
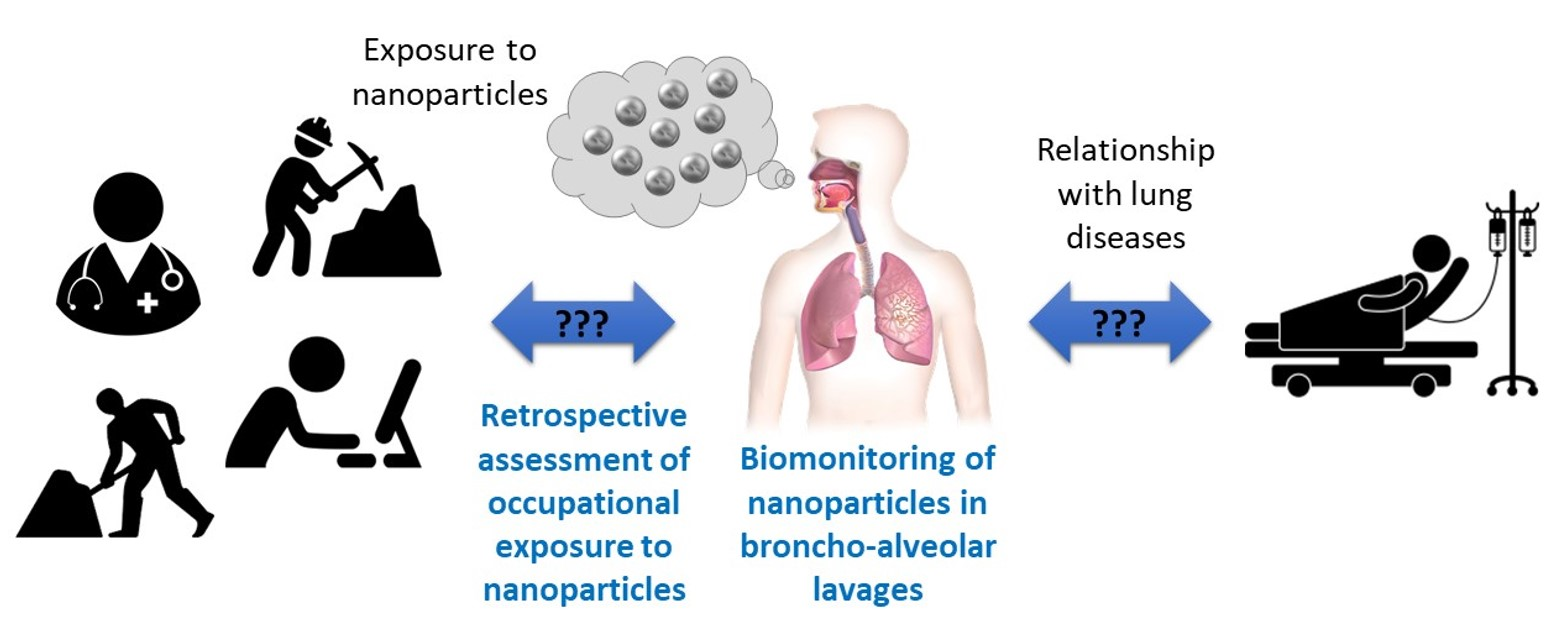
Relationship between Occupational Exposure to Airborne Nanoparticles, Nanoparticle Lung Burden and Lung Diseases

 ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Broncho-Alveolar Lavages
2.3. Sample Pre-Treatment and Analysis
2.4. Comparison to Clinical Data
2.5. Retrospective Occupational Exposure to Nanoparticles Assessment
3. Results
3.1. Relationship between Biomonitoring of Nanoparticles in Broncho-Alveolar Lavages and Lung Diseases
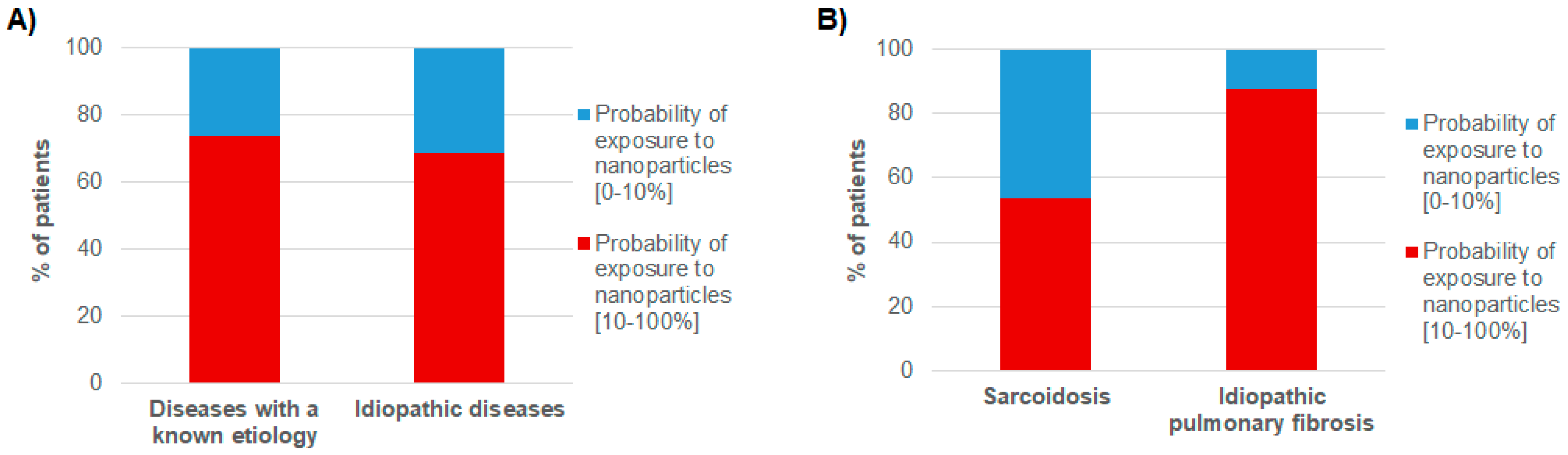
3.2. Relationship between Lung Diseases and Occupational Exposure
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Stone, V.; Miller, M.R.; Clift, M.J.D.; Elder, A.; Mills, N.L.; Møller, P.; Schins, R.P.F.; Vogel, U.; Kreyling, W.G.; Alstrup Jensen, K.; et al. Nanomaterials Versus Ambient Ultrafine Particles: An Opportunity to Exchange Toxicology Knowledge. Environ. Health Perspect. 2017, 125, 106002. [Google Scholar] [CrossRef]
- Manno, M.; Viau, C.; Cocker, J.; Colosio, C.; Lowry, L.; Mutti, A.; Nordberg, M.; Wang, S. Biomonitoring for occupational health risk assessment (BOHRA). Toxicol. Lett. 2010, 192, 3–16. [Google Scholar] [CrossRef]
- Silins, I.; Högberg, J. Combined Toxic Exposures and Human Health: Biomarkers of Exposure and Effect. Int. J. Environ. Res. Public Health 2011, 8, 629–647. [Google Scholar] [CrossRef] [Green Version]
- De Vuyst, P.; Karjalainen, A.; Dumortier, P.; Pairon, J.-C.; Monsó, E.; Brochard, P.; Teschler, H.; Tossavainen, A.; Gibbs, A. Guidelines for mineral fibre analyses in biological samples: Report of the ERS Working Group. European Respiratory Society. Eur. Respir. J. 1998, 11, 