
Association between Levels of Urine Di-(2-ethylhexyl)phthalate Metabolites and Heart Rate Variability in Young Adults

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
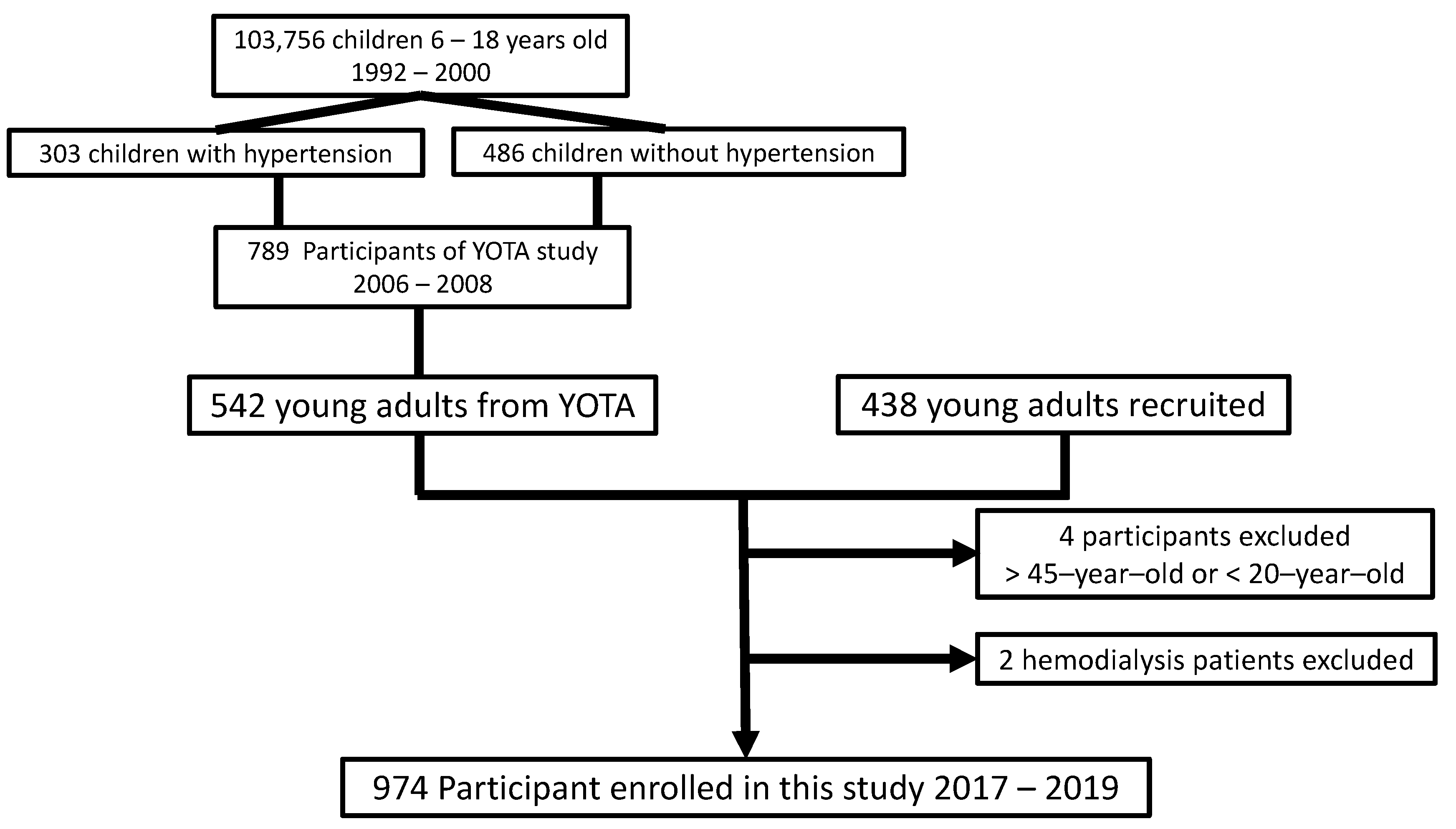
2.1. Subjects
2.2. Assessment of Clinical Information and Risk Stratification
2.3. Urinary Phthalates Metabolites
2.4. Heart Rate Variability Analysis
2.5. Statistical Analysis
3. Results
3.1. Participant Characteristics
3.2. Heart Rate Variability Analysis
3.3. Multiple Linear Regression Models
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kamrin, M.A. Phthalate risks, phthalate regulation, and public health: A review. J. Toxicol. Environ. Health B Crit. Rev. 2009, 12, 157–174. [Google Scholar] [CrossRef]
- Lorz, P.M.; Rowae, F.K.; Enke, W.; Jäckh, R.; Bhargava, N.; Hillesheim, W. (Eds.) Phthalic Acid and Derivatives, 7th ed.; Wiley-VCH: Weinheim, Germany, 2007; pp. 132–180. [Google Scholar]
- Koch, H.M.; Bolt, H.M.; Angerer, J. Di(2-ethylhexyl)phthalate (DEHP) metabolites in human urine and serum after a single oral dose of deuterium-labelled DEHP. Arch. Toxicol. 2004, 78, 123–130. [Google Scholar] [CrossRef]
- Koch, H.M.; Preuss, R.; Angerer, J. Di(2-ethylhexyl)phthalate (DEHP): Human metabolism and internal exposure—An update and latest results1. Int. J. Androl. 2006, 29, 155–165. [Google Scholar] [CrossRef]
- Silva, M.J.; Samandar, E.; Preau, J.L., Jr.; Needham, L.L.; Calafat, A.M. Urinary oxidative metabolites of di(2-ethylhexyl) phthalate in humans. Toxicol. 2006, 219, 22–32. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Silva, M.J.; Reidy, J.A.; Hurtz, D., 3rd; Malek, N.A.; Needham, L.L.; Nakazawa, H.; Barr, D.B.; Calafat, A.M. Mono(2-ethyl-5-hydroxyhexyl) phthalate and mono-(2-ethyl-5-oxohexyl) phthalate as biomarkers for human exposure assessment to di-(2-ethylhexyl) phthalate. Environ. Health Perspect. 2004, 112, 327–330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trasande, L.; Sathyanarayana, S.; Spanier, A.J.; Trachtman, H.; Attina, T.M.; Urbina, E.M. Urinary phthalates are associated with higher blood pressure in childhood. J. Pediatr. 2013, 163, 747–753.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trasande, L.; Spanier, A.J.; Sathyanarayana, S.; Attina, T.M.; Blustein, J. Urinary phthalates and increased insulin resistance in adolescents. Pediatrics 2013, 132, e646–e655. [Google Scholar] [CrossRef] [Green Version]
- Chen, S.Y.; Hwang, J.S.; Sung, F.C.; Lin, C.Y.; Hsieh, C.J.; Chen, P.C.; Su, T.C. Mono-2-ethylhexyl phthalate associated with insulin resistance and lower testosterone levels in a young population. Environ. Pollut. 2017, 225, 112–117. [Google Scholar] [CrossRef]
