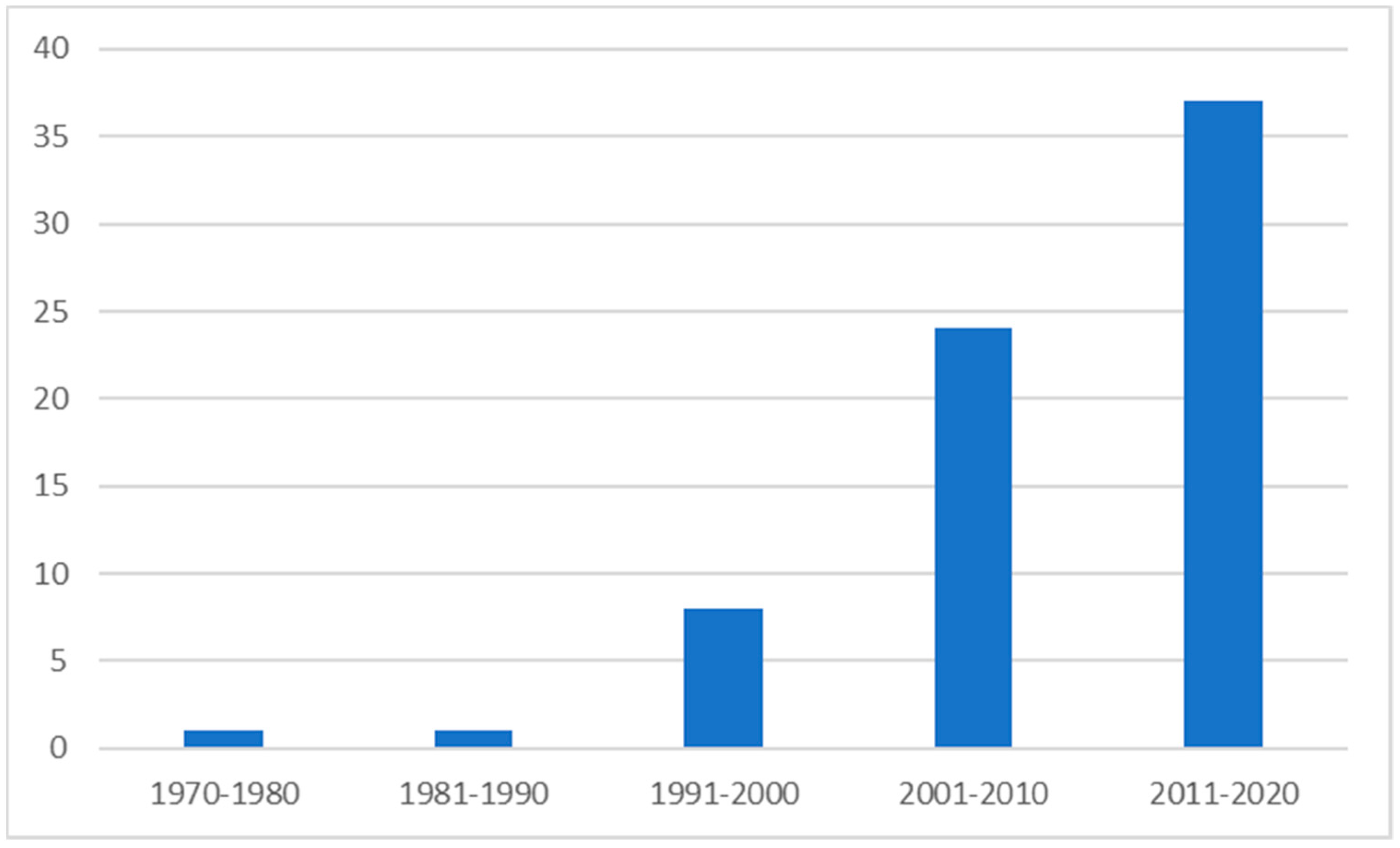
Figure 3.
Distribution of articles by primary area of focus.