1416–1426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Case, B.W.; Abraham, J.L.; Meeker, G.; Pooley, F.D.; Pinkerton, K.E. Applying Definitions of “Asbestos” to Environmental and “Low-Dose” Exposure Levels and Health Effects, Particularly Malignant Mesothelioma. J. Toxicol. Environ. Health B Crit. Rev. 2011, 14, 3–39. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mossman, B.T.; Lippmann, M.; Hesterberg, T.W.; Kelsey, K.T.; Barchowsky, A.; Bonner, J.C. Pulmonary Endpoints (Lung Carcinomas and Asbestosis) Following Inhalation Exposure to Asbestos. J. Toxicol. Environ. Health B Crit. Rev. 2011, 14, 76–121. [Google Scholar] [CrossRef] [PubMed]
- Bargagli, E.; Lavorini, F.; Pistolesi, M.; Rosi, E.; Prasse, A.; Rota, E.; Voltolini, L. Trace metals in fluids lining the respiratory system of patients with idiopathic pulmonary fibrosis and diffuse lung diseases. J. Trace Elem. Med. Biol. 2017, 42, 39–44. [Google Scholar] [CrossRef]
- Bergamaschi, E.; Poland, C.; Guseva Canu, I.; Prina-Mello, A. The role of biological monitoring in nano-safety. Nano Today 2015, 10, 274–277. [Google Scholar] [CrossRef]
- Bitounis, D.; Pourchez, J.; Forest, V.; Boudard, D.; Cottier, M.; Klein, J.-P. Detection and analysis of nanoparticles in patients: A critical review of the status quo of clinical nanotoxicology. Biomaterials 2016, 76, 302–312. [Google Scholar] [CrossRef] [Green Version]
- Rapport de l’Anses—Anses Particules de l’air Ambiant Extérieur—Impact Sur La Pollution Atmosphérique Des Technologies et de La Composition Du Parc de Véhicules Automobiles Circulant En France. 2019. Available online: https://www.anses.fr/fr/content/rapport-de-lanses-particules-de-l’air-ambiant-extérieur-impact-sur-la-pollution (accessed on 9 July 2021).