- James-Todd, T.; Stahlhut, R.; Meeker, J.D.; Powell, S.G.; Hauser, R.; Huang, T.; Rich-Edwards, J. Urinary phthalate metabolite concentrations and diabetes among women in the National Health and Nutrition Examination Survey (NHANES) 2001–2008. Environ. Health Perspect. 2012, 120, 1307–1313. [Google Scholar] [CrossRef] [Green Version]
- Ferguson, K.K.; Loch-Caruso, R.; Meeker, J.D. Exploration of oxidative stress and inflammatory markers in relation to urinary phthalate metabolites: NHANES 1999–2006. Environ. Sci. Technol. 2012, 46, 477–485. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferguson, K.K.; Loch-Caruso, R.; Meeker, J.D. Urinary phthalate metabolites in relation to biomarkers of inflammation and oxidative stress: NHANES 1999–2006. Environ. Res. 2011, 111, 718–726. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, C.Y.; Hsieh, C.J.; Lo, S.C.; Chen, P.C.; Torng, P.L.; Hu, A.; Sung, F.C.; Su, T.C. Positive association between concentration of phthalate metabolites in urine and microparticles in adolescents and young adults. Environ. Int. 2016, 92–93, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Su, T.C.; Hwang, J.S.; Torng, P.L.; Wu, C.; Lin, C.Y.; Sung, F.C. Phthalate exposure increases subclinical atherosclerosis in young population. Environ. Pollut. 2019, 250, 586–593. [Google Scholar] [CrossRef]
- Shiue, I. Urine phthalate concentrations are higher in people with stroke: United States National Health and Nutrition Examination Surveys (NHANES), 2001–2004. Eur. J. Neurol. 2013, 20, 728–731. [Google Scholar] [CrossRef]
- Su, T.C.; Hwang, J.J.; Sun, C.W.; Wang, S.L. Urinary phthalate metabolites, coronary heart disease, and atherothrombotic markers. Ecotoxicol. Environ. Saf. 2019, 173, 37–44. [Google Scholar] [CrossRef]
- Zhao, J.F.; Hsiao, S.H.; Hsu, M.H.; Pao, K.C.; Kou, Y.R.; Shyue, S.K.; Lee, T.S. Di-(2-ethylhexyl) phthalate accelerates atherosclerosis in apolipoprotein E-deficient mice. Arch. Toxicol. 2016, 90, 181–190. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.Y.; Lee, H.L.; Hwang, Y.T.; Wang, C.; Hsieh, C.J.; Wu, C.; Sung, F.C.; Su, T.C. The association between urine di-(2-ethylhexyl) phthalate metabolites, global DNA methylation, and subclinical atherosclerosis in a young Taiwanese population. Environ. Pollut. 2020, 265, 114912. [Google Scholar] [CrossRef]
- Posnack, N.G. The adverse cardiac effects of Di(2-ethylhexyl)phthalate and Bisphenol A. Cardiovasc. Toxicol. 2014, 14, 339–357. [Google Scholar] [CrossRef] [Green Version]
- Tsuji, H.; Larson, M.G.; Venditti, F.J., Jr.; Manders, E.S.; Evans, J.C.; Feldman, C.L.; Levy, D. Impact of reduced heart rate variability on risk for cardiac events. The Framingham Heart Study. Circulation 1996, 94, 2850–2855. [Google Scholar] [CrossRef]