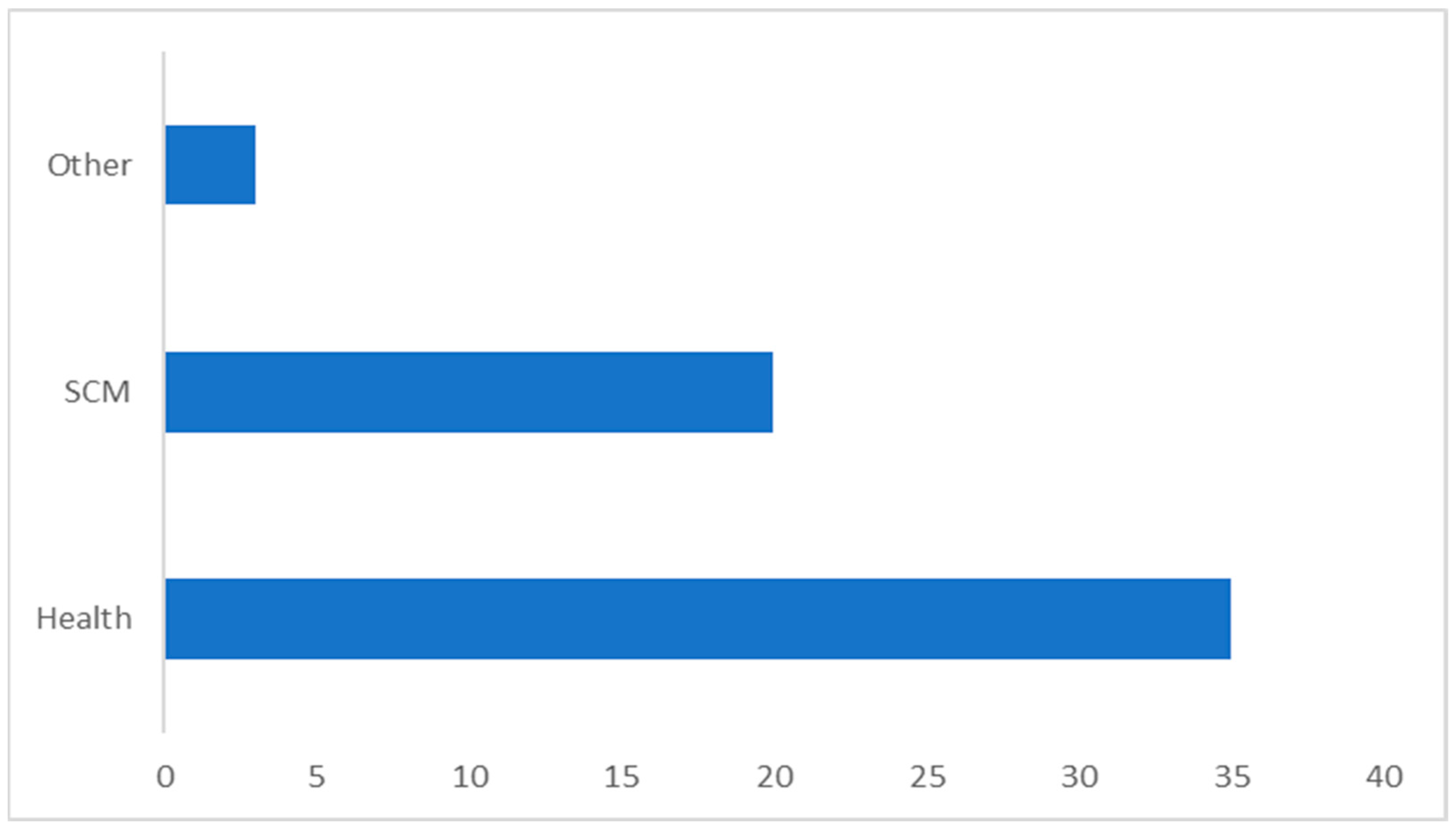
Figure 4.
Distribution of articles by research methodologies.

Figure 5.
Risk allocation across different health supply chain stakeholders.