- Groopman, J.D.; Kensler, T.W. The light at the end of the tunnel for chemical-specific biomarkers: Daylight or headlight? Carcinogenesis 1999, 20, 1–11. [Google Scholar] [CrossRef]
- Angerer, J.; Ewers, U.; Wilhelm, M. Human biomonitoring: State of the art. Int. J. Hyg. Environ. Health 2007, 210, 201–228. [Google Scholar] [CrossRef] [PubMed]
- Rinaldo, M.; Andujar, P.; Lacourt, A.; Martinon, L.; Canal Raffin, M.; Dumortier, P.; Pairon, J.-C.; Brochard, P. Perspectives in Biological Monitoring of Inhaled Nanosized Particles. Ann. Occup. Hyg. 2015, 59, 669–680. [Google Scholar] [CrossRef] [Green Version]
- Forest, V.; Vergnon, J.-M.; Pourchez, J. Biological Monitoring of Inhaled Nanoparticles in Patients: An Appealing Approach To Study Causal Link between Human Respiratory Pathology and Exposure to Nanoparticles. Chem. Res. Toxicol. 2017, 30, 1655–1660. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bitounis, D.; Klein, J.-P.; Mery, L.; El-Merhie, A.; Forest, V.; Boudard, D.; Pourchez, J.; Cottier, M. Ex vivo detection and quantification of gold nanoparticles in human seminal and follicular fluids. Analyst 2018, 143, 475–486. [Google Scholar] [CrossRef]
- Rinaldi, L.; Barabino, G.; Klein, J.-P.; Bitounis, D.; Pourchez, J.; Forest, V.; Boudard, D.; Leclerc, L.; Sarry, G.; Roblin, X.; et al. Metals distribution in colorectal biopsies: New insight on the elemental fingerprint of tumour tissue. Dig. Liver Dis. 2015, 47, 602–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raia-Barjat, T.; Prieux, C.; Leclerc, L.; Sarry, G.; Grimal, L.; Chauleur, C.; Pourchez, J.; Forest, V. Elemental fingerprint of human amniotic fluids and relationship with potential sources of maternal exposure. J. Trace Elem. Med. Biol. 2020, 60, 126477. [Google Scholar] [CrossRef] [Green Version]
- Forest, V.; Vergnon, J.-M.; Guibert, C.; Bitounis, D.; Leclerc, L.; Sarry, G.; Pourchez, J. Metal load assessment in patient pulmonary lavages: Towards a comprehensive mineralogical analysis including the nano-sized fraction. Nanotoxicology 2017, 11, 1211–1224. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Forest, V.; Pourchez, J.; Guibert, C.; Bitounis, D.; Leclerc, L.; Sarry, G.; Vergnon, J.-M. Nano to micron-sized particle detection in patients’ lungs and its pathological significance. Environ. Sci. Nano 2019, 6, 1343–1350. [Google Scholar] [CrossRef]
- Bitounis, D.; Barnier, V.; Guibert, C.; Pourchez, J.; Forest, V.; Boudard, D.; Hochepied, J.-F.; Chelle, P.; Vergnon, J.-M.; Cottier, M. A method for the quantitative extraction of gold nanoparticles from human bronchoalveolar lavage fluids through a glycerol gradient. Nanoscale 2018, 10, 2955–2969. [Google Scholar] [CrossRef] [PubMed]
- Mikolasch, T.A.; Garthwaite, H.S.; Porter, J.C. Update in diagnosis and management of interstitial lung disease. Clin. Med. (Lond.) 2017, 17, 146–153. [Google Scholar] [CrossRef]
- National Institute for Statistics and Economic Studies (INSEE). Nomenclature d’Activités Françaises. 2000. Available online: https://www.insee.fr/fr/information/2406147 (accessed on 7 July 2021).