- Dekker, J.M.; Crow, R.S.; Folsom, A.R.; Hannan, P.J.; Liao, D.; Swenne, C.A.; Schouten, E.G. Low heart rate variability in a 2-minute rhythm strip predicts risk of coronary heart disease and mortality from several causes: The ARIC Study. Atherosclerosis Risk In Communities. Circulation 2000, 102, 1239–1244. [Google Scholar] [CrossRef]
- Hillebrand, S.; Gast, K.B.; de Mutsert, R.; Swenne, C.A.; Jukema, J.W.; Middeldorp, S.; Rosendaal, F.R.; Dekkers, O.M. Heart rate variability and first cardiovascular event in populations without known cardiovascular disease: Meta-analysis and dose-response meta-regression. Europace 2013, 15, 742–749. [Google Scholar] [CrossRef] [PubMed]
- Kotecha, D.; New, G.; Flather, M.D.; Eccleston, D.; Pepper, J.; Krum, H. Five-minute heart rate variability can predict obstructive angiographic coronary disease. Heart 2012, 98, 395–401. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.H.; Ma, H.P.; Lin, Y.T.; Hung, C.S.; Huang, S.H.; Chuang, B.L.; Lin, C.; Lo, M.T.; Peng, C.K.; Lin, Y.H. Usefulness of heart rhythm complexity in heart failure detection and diagnosis. Sci. Rep. 2020, 10, 14916. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.H.; Ma, H.P.; Lin, Y.T.; Hung, C.S.; Hsieh, M.C.; Chang, T.Y.; Kuo, P.H.; Lin, C.; Lo, M.T.; Hsu, H.H.; et al. Heart Rhythm Complexity Impairment in Patients with Pulmonary Hypertension. Sci. Rep. 2019, 9, 10710. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Zhou, X.; Zhang, H.; Liu, Y.; Cao, C.; Dong, R.; Yuan, Y.; Wang, M.; Lu, Y.; Wu, M.; et al. Association between urinary concentration of phthalate metabolites and impaired renal function in Shanghai adults. Environ. Pollut. 2019, 245, 149–162. [Google Scholar] [CrossRef]
- Nolan, J.; Batin, P.D.; Andrews, R.; Lindsay, S.J.; Brooksby, P.; Mullen, M.; Baig, W.; Flapan, A.D.; Cowley, A.; Prescott, R.J.; et al. Prospective study of heart rate variability and mortality in chronic heart failure: Results of the United Kingdom heart failure evaluation and assessment of risk trial (UK-heart). Circulation 1998, 98, 1510–1516. [Google Scholar] [CrossRef] [Green Version]
- Kleiger, R.E.; Miller, J.P.; Bigger, J.T., Jr.; Moss, A.J. Decreased heart rate variability and its association with increased mortality after acute myocardial infarction. Am. J. Cardiol. 1987, 59, 256–262. [Google Scholar] [CrossRef]
- Bigger, J.T., Jr.; Fleiss, J.L.; Steinman, R.C.; Rolnitzky, L.M.; Kleiger, R.E.; Rottman, J.N. Frequency domain measures of heart period variability and mortality after myocardial infarction. Circulation 1992, 85, 164–171. [Google Scholar] [CrossRef] [Green Version]
- Buccelletti, E.; Gilardi, E.; Scaini, E.; Galiuto, L.; Persiani, R.; Biondi, A.; Basile, F.; Silveri, N.G. Heart rate variability and myocardial infarction: Systematic literature review and metanalysis. Eur. Rev. Med. Pharmacol. Sci. 2009, 13, 299–307. [Google Scholar]