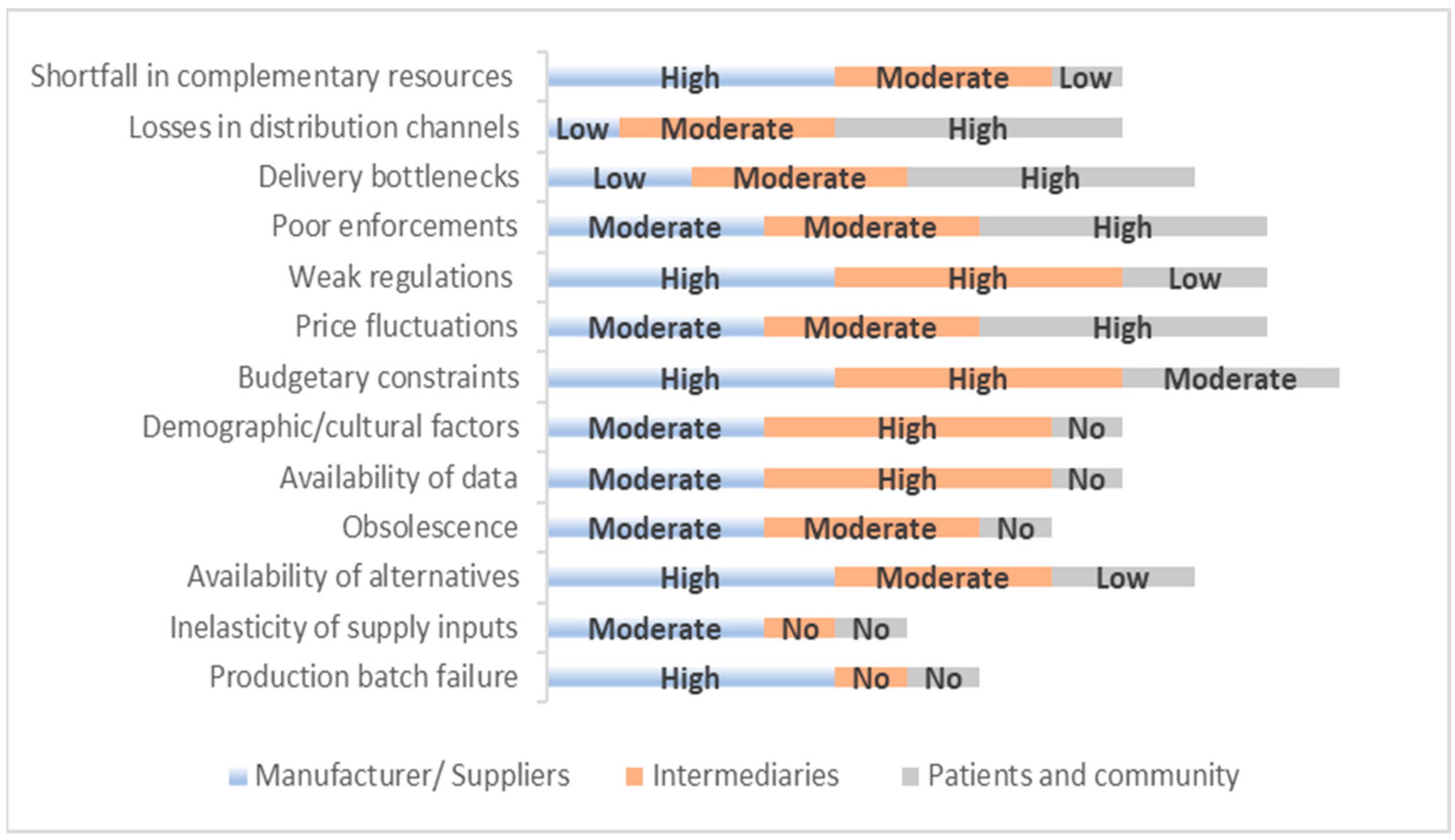
Figure 6.
Heat map showing the enablers and blockers.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 1.