- International Labour Organization. International Standard Classification of Occupations; ILO: Geneva, Switzerland, 1968; Available online: https://ilo.primo.exlibrisgroup.com/discovery/fulldisplay/alma991141423402676/41ILO_INST:41ILO_V2 (accessed on 7 July 2021).
- Song, Y.; Li, X.; Du, X. Exposure to nanoparticles is related to pleural effusion, pulmonary fibrosis and granuloma. Eur. Respir. J. 2009, 34, 559–567. [Google Scholar] [CrossRef]
- Song, Y.; Li, X.; Wang, L.; Rojanasakul, Y.; Castranova, V.; Li, H.; Ma, J. Nanomaterials in Humans: Identification, Characteristics, and Potential Damage. Toxicol. Pathol. 2011, 39, 841–849. [Google Scholar] [CrossRef] [Green Version]
- Andujar, P.; Simon-Deckers, A.; Galateau-Sallée, F.G.; Fayard, B.; Beaune, G.; Clin, B.; Billon-Galland, M.-A.; Durupthy, O.; Pairon, J.-C.; Doucet, J.; et al. Role of metal oxide nanoparticles in histopathological changes observed in the lung of welders. Part. Fibre Toxicol. 2014, 11, 23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leprince, M.; Sancey, L.; Coll, J.-L.; Motto-Ros, V.; Busser, B. Elemental imaging using laser-induced breakdown spectroscopy: Latest medical applications. Med. Sci. MS 2019, 35, 682–688. [Google Scholar] [CrossRef]
- Viitanen, A.-K.; Uuksulainen, S.; Koivisto, A.J.; Hämeri, K.; Kauppinen, T. Workplace Measurements of Ultrafine Particles-A Literature Review. Ann. Work. Expo. Health 2017, 61, 749–758. [Google Scholar] [CrossRef] [PubMed]
- Audignon-Durand, S.; Gramond, C.; Ducamp, S.; Manangama, G.; Garrigou, A.; Delva, F.; Brochard, P.; Lacourt, A. Development of a Job-Exposure Matrix for Ultrafine Particle Exposure: The MatPUF JEM. Ann. Work Expo. Health 2021, 65, 516–527. [Google Scholar] [CrossRef] [PubMed]
- Manangama, G.; Migault, L.; Audignon-Durand, S.; Gramond, C.; Zaros, C.; Bouvier, G.; Brochard, P.; Sentilhes, L.; Lacourt, A.; Delva, F. Maternal occupational exposures to nanoscale particles and small for gestational age outcome in the French Longitudinal Study of Children. Environ. Int. 2019, 122, 322–329. [Google Scholar] [CrossRef]
- Manangama, G.; Gramond, C.; Audignon-Durand, S.; Baldi, I.; Fabro-Peray, P.; Gilg Soit Ilg, A.; Guénel, P.; Lebailly, P.; Luce, D.; Stücker, I.; et al. Occupational exposure to unintentionally emitted nanoscale particles and risk of cancer: From lung to central nervous system—Results from three French case-control studies. Environ. Res. 2020, 191, 110024. [Google Scholar] [CrossRef]
- Abramson, M.J.; Murambadoro, T.; Alif, S.M.; Benke, G.P.; Dharmage, S.C.; Glaspole, I.; Hopkins, P.; Hoy, R.F.; Klebe, S.; Moodley, Y.; et al. Occupational and environmental risk factors for idiopathic pulmonary fibrosis in Australia: Case-control study. Thorax 2020, 75, 864–869. [Google Scholar] [CrossRef]
- Andersson, M.; Blanc, P.D.; Torén, K.; Järvholm, B. Smoking, occupational exposures, and idiopathic pulmonary fibrosis among Swedish construction workers. Am. J. Ind. Med. 2021, 64, 251–257. [Google Scholar] [CrossRef]