- Jaimes, R., 3rd; Swiercz, A.; Sherman, M.; Muselimyan, N.; Marvar, P.J.; Posnack, N.G. Plastics and cardiovascular health: Phthalates may disrupt heart rate variability and cardiovascular reactivity. Am. J. Physiol. Heart Circ. Physiol. 2017, 313, H1044–H1053. [Google Scholar] [CrossRef]
- Su, T.C.; Liao, C.C.; Chien, K.L.; Hsu, S.H.; Sung, F.C. An overweight or obese status in childhood predicts subclinical atherosclerosis and prehypertension/hypertension in young adults. J. Atheroscler. Thromb. 2014, 21, 1170–1182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brinton, T.J.; Cotter, B.; Kailasam, M.T.; Brown, D.L.; Chio, S.S.; O’Connor, D.T.; DeMaria, A.N. Development and validation of a noninvasive method to determine arterial pressure and vascular compliance. Am. J. Cardiol. 1997, 80, 323–330. [Google Scholar] [CrossRef]
- Heart rate variability: Standards of measurement, physiological interpretation and clinical use. Task Force of the European Society of Cardiology and the North American Society of Pacing and Electrophysiology. Circulation 1996, 93, 1043–1065.
- Chen, S.Y.; Chan, C.C.; Su, T.C. Particulate and gaseous pollutants on inflammation, thrombosis, and autonomic imbalance in subjects at risk for cardiovascular disease. Environ. Pollut. 2017, 223, 403–408. [Google Scholar] [CrossRef] [PubMed]
- Posnack, N.G.; Lee, N.H.; Brown, R.; Sarvazyan, N. Gene expression profiling of DEHP-treated cardiomyocytes reveals potential causes of phthalate arrhythmogenicity. Toxicology 2011, 279, 54–64. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gillum, N.; Karabekian, Z.; Swift, L.M.; Brown, R.P.; Kay, M.W.; Sarvazyan, N. Clinically relevant concentrations of di (2-ethylhexyl) phthalate (DEHP) uncouple cardiac syncytium. Toxicol. Appl. Pharmacol. 2009, 236, 25–38. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Custodis, F.; Baumhäkel, M.; Schlimmer, N.; List, F.; Gensch, C.; Böhm, M.; Laufs, U. Heart rate reduction by ivabradine reduces oxidative stress, improves endothelial function, and prevents atherosclerosis in apolipoprotein E-deficient mice. Circulation 2008, 117, 2377–2387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, B.M.; Brantley, L.; White, C.; Seigler, N.; Harris, R.A. Association beween resting heart rate, shear and flow-mediated dilation in healthy adults. Exp. Physiol. 2014, 99, 1439–1448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aydin Sunbul, E.; Sunbul, M.; Gulec, H. The impact of major depression on heart rate variability and endothelial dysfunction in patients with stable coronary artery disease. Gen. Hosp. Psychiatry 2017, 44, 4–9. [Google Scholar] [CrossRef]
- Bhati, P.; Alam, R.; Moiz, J.A.; Hussain, M.E. Subclinical inflammation and endothelial dysfunction are linked to cardiac autonomic neuropathy in type 2 diabetes. J. Diabetes Metab. Disord. 2019, 18, 419–428. [Google Scholar] [CrossRef]