Contributions of studies in the literature.
| Authors | Health | SCM | Forecasting | Risks | Incentives |
|---|---|---|---|---|---|
| Lee, et al., [1] | NA | * | NA | * | NA |
| Kraiselburd, et al., [2] | * | * | NA | NA | NA |
| Sued, et al., [3] | * | * | NA | NA | NA |
| Assmus [4] | NA | NA | * | NA | NA |
| Stark, et al., [5] | * | NA | * | NA | NA |
| Mahajan, et al., [8] | NA | NA | * | NA | NA |
| Kahn, [12] | NA | NA | * | NA | NA |
| Meade, et al., [14] | NA | NA | * | * | NA |
| Kasapoglu, [15] | * | NA | * | NA | NA |
| Jbaily, et al., [16] | * | * | NA | NA | NA |
| Matthews, [18] | NA | * | NA | * | NA |
| Moschuri, et al., [19] | * | * | NA | NA | NA |
| Jarret, [20] | * | * | NA | NA | NA |
| Magali, [21] | * | * | NA | NA | NA |
| Sullivan, et al., [24] | * | * | NA | NA | NA |
| Sekhri, et al., [25] | * | NA | * | * | NA |
| USAID, [26] | * | * | * | NA | NA |
| Sekhri, et al., [27] | * | NA | * | NA | NA |
| Nikolopoulos, et al., [28] | * | NA | * | NA | NA |
| Mas-Machuca, et al., [29] | NA | NA | * | NA | NA |
| Schaefer, et al., [30] | * | NA | * | * | NA |
| Adler, et al., [31] | * | NA | NA | NA | NA |
| Hodgson, et al., [32] | * | NA | * | NA | NA |
| Mackintosh, et al., [34] | * | * | NA | NA | NA |
| Soyiri, et al., [35] | * | NA | * | NA | NA |
| Steele, et al., [36] | * | * | * | NA | NA |
| Yadav, et al., [38] | * | * | NA | NA | * |
| Dixon-Woods, et al., [39] | * | NA | NA | * | NA |
| Wolfgang, et al., [40] | NA | * | * | NA | NA |
| Hermes, et al., [41] | * | NA | NA | * | NA |
| Barder, et al. [42] | * | NA | NA | * | NA |
| Taylor, [45] | * | NA | NA | * | NA |
| Bollyky, et al., [46] | * | NA | NA | * | NA |
| Grépin, et al., [47] | * | NA | NA | * | NA |
| Grace, [48] | NA | * | NA | * | NA |
| Bulíř, et al., [49] | * | NA | NA | * | NA |
| Yadav, et al., [50] | NA | * | * | NA | NA |
| Brun, et al., [51] | NA | * | NA | NA | NA |
| Chen, et al., [52] | NA | * | NA | * | NA |
| Duong, et al., [53] | * | * | NA | * | NA |
| Duong, et al., [54] | * | * | NA | NA | NA |
| Fisher, [55] | NA | * | NA | * | NA |
| Seidman, et al., [56] | NA | * | NA | * | NA |
| Ejughemre, [57] | * | NA | NA | * | NA |
| Chalkidou, et al., [58] | * | NA | NA | * | NA |
| Current study | * | * | * | * | * |
NA—Not applicable; *—Applicable.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Subramanian, L. Effective Demand Forecasting in Health Supply Chains: Emerging Trend, Enablers, and Blockers. Logistics 2021, 5, 12. https://0-doi-org.brum.beds.ac.uk/10.3390/logistics5010012
AMA Style
Subramanian L. Effective Demand Forecasting in Health Supply Chains: Emerging Trend, Enablers, and Blockers. Logistics. 2021; 5(1):12. https://0-doi-org.brum.beds.ac.uk/10.3390/logistics5010012
Chicago/Turabian StyleSubramanian, Lakshmy. 2021. "Effective Demand Forecasting in Health Supply Chains: Emerging Trend, Enablers, and Blockers" Logistics 5, no. 1: 12. https://0-doi-org.brum.beds.ac.uk/10.3390/logistics5010012