- Jonsson, E.; Järvholm, B.; Andersson, M. Silica dust and sarcoidosis in Swedish construction workers. Occup. Med. 2019, 69, 482–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graff, P.; Larsson, J.; Bryngelsson, I.-L.; Wiebert, P.; Vihlborg, P. Sarcoidosis and silica dust exposure among men in Sweden: A case–control study. BMJ Open 2020, 10, e038926. [Google Scholar] [CrossRef] [PubMed]
- Rafnsson, V.; Ingimarsson, O.; Hjalmarsson, I.; Gunnarsdottir, H. Association between exposure to crystalline silica and risk of sarcoidosis. Occup. Environ. Med. 1998, 55, 657–660. [Google Scholar] [CrossRef] [Green Version]
- Taskar, V.; Coultas, D. Exposures and Idiopathic Lung Disease. Semin. Respir. Crit. Care Med. 2008, 29, 670–679. [Google Scholar] [CrossRef]
- Vincent, M.; Lievre, M. Sarcoidosis and pulmonary dust exposure, a plausible pathogenic link. Rev. Mal. Respir. 2002, 19, 103–104. [Google Scholar] [PubMed]
- Nanoparticle Task Force ACOEM. Nanotechnology and Health. J. Occup. Environ. Med. 2011, 53, 687–689. [Google Scholar] [CrossRef]
- Yokel, R.A.; MacPhail, R.C. Engineered nanomaterials: Exposures, hazards, and risk prevention. J. Occup. Med. Toxicol. 2011, 6, 7. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease | Number of Patients | Median Age (Min–Max) | Sex Ratio (M:F) | Smokers (Former Smokers) |
|---|---|---|---|---|
| With a known etiology | 58 | 70.5 (22–87) | 43:15 | 10.3% (46.6%) |
| Drug related ILD | 15 | 71 (46–81) | 14:1 | 6.7% (73.3%) |
| Infectious ILD | 12 | 69.5 (42–85) | 7:5 | 16.7% (33.3%) |
| Hypersensitivity pneumonitis | 7 | 75 (34–78) | 6:1 | 0% (14.3%) |
| Auto-immune pneumonitis | 5 | 72 (22–87) | 2:3 | 0% (40%) |
| Lymphangitis carcinomatosis/Neoplasia | 4 | 75.5 (67–83) | 2:2 | 0% (50%) |
| Desquamative interstitial pneumonia | 3 | 71 (48–81) | 2:1 | 66.7% (0%) |
| Pneumoconiosis | 2 | 50 (41–59) | 2:0 | 50% (50%) |
| Pulmonary veno-occlusive disease | 2 | 73 (72–74) | 2:0 | 0% (100%) |
| Antisynthetase syndrome | 2 | 70.5 (70–71) | 1:1 | 0% (50%) |
| Silicosis | 1 | 55 | 1:0 | 0% (100%) |
| Microscopic polyangiitis | 1 | 71 | 0:1 | 0% (0%) |
| Granulomatosis with polyangitis (Wegener’s granulomatosis) | 1 | 65 | 1:0 | 0% (0%) |
| Left heart failure | 1 | 59 | 1:0 | 0% (100%) |
| Lipoid pneumonia | 1 | 69 | 1:0 | 0% (100%) |
| Bronchiolitis obliterans | 1 | 40 | 1:0 | 0% (0%) |
| Idiopathic | 34 | 67.5 (25–81) | 22:12 | 14.7% (23.5%) |
| Sarcoidosis | 14 | 47 (25–80) | 6:8 | 14.3% (7.1%) |
| Idiopathic nonspecific interstitial pneumonia | 11 | 76 (46–81) | 8:3 | 9.1% (27.3%) |
| Idiopathic pulmonary fibrosis | 9 | 69 (61–81) | 8:1 | 22.2% (36.4%) |
| Others | 8 | 61 (46–83) | 3:5 | 0% (28.6%) |
| Patient Number | Lung Disease | Group (E: Disease of Known Etiology, I: Idiopathic Disease) | Occupations | Probability of Exposure to Nanoparticles: 0 Not Found, 1: Possible < 10%, 2: Likely 10–50%, 3: Very Likely > 50% | Final Exposure to Nanoparticles Probability: Highest Probability of Exposure to Nanoparticles in the Career | ||||
| 1 | 2 | 3 | Occupation 1 | Occupation 2 | Occupation 3 | ||||