- Hoshi, R.A.; Santos, I.S.; Dantas, E.M.; Andreão, R.V.; Mill, J.G.; Goulart, A.C.; Lotufo, P.A.; Bensenor, I. Relationship between heart rate variability and carotid intima-media thickness in the Brazilian Longitudinal Study of Adult Health-ELSA-Brasil. Clin. Physiol. Funct. Imaging 2020, 40, 122–130. [Google Scholar] [CrossRef]
- Pereira, V.L., Jr.; Dobre, M.; Dos Santos, S.G.; Fuzatti, J.S.; Oliveira, C.R.; Campos, L.A.; Brateanu, A.; Baltatu, O.C. Association between carotid intima media thickness and heart rate variability in adults at increased cardiovascular risk. Front. Physiol. 2017, 8, 248. [Google Scholar] [CrossRef] [Green Version]
- Chu, P.C.; Wu, C.; Su, T.C. Association between urinary phthalate metabolites and markers of endothelial dysfunction in adolescents and young adults. Toxics 2021, 9, 33. [Google Scholar] [CrossRef] [PubMed]
- Koch, H.M.; Bolt, H.M.; Preuss, R.; Angerer, J. New metabolites of di(2-ethylhexyl)phthalate (DEHP) in human urine and serum after single oral doses of deuterium-labelled DEHP. Arch. Toxicol. 2005, 79, 367–376. [Google Scholar] [CrossRef] [PubMed]
- Fourth Report on Human Exposure to Environmental Chemicals; Department of Health and Human Services, Centers for Disease Control and Prevention: Atlanta, GA, USA, 2009.
- Mäkikallio, T.H.; Huikuri, H.V.; Hintze, U.; Videbaek, J.; Mitrani, R.D.; Castellanos, A.; Myerburg, R.J.; Møller, M. Fractal analysis and time- and frequency-domain measures of heart rate variability as predictors of mortality in patients with heart failure. Am. J. Cardiol. 2001, 87, 178–182. [Google Scholar] [CrossRef]
- Jovic, A.; Bogunovic, N. Electrocardiogram analysis using a combination of statistical, geometric, and nonlinear heart rate variability features. Artif. Intell. Med. 2011, 51, 175–186. [Google Scholar] [CrossRef]
- Tranfo, G.; Caporossi, L.; Pigini, D.; Capanna, S.; Papaleo, B.; Paci, E. Temporal Trends of Urinary Phthalate Concentrations in Two Populations: Effects of REACH Authorization after Five Years. Int. J. Environ. Res. Public Health 2018, 15, 1950. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Log MEHP (μg/g Creatinine) | Log MEHHP (μg/g Creatinine) | Log MEOHP (μg/g Creatinine) | |||||
|---|---|---|---|---|---|---|---|
| N (%) | Mean (SD) | p-Value | Mean (SD) | p-Value | Mean (SD) | p-Value | |
| Total | 974 (100) | 0.682 (0.693) | 0.783 (0.296) | −0.386 (0.327) | |||
| Median (IQR) * | 0.553 (0.943) * | 0.774 (0.376) * | −0.395 (0.407) * | ||||
| Sex | 0.193 | 0.001 | < 0.001 | ||||
| Male | 407 (41.8) | 0.648 (0.709) | 0.747 (0.297) | −0.448 (0.332) | |||
| Female | 567 (58.2) | 0.707 (0.681) | 0.809 (0.293) | −0.341 (0.316) | |||