| 1 | Drug related ILD | E | Coachbuilder/painter | Welder | Printing machine operator | 3 | 3 | 1 | 3 |
| 2 | Idiopathic pulmonary fibrosis | I | Textile products machine operator | 1 | 1 | ||||
| 3 | Drug related ILD | E | Farmer | Switching operator | Switching operator | 3 | 1 | 1 | 3 |
| 4 | Lymphangitis carcinomatosis/Neoplasia | E | Farmer | 2 | 2 | ||||
| 5 | Other | Mason | Refractory bricklayer | Ceramics operator | 3 | 3 | 3 | 3 | |
| 6 | Drug related ILD | E | Market gardener | Farmer | Farm hands | 0 | 2 | 1 | 3 |
| 7 | Other | Seamstress | Cook | Childminder | 1 | 3 | 1 | 3 | |
| 8 | Other | Floor sander | Truck driver | Pressman | 3 | 3 | 1 | 3 | |
| 9 | Idiopathic pulmonary fibrosis | I | Miner | Miner | Train driver | 3 | 3 | 3 | 3 |
| 10 | Drug related ILD | E | Miner | Tile setter | 3 | 3 | 3 | ||
| 11 | Auto-immune pneumonitis | E | Domestic help | Domestic help | 1 | 1 | 1 | ||
| 12 | Drug related ILD | E | Farmer | 3 | 3 | ||||
| 13 | Hypersensitivity pneumonitis | E | Bank employee | 0 | 0 | ||||
| 14 | Infectious ILD | E | Accountant | Medical secretary | 0 | 0 | 0 | ||
| 15 | Other | / | |||||||
| 16 | Infectious ILD | E | Printing machine operator | Printing machine operator | 1 | 1 | 1 | ||
| 17 | Lymphangitis carcinomatosis/Neoplasia | E | Masseuse | Chocolate—products machine operator | Waitress/manageress | 0 | 0 | 1 | 1 |
| 18 | Infectious ILD | E | Teacher | Teacher | 0 | 0 | 0 | ||
| 19 | Idiopathic pulmonary fibrosis | I | Mason | 3 | 3 | ||||
| 20 | Drug related ILD | E | Truck driver | Salesman | Company director | 3 | 0 | 0 | 3 |
| 21 | Drug related ILD | E | Pipe fitter/welder | 3 | 3 | ||||
| 22 | Desquamative interstitial pneumonia | E | Coachbuilder/painter | 3 | 3 | ||||
| 23 | Drug related ILD | E | Waitress | Waitress | Candle production machine operator | 0 | 2 | 0 | 2 |
| 24 | Other | Factory worker | Factory worker | Market gardener | 0 | 3 | 0 | 3 | |
| 25 | Pulmonary veno-occlusive disease | E | Farmer | 3 | 3 | ||||
| 26 | Idiopathic pulmonary fibrosis | I | Printing machine operator | Truck driver | Salesman | 1 | 3 | 0 | 3 |
| 27 | Idiopathic nonspecific interstitial pneumonia | I | Mason | Joiner | 3 | 3 | 3 | ||
| 28 | Idiopathic nonspecific interstitial pneumonia | I | Secretary | Secretary | Domestic help | 0 | 0 | 1 | 1 |
| 29 | Drug related ILD | E | Mason | Factory worker | 3 | 1 | 3 | ||
| 30 | Sarcoidosis | I | Seamstress | Childminder | Seamstress | 1 | 0 | 0 | 1 |
| 31 | Drug related ILD | E | Baker | Post officer | Foundry worker | 3 | 0 | 3 | 3 |
| 32 | Pneumoconiosis | E | Dental prosthetist | 3 | 3 | ||||
| 33 | Auto-immune pneumonitis | E | Carer | 0 | 0 | ||||
| 34 | Idiopathic nonspecific interstitial pneumonia | I | Baker | 3 | 3 | ||||
| 35 | Bronchiolitis obliterans | E | Boilermaker/welder | Pipe fitter/boilermaker/welder | 3 | 3 | 3 | ||
| 36 | Other | Cleaner | Saleswoman | Waitress/manageress | 0 | 0 | 1 | 1 | |
| 37 | Idiopathic nonspecific interstitial pneumonia | I | Domestic help | Food salesperson | Cashier | 1 | 2 | 0 | 2 |
| 38 | Sarcoidosis | I | Farmer | 3 | 3 | ||||
| 39 | Antisynthetase syndrome | E | |||||||
| 40 | Pulmonary veno-occlusive disease | E | Farmer | 3 | 3 | ||||
| 41 | Idiopathic pulmonary fibrosis | I | Plant operator | Plant operator | Cleaner | 1 | 3 | 1 | 3 |
| 42 | Granulomatosis with polyangitis (Wegener’s granulomatosis) | E | Joiner | 3 | 3 | ||||
| 43 | Sarcoidosis | I | Seamstress | Cleaner | Childminder | 1 | 1 | 0 | 1 |
| 44 | Left heart failure | E | Boilermaker/welder | Carpenter/metal fitter | Carpenter/metal fitter | 3 | 3 | 3 | 3 |
| 45 | Hypersensitivity pneumonitis | E | Farmer | 3 | 3 | ||||
| 46 | Infectious ILD | E | Joiner | 3 | 3 | ||||
| 47 | Idiopathic pulmonary fibrosis | I | Manufacturing labourer | Manufacturing labourer | 3 | 3 | 3 | ||
| 48 | Sarcoidosis | I | Salesman | Accountant | 0 | 0 | 0 | ||
| 49 | Idiopathic nonspecific interstitial pneumonia | I | Butcher | 1 | 1 | ||||
| 50 | Idiopathic pulmonary fibrosis | I | Manufacturing labourer | Baker | Mason | 3 | 3 | 3 | 3 |
| 51 | Pneumoconiosis | E | Joiner | 3 | 3 | ||||
| 52 | Microscopic polyangiitis | E | Saleswoman | 0 | 0 | ||||
| 53 | Idiopathic nonspecific interstitial pneumonia | I | Machine-tool operator | Manufacturing labourer | Fiberglass plant operator | 3 | 1 | 1 | 3 |
| 54 | Desquamative interstitial pneumonia | E | Waitress | Fruit picker | Cleaner in a plastic products factory | 2 | 0 | 2 | 2 |
| 55 | Sarcoidosis | I | Animator in retirement home | 0 | 0 | ||||
| 56 | Idiopathic nonspecific interstitial pneumonia | I | Foundry moulder | 3 | 3 | ||||
| 57 | Idiopathic pulmonary fibrosis | I | Hospital caregiver | 2 | 2 | ||||
| 58 | Sarcoidosis | I | Cleaner | 2 | 2 | ||||
| 59 | Idiopathic pulmonary fibrosis | I | |||||||
| 60 | Other | Speech therapist | Speech therapist | Speech therapist | 0 | 0 | 0 | 0 | |
| 61 | Infectious ILD | E | Gym teacher | 0 | 0 | ||||
| 62 | Auto-immune pneumonitis | E | Farmer | Textile products machine operator | 3 | 1 | 0 | 3 | |
| 63 | Drug related ILD | E | Optical assembler | Butcher | 0 | 0 | 0 | ||
| 64 | Lipoid pneumonia | E | Steel materials handling | Machine-tool operator | Mason | 3 | 3 | 3 | 3 |
| 65 | Desquamative interstitial pneumonia | E | Metal carpenter | 3 | 3 | ||||
| 66 | Sarcoidosis | I | Secretary | Policeman | 0 | 0 | 0 | ||
| 67 | Auto-immune pneumonitis | E | Office worker | Communications manager | Director | 1 | 0 | 1 | 1 |
| 68 | Infectious ILD | E | Plasterer/painter | Handler | 3 | 2 | 3 | ||
| 69 | Hypersensitivity pneumonitis | E | Cleaner | Quality manager | Windshield manufacturer | 2 | 0 | 3 | 3 |
| 70 | Auto-immune pneumonitis | E | Joiner | 3 | 3 | ||||
| 71 | Other | ||||||||
| 72 | Infectious ILD | E | Carer | 0 | 0 | ||||
| 73 | Hypersensitivity pneumonitis | E | Wood-products machine operator | Farmer | 3 | 3 | 3 | ||
| 74 | Drug related ILD | E | Metal polish | 3 | 3 | ||||
| 75 | Drug related ILD | E | Baker | Salesman | Estate agent | 3 | 1 | 1 | 3 |
| 76 | Hypersensitivity pneumonitis | E | Mason | Train driver | 3 | 3 | 3 | ||