| Age | 0.040 | 0.303 | 0.048 | ||||
| 18–32 | 453 (46.5) | 0.725 (0.720) | 0.773 (0.281) | −0.408 (0.320) | |||
| >32 | 521 (53.5) | 0.634 (0.659) | 0.792 (0.309) | −0.367 (0.332) | |||
| Hypertension | 0.097 | 0.132 | 0.314 | ||||
| Yes | 41 (4.2) | 0.916 (0.905) | 0.858 (0.317) | −0.329 (0.365) | |||
| No | 933 (95.8) | 0.673 (0.681) | 0.780 (0.295) | −0.388 (0.325) | |||
| Diabetes mellitus | 0.536 | 0.102 | 0.290 | ||||
| Yes | 30 (3.1) | 0.759 (0.674) | 0.858 (0.245) | −0.337 (0.252) | |||
| No | 944 (96.9) | 0.680 (0.694) | 0.781 (0.298) | −0.388 (0.329) | |||
| LDL-C, mg/dL | 0.532 | 0.084 | 0.010 | ||||
| ≥130 | 273 (28) | 0.660 (0.736) | 0.757 (0.294) | −0.429 (0.324) | |||
| <130 | 701 (72) | 0.692 (0.676) | 0.794 (0.297) | −0.369 (0.124) | |||
| BMI Z-score | 0.740 | 0.789 | 0.613 | ||||
| ≥−0.20 | 511 (52.5) | 0.676 (0.718) | 0.781 (0.309) | −0.391 (0.344) | |||
| <−0.20 | 463 (47.5) | 0.690 (0.665) | 0.786 (0.281) | −0.380 (0.307) | |||
| Smoking habit | 0.513 | 0.270 | 0.089 | ||||
| Smoker | 177 (18.2) | 0.652 (0.682) | 0.761 (0.299) | −0.426 (0.345) | |||
| Nonsmoker | 797 (81.8) | 0.689 (0.696) | 0.788 (0.295) | −0.377 (0.323) | |||
| Education | 0.469 | 0.020 | 0.001 | ||||
| College | 881 (90.5) | 0.677 (0.695) | 0.775 (0.288) | −0.397 (0.320) | |||
| High school | 93 (9.5) | 0.731 (0.677) | 0.864 (0.353) | −0.278 (0.370) | |||
| HRV | Log Mean RRI | Log SDNN (ms) | Log RMSSD (ms) | Log pNN50 (%) | Log HRV Triangular Index | Log TINN (ms) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β (SE) | p | β (SE) | p | β (SE) | p | β (SE) | p | β (SE) | p | β (SE) | p | |
| MEHP | 0.001 (0.009) | 0.786 | −0.012 (0.009) | 0.182 | −0.005 (0.012) | 0.645 | −0.021 (0.032) | 0.507 | −0.008 (0.008) | 0.299 | −0.011 (0.010) | 0.266 |
| MEHHP | 0.006 (0.007) | 0.349 | −0.032 (0.020) | 0.121 | −0.003 (0.028) | 0.903 | 0.039 (0.074) | 0.597 | −0.041 (0.018) | 0.025 | −0.066 (0.023) | 0.005 |
| MEOHP | 0.004 (0.006) | 0.495 | −0.034 (0.019) | 0.071 | −0.008 (0.026) | 0.751 | 0.035 (0.068) | 0.608 | −0.040 (0.017) | 0.016 | −0.051 (0.021) | 0.017 |
| ΣDEHP | 0.059 (0.235) | 0.801 | −0.132 (0.077) | 0.089 | −0.041 (0.057) | 0.468 | −0.014 (0.023) | 0.531 | −0.141 (0.087) | 0.105 | −0.138 (0.069) | 0.044 |
| Log VLF (0.00–0.04 Hz) | Log LF (0.04–0.15 Hz) | Log HF (0.15–0.4 Hz) | Log LF/HF | |||||
|---|---|---|---|---|---|---|---|---|
| β (SE) | p-Value | β (SE) | p-Value | β (SE) | p-Value | β (SE) | p-Value | |
| MEHP | −0.160 (0.022) | 0.460 | −0.027 (0.021) | 0.198 | −0.016 (0.024) | 0.512 | −0.008 (0.020) | 0.688 |
| MEHHP | −0.154 (0.051) | 0.003 | −0.112 (0.049) | 0.022 | −0.004 (0.056) | 0.941 | −0.112 (0.047) | 0.018 |
| MEOHP | −0.101 (0.047) | 0.032 | −0.134 (0.044) | 0.003 | −0.019 (0.051) | 0.715 | 0.121 (0.043) | 0.005 |
| ΣDEHP | −0.046 (0.031) | 0.137 | −0.062 (0.032) | 0.058 | −0.027 (0.028) | 0.342 | −0.026 (0.033) | 0.435 |
| Log HRV Triangular Index | Log TINN (ms) | |||
|---|---|---|---|---|
| β (95% CI) | p-Value | β (95% CI) | p-Value | |
| MEHP | −0.001 (−0.015~0.014) | 0.918 | −0.008 (−0.270~0.012) | 0.432 |
| MEHHP | −0.019 (−0.053~0.016) | 0.290 | −0.057 (−0.102~-0.011) | 0.016 |
| MEOHP | −0.017 (−0.048~0.015) | 0.310 | −0.040 (−0.082~0.003) | 0.067 |
| ΣDEHP | −0.005 (−0.027~0.017) | 0.652 | −0.026 (−0.056~0.004) | 0.091 |
| Log VLF (0.00–0.04 Hz) | Log LF (0.04–0.15 Hz) | Log HF (0.15–0.4 Hz) | Log LF/HF | |||||
|---|---|---|---|---|---|---|---|---|
| β (95% CI) | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | β (95% CI) | p-Value | |
| MEHP | −0.004 (−0.047~0.038) | 0.839 | −0.005 (−0.043~0.034) | 0.813 | 0.010 (−0.033~0.052) | 0.651 | −0.011 (−0.049~0.027) | 0.573 |
| MEHHP | −0.010 (−0.210~0.010) | 0.031 | −0.041 (−0.133~0.050) | 0.373 | 0.067 (−0.034~0.167) | 0.194 | −0.110 (−0.200~-0.020) | 0.016 |
| MEOHP | −0.049 (−0.141~0.043) | 0.297 | −0.053 (−0.137~0.031) | 0.213 | 0.043 (−0.049~0.136) | 0.359 | −0.101 (−0.184~-0.019) | 0.001 |
| ΣDEHP | −0.026 (−0.090~0.039) | 0.436 | −0.017 (−0.076~0.042) | 0.567 | 0.016 (−0.049~0.081) | 0.628 | −0.030 (−0.088~0.028) | 0.304 |
| Log MEHHP | Log LF/HF | Log MEOHP | Log LF/HF | ||||
|---|---|---|---|---|---|---|---|
| Mean | SD | p-Value for Linear Trend | Mean | SD | p-Value for Linear Trend | ||
| 1st quartile (<0.589) | 0.137 | 0.446 | 0.014 | 1st quartile (<−0.592) | 0.143 | 0.450 | 0.001 |
| 2nd quartile (<0.774) | 0.112 | 0.386 | 2nd quartile (<−0.395) | 0.123 | 0.411 | ||
| 3rd quartile (<0.965) | 0.054 | 0.482 | 3rd quartile (<−0.185) | 0.084 | 0.437 | ||
| 4th quartile (≥0.965) | 0.088 | 0.438 | 4th quartile (≥−0.185) | 0.089 | 0.452 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, C.-W.; Tang, S.-Y.; Hwang, J.-S.; Chan, C.-C.; Hsu, C.-C.; Lin, C.-Y.; Su, T.-C. Association between Levels of Urine Di-(2-ethylhexyl)phthalate Metabolites and Heart Rate Variability in Young Adults. Toxics 2021, 9, 351. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9120351
Chen C-W, Tang S-Y, Hwang J-S, Chan C-C, Hsu C-C, Lin C-Y, Su T-C. Association between Levels of Urine Di-(2-ethylhexyl)phthalate Metabolites and Heart Rate Variability in Young Adults. Toxics. 2021; 9(12):351. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9120351
Chicago/Turabian StyleChen, Ching-Way, Shu-Yu Tang, Jin-Shiang Hwang, Chang-Chuan Chan, Cheng-Chih Hsu, Chien-Yu Lin, and Ta-Chen Su. 2021. "Association between Levels of Urine Di-(2-ethylhexyl)phthalate Metabolites and Heart Rate Variability in Young Adults" Toxics 9, no. 12: 351. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9120351