| 77 | Sarcoidosis | I | Manufacturing labourers | Construction sites truck driver | Manufacturing labourers | 3 | 3 | 3 | 3 |
| 78 | Infectious ILD | E | Mason | Rubber products (tyre) machine operator | Textile products machine operator | 3 | 3 | 1 | 3 |
| 79 | Drug related ILD | E | Metal industry operator | Machine-tool operator | Boilermaker | 3 | 3 | 3 | 3 |
| 80 | Idiopathic nonspecific interstitial pneumonia | I | Manufacturing labourers | Textile products machine operator | 3 | 1 | 3 | ||
| 81 | Sarcoidosis | I | |||||||
| 82 | Lymphangitis carcinomatosis/Neoplasia | E | Meter reader | Storekeeper | Executive | 0 | 0 | 0 | 0 |
| 83 | Idiopathic nonspecific interstitial pneumonia | I | Textile products machine operator | 1 | 1 | ||||
| 84 | Antisynthetase syndrome | E | Baker | Machine-tool operator | Security officer | 3 | 3 | 0 | 3 |
| 85 | Infectious ILD | E | Farmer | 3 | 3 | ||||
| 86 | Silicosis | E | Miner | Mason | 3 | 3 | 3 | ||
| 87 | Sarcoidosis | I | Mason | 3 | 3 | ||||
| 88 | Infectious ILD | E | Textile products machine operator | 3 | 3 | ||||
| 89 | Infectious ILD | E | Chocolate—products machine operator | 1 | 1 | ||||
| 90 | Hypersensitivity pneumonitis | E | Plumber | 3 | 3 | ||||
| 91 | Drug related ILD | E | Machine-tool operator | Machine-tool operator | Metal coating machine operator | 3 | 3 | 3 | 3 |
| 92 | Idiopathic nonspecific interstitial pneumonia | I | Boilermaker | 3 | 3 | ||||
| 93 | Sarcoidosis | I | Electrician | Electrician in food industry | Electrician in mining plant | 1 | 1 | 3 | 3 |
| 94 | Idiopathic nonspecific interstitial pneumonia | I | Farmer | Machine finishing | Machine operator | 3 | 3 | 2 | 3 |
| 95 | Infectious ILD | E | Post officer | 0 | 0 | ||||
| 96 | Lymphangitis carcinomatosis/Neoplasia | E | Machine-tool operator | Policeman | 3 | 0 | 3 | ||
| 97 | Sarcoidosis | I | Train controller | Music teacher | 0 | 0 | 0 | ||
| 98 | Hypersensitivity pneumonitis | E | Welder/machine-tool operator | 3 | 3 | ||||
| 99 | Sarcoidosis | I | Electrician | 3 | 3 | ||||
| 100 | Sarcoidosis | I | Mason | Mover | Metal-heat-treating plant operator | 3 | 1 | 3 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Forest, V.; Pourchez, J.; Pélissier, C.; Audignon Durand, S.; Vergnon, J.-M.; Fontana, L. Relationship between Occupational Exposure to Airborne Nanoparticles, Nanoparticle Lung Burden and Lung Diseases. Toxics 2021, 9, 204. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9090204
Forest V, Pourchez J, Pélissier C, Audignon Durand S, Vergnon J-M, Fontana L. Relationship between Occupational Exposure to Airborne Nanoparticles, Nanoparticle Lung Burden and Lung Diseases. Toxics. 2021; 9(9):204. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9090204
Chicago/Turabian StyleForest, Valérie, Jérémie Pourchez, Carole Pélissier, Sabyne Audignon Durand, Jean-Michel Vergnon, and Luc Fontana. 2021. "Relationship between Occupational Exposure to Airborne Nanoparticles, Nanoparticle Lung Burden and Lung Diseases" Toxics 9, no. 9: 204. https://0-doi-org.brum.beds.ac.uk/10.3390/toxics9